vitamin
It has been reported that Kash Patel, Donald Trump’s pick to lead the FBI. Patel seems to be a scary man. During 2023 appearance on Steve Bannon‘s “War Room” podcast, Patel agreed that Trump is “dead serious” about his intent to seek revenge against his political enemies should he be elected in 2024. Patel stated:
“We will go out and find the conspirators — not just in government, but in the media … we’re going to come after the people in the media who lied about American citizens, who helped Joe Biden rig presidential elections … We’re going to come after you. Whether it’s criminally or civilly, we’ll figure that out. But yeah, we’re putting you all on notice, and Steve, this is why they hate us. This is why we’re tyrannical. This is why we’re dictators … Because we’re actually going to use the Constitution to prosecute them for crimes they said we have always been guilty of but never have.”
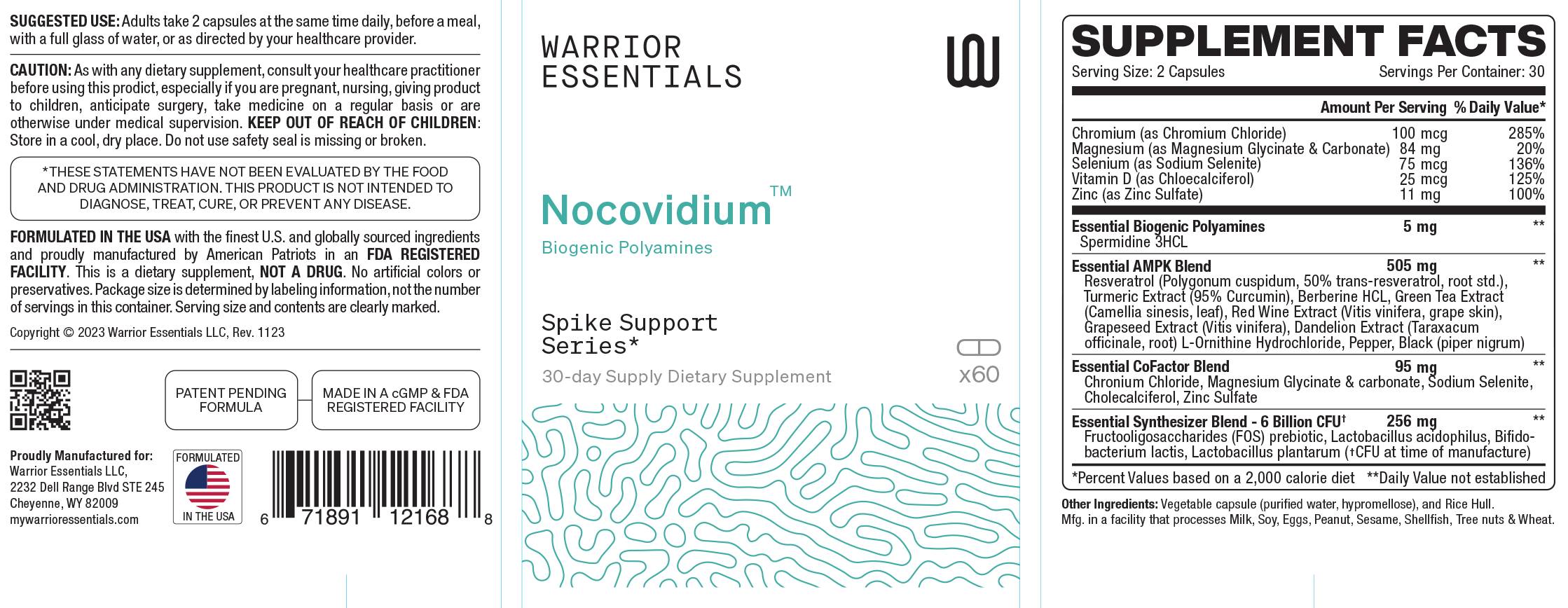
Meanwhile, Patel has been flogging a range of very odd products aimed at the MAGA crowd, making hundreds of thousands of dollars from Trump-aligned businesses. In particular, Patel promoted pills that claim to reverse the effects of the Covid-19 vaccine. Marketed under the trademark “Nocovidium,” the pills from a company called ‘Warrior Essentials’ contain a range of ‘natural ingredients none of which has been shown to do anything significant in relation to Covid-19 or vaccines:
“Spike the Vax, order this homerun kit to rid your body of the harms of the vax,” Patel said in a Truth Social post promoting the SCAM remedy. Another advert stated: “You were immune to the propaganda, but are you immune to the shedders.”
