Monthly Archives: July 2023
We have discussed the currently fashionable herbal remedy, ‘kratom‘, before:
Inadequate regulation of Kratom supplements put consumers at risk
News about Kratom: the herb was recently (semi-)legalized in Thailand
Kratom: a ‘herbal drug’ with the potental to do more harm than good
A quick recap:
Kratom is made of the leaves of Mitragyna speciosa, a tree endogenous to parts of Southeast Asia. It has been used traditionally for its stimulant, mood-elevating, and analgesic effects. The plant’s active constituents, mitragynine and 7-hydroxymitragynine, have been shown to modulate opioid receptors, acting as partial agonists at mu-opioid receptors and competitive antagonists at kappa- and delta-opioid receptors. Both alkaloids are G protein-biased agonists of the mu-opioid receptor and therefore, may induce less respiratory depression than classical opioid agonists. The Mitragyna alkaloids also appear to exert diverse activities at other brain receptors (including adrenergic, serotonergic, and dopaminergic receptors), which may explain the complex pharmacological profile of raw kratom extracts. By the early 2000s, kratom was increasingly used in the US as a substitute for prescription and illicit opioids for managing pain and opioid withdrawal by people seeking abstinence from opioids. There are numerous assessments where people have been unable to stop using kratom and withdrawal signs and symptoms are problematic. Kratom does not appear in normal drug screens and, when taken with other substances of abuse, may not be recognized.
Now it has been reported that the family of a Florida woman who died in 2021 after ingesting kratom has been awarded more than $11m from a distributor of the herbal extract. “There is of course no amount of money that will make up for the pain and suffering that Ms Talavera’s children are enduring because of their mother’s death,” Middlebrooks wrote in court records addressing the sanction against Kratom Distro. “The law nonetheless recognizes that the defendant must pay something, however inadequate.”
The US Drug Enforcement Agency in 2016 had imposed its strictest restrictions on kratom, which is made from the leaves of an evergreen tree and is often used by people to self-treat pain, anxiety, depression, and opioid addiction as well as withdrawal. There was an intense, immediate public backlash to that approach, however, and it prompted the DEA to rescind its prohibition of kratom, which is sold in stores and online.
The US Food and Drug Administration nonetheless has warned consumers over possible safety and addiction risks associated with kratom, and it has spoken in favor of more research aimed at gaining a better understanding of “the substance and its components”.
Friends of Talavera, a resident of the Florida community of Boynton Beach, introduced her to kratom years before her death. Her family said she regarded it as a safe, natural supplement and had taken some after buying it online from the Kratom Distro when her partner and the father of her youngest child – Biagio Vultaggio – found her unconscious in the living room on 20 June 2021. The 39-year-old Talavera was face down on the ground next to an open bag of a kratom derivative marketed as a “space dust”, her family has said. Vultaggio called paramedics, and they took Talavera to a hospital where she was pronounced dead. An autopsy later listed Talavera’s cause of death as acute intoxication from mitragynine, the main kratom component. The local coroner wrote in a report that “at high concentrations, mitragynine produces opioid-like effects, such as respiratory failure”.
________________________
Kratom Disro claims that 
Product Consistency
- Our kratom powder is sourced directly from Indonesia monthly. Your order was literally on a farm in Indonesia two months ago. No old powder.
- Our kratom extracts are produced in the US by a licensed chemist and a professionally trained staff.
- We only use delicious flavors and quality ingredients.
Complete Transparency
- Every batch of products we receive is lab tested and will not ship out without meeting our meticulous quality standards.
- Current labs – We will never show you an out-of-date lab with our products.
- Guaranteed purity levels and free of all toxins.
Get It When You Want It
- Many orders shipped same day.
- USPS shipping on all orders under 6 pounds.
- Larger orders can ship USPS Priority for a small additional charge.
