Monthly Archives: February 2019
Collagen is a fibrillar protein of the conjunctive and connective tissues in the human body, essentially skin, joints, and bones. Due to its abundance in our bodies, its strength and its relation with skin aging, collagen has gained great interest as an oral dietary supplement as well as an ingredient in cosmetics. Collagen fibres get damaged with the pass of time, losing thickness and strength which has been linked to skin aging phenomena. Collagen can be obtained from natural sources such as plants and animals or by recombinant protein production systems. Because of its increased use, the collagen market is worth billions. The question therefore arises: is it worth it?
This 2019 systematic review assessed all available randomized-controlled trials using collagen supplementation for treatment efficacy regarding skin quality, anti-aging benefits, and potential application in medical dermatology. Eleven studies with a total of 805 patients were included. Eight studies used collagen hydrolysate, 2.5g/d to 10g/d, for 8 to 24 weeks, for the treatment of pressure ulcers, xerosis, skin aging, and cellulite. Two studies used collagen tripeptide, 3g/d for 4 to 12 weeks, with notable improvement in skin elasticity and hydration. Lastly, one study using collagen dipeptide suggested anti-aging efficacy is proportionate to collagen dipeptide content.
The authors concluded that preliminary results are promising for the short and long-term use of oral collagen supplements for wound healing and skin aging. Oral collagen supplements also increase skin elasticity, hydration, and dermal collagen density. Collagen supplementation is generally safe with no reported adverse events. Further studies are needed to elucidate medical use in skin barrier diseases such as atopic dermatitis and to determine optimal dosing regimens.
These conclusions are similar to those of a similar but smaller review of 2015 which concluded that the oral supplementation with collagen peptides is efficacious to improve hallmarks of skin aging.
And what about the many other claims that are currently being made for oral collagen?
A 2006 review of collagen for osteoarthritis concluded that a growing body of evidence provides a rationale for the use of collagen hydrolysate for patients with OA. It is hoped that ongoing and future research will clarify how collagen hydrolysate provides its clinical effects and determine which populations are most appropriate for treatment with this supplement. For other indication, the evidence seems less conclusive.
So, what should we make of this collective evidence. My interpretation is that, of course, there are caveats. For instance, most studies are small and not as rigorous as one would hope. But the existing evidence is nevertheless intriguing (and much more compelling than that for most other supplements). Moreover, there seem to be very few adverse effects with oral usage (don’t inject the stuff for cosmetic purposes, as often recommended!). Therefore, I feel that collagen might be one of the few dietary supplements worth keeping an eye on.
Osteopathic visceral manipulation (OVM) have been our subject several times before. The method has been developed by the French Osteopath and Physical Therapist Jean-Pierre Barral. According to uncounted Internet-sites, books and other promotional literature, OVM is a miracle cure for just about every disease imaginable. Most of us hearing such claims hear alarm bells ringing – rightly so, I think. The evidence for OVM is thin, to put it mildly. But now, there is a new study to consider.
Brazilian researchers designed a placebo-controlled study using placebo visceral manipulation as the control to evaluate the effect of OVM of the stomach and liver on pain, cervical mobility, and electromyographic activity of the upper trapezius (UT) muscle in individuals with nonspecific neck pain (NS-NP) and functional dyspepsia. Twenty-eight NS-NP patients were randomly assigned into two groups: treated with OVM (OVMG; n = 14) and treated with placebo visceral manipulation (PVMG; n = 14). The effects were evaluated immediately and 7 days after treatment through pain, cervical range, and electromyographic activity of the UT muscle.
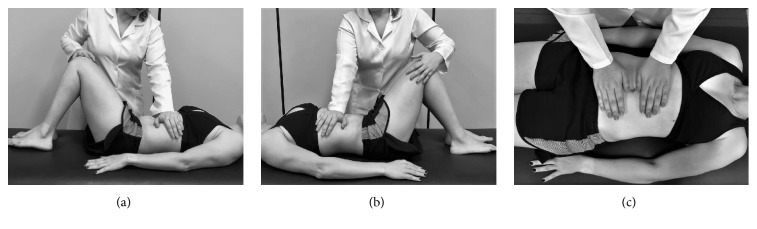
Visceral manipulation techniques for stomach (a), liver (b), and placebo technique (c).
Significant effects were confirmed immediately after treatment (OVMG and PVMG) for numeric rating scale scores and pain area. Significant increases in EMG amplitude were identified immediately and 7 days after treatment for the OVMG. No differences were identified between the OVMG and the PVMG for cervical range of motion.