The website explains:
“The ingredients are listed above, but they break down into a few distinct categories. Polyamines are the driving force that helps to push the body into autophagy. These are found in many foods and are also in all living organisms. Our formula is designed to give a boost of externally supplied polyamines, while also working to turn your body into a polyamine producing gigafactory. This is done by providing the body the precursors, activators, and synthesizers to ramp up production. The third goal is to inhibit pathogens, including the spike protein, from interfering with the process. It’s a 1-2-3 patent-pending punch. Every ingredient was specifically chosen and balanced for its ability to promote autophagy, polyamine production, the inhibition of factors that can stop the process, or a combination of all three.”
The website even explains how the supplement works: “With regards to the spike protein, the body identifies this as a foreign object, and the autophagy process is designed to help protect your body by completely eliminating items like the spike. Many indicators show that the spike’s ability to block this process may be why the spikes are lasting far longer in the body than anybody ever expected. Our formula was developed to counter these measures allowing the process to complete and the objects, including the spike, identified by the body for removal, to be eliminated.”
Is there any evidence?
One should not ask such probing questions!
Why not?
The answer is as simple as it is scary: “We’re going to come after you!”
A journalist from the DAILY MAIL alerted me to the fact that yet another celebrity having decided to sell dietary supplements, interviewed me on the subject, and eventually published an article about it. One would not have thought that the Beckhams are short of money – so, why did David Beckham turn into a snake-oil salesman? I am far from being able to answer this question. What I now do know is that, via his firm ‘IM8’, he has started marketing two supplements (one of his slogans is ‘Built by Science, Trusted by Beckham’):
Daily Ultimate Essentials: All-in-One Supplement
This is a ‘multi-everything’ supplement. The only truly remarkable thing about it is its price tag. There are hundreds of similar products on the market. Almost all of them are much cheaper, and none is helpful for anyone who is healthy and consumes a balanced diet, as far as I can see.
Daily Ultimate Longevity: Healthy Aging
The implication here seems to be not a trivial one; the name clearly implies that we live longer, if we regularly bought this supplement. Not onlly that, we would also be healthier! I can see no evidence for either of these claims, yet a simple calculation tells me that we would be considerably poorer, if we fell for this advertising gimmick.
On the website, we learn a bit more:
At IM8, our commitment to science goes beyond innovation—it’s the foundation of everything we do. A world-class team of experts from space science, medicine, and academia has united with one goal: to revolutionize wellness. We’ve pioneered CRT8™ (Cell Rejuvenation Technology 8), designed to enhance cellular rejuvenation and push the limits of what’s possible in health.
Each of our products undergoes rigorous third-party testing and clinical trials, ensuring purity, efficacy, and results you can trust. With IM8, you’re getting scientifically driven core nutrition for optimal health and longevity.
___________________
I feel embarrassed for the ‘world-class team of experts from space science, medicine, and academia’ who give their good name to this hyped up nonsense. Moreover, I ask myself whether David Beckham’s new attempt to increase his wealth might be a case for the Advertising Standards Authority (ASA).
While medical experts across the world have expressed dismay at Trump’s appointment of Robert Kennedy, the ‘International chiropractors Association’ has just published this remarkable note:
Donald J. Trump made it official that he was nominating Robert F. Kennedy, Jr. to serve as the Secretary of Health and Human Services. Secretary-designee Kennedy has spent his entire career championing the health of the nation through education, advocacy, research and when needed litigation.
Among his many accomplishments are protecting the environment with Riverkeeper and the Natural Resources Defense Council His work at Riverkeeper succeeded in setting long-term environmental legal standards. Kennedy won legal battles against large corporate polluters. He became an adjunct professor of environmental law at Pace University School of Law in 1986 and founded the Pace’s Environmental Litigation Clinic which he co-directed for a decade.
It would be in the Pace Law Review that the landmark paper, “Unanswered Questions from the Vaccine Injury Compensation Program: A Review of Compensated Cases of Vaccine-Induced Brain Injury” (https://digitalcommons.pace.edu/cgi/viewcontent.cgi?article=1681&context=pelr) would be published in 2011.
Kennedy became laser focused on the autism epidemic while giving lectures on the dangers of mercury in fish, he was repeatedly approached by the mothers of children born healthy who regressed into autism after suffering adverse reactions from childhood vaccines, including their concern about the mercury-based preservative, thimerosal, being used in vaccines including the Hepatitis B vaccine given at birth. Kennedy’s approach to the issue was the same as it always, looking at the science. He assembled a team who gathered all the science and reviewed the issues with him. This resulted in the publication of the book, Thimerosal: Let the Science Speak
The Evidence Supporting the Immediate Removal of Mercury—a Known Neurotoxin—from Vaccines.
After establishing and leading the nonprofit Children’s Health Defense, last year Kennedy stepped back from the organization to throw his hat in the ring to be President. Becoming the embodiment of his uncle John F. Kennedy’s famous quote, “Ask not what your country can do for you, but what you can do for your country!”, Kennedy reached out to President Trump to form an alliance to focus on the crisis of chronic disease in the United States, and suspended his campaign to focus on the Make American Healthy Again (MAHA) Initiative.