_________________________________
Back to the above lawsuit:
One of the attorneys for Talavera’s family, Tamara Williams, said in a statement that the judgment won by her clients “should be a wakeup call to the kratom industry”. Williams’s law firm had also recently won a $2.5m jury verdict against a kratom manufacturer in Washington state after a separate lawsuit alleging wrongful death. A colleague of Williams called on government officials to take steps “to protect other families from having to deal with unnecessary kratom overdose deaths”.
As we have recently discussed diet and its effects on health, it seems reasonable to ask whether there is a diet that is demonstrably healthy. A recent investigation attempted to answer this question.
This study was aimed at developing a healthy diet score that is associated with health outcomes and is globally applicable. It used data from the Prospective Urban Rural Epidemiology (PURE) study and tried to replicate it in five independent studies on a total of 245 000 people from 80 countries.
A healthy diet score was developed on the basis of the data from 147 642 people from the general population, from 21 countries in the PURE study. The consistency of the associations of the score with events was examined in five large independent studies from 70 countries.
The healthy diet score was developed based on six foods each of which has been associated with a significantly lower risk of mortality [i.e. fruit, vegetables, nuts, legumes, fish, and dairy (mainly whole-fat); range of scores, 0–6]. The main outcome measures were all-cause mortality and major cardiovascular events [cardiovascular disease (CVD)].
During a median follow-up of 9.3 years in PURE, compared with a diet score of ≤1 point, a diet score of ≥5 points was associated with a lower risk of:
- mortality [hazard ratio (HR) 0.70; 95% confidence interval (CI) 0.63–0.77)],
- CVD (HR 0.82; 0.75–0.91),
- myocardial infarction (HR 0.86; 0.75–0.99),
- stroke (HR 0.81; 0.71–0.93).
In three independent studies with vascular patients, similar results were found, with a higher diet score being associated with lower mortality (HR 0.73; 0.66–0.81), CVD (HR 0.79; 0.72–0.87), myocardial infarction (HR 0.85; 0.71–0.99), and a non-statistically significant lower risk of stroke (HR 0.87; 0.73–1.03). Additionally, in two case-control studies, a higher diet score was associated with lower first myocardial infarction [odds ratio (OR) 0.72; 0.65–0.80] and stroke (OR 0.57; 0.50–0.65). A higher diet score was associated with a significantly lower risk of death or CVD in regions with lower than with higher gross national incomes (P for heterogeneity <0.0001). The PURE score showed slightly stronger associations with death or CVD than several other common diet scores (P < 0.001 for each comparison).

The authors concluded that consumption of a diet comprised of higher amounts of fruits, vegetables, nuts, legumes, and a moderate amount of fish and whole-fat dairy is associated with a lower risk of CVD and mortality in all world regions, but especially in countries with lower income where consumption of these natural foods is low. Similar associations were found with the inclusion of meat or whole grain consumption in the diet score (in the ranges common in the six studies that we included). Our findings indicate that the risks of deaths and vascular events in adults globally are higher with inadequate intake of protective foods.
The authors rightly stress that their analyses have a number of limitations:
First, diet (as in most large epidemiologic studies) was self-reported and variations in reporting might lead to random errors that could dilute real associations between diet scores and clinical outcomes. Therefore, the beneficial effects of a healthier diet may be larger than estimated.
Second, the researchers did not examine the role of individual types of fruits and vegetables as components in the diet score, since the power to detect associations of the different types of fruits and vegetables vs. CVD or mortality is low (i.e. given that the number of events per type of fruit and vegetable was relatively low). Recent evidence suggests that bioactive compounds and, in particular, polyphenols which are found in certain fruit or vegetables (e.g. berries, spinach, and beans) may be especially protective against CVD.
Third, in observational studies, the possibility of residual confounding from unquantified or imprecise measurement of covariates cannot be ruled out—especially given that the differences in risk of clinical events are modest (∼10%–20% relative differences). Ideally, large randomized trials would be needed to clarify the clinical impact on events of a policy of proposing a dietary pattern in populations.
Fourth, the use of the median intake of each food component as a cut-off in the scoring scheme for each diet may not reflect the full range of consumption or provide a meaningful indicator of consumption associated with the disease. However, the use of quintiles instead of medians within each study or within each region yielded the same results indicating the robustness of our findings.