The authors concluded that the results of this pilot study indicate that a single session of osteopathic visceral manipulation for the stomach and liver reduces cervical pain and increases the amplitude of the upper trapezius muscle EMG signal immediately and 7 days after treatment in patients with nonspecific neck pain and functional dyspepsia. Patients treated with placebo visceral mobilisation reported a significant decrease in pain immediately after treatment. The effect of this intervention on the cervical range of motion was inconclusive. The results of this study suggest that further investigation is necessary.
There are numerous problems with this study:
- The authors call it a pilot study. Such a trial is for exploring the feasibility of a proper study. With the introduction of a placebo-OVM, this would make sense. The relevant question would then be: is the placebo valid and indistinguishable from the real thing? Sadly, this issue is not even addressed in the trial.
- A pilot study certainly is not for evaluating the effectiveness of an intervention. Sadly, this is precisely what the authors used it for. The label ‘pilot’, it seems, was merely given to excuse the many methodological flaws of their trial.
- For an evaluation of treatment effects, the study was far too small. This means the reported results can be discarded as meaningless.
- If we nevertheless took them seriously, we would want to explain how the findings were generated. The authors believe that they were caused by OVM. I find this most unlikely.
- The more plausible explanation would be that patient-blinding was unsuccessful. In other words, the placebo is not indistinguishable from the real OVM. Looking at the pictures above, one can easily see that the patients were able to tell to which group they had been allocated.
- The failure to blind patients (and, of course, the therapists), in turn, would mean that the verum group were better motivated to out-perform the placebo group in the outcome measures.
- Finally, I disagree with the authors’ view that the results of this study suggest that further investigation is necessary. On the contrary, I think that any further investment into OVM is ill-advised.
My conclusion: OVM is an implausible, non-evidence-based SCAM, and dodgy science is not going to make it look any more convincing.
Excellent journals always publish excellent science!
If this is what you believe, you might want to read a study of chiropractic just published in the highly respected SCIENTIFIC REPORTS.
The objective of this study was to investigate whether a single session of chiropractic care could increase strength in weak plantar flexor muscles in chronic stroke patients. Maximum voluntary contractions (strength) of the plantar flexors, soleus evoked V-waves (cortical drive), and H-reflexes were recorded in 12 chronic stroke patients, with plantar flexor muscle weakness, using a randomized controlled crossover design. Outcomes were assessed pre and post a chiropractic care intervention and a passive movement control. Repeated measures ANOVA was used to asses within and between group differences. Significance was set at p < 0.05. Following the chiropractic care intervention there was a significant increase in strength (F (1,11) = 14.49, p = 0.002; avg 64.2 ± 77.7%) and V-wave/Mmax ratio (F(1,11) = 9.67, p = 0.009; avg 54.0 ± 65.2%) compared to the control intervention. There was a significant strength decrease of 26.4 ± 15.5% (p = 0.001) after the control intervention. There were no other significant differences. Plantar flexor muscle strength increased in chronic stroke patients after a single session of chiropractic care. An increase in V-wave amplitude combined with no significant changes in H-reflex parameters suggests this increased strength is likely modulated at a supraspinal level. Further research is required to investigate the longer term and potential functional effects of chiropractic care in stroke recovery.
In the article we find the following further statements (quotes in bold, followed by my comments in normal print):
- Data were collected by a team of researchers from the Centre for Chiropractic Research at the New Zealand College of Chiropractic. These researchers can be assumed to be highly motivated in generating a positive finding.
- The entire spine and both sacroiliac joints were assessed for vertebral subluxations, and chiropractic adjustments were given where deemed necessary, by a New Zealand registered chiropractor. As there is now near-general agreement that such subluxations are a myth, the researchers treated a non-existing entity.
- The chiropractor did not contact on a segment deemed to be subluxated during the control set-up and no adjustive thrusts were applied during any control intervention. The patients therefore were clearly able to tell the difference between real and control treatments. Participants were not checked for blinding success.
- Maximum isometric plantarflexion force was measured using an isometric strain gauge. Such measurements crucially depend on the motivation of the patient.
- The grant proposal for this study was reviewed by the Australian Spinal Research Foundation to support facilitation of funding from the United Chiropractic Association. Does this not mean the researchers had a conflict of interest?
- The authors declare no competing interests. Really? They were ardent subluxationists supported by the United Chiropractic Association, an organisation stating that chiropractic is concerned with the preservation and restoration of health, and focuses particular attention on the subluxation, and subscribes to to the obsolete concept of vitalism: we ascribe to the idea that all living organisms are sustained by an innate intelligence, which is both different from and greater than physical and chemical forces. Further, we believe innate intelligence is an expression of universal intelligence.