ICA President, Dr. Selina Sigafoose Jackson, who is currently in Brazil promoting the protection of chiropractic as a separate and distinct profession stated, “Many ICA members have been supporters of Robert F. Kennedy, Jr.’s philanthropic activities and are all in on the MAHA Initiative. The Mission, Vision, and Values of the ICA align with the stated goals of the MAHA Initiative. We stand ready to provide policy proposals and experts to serve as advisors to the incoming Administration and to Secretary Kennedy upon his swearing in.”
____________________________
Perhaps I am permitted to contrast this with some health-related truths about Robert F. Kennedy, Jr. (my apologies, if the list is incomplete – please add to it by posting further important issues):
- Robert F. Kennedy, Jr. has, since about 20 years, been a leading figure of the anti-vaccine movement.
- During the epidemic, he pushed the conspiracy theory that “the quarantine” was used as cover to install 5G cell phone networks.
- He claimed that “one out of every six American women has so much mercury in her womb that her children are at risk for a grim inventory of diseases, including autism, blindness, mental retardation and heart, liver and kidney disease.”
- He wrote that, “while people were dying at the rate of 10,000 patients a week, Dr. Fauci declared that hydroxychloroquine should only be used as part of a clinical trial. For the first time in American history, a government official was overruling the medical judgment of thousands of treating physicians, and ordering doctors to stop practicing medicine as they saw fit.”
- He pushed the conspiracy theory that COVID-19 had been “ethnically targeted” to spare Ashkenazi Jews and Chinese people.”
- He claimed in a 2023 podcast interview that “There’s no vaccine that is safe and effective”.
- In a 2021 podcast, he urged people to “resist” CDC guidelines on when kids should get vaccines.
- He founded Children’s Health Defense’ that spreads fear and mistrust in science. One chiropractic group in California had donated $500,000 to this organisation.
- In 2019, he visited Samoa where he became partly responsible for an outbreak of measles, which made 5,700 people sick and killed 83 of them.
- He called mercury-containing vaccines aimed at children a holocaust. In 2015, he compared the horrors committed against Jews to the effects of vaccines on children. “They get the shot, that night they have a fever of a hundred and three, they go to sleep, and three months later their brain is gone. This is a holocaust, what this is doing to our country.”
- He repeatedly alleged that exposure to chemicals — “endocrine disruptors” — is causing gender dysphoria in children and contributing to a rise in LGBTQ-youth. According to him, endocrine disruptors are “chemicals that interfere with the body’s hormones and are commonly found in pesticides and plastic.”
- He stated “Telling people to “trust the experts” is either naive or manipulative—or both.”
- He plans to stop water fluoridation.
- He slammed the FDA’s “suppression” of raw milk.
- He said that a worm ate part of his brain which led to long-lasting “brain fog.”
- He has a 14-year-long history of abusing heroin from the age of 15. The police once arrested him for possession; he then faced up to two years in jail for the felony but was sentenced to two years probation after pleading guilty.
- He stated: “WiFi radiation … does all kinds of bad things, including causing cancer…cell phone tumors behind the ear.”
- He claimed that rates of autism have increased even though “there has been no change in diagnosis and no change in screening either.” Yet, both have changed significantly.
- He wrote: (Fauci’s) “obsequious subservience to the Big Ag, Big Food, and pharmaceutical companies has left our children drowning in a toxic soup of pesticide residues, corn syrup, and processed foods, while also serving as pincushions for 69 mandated vaccine doses by age 18—none of them properly safety tested.”
- He stated that cancer rates are skyrocketing in the young and the old – a statement that is evidently untrue.
- He authored a viral post on X: “FDA’s war on public health is about to end. This includes its aggressive suppression of psychedelics, peptides, stem cells, raw milk, hyperbaric therapies, chelating compounds, ivermectin, hydroxychloroquine, vitamins, clean foods, sunshine, exercise, nutraceuticals and anything else that advances human health and can’t be patented by Pharma. If you work for the FDA and are part of this corrupt system, I have two messages for you: 1. Preserve your records, and 2. Pack your bags.”
- He has also aligned himself with special interests groups such as anti-vaccine chiropractors.
- He stated categorically: “You cannot trust medical advice from medical professionals.”
- He said he’s going to put a pause on infectious diseases research for 8 years.
- He promoted the unfounded theory that the CIA killed his uncle, former President John F. Kennedy.
- He linked school shootings to the increased prescription of antidepressants.
- An evaluation of verified Twitter accounts from 2021, found Kennedy’s personal Twitter account to be the top “superspreader” of vaccine misinformation on Twitter, responsible for 13% of all reshares of misinformation, more than three times the second most-retweeted account.