Fifth, the level of intake to meet the cut-off threshold for each food group in the diet score may differ between countries. However, in sensitivity analyses where region-specific median cut-offs were used to classify participants on each component of the diet score, the results were similar to using the overall cohort median of each food component. Further, with unprocessed red meat and whole grains included or excluded from the diet score in these sensitivity analyses, the results were again similar.
Sixth, misclassification of exposures cannot be ruled out as repeat measures of diet were not available in all studies. However, the ORIGIN study, in which repeat diet assessments at 2 years were conducted, showed similar results based on the first vs. second diet assessments. This indicates that misclassification of dietary intake during follow-up was not undermining the findings.
Seventh, one unique aspect of the study is the focus on only protective foods, i.e. a dietary pattern score that highlights what is missing from the food supply, especially in poorer world regions, but this does not negate the importance of limiting the consumption of harmful foods such as highly processed foods. While the PURE diet score had significantly stronger associations with events than other diet scores, the HRs were only slightly larger for PURE than for most other diet scores. However, the Planetary score was the least predictive of events. The analyses provide empirical evidence that all diet scores (other than the Planetary diet score) are of value to predicting death or CVD globally and in all regions of the world.
So, what should we, according to these findings, be looking for and how much of it should we consume? Here is the table that should answer these questions:
| Fruits and vegetables | 4 to 5 servings daily | 1 medium apple, banana, pear; 1 cup leafy vegs; 1/2 cup other vegs |
| Legumes | 3 to 4 servings weekly | 1/2 cup beans or lentils |
| Nuts | 7 servings weekly | 1 oz., tree nuts or peanuts |
| Fish | 2 to 3 servings weekly | 3 oz. cooked (pack of cards size) |
| Dairy | 14 servings weekly | 1 cup milk or yogurt; 1 ½ oz cheese |
| Whole grainsc | Moderate amounts (e.g. 1 serving daily) can be part of a healthy diet | 1 slice (40 g) bread; ½ medium (40 g) flatbread; ½ cup (75–120 g) cooked rice, barley, buckwheat, semolina, polenta, bulgur, or quinoa |
| Unprocessed meatsc | Moderate amounts (e.g. 1 serving daily) can be part of a healthy diet | 3 oz. cooked red meat or poultry |
Sobrenix (Kudzu, Milk Thistle, B Vitamins & More) is “designed to reduce alcohol cravings and help you detoxify your body so you can successfully manage alcohol consumption. Even better, taken before drinking, Sobrenix’s ingredients help you stop before you’ve had too much. DETOXIFY YOUR BODY with a powerful formula that combines herbs and nutrients that support liver health, curb cravings, and help you wake up without a nasty hangover. Sobrenix kick-starts the detoxification process with essential herbs like Milk Thistle and Chanca Piedra. Additionally, the formula contains the critical B-Vitamins that alcohol washes away so you can wake up happy and healthy again!”
Yes, you suspected correctly: this is pure BS!
Not only that but the Federal Trade Commission is taking action under the FTC Act and the Opioid Addiction Recovery Fraud Prevention Act of 2018 (OARFPA) against the makers of Sobrenix. According to the FTC’s complaint, the makers, a company, Rejuvica, and its owners, Kyle Armstrong and Kyle Dilger, made numerous unsubstantiated and false claims about Sobrenix and used paid endorsers in deceptively formatted advertising. The defendants also used bogus review sites to deceive consumers about their products.
As a result of the FTC’s suit, the defendants have agreed to a proposed court order that would permanently ban them from making any unsubstantiated claims about healthcare products or services, as well as require them to pay $650,000 to the FTC to be used for providing refunds to consumers.
“We will not tire in our pursuit of those who prey on individuals struggling with alcohol or other substance use disorders,” said Samuel Levine, Director of the Bureau of Consumer Protection. “This case evidences the breadth of the FTC’s authority to pursue such wrongdoing under both the FTC Act and OARFPA.”