So, in essence, what we have here is an under-powered study sponsored by vitalists and conducted by subluxationists treating a mythical entity with dubious interventions without controlling for patients’ expectation pretending their false-positive findings are meaningful.
I cannot help wondering what possessed the SCIENTIFIC REPORTS to publish such poor science.
So-called alternative medicine (SCAM) for animals is popular. A recent survey suggested that 76% of US dog and cat owners use some form of SCAM. Another survey showed that about one quarter of all US veterinary medical schools run educational programs in SCAM. Amazon currently offers more that 4000 books on the subject.
The range of SCAMs advocated for use in animals is huge and similar to that promoted for use in humans; the most commonly employed practices seem to include acupuncture, chiropractic, energy healing, homeopathy (as discussed in the previous post) and dietary supplements. In this article, I will briefly discuss the remaining 4 categories.
ACUPUNCTURE
Acupuncture is the insertion of needles at acupuncture points on the skin for therapeutic purposes. Many acupuncturists claim that, because it is over 2 000 years old, acupuncture has ‘stood the test of time’ and its long history proves acupuncture’s efficacy and safety. However, a long history of usage proves very little and might even just demonstrate that acupuncture is based on the pre-scientific myths that dominated our ancient past.
There are many different forms of acupuncture. Acupuncture points can allegedly be stimulated not just by inserting needles (the most common way) but also with heat, electrical currents, ultrasound, pressure, bee-stings, injections, light, colour, etc. Then there is body acupuncture, ear acupuncture and even tongue acupuncture. Traditional Chinese acupuncture is based on the Taoist philosophy of the balance between two life-forces, ‘yin and yang’. In contrast, medical acupuncturists tend to cite neurophysiological theories as to how acupuncture might work; even though some of these may appear plausible, they nevertheless are mere theories and constitute no proof for acupuncture’s validity.
The therapeutic claims made for acupuncture are legion. According to the traditional view, acupuncture is useful for virtually every condition. According to ‘Western’ acupuncturists, acupuncture is effective mostly for chronic pain. Acupuncture has, for instance, been used to improve mobility in dogs with musculoskeletal pain, to relieve pain associated with cervical neurological disease in dogs, for respiratory resuscitation of new-born kittens, and for treatment of certain immune-mediated disorders in small animals.
While the use of acupuncture seems to gain popularity, the evidence fails to support this. Our systematic review of acupuncture (to the best of my knowledge the only one on the subject) in animals included 14 randomized controlled trials and 17 non-randomized controlled studies. The methodologic quality of these trials was variable but, on average, it was low. For cutaneous pain and diarrhoea, encouraging evidence emerged that might warrant further investigation. Single studies reported some positive inter-group differences for spinal cord injury, Cushing’s syndrome, lung function, hepatitis, and rumen acidosis. However, these trials require independent replication. We concluded that, overall, there is no compelling evidence to recommend or reject acupuncture for any condition in domestic animals. Some encouraging data do exist that warrant further investigation in independent rigorous trials.
Serious complications of acupuncture are on record and have repeatedly been discussed on this blog: acupuncture needles can, for instance, injure vital organs like the lungs or the heart, and they can introduce infections into the body, e. g. hepatitis. About 100 human fatalities after acupuncture have been reported in the medical literature – a figure which, due to lack of a monitoring system, may disclose just the tip of an iceberg. Information on adverse effects of acupuncture in animals is currently not available.
Given that there is no good evidence that acupuncture works in animals, the risk/benefit balance of acupuncture cannot be positive.
CHIROPRACTIC
Chiropractic was created by D D Palmer (1845-1913), an American magnetic healer who, in 1895, manipulated the neck of a deaf janitor, allegedly curing his deafness. Chiropractic was initially promoted as a cure-all by Palmer who claimed that 95% of diseases were due to subluxations of spinal joints. Subluxations became the cornerstone of chiropractic ‘philosophy’, and chiropractors who adhere to Palmer’s gospel diagnose subluxation in nearly 100% of the population – even in individuals who are completely disease and symptom-free. Yet subluxations, as understood by chiropractors, do not exist.
There is no good evidence that chiropractic spinal manipulation might be effective for animals. A review of the evidence for different forms of manual therapies for managing acute or chronic pain syndromes in horses concluded that further research is needed to assess the efficacy of specific manual therapy techniques and their contribution to multimodal protocols for managing specific somatic pain conditions in horses. For other animal species or other health conditions, the evidence is even less convincing.
In humans, spinal manipulation is associated with serious complications (regularly discussed in previous posts), usually caused by neck manipulation damaging the vertebral artery resulting in a stroke and even death. Several hundred such cases have been documented in the medical literature – but, as there is no system in place to monitor such events, the true figure is almost certainly much larger. To the best of my knowledge, similar events have not been reported in animals.