PS
Let me finish with a true statement: The World Health Organization has estimated that global immunization efforts have saved at least 154 million lives in the past 50 years.
Advocates of so-called alternative medicine (SCAM) almost uniformly stress the importance of prevention and pride themselves to make much use of SCAM for the purpose of prevention. SCAM, they often claim, is effective for prevention, while conventional medicine tends to neglect it. Therefore, it seems timely to ponder a bit about the subject.
It makes sense to differentiate three types of prevention:
- Primary prevention aims to prevent disease or injury before it ever occurs.
- Secondary prevention aims to reduce the impact of a disease or injury that has already occurred.
- Tertiary prevention aims to soften the impact of an ongoing illness or injury that has lasting effects.
Here I will includes all three and I will ask what SCAM has to offer in any form of prevention. I will do this by looking at what we have previously discussed on this blog in relation to several specific SCAM and add in each case a very brief evaluation of the evidence.
Acupuncture
- Acupuncture for the prevention of headache? How to fool (almost) everyone with an RCT – NO CONVINCING EVIDENCE
- Acupuncture for chronic migraine prevention? Two new systematic reviews yield encouraging evidence – ENCOURAGING EVIDENCE
Chiropractic
- Chiropractic manipulation and primary prevention. It’s time that chiropractors stop misleading the public in order to fill their pockets – NO CONVINCING EVIDENCE
- ‘Maintenance care’ is very good for chiropractic economics … but not for anything else! – NO CONVINCING EVIDENCE
- No evidence that spinal manipulation improves immune function – NO CONVINCING EVIDENCE
- Chiropractic maintenance care: boosting chiropractic cash flow in perpetuity – NO CONVINCING EVIDENCE
- Birth-trauma: a diagnosis that richly fills the pockets of many chiropractors – NO CONVINCING EVIDENCE
- If you don’t want to get the flu…consult your chiropractor urgently! – NO CONVINCING EVIDENCE
Herbal medicine
- Prevention of acute radiation-induced proctitis with Aloe vera – ENCOURAGING EVIDENCE
- Can Chinese Medicine Be Used for Prevention of Corona Virus Disease? – NO CONVINVING EVIDENCE
Homeopathy
- Effectiveness of Homeopathic Arsenicum album 30C in the Prevention of COVID-19 – NO CONVINCING EVIDENCE
- Disturbing news on the recent trial of homeopathy for COVID prevention – NO CONVINCING EVIDENCE
- A new study of homeopathy for the prevention of COVID-19 infections – NO CONVINCING EVIDENCE
- Is this the crown of the Corona-idiocy? Nosodes In Prevention And Management Of COVID -19 – NO CONVINCING EVIDENCE
- Homeopathic Prevention and Management of Epidemic Diseases – NO CONVINCING EVIDENCE
- Influenzinum: the homeopathic flu prevention that does not prevent flu – NO CONVINCING EVIDENCE
- Homeopathy for preventing and treating acute respiratory tract infections in children – NO CONVINCING EVIDENCE
- A new trial of homeopathy for preventing COVID-19 infections – NO CONVINCING EVIDENCE
- Oscillococcinum, the homeopathic solution to the coronavirus threat? – NO CONVINCING EVIDENCE
- An RCT suggests that homeopathy can prevent epidemics!!! But how reliable is this evidence? – NO CONVINCING EVIDENCE
- HOMEOPATHS LOVE IT: the epidemiological evidence suggesting that homeopathy works – NO CONVINCING EVIDENCE
- Understanding homeoprophylaxis: it is dangerous nonsense!!! – NO CONVINCING EVIDENCE
- “Homeoprophylaxis, the homeopathic vaccine alternative, prevents disease through nosodes.” NO CONVINCING EVIDENCE
- Boiron’s new study of homeopathy NO GOOD EVIDENCE
Mind-body therapies
- Meditation for the primary and secondary prevention of cardiovascular disease – NO CONVINCING EVIDENCE
- Transcendental meditation (TM) for the primary prevention of cardiovascular disease? – NO CONVINCING EVIDENCE
Osteopathy
Does Osteopathy Prevent Motion Sickness? – NO CONVINCING EVIDENCE
Supplements
- Multivitamins in the prevention of cancer and cardiovascular disease – NO CONVINCING EVIDENCE
- Zinc for the prevention or treatment of acute viral respiratory tract infections in adults? A new systematic review – NO CONVINCING EVIDENCE
- Vitamin D for the prevention or treatment of COVID-19? NO CONVINCING EVIDENCE
- Supplements for the prevention of cardiovascular disease and cancer – NO CONVINCING EVIDENCE
- Do Vitamin, Mineral, and Multivitamin Supplements Prevent Cardiovascular Disease and Cancer? – NO CONVINCING EVIDENCE
- Does vitamin D supplementation lower the risk of cancer and precancers? – NO CONVINCING EVIDENCE
- Glucosamine is associated with decreased risk of lung cancer – ENCOURAGING EVIDENCE
Yoga
- Yoga for the prevention of cardiovascular disease: more than wishful thinking? – NO CONVINCING EVIDENCE
- Who says it’s all negative? The addition of yoga to aerobic exercise programs reduces global cardiovascular risk – ENCOURAGING EVIDENCE
I hope you agree: this list is impressive!