The FTC charges that the defendants marketed Sobrenix with messages like:
- “STRUGGLING TO CONTROL YOUR ALCOHOL CONSUMPTION? Sobrenix is designed to reduce alcohol cravings and help you detoxify your body so you can successfully manage alcohol consumption. Even better, taken before drinking, Sobrenix’s ingredients help you stop before you’ve had too much.”
The FTC charges that Rejuvica and its owners lacked adequate evidence to support these claims. The complaint charges that Rejuvica, Armstrong, and Dilger violated both the FTC Act and OARFPA. The proposed order contains a total monetary judgment of $3,247,737, which is partially suspended based on the defendants’ inability to pay the full amount. The defendants will be required to pay $650,000 to the FTC to be used to refund consumers. If the defendants are found to have lied to the FTC about their financial status, the full judgment will be immediately due.
______________________________
A few short comments might be in order:
- Regulators have the duty to protect consumers from false health claims.
- It is commendable that some authorities sometimes do their duty and go after some of the people responsible for making false claims related to dietary supplements.
- Such actions should, however, occur MUCH more often.
- They ought to happen also in countries other than the US.
- Similar actions should be initiated against ALL false claims made for healthcare products and services.
- This means that all practitioners of so-called alternative medicine (SCAM) would need to review their advertising, websites, etc., and erase therapeutic claims that are not supported by evidence.
- This would unquestionably amount to an enormously valuable service to public health.
- Most countries already have legislation that would make such steps possible; my question, therefore, is this:
WHY ARE CONSUMERS NOT ADEQUATELY PROTECTED BY THEIR NATIONAL REGULATORS FROM CHARLATANS WHO SELL INEFFECTIVE AND OFTEN DANGEROUS SCAMs AT HIGH COSTS?
The website of the World Federation of Chiropractic (WFC) points out that public health is defined by the WHO as follows:
“Activities to strengthen public health capacities and service aim to provide conditions under which people can maintain to be healthy, improve their health and wellbeing, or prevent the deterioration of their health. Public health focuses on the entire spectrum of health and wellbeing, not only the eradication of particular diseases.”
The WFC then continues stating this:
As primary contact health professionals, chiropractors can play an important role as public health advocates. This can range from providing support and advice on health matters such as physical activity, diet, and fitness as well as lifestyle choices such as injury prevention and avoiding tobacco use. Chiropractors can also play a role in counselling patients and communities on the benefits of public health measures, especially as this relates to immediate health needs of each region.
I think that this might merit a few comments.
- Physical activity is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Diet is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Fitness is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Lifestyle choice is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Injury prevention is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Avoiding tobacco use is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Counseling is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
So, what is the real contribution of chiropractors to public health?
- Chiropractors tend to advise their clients against vaccinations.
- Some mislead the public by claiming they boost immunity and prevent serious infections.
- Many undermine evidence-based medicine by promoting obsolete myths such as ‘the innate’ or subluxations.
- Many sell supplements that could interact with prescription drugs.
- Many make bogus health claims for profit.
I would therefore argue that, on balance, the contribution of chiropractors to public health might be considerable …
sadly, however, it goes in the wrong direction.
Charles has a well-documented weakness for so-called alternative medicine (SCAM) – not just any SCAM but predominantly the type of SCAM that is both implausible and ineffective. Therefore, nobody can be all that surprised to read in THE TIMES that he has decided to use SCAM for helping women who have difficulties getting pregnant.

If one really wanted to employ SCAM for this aim one is spoilt for choice. In fact, there are only few SCAMs that don’t claim to be useful for this purpose.
A recent review, for instance, suggested that some supplements might be helpful. Other authors advocate SCAMs such as acupuncture, moxibustion, Chinese herbal medicine, psychological intervention, biosimilar electrical stimulation, homeopathy, or hyperbaric oxygen therapy.
Yes, I know! The evidence for these treatments is lousy, and I would never issue a recommendation based on such flimsy evidence.