Since there is no good evidence that chiropractic spinal manipulations work in animals, the risk/benefit balance of chiropractic fails to be positive.
ENERGY HEALING
Energy healing is an umbrella term for a range of paranormal healing practices, e. g. Reiki, Therapeutic Touch, Johrei healing, faith healing. Their common denominator is the belief in an ‘energy’ that can be used for therapeutic purposes. Forms of energy healing have existed in many ancient cultures. The ‘New Age’ movement has brought about a revival of these ideas, and today ‘energy’ healing systems are amongst the most popular alternative therapies in many countries.
Energy healing relies on the esoteric belief in some form of ‘energy’ which refers to some life force such as chi in Traditional Chinese Medicine, or prana in Ayurvedic medicine. Some proponents employ terminology from quantum physics and other ‘cutting-edge’ science to give their treatments a scientific flair which, upon closer scrutiny, turns out to be little more than a veneer of pseudo-science.
Considering its implausibility, energy healing has attracted a surprisingly high level of research activity in the form of clinical trials on human patients. Generally speaking, the methodologically best trials of energy healing fail to demonstrate that it generates effects beyond placebo. There are few studies of energy healing in animals, and those that are available are frequently less than rigorous (see for instance here and here). Overall, there is no good evidence to suggest that ‘energy’ healing is effective in animals.
Even though energy healing is per se harmless, it can do untold damage, not least because it can lead to neglect of effective treatments and it undermines rationality in our societies. Its risk/benefit balance therefore fails to be positive.
DIETARY SUPPLEMENTS
Dietary supplements for veterinary use form a category of remedies that, in most countries, is a regulatory grey area. Supplements can contain all sorts of ingredients, from minerals and vitamins to plants and synthetic substances. Therefore, generalisations across all types of supplements are impossible. The therapeutic claims that are being made for supplements are numerous and often unsubstantiated. Although they are usually promoted as natural and safe, dietary supplements do not have necessarily either of these qualities. For example, in the following situations, supplements can be harmful:
- Combining one supplement with another supplement or with prescribed medicines
- Substituting supplements for prescription medicines
- Overdosing some supplements, such as vitamin A, vitamin D, or iron
Examples of currently most popular supplements for use in animals include chondroitin, glucosamine, probiotics, vitamins, minerals, lutein, L-carnitine, taurine, amino acids, enzymes, St John’s wort, evening primrose oil, garlic and many other herbal remedies. For many supplements taken orally, the bioavailability might be low. There is a paucity of studies testing the efficacy of dietary supplements in animals. Three recent exceptions (all of which require independent replication) are:
- A trial showing that the dietary supplementation with Maca increased sperm production in stallions.
- A study demonstrating that curcumin supplementation appeared to reduce arthritis pain in dogs.
- An investigation suggesting that royal jelly supplementation can improve the egg quality of hens.
Dietary supplements are promoted as being free of direct risks. On closer inspection, this notion turns out to be little more than an advertising slogan. As discussed repeatedly on this blog, some supplements contain toxic materials, contaminants or adulterants and thus have the potential to do harm. A report rightly concluded that many challenges stand in the way of determining whether or not animal dietary supplements are safe and at what dosage. Supplements considered safe in humans and other cross-species are not always safe in horses, dogs, and cats. An adverse event reporting system is badly needed. And finally, regulations dealing with animal dietary supplements are in disarray. Clear and precise regulations are needed to allow only safe dietary supplements on the market.
It is impossible to generalise about the risk/benefit balance of dietary supplements; however, caution is advisable.
CONCLUSION
SCAM for animals is an important subject, not least because of the current popularity of many treatments that fall under this umbrella. For most therapies, the evidence is woefully incomplete. This means that most SCAMs are unproven. Arguably, it is unethical to use unproven medicines in routine veterinary care.
PS
I was invited several months ago to write this article for VETERINARY RECORD. It was submitted to peer review and subsequently I withdrew my submission. The above post is a slightly revised version of the original (in which I used the term ‘alternative medicine’ rather than ‘SCAM’) which also included a section on homeopathy (see my previous post). The reason for the decision to withdraw this article was the following comment by the managing editor of VETERINARY RECORD: A good number of vets use these therapies and a more balanced view that still sets out their efficacy (or otherwise) would be more useful for the readership.