- Impressive in the way of showing how often we have discussed SCAM for prevention in one form or another.
- Impressive also to see how little positive evidence there is for effective prevention with SCAM
Of course, this is merely based on posts that were published on my blog. Some will argue that I missed out on some effective SCAMs for prevention. Others might claim that I judged some of the the above cited articles too harshly. If you share such sentiments, I invite you to show me the evidence – and I promise to look at it and evaluate it critically.
Meanwhile, I will draw the following conclusion:
Despite the prominent place prevention assumes in discussions about SCAM, the actual evidence fails to show that it has an important role to play in primary, secondary or tertiary prevention.
It has been reported that the American Board of Internal Medicine (ABIM) has revoked the certifications for two prominent US physicians. They are both (in)famous for leading an organization that promotes ivermectin as a treatment for COVID-19.
- Pierre Kory, MD, is no longer certified in critical care medicine, pulmonary disease, and internal medicine, according to the ABIM website.
- Paul Ellis Marik, MD, is no longer certified in critical care medicine or internal medicine.
Marik is the chief scientific officer and Kory is president emeritus of the Front Line COVID-19 Critical Care (FLCCC) Alliance, a group they founded in March 2020. The FLCCC gained notoriety during the height of the pandemic for advocating ivermectin as a treatment for COVID. It now espouses regimens of supplements to treat “vaccine injury” and also offers treatments for Lyme disease.
Kory and Marik stated, “we believe this decision represents a dangerous shift away from the foundation principles of medical discourse and scientific debate that have historically been the bedrock of medical education associations.” The FLCCC said in the statement that it, along with Kory and Marik, are “evaluating options to challenge these decisions.” Kory and Marik said they were notified in May 2022 that they were facing a potential ABIM disciplinary action. An ABIM committee recommended the revocation in July 2023, saying the two men were spreading “false or inaccurate medical information,” according to FLCCC. Kory and Marik lost an appeal. In a 2023 statement, Kory and Marik called the ABIM action an “attack on freedom of speech.”
To this, Wikipedia adds that, Marik is the inventor of the “Marik protocol”, also known as the “HAT” protocol, which proposes intravenous administration of hydrocortisone, ascorbic acid, and thiamine as a treatment for preventing sepsis for people in intensive care. Marik’s own initial research, published with four other authors in Chest in 2017, showed a dramatic evidence of benefit. The single-center, observational study compared outcomes of 47 consecutive sepsis patients who were treated with HAT during a 7-month period to 47 consecutive control patients during the preceding 7-month period. The study reported 19 deaths in the control group and 4 deaths in the treatment group. Marik’s findings received attention on social media and National Public Radio, but drew criticism from the wider medical community for being science by press conference. ER doctor Jeremy Faust was one of a number of skeptics of the results, noting the low reliability of the study design and potential for bias. The controversy prompted other groups to conduct studies of the HAT protocol. A systematic review of six randomized and five non-randomized controlled trials in 2021 eventually concluded that the claimed benefits of the protocol could not be confirmed.
In November 2022, Pierre Kory and the FLCCC began marketing a cocktail of supplements and drugs (e.g. ivermectin and nitazoxanide) for other viruses, influenza and Respiratory syncytial virus (RSV). Like the FLCCC-advocated COVID treatments, the recommendations lacked credible supporting scientific evidence. The cocktail could cost over $500.
Wikipedia also mentions that, in March 2024, Kory and Marik published an op-ed in The Hill claiming that long COVID was caused by COVID-19 vaccination instead of COVID-19 infection. The op-ed was republished by the German disinformation outlet Disclose.tv. The fact-checking website Health Feedback found that the op-ed relied on anecdotes that did not provide evidence to support the claim.
A new market report predicts that the worldwide market for so-called alternative medicine (SCAM) will grow from $100 billion in 2022 to $438 billion by 2032.
According to the report, the SCAM market is expected to see innovation and expansion through mergers, acquisitions, and partnerships among large companies. Companies that are capitalizing on these trends include health supplement companies, companies that specialize in Ayurvedic health, those that offer TCM solutions, and those that offer more general holistic solutions to health. Major supplement brands include Herb Pharm LLC, Gaia Herbs, NOW Foods, Life Extension, Pure Encapsulations, Douglas Laboratories, Nordic Naturals, Nordic Nutraceuticals, Quality of Life Labs, Nature’s Bounty Co., Valensa International, Herbo Nutra, and Emerson Ecologics.