Yet, the SCAM project at Dumfries House, the Scottish stately home Charles restored in 2007, offers acupuncture, reflexology, massage, yoga, and hypnotherapy for infertile women.
REFLEXOLOGY for female infertility?
Reflexology, also called zone therapy, is a manual treatment where pressure is applied usually to the sole of the patient’s foot and sometimes also to other areas such as the hands or ears. According to its proponents, foot reflexology is more than a simple foot massage that makes no therapeutic claims beyond relaxation. It is based on the idea that the human body is divided into 10 zones each of which is represented on the sole of the foot. Reflexologists employ maps of the sole of the foot where the body’s organs are depicted. By massaging specific zones which are assumed to be connected to specific organs, reflexologists believe to positively influence the function of these organs. While reflexology is mostly used as a therapy, some therapists also claim they can diagnose health problems through feeling tender or gritty areas on the sole of the foot which, they claim, correspond to specific organs.
Reflexology is not merely implausible as a treatment for infertility, it also boasts of some fairly rigorous trial evidence. A clinical trial (perhaps even the most rigorous of all the trials of SCAM for female fertility problems) testing whether foot reflexology might have a positive effect on the induction of ovulation stated that “the results suggest that any effect on ovulation would not be clinically relevant”.
So, as so often before in the realm of SCAM, Charles has demonstrated that his lack of critical thinking leads him to the least promising options.
Well done, Your Majesty!
As the organizer of several demos in the area of Linz, Austria, a ‘corona activist’ and ‘Holocaust denier’ had repeatedly made headlines over the past two years. Now the 39-year-old Austrian man is in the headlines yet again.
It has been reported that, on the evening of July 23, he was stopped by the police for a routine traffic control. His three children, aged 15, 11, and 5, were also in the car. “I know I’m wanted. I don’t have a driver’s license and I have a dead body in the trunk,” he said as he got out of the car. As the officers soon realized, he was only partly joking. A legal case for Holocaust denial was pending against the man who had not appeared at his main hearing last August, so a search was underway for him.
When police officers checked the car, they made the horrifying discovery. In the trunk was a woman’s body, wrapped in sheets. The dead woman turned out to be the wife, aged 38, of the driver. According to preliminary findings, she had died 4 hours earlier. Apparently, she had suffered from incurable cancer, and the police suspect that the illness had not been treated – her husband did not just not believe in vaccinations but disliked all drugs.
The husband, who already had several previous convictions, claimed that he was on his way to bury his wife somewhere “in nature”. The 39-year-old man was arrested and is now in pre-trial detention – though not for the incident with his wife’s body, but for Holocaust denial. He is said to have compared the Corona measures to the Holocaust, and the arrest order was issued because he failed to appear for his trial.
_________________________
One does not need to be a clairvoyant to predict that this remarkable man will come up with more surprises. I wonder what he might think of next.
Like ultra-processed food (UPF) itself, the subject of UPF is everywhere – radio, TV, Twitter, you name it, the topic crops up. I too could not resist writing a post on it a few months ago. And now I am publishing another one but one in a slightly more irritated mood.
Why do these endless discussions on UPF irritate me?