Ever since Samuel Hahnemann, the German physician who invented homeopathy, gave a lecture on the subject in the mid-1810s, homeopathy has been used for treating animals. Initially, veterinary medical schools tended to reject homoeopathy as implausible, and the number of veterinary homeopaths remained small. In the 1920ies, however, veterinary homoeopathy was revived in Germany, and in 1936, members of the “Studiengemeinschaft für tierärztliche Homöopathie” (Study Group for Veterinary Homoeopathy) started to investigate homeopathy systematically.
Today, veterinary homeopathy is popular not least because of the general boom in so-called alternative medicine (SCAM). Prince Charles is just one of many prominent advocates who claims to treat animals with homeopathy. In many countries, veterinary homeopaths have their own professional organisations, while elsewhere veterinarians are banned from practicing homeopathy. In the UK, only veterinarians are currently allowed to use homeopathy on animals (but ironically, anyone regardless of background can use it on human patients).
Considering the implausibility of its assumptions, it seems unlikely that homeopathic remedies can be anything other than placebos. Yet homeopaths and their followers regularly produce clinical trials that seem to suggest efficacy. Today, there are about 500 controlled clinical trials of homeopathy (mostly on humans), and it is no surprise that, purely by chance, some of them show positive results. To avoid being misled by random findings, cherry-picking, or flawed science, we ought to critically evaluate the totality of the available evidence. In other words, we should rely not on single studies but on systematic reviews of all reliable trials.
A 2015 systematic review by ardent homeopaths tested the hypothesis that the outcome of veterinary homeopathic treatments is distinguishable from placebos. A total of 15 trials could be included, but only two comprised reliable evidence without overt vested interest. The authors concluded that there is “very limited evidence that clinical intervention in animals using homeopathic medicines is distinguishable from corresponding intervention using placebos.”
A more recent systematic review compared the efficacy of homeopathy to that of antibiotics in cattle, pigs and poultry. A total number of 52 trials were included of which 28 were in favour of homeopathy and 22 showed no effect. No study had been independently replicated. The authors concluded that “the use of homeopathy cannot claim to have sufficient prognostic validity where efficacy is concerned.”
Discussing this somewhat unclear and contradictory findings of trials of homeopathy for animals, Lee et al concluded that “…it is overwhelmingly likely that small effects observed in the RCTs and systematic reviews are the result of residual bias in the trials.” To this, I might add that ‘publication bias’, i. e. the phenomenon that negative trials often remain unpublished, might be the reason why systematic reviews of homeopathy are never entirely negative.
In recent years, several scientific bodies have assessed the evidence on homeopathy and published statements about it. Here are the key passages from some of these ‘official verdicts’:
“The principles of homeopathy contradict known chemical, physical and biological laws and persuasive scientific trials proving its effectiveness are not available”
Russian Academy of Sciences, Russia
“Homeopathy should not be used to treat health conditions that are chronic, serious, or could become serious. People who choose homeopathy may put their health at risk if they reject or delay treatments for which there is good evidence for safety and effectiveness.”
National Health and Medical Research Council, Australia
“These products are not supported by scientific evidence.”
Health Canada, Canada
“Homeopathic remedies don’t meet the criteria of evidence-based medicine.”
Hungarian Academy of Sciences, Hungary
“The incorporation of anthroposophical and homeopathic products in the Swedish directive on medicinal products would run counter to several of the fundamental principles regarding medicinal products and evidence-based medicine.”
Swedish Academy of Sciences, Sweden
“There is little evidence to support homeopathy as an effective treatment for any specific condition”
National Centre for Complementary and Integrative Health, USA
“There is no good-quality evidence that homeopathy is effective as a treatment for any health condition”
 National Health Service, UK
National Health Service, UK
“Homeopathic remedies perform no better than placebos, and the principles on which homeopathy is based are “scientifically implausible””
House of Commons Science and Technology Committee, UK
“Homeopathy has not definitively proven its efficacy in any specific indication or clinical situation.”
Ministry of Health, Spain
“… homeopathy should be treated as one of the unscientific methods of the so called ‘alternative medicine’, which proposes worthless products without scientifically proven efficacy.”
National Medical Council, Poland
“… there is no valid empirical proof of the efficacy of homeopathy beyond the placebo effect.”
Federaal Kenniscentrum voor de Gezondheidszorg, Belgium
As they are usually far too dilute to contain anything, homeopathic remedies are generally harmless, provided they are produced according to good manufacturing practice (which is not always the case). Unfortunately, however, this harmlessness does not necessarily apply to homeopathy in general. When employed to replace an effective therapy, even the most innocent but ineffective treatment can become life-threatening. Since homeopaths recommend their remedies for even the most serious conditions, this is by no means a theoretical consideration. I have therefore often stated that HOMEOPATHICS MIGHT BE HARMLESS, BUT HOMEOPATHS CERTAINLY ARE NOT.