Other major players mentioned in the report are:
- AYUSH Ayurvedic Pte Ltd, Dabur India Ltd., Himalaya Global Holdings Ltd., Banyan Botanicals, and Arya Vaidya Pharmacy offer Ayurvedic health and wellness products while aiming to advance the science behind Ayurveda.
- Sheng Chang Pharmaceutical Company produces traditional Chinese medicines and herbal products that is one of the largest TCM pharma companies.
- All and One Medical provides healthcare solutions that combine conventional medicine with complementary and alternative therapies to promote overall wellness and preventive care.
- The John Schumacher Unity Woods Yoga Center is another that focuses on enhancing physical and mental well-being through the practice of Iyengar Yoga and offers classes and workshops.
- New Life Chiropractic aims to improve overall health and well-being by providing comprehensive chiropractic care that focuses on spinal health and preventive wellness.
- The Chicago Body Works offers a range of therapies and treatments designed to enhance physical and mental well-being, including massage and bodywork services.
- Weleda AG aims to connect people with nature by producing natural organic products that support health, beauty, and overall wellness while practicing sustainability and social responsibility.
- Quantum-Touch Inc. teaches energy healing techniques that promote physical, emotional, and spiritual health.
- Spectrum Chemical Manufacturing Corporation focuses on delivering high-quality chemicals and laboratory supplies to support scientific research and innovation across various industries, including health and wellness.
I must admit, I do like these market reports. They never fail to amuse me – for two main reasons:
- They are as reliable as reading tea leafs.
- The only reliable info they do provide is that the SCAM proponents’ often-voiced argument, “we are very different from BIG PHARMA” is pure nonsense.
We have recently heard much about spinal manipulations for kids. It might therefore be relevant to learn about an international taskforce of clinician-scientists formed by specialty groups of World Physiotherapy – International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT) & International Organisation of Physiotherapists in Paediatrics (IOPTP) – to develop evidence-based practice position statements directing physiotherapists clinical reasoning for the safe and effective use of spinal manipulation and mobilisation for paediatric populations (<18 years) with varied musculoskeletal or non-musculoskeletal conditions.
A three-stage guideline process using validated methodology was completed: 1. Literature review stage (one scoping review, two reviews exploring psychometric properties); 2. Delphi stage (one 3-Round expert Delphi survey); and 3. Refinement stage (evidence-to-decision summative analysis, position statement development, evidence gap map analyses, and multilayer review processes).
Evidence-based practice position statements were developed to guide the appropriate use of spinal manipulation and mobilisation for paediatric populations. All were predicated on clinicians using biopsychosocial clinical reasoning to determine when the intervention is appropriate.
1. It is not recommended to perform:
• Spinal manipulation and mobilisation on infants.
• Cervical and lumbar spine manipulation on children.
•Spinal manipulation and mobilisation on infants, children, and adolescents for non-musculoskeletal paediatric conditions including asthma, attention deficit hyperactivity disorder, autism spectrum disorder, breastfeeding difficulties, cerebral palsy, infantile colic, nocturnal enuresis, and otitis media.
2. It may be appropriate to treat musculoskeletal conditions including spinal mobility impairments associated with neck-back pain and neck pain with headache utilising:
• Spinal mobilisation and manipulation on adolescents;
• Spinal mobilisation on children; or
• Thoracic manipulation on children for neck-back pain only.
3. No high certainty evidence to recommend these interventions was available.
Reports of mild to severe harms exist; however, risk rates could not be determined.
It was concluded that specific directives to guide physiotherapists’ clinical reasoning on the appropriate use of spinal manipulation or mobilisation were identified. Future research should focus on trials for priority conditions (neck-back pain) in children and adolescents, psychometric properties of key outcome measures, knowledge translation, and harms.
Whether one agrees with these directions or not (and I am not sure I fully do), I have always thought that people who, despite the largely lacking or flimsy evidence for spinal manipulations, insist on having manual therapy should consult a physiotherapist, rather than a chiropractor or osteopath.
Why?
Because, in my experience, physiotherapist:
- display less cult-dependent behaviours,
- do not follow the gospel of charlatans, like Palmer and Still,
- do not believe in the fiction of subluxation,
- are not so money-minded,
- less prone to use un- or disproven methods, like applied kinesiology, homeopathy, cranial osteopathy, etc.,
- unlikely to try to sell you useless dietary supplements,
- tend to judge better their limits of professional competence,
- are far less likely to try to persuade you of BS related to anti-vax, anti-drug, anti-science, anti-EBM, etc.
Although the vaccine has many individual and social benefits, ‘Vaccine Hesitancy’ has led to an increase in the number of vaccine-preventable diseases.