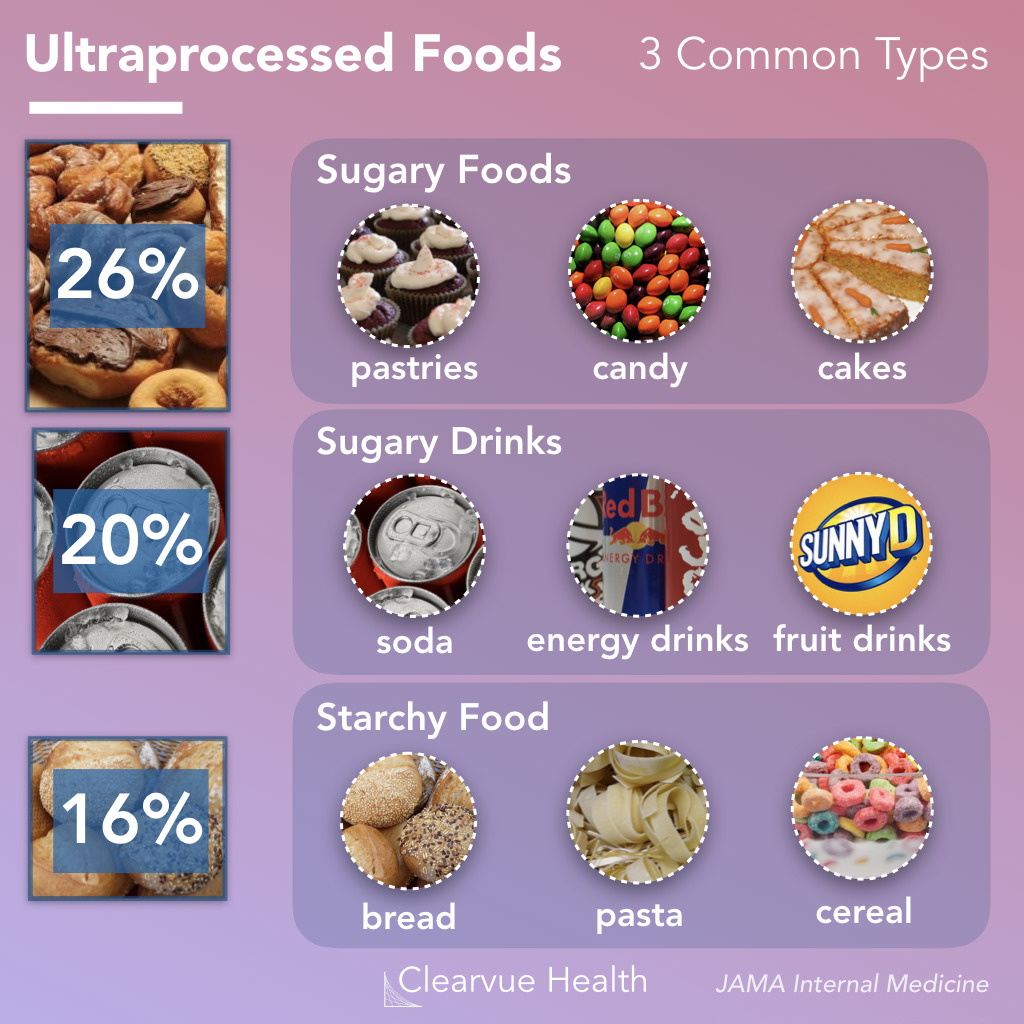
To start with, there is no uniform definition of UPF, and many commentators seem more than a little confused about what UPF actually is. One definition holds that Ultra-processed foods are foods that have been altered to include fats, starches, sugars, salts and hydrogenated oils extracted from other foods. They contain ingredients, additives, and preservatives that are not normally used in home cooking. It seems obvious that discussions on UPF without a clear and understandable definition of the term are merely generating confusion in the general public.
But there are, of course, lists of UPF that might render the subject a bit clearer. The trouble, however, is that these lists reveal disagreement among each other. Thus they are prone to generate even more confusion.
Next, there is the evidence – and there is lots of it. It suggests that the regular consumption of UPF is bad for virtually every aspect of health. And if there is no evidence that it is detrimental for a given condition, it probably is merely because nobody has yet bothered to do the analyses. The trouble is, however, that all the relevant research comes from either basic science or epidemiology. This means that causality is unproven.
A further problem is that even the experts don’t know what the alleged causal factors in UPF are.
- Is it the processing?
- The additives?
- The sugar?
- The fats?
- If so, which fats exactly?
- Is it perhaps a complex inter-play of some of these factors?
If we want to make progress, we need to know! If not, we cannot possibly begin to avoid the health-threatening effects of UPF.
The final and arguably biggest problem is that UPF is everywhere. Nobody living in an industrialized country and earning a regular living can avoid consuming UPF. This means, I fear, that all the current hype about UPF is not just irritating but possibly counter-productive.