It follows that an independent risk/benefit analysis of homeopathy fails to arrive at a positive conclusion. In other words, homeopathy has not been shown to generate more good than harm. In turn, this means that homeopathy has no place in veterinary (or human) evidence-based medicine.
Determined to cover as many so-called alternative medicines (SCAMs) as I possibly can, I was intrigued to see an article in the EVENING STANDARD about a SCAM I had not been familiar with: YANG SHENG.
Here is an excerpt of this article:
When people meet Katie Brindle, they usually ask whether she does acupuncture. “In fact, I specialise in yang sheng,” she says, a sigh in her voice. “It’s a massive aspect of Chinese medicine that no one knows anything about.” She’s on a mission to change that. Yang sheng is, in simplest terms, “prevention not cure” and Brindle puts it into practice with Hayo’u, her part-beauty brand, part-wellness programme, which draws on rituals in Far Eastern medicine. The “Reset” ritual, for example, is based on the Chinese martial art of qigong and involves shaking, drumming and twisting the body to wake up your circulation — Brindle says it stimulates digestion and boosts immunity. The “Body Restorer”, a gentle massage of the neck, chest and back, has a history of being used as a form of treatment for fever, muscle pain, inflammation and migraines. The principle underpinning all the practices is that small changes in your daily routine can help prevent your body from illness. Brindle wants it to be accessible: the website is free, and she is planning Facebook live-streams later in the year. There will also be a book in April, focusing on prevention rather than cure…
Frustrated about the overtly adversorial nature of this article, I did a few searches (not made easy by the fact that Yang and Sheng are common names of authors and yangsheng is the name of an acupuncture point) and found that Yang Sheng is said to be a health-promoting method in Traditional Chinese Medicine (TCM) that includes movement, mental exercise, and breathing technique. It is used mainly in China but has apparently it is currently enjoying an ever-widening acceptance in the Western world as well.
Is there any evidence for it?
Good question!
A paper from 1998 reported an observational study with 30 asthma patients, with varying degrees of illness severity. They were taught Qigong Yangsheng under medical supervision and asked to exercise independently, if possible, on a daily basis. They kept a diary of their symptoms for half a year including peak-flow measurements three times daily, use of medication, frequency and length of exercise as well as five asthma-relevant symptoms (sleeping through the night, coughing, expectoration, dyspnea, and general well-being). A decrease of at least 10 percent in peak-flow variability between the 1st and the 52nd week occurred more frequently in the group of the exercisers (n = 17) than in the group of non-exercisers (n = 13). When comparing the study year with the year before the study, there was improvement also in reduced hospitalization rate, less sickness leave, reduced antibiotic use and fewer emergency consultations resulting in reduced treatment costs. The authors concluded that Qigong Yangsheng is recommended for asthma patients with professional supervision. An improvement in airway capability and a decrease in illness severity can be achieved by regular self-conducted Qigong exercises.
The flaws of this study are obvious, and I don’t even bother to criticise it here.
Unfortunately, that was the only ‘study’ I found.
I also located many websites most of which are all but useless. Here is one that offers some explanations:
Yang sheng is a self-care approach. What makes this any different from all those other wellbeing manuals? The short answer is, that this is advice rooted in thousands of years of wisdom. Texts on how to preserve and extend life, health and wellbeing have been part of the Chinese tradition since the 4thcentury BC. They’ve had over 25 centuries to be refined and are time tested.
Yang sheng takes into account core theories like yin and yang, adhering to the laws of nature and harmonious free flow of Qi around the body (see below). As the active pursuit of the best possible functioning and balance of the whole self – body, mind and spirit. Yang Sheng takes into consideration your relationships to people and the environment.
In the West, we systematically neglect wellness and disease prevention. We take our good health for granted. We assume that we cannot avoid disease. And then when we are ill, we treat the symptoms of disease rather than finding the root cause.
Yang Sheng is about discovering energy imbalances long before they turn into overt disease. It works on the approach of eliminating small health niggles and balancing the body to stay healthy.
If this sounds like a conspiracy of BS to you, I would not blame you.
So, what can we conclude from this? I think, it is fair to say that:
- Yang Sheng is being promoted as yet another TCM miracle.
- It is based on all the obsolete nonsense that TCM has to offer.
- Numerous therapeutic and preventative claims are being made for it.
- None of them is supported by anything resembling good evidence.
- Anyone with a serious condition who trusts Yang Sheng advocates puts her/his life in danger.
- The EVENING STANDARD is not a source for reliable medical information.