The aim of this study is to determine the effect of ideas that cause vaccine hesitancy to comply with traditional medicine practices and drugs and to determine the ratio of parents’ preference for so-called alternative medicine (SCAM).
This study was performed on the parents who refused vaccination in their children under the age of 8 between the years 2017-2022. Parents of the vaccinated children who were matched for age and gender were determined as the control group. Demographic characteristics of families, education levels, compliance ratios for well-child follow-up and pregnancy follow-up, preference ratios for traditional medicine and/or SCAM applications were compared.
A total of 123 families, 61 of whom were vaccine refusal and 62 of the control group, were included in the study. It was determined that the ratio of parents who refuse vaccination have increased in the last five years. The education level was found to be higher in the SCAM group (p=0.019). The most common reasons for vaccine refusal were distrust of the vaccine content (72.1%) and noncompliance with religious beliefs (49.1%). It was also found that the ratios of prophylactic vitamin use and tetanus vaccination of mothers during pregnancy were lower in the SCAM group. While the rate of compliance with vitamin D and iron prophylaxis for infants was lower in the vaccine refusal group, the ratio of preference for SCAM was higher.
The authors conclused that vaccine hesitancy is a complex issue that affects public health, in which many individual, religious, political and sociological factors play a role. As with recent studies, this research shows that the most important reason for vaccine rejection is “lack of trust”. The higher education level in the vaccine refusal group may also be a sign of this distrust. Not only the rejection of the vaccine, but also the lack of use of vitamin drugs seems to be related to lack of trust. This may also cause SCAM methods to be preferred more. These results show that providing trust in vaccination is the biggest step in the fight against vaccine hesitancy.
We have discussed the link between SCAM and vaccination hesitancy many times before, e.g.:
- How to reduce vaccination hesitancy?
- Reasons for parental hesitancy or refusal of childhood vaccination
- Anthroposophic medicine and vaccine hesitancy: are there links?
- Endorsement of so-called alternative medicine (SCAM) and vaccine hesitancy among physicians
- So-called alternative medicine (SCAM) and vaccine hesitancy among physicians: findings from Germany, Finland, Portugal, and France
- Echo chambers of vaccine hesitancy and so-called alternative medicine (SCAM)
- Intelligence, Religiosity, SCAM, Vaccination Hesitancy – are there links?
- Vaccine hesitancy and so-called alternative medicine (SCAM)
This new study seems to imply that the common denominator of both SCAM use and vaccination hesitancy is distrust, distrust in vaccinations and distrust in conventional medicine. That makes sense at first glance but not when you think about it for only a minute.
I can see why people distrust conventional medicine (to some extend, I do it myself). But why should distrust motivate some people to put their trust into SCAM which is even less trustworthy than conventional medicine. The rational thing for a distrusting person would be to critically assess the evidence and go where the evidence leads him/her. This path cannot possibly lead to SCAM but would lead to the best available evidence-based therapies.
If we consider this carefully, we arrive at the conclusion that not distrust but a degree of irrationality is more likely be the common denominator between SCAM use and vaccination hesitancy.
What do you think?
In the previous two parts of this series (see here and here), we discussed the following SCAM diagnoses:
- adrenal fatigue,
- candidiasis hypersensitivity,
- chronic intoxications,
- chronic Lyme disease,
- electromagnetic hypersensitivity,
- homosexuality.
Today, I will add three further fake diagnoses to the list.
Leaky gut syndrome
Leaky gut syndrome is allegedly caused by the passage of harmful substances from the gut wall into the body. SCAM proponents claim it is the origin of many conditions, including multiple sclerosis and autism. However, there is no evidence to show that these claims are true. SCAM practitioners nevertheless recommend many types of SCAM to treat the non-existing entity, e.g. SCAM diets, supplements, etc. It goes without saying that none of them have been shown to be effective.
Multiple chemical sensitivity
Multiple chemical sensitivity is allegedly caused by a hypersensitivity to commonly used chemicals. The symptoms are vague such as headache, dizziness, fatigue. Even those who believe that the condition exist are unable to offer a generally accepted definition of the syndrome.
The SCAMs recommended include:
- Nutritional supplements
- Digestive aids
- Hormone balancing
- Detoxification
- Desensitization
- Eliminating occult infections
- Oxygen
- Immune stimulation
Naturally, none of them is supported by sound evidence.
Neurasthenia
In 1869, physician George Miller Beard developed a diagnostic profile for a mental disorder that appeared to be common in the US. Neurasthenia was allegedly characterised by migraines, fatigue, depression, and digestive problems.
The cure, according to Beard, was to flee the city – because it was the stresses of city life that caused the condition. Women were encouraged to rest, while men were asked to engage in outdoor activities. By the early 20th century, this mental disorder had become a status symbol, and it soon spread to other parts of the world. But this pandemic was short-lived: by 1930, neurasthenia had virtually disappeared from conventional medicine.