Imagine an average person trying to make sense of these discussions. She would soon give up and conclude that all these ‘clever’ experts know nothing at all. Her foremost concern is to make ends meet. In the end, she will carry on as before. Alternatively, she might even conclude that, as the even experts do not make sense, UPF cannot be all that bad after all.
After reading about and listening to the arguments around UPF, I ask myself this: would it not be more productive to apply more common sense and focus on a few nutritional messages that are 1) solidly based on evidence and 2) an average person can actually follow?
Diabetic peripheral neuropathy (DPN) is a common complication of diabetes mellitus (DM) that can cause annoying symptoms. To address this condition, several treatment approaches have been proposed, including static magnetic field (SMF) therapy, which has shown promise in treating neurological conditions. Therefore, this study aimed to investigate the effects of SMF therapy on symptomatic DPN and the quality of life (QoL) in patients with type 2 diabetes.
A double-blind, randomized, placebo-controlled trial was conducted from April to October 2021. Sixty-four DPN patients (20 males, 44 females) were recruited for the study via invitation. The participants were divided into two groups: the magnet group, which used magnetic ankle bracelets (155 mT) for 12 weeks, and the sham group, which used non-magnetic ankle bracelets for the same duration. Neuropathy Symptom Score (NSS), Neuropathic Disability Score (NDS), and Visual Analogue Scale (VAS) were used to assess neuropathy symptoms and pain. In addition, the Neuropathy Specific Quality of Life Questionnaire (Neuro-QoL) tool was used to measure the patients’ quality of life.
Before treatment, there were no significant differences between the magnet and sham groups in terms of the NSS scores (P = 0.50), NDS scores (P = 0.74), VAS scores (P = 0.17), and Neuro-QoL scores (P = 0.82). However, after 12 weeks of treatment, the SMF exposure group showed a significant reduction in NSS scores (P < 0.001), NDS scores (P < 0.001), VAS scores (P < 0.001), and Neuro-QoL scores (P < 0.001) compared to the baseline. The changes in the sham group, on the other hand, were not significant.
The authors concluded that according to obtained data, SMF therapy is recommended as an easy-to-use and drug-free method for reducing DPN symptoms and improving QoL in diabetic type-2 patients.
Our own study and systematic review of the effects of magnetic bracelets and similar devices suggested that the effects of such treatments are due to placebo responses. Therefore, I find the findings of this new study most surprising. Not only that, to be honest, I also find them suspect. Apart from the fact that the treatment has no biological plausibility, I have three main reasons for my skepticism.
- The authors stated that there was no distinguishable difference between the sham and SMF devices in terms of their appearance, weight, or texture, which helped to ensure that the study was double-blinded. This is nonsense, I am afraid! The verum device is magnetic and the sham device is not. It is hardly conceivable that patients who handle such devices for any length of time do not discover this simple fact and thus de-blind themselves. In turn, this means that a placebo effect can easily explain the outcomes.
- Authors who feel that their tiny study of a highly implausible therapy lends itself to concluding that their therapy ‘is recommended as an easy-to-use and drug-free method for reducing DPN symptoms and improving QoL’ can, in my view, not be taken seriously.
- Something that always makes me suspicious of clinical trials is a lack of a placebo response where one would normally expect one. In this study, the control group exhibits hardly any placebo response. Wearing a strap around your ankle that allegedly emits therapeutic radiation would result in quite a strong placebo effect, according to our own findings.
So, forgive me if I do not trust this study any further than I can throw it! And pardon me if I still think that our previous conclusion is correct: The evidence does not support the use of static magnets for pain relief, and therefore magnets cannot be recommended as an effective treatment.
In a video, Mr.Darkmoore speaks from a hospital bed and says the cause behind his visit to the emergency room stemmed from a chiropractor’s work on him. Three days ago, he had a ringing in his ear due to a long-term condition he knew as tinnitus. Thus, he decided to visit a chiropractor. “I figured $100 to a chiro, let them adjust a few things, if all else fails, I’ll go to a doctor,” explains Darkmoore.