I don’t expect many of my readers to be surprised, concerned or alarmed by any of this. In my view, however, this lack of alarm is exactly what is alarming! We have become so used to seeing bogus claims and dangerous BS in the realm of SCAM that abnormality has gradually turned into something close to normality.
I find the type of normality that incessantly misleads consumers and endangers patients quite simply unacceptable.
Pertussis (whooping-cough) is a serious condition. Today, we have vaccinations and antibiotics against it and therefore it is rarely a fatal disease. A century or so, the situation was different. Then all sorts of quacks claimed to be able to treat pertussis and many patients, particularly children, died.
This article starts with this amazing introduction: Osteopathic physicians may want to consider using osteopathic manipulative treatment (OMT) as an adjunctive treatment modality for pertussis; however, suitable OMT techniques are not specified in the research literature.
For the paper, the author then searched the historical osteopathic literature to identify OMT techniques that were used in the management of pertussis in the pre-antibiotic era. The 24 identified sources included 8 articles and 16 book contributions from the years 1886 to 1958. Most sources were published within the first quarter of the 20th century. Commonly identified OMT techniques included mobilization techniques, lymphatic pump techniques, and other manipulative techniques predominantly in the cervical and thoracic regions.
The author concluded that the wealth of OMT techniques for patients with pertussis that were identified suggests that pertussis was commonly treated by early osteopaths. Further research is necessary to identify or establish the evidence base for these techniques so that in case of favorable outcomes, their use by osteopathic physicians is justified as adjunctive modalities when encountering a patient with pertussis.
I found it hard to decide whether to laugh or to cry after reading this. One could easily have a good giggle about the silliness of the idea to revive obsolete techniques for treating a potentially serious infection. One the other hand, I cannot help but ask myself:
- Is there any suggestion at all that OMT was successful in treating pertussis?
- If the answer is negative (and I fear it is), why would anyone spend considerable resources to establish the evidence base for these techniques?
- Do osteopaths believe in progress at all?
- Do they really think that there is even a remote chance that mobilization techniques, lymphatic pump techniques, and other manipulative techniques will, one day, come back as adjunctive therapies for pertussis?
- Do they not believe in a rational approach to prioritising medical research such that scarce resources are spent ethically and wisely?
You may think that none of this really matters. The author of this paper is just a lone loon! That may well be so, but even lone loons can do a lot of harm, if they convince consumers of their bizarre ideas.
But surely, the profession of osteopathy would not tolerate this, you say. I am not convinced. The article was published in the Journal of the American Osteopathic Association. This seems significant to me. It is comparable to the JAMA or the BMJ publishing an article calling for a programme of research into the possible benefits of blood-letting as a treatment of pneumonia!
Acupuncture is all over the news today. The reason is a study just out in BMJ-Open.
The aim of this new RCT was to investigate the efficacy of a standardised brief acupuncture approach for women with moderate-tosevere menopausal symptoms. Nine Danish primary care practices recruited 70 women with moderate-to-severe menopausal symptoms. Nine general practitioners with accredited education in acupuncture administered the treatments.
The acupuncture style was western medical with a standardised approach in the pre-defined acupuncture points CV-3, CV-4, LR-8, SP-6 and SP-9. The intervention group received one treatment for five consecutive weeks. The control group received no acupuncture but was offered treatment after 6 weeks. Outcomes were the differences between the two groups in changes to mean scores using the scales in the MenoScores Questionnaire, measured from baseline to week 6. The primary outcome was the hot flushes scale; the secondary outcomes were the other scales in the questionnaire. All analyses were based on intention-to-treat analysis.
Thirty-six patients received the intervention, and 34 were in the control group. Four participants dropped out before week 6. The acupuncture intervention significantly decreased hot flushes, day-and-night sweats, general sweating, menopausal-specific sleeping problems, emotional symptoms, physical symptoms and skin and hair symptoms compared with the control group at the 6-week follow-up. The pattern of decrease in hot flushes, emotional symptoms, skin and hair symptoms was already apparent three weeks into the study. Mild potential adverse effects were reported by four participants, but no severe adverse effects were reported.
The authors concluded that the standardised and brief acupuncture treatment produced a fast and clinically relevant reduction in moderate-to-severe menopausal symptoms during the six-week intervention.
The only thing that I find amazing here is the fact the a reputable journal published such a flawed trial arriving at such misleading conclusions.
- The authors call it a ‘pragmatic’ trial. Yet it excluded far too many patients to realistically qualify for this characterisation.
- The trial had no adequate control group, i.e. one that can account for placebo effects. Thus the observed outcomes are entirely in keeping with the powerful placebo effect that acupuncture undeniably has.