In SCAM, however, neurasthenia is still a well-establisged money earner. SCAM practitioners do not hesitate to recomment virually every SCAM under the sun for it. They all have one thing in common: they do not work.
He came to my attention via the sad story recently featured here about patients allegedly being harmed or killed in a Swiss hospital for so-called alternative medicine (SCAM). What I then learned about the doctor in charge of this place fascinated me:
Rau states about himself (my translation):
Early on, Dr Rau focused on natural therapies, in particular homeopathy and dietary changes. The healing success of his patients proved him right, so he studied alternative healing methods with leading practitioners. These included orthomolecular medicine, Chinese and Ayurvedic medicine and European holistic medicine. With his wealth of knowledge and over 30 years of experience, Dr Rau formed his own holistic theory of healing: Swiss Biological Medicine – Dr Rau’s Biological Medicine. It is based on the principles of detoxification, nutrition, digestion and sustainable strengthening of the immune system.
Career & studies:
- Medical studies at the University of Bern
- Final medical examinations in Switzerland and the USA
- Subsequent work in rheumatology, internal and general medicine
- Member of the Swiss Medical Association FMH since 1981
- 1981 to 1992 conventional physician & medical director of a Swiss spa centre for rheumatology and rehabilitation medicine
- 1983 to 1992 Doctor at a drug rehabilitation centre
- 1992 to 2019 Establishment of the Paracelsus Clinic Lustmühle as medical director and partner
- until 2020 Head of the academic network and training organisation “Paracelsus Academy”
Rau also states this:
- 2019 mit dem Honorarprofessoren-Titel von der Europäischen Universität in Wien ausgezeichnet (2019, he was awarded the title of homorary professor at the European University in Vienna)
This puzzles me because there is no such institution as the ‘Europäische Universität in Wien’. There is a Central European University but this can hadly be it?!
Now, I am intrigued and see what the ‘honorary professor’ might have published. Sadly, there seems to be nothing on Medline except 2 interviews. In one interview, Rau explains (amongst other things) ‘live blood analysis’, a method that we have repeatedly discussed before (for instance, here and here):
Darkfield microscopy shows a lot. We take 1 drop of blood and look at it under a very large-scale magnification. The blood is life under the glass. Once it’s on the glass, there isn’t oxygen or light or heat. This is a giant stress for the blood. So we see how, over a time, the blood reacts to this stress, and how the blood cells tolerate the stress. You can see the changes. So we take a drop of blood that represents the organism and put it under stress and look at how the cells react to the stress, and then we can see the tolerance and the resistiveness of these cells. Do they have a good cell-membrane face? Do they have good energetic behavior? Do they clot together? Is there a chance for degenerative diseases? Is there a cancerous tendency in this blood? We see tendencies. And that’s what we are interested in, tendencies.
Question: If you saw a cancerous tendency, what would that look like?
Rau: Cancerous tendency is a change in the cells. They get rigid, so to say. They don’t react very well.
Question: And how long does blood live outside the body?
Rau: It can live for several days. But after 1 hour, the blood is already seriously changed. For example, a leukemia patient came to my clinic for another disease. But when we did darkfield, I found the leukemia. We saw that his white blood cells were atypical. Look at this slide—the fact that there are so many white blood cells together is absolutely unusual, and the fact that there are atypical white blood cells. This shows me that the patient has myeloid leukemia. The patient had been diagnosed as having rheumatoid lung pain, but it was absolutely not true. The real cause of his pain was an infiltration of the spinal bone by these lymphocytes.
This is, of course, complete nonsense. As I explained in my blog post, live blood analysis (LBA) is not plausible and there is no evidence to support the claims made for it. It also is by no means new; using his lately developed microscope, Antony van Leeuwenhoek observed in 1686 that living blood cells changed shape during circulation. Ever since, doctors, scientists and others have studied blood samples in this and many other ways.
New, however, is what today’s SCAM practitioners claim to be able to do with LBA. Proponents believe that the method provides information about the state of the immune system, possible vitamin deficiencies, amount of toxicity, pH and mineral imbalance, areas of concern and weaknesses, fungus and yeast infections, as well as just about everything else you can imagine.
LBA is likely to produce false-positive and false-negative diagnoses. A false-positive diagnosis is a condition which the patient does not truly have. This means she will receive treatments that are not necessary, potentially harmful and financially wasteful. A false-negative diagnosis would mean that the patient is told she is healthy, while in fact she is not. This can cost valuable time to start an effective therapy and, in extreme cases, it would hasten the death of that patient. The conclusion is thus clear: LBA is an ineffective, potentially dangerous diagnostic method for exploiting gullible consumers. My advice is to avoid practitioners who employ this technique.
And what does that say about ‘honorary professor’ Rau?
I think I let you answer that question yourself.