This $100 visit led to several other complications and doctor’s bills worth thousands of dollars. The day after he was treated by the chiropractor, he experienced a headache that eventually led to dizzy spells. He decided to visit the emergency room where a CT scan was ordered which showed that the chiropractor had dissected an artery in his neck.
Next, Darkmoore was put on blood thinners to avoid blood clots that could result in a stroke or worse. Darkmoore explains that he will be on two blood thinners for the next three months to prevent clotting. If the dissection heals partially, he says he will need to take aspirin every day for the rest of his life. If it doesn’t heal, he claims that he will need surgery.
Many viewers of the video claimed they have had the same “chiropractor gone wrong” experience as Darkmoore.
- “Wow. How scary. I had a similar thing happen to me. Extremely bad headache after going one time. Haven’t gone since,” one commenter wrote.
- “I’m so sorry this happened to u,” another user echoed. “My chiropractor also caused an injury which required emergency surgery & I have permanent damage. I’m glad u survived.”
Darkmore captioned his last update video, “I appreciate the thoughts and prayers. Hopefully, I’ll be okay after 3 months of recovery.”
__________________
Let’s hope that he is correct and that he will make a speedy and full recovery.
Of course, chiros will queue up to stress that important details are missing in this case report. To them, I would merely say this:
THERE IS NO GOOD EVIDENCE THAT NECK MANIPULATIONS BRING ANY BENEFIT AND QUITE A BIT OF EVIDENCE THAT THEY CAN CAUSE SERIOUS HARM.
SO, WHY NOT JUST STOP OFFERING THE PROCEDURE?
We have discussed dental amalgam and its risks to human health before. Finally, there is new legislation in sight. The European Commission has revised the EU Mercury Regulation to protect EU citizens and the environment from toxic mercury. Among other things, this will completely ban the use of dental amalgam, for which 40 tons of mercury are currently consumed annually in the EU. The revised mercury ordinance provides for the following:
– No more use of dental amalgam from January 1, 2025; viable mercury-free alternatives are available.
– Ban on the manufacture and export of dental amalgam from the EU from January 1, 2025;
– Ban on the manufacture and export of six mercury-containing lamps from January 1, 2026 and January 1, 2028 (depending on lamp type).
The delegated act adopted under the Mercury Regulation transposes into EU law the decisions taken at the fourth Conference of the Parties (2022) to the Minamata Convention by introducing a ban on the production, import, and export of eight additional mercury-containing products, including mercury-containing lamps and non-electrical equipment.
The Minamata Convention is the main international legal framework for the protection of human health and the environment from anthropogenic emissions and releases of mercury to air, water, and soil. Like the Mercury Regulation, it addresses the entire life cycle of mercury, from primary mercury mining to mercury waste management.
The revised Mercury Regulation must now be approved by the European Parliament and the Council under the ordinary legislative procedure. The delegated act will be sent to the European Parliament and the Council for consideration.
Mercury is a highly toxic chemical that poses a threat to both human health and the environment. When released into the environment, it enters the food chain where it accumulates (mainly in fish). High mercury exposure can damage the brain, lungs, kidneys, and immune system.
Historically, mercury has been used in a wide range of applications, including gold mining, batteries, fluorescent tubes, thermometers, and barometers. Over the last twenty years, the EU has developed a comprehensive body of legislation, in particular the Mercury Regulation, which protects human health and the environment from anthropogenic emissions and releases of mercury, taking into account the entire life cycle of mercury from primary mercury mining to final disposal of mercury waste. It also includes measures on trade in mercury-containing products and mercury pollution.
The Minamata Convention entered into force on August 16, 2017, and has so far been ratified by the European Union and 143 countries, including all EU Member States. The fifth session of the Conference of the Parties to the Minamata Convention on Mercury (COP-5) will be held in Geneva, Switzerland, from October 30 to November 3, 2023.
_____________________________