- The authors nevertheless conclude that ‘acupuncture treatment produced a fast and clinically relevant reduction’ of symptoms.
- They also state that they used this design because no validated sham acupuncture method exists. This is demonstrably wrong.
- In my view, such misleading statements might even amount to scientific misconduct.
So, what would be the result of a trial that is rigorous and does adequately control for placebo-effects? Luckily, we do not need to rely on speculation here; we have a study to demonstrate the result:
Background: Hot flashes (HFs) affect up to 75% of menopausal women and pose a considerable health and financial burden. Evidence of acupuncture efficacy as an HF treatment is conflicting.
Objective: To assess the efficacy of Chinese medicine acupuncture against sham acupuncture for menopausal HFs.
Design: Stratified, blind (participants, outcome assessors, and investigators, but not treating acupuncturists), parallel, randomized, sham-controlled trial with equal allocation. (Australia New Zealand Clinical Trials Registry: ACTRN12611000393954)
Setting: Community in Australia.
Participants: Women older than 40 years in the late menopausal transition or postmenopause with at least 7 moderate HFs daily, meeting criteria for Chinese medicine diagnosis of kidney yin deficiency.
Interventions:10 treatments over 8 weeks of either standardized Chinese medicine needle acupuncture designed to treat kidney yin deficiency or noninsertive sham acupuncture.
Measurements: The primary outcome was HF score at the end of treatment. Secondary outcomes included quality of life, anxiety, depression, and adverse events. Participants were assessed at 4 weeks, the end of treatment, and then 3 and 6 months after the end of treatment. Intention-to-treat analysis was conducted with linear mixed-effects models.
Results: 327 women were randomly assigned to acupuncture (n = 163) or sham acupuncture (n = 164). At the end of treatment, 16% of participants in the acupuncture group and 13% in the sham group were lost to follow-up. Mean HF scores at the end of treatment were 15.36 in the acupuncture group and 15.04 in the sham group (mean difference, 0.33 [95% CI, −1.87 to 2.52]; P = 0.77). No serious adverse events were reported.
Limitation: Participants were predominantly Caucasian and did not have breast cancer or surgical menopause.
Conclusion: Chinese medicine acupuncture was not superior to noninsertive sham acupuncture for women with moderately severe menopausal HFs.
My conclusion from all this is simple: acupuncture trials generate positive findings, provided the researchers fail to test it rigorously.
Did we not have a flurry of systematic reviews of homeopathy in recent months?
And were they not a great disappointment to homeopaths and their patients?
Just as we thought that this is more than enough evidence to show that homeopathy is not effective, here comes another one.
This new review evaluated RCTs of non-individualised homeopathic treatment (NIHT) in which the control group received treatments other than placebo (OTP). Specifically, its aim was to determine the comparative effectiveness of NIHT on health-related outcomes for any given condition.
For each eligible trial, published in the peer-reviewed literature up to the end of 2016, the authors assessed its risk of bias (internal validity) using the seven-domain Cochrane tool, and its relative pragmatic or explanatory attitude (external validity) using the 10-domain PRECIS tool. The researchers grouped RCTs by whether these examined homeopathy as an alternative treatment (study design 1a), adjunctively with another intervention (design 1b), or compared with no intervention (design 2). RCTs were sub-categorised as superiority trials or equivalence/non-inferiority trials. For each RCT, a single ‘main outcome measure’ was selected to use in meta-analysis.
Seventeen RCTs, representing 15 different medical conditions, were eligible for inclusion. Three of the trials were more pragmatic than explanatory, two were more explanatory than pragmatic, and 12 were equally pragmatic and explanatory. Fourteen trials were rated ‘high risk of bias’ overall; the other three trials were rated ‘uncertain risk of bias’ overall. Ten trials had data that were extractable for meta-analysis. Significant heterogeneity undermined the planned meta-analyses or their meaningful interpretation. For the three equivalence or non-inferiority trials with extractable data, the small, non-significant, pooled effect size was consistent with a conclusion that NIHT did not differ from treatment by a comparator (Ginkgo biloba or betahistine) for vertigo or (cromolyn sodium) for seasonal allergic rhinitis.
The authors concluded that the current data preclude a decisive conclusion about the comparative effectiveness of NIHT. Generalisability of findings is restricted by the limited external validity identified overall. The highest intrinsic quality was observed in the equivalence and non-inferiority trials of NIHT.
I do admire the authors’ tenacity in meta-analysing homeopathy trials and empathise with their sadness of the multitude of negative results they thus have to publish. However, I do disagree with their conclusions. In my view, at least two firm conclusions ARE possible:
- This dataset confirms yet again that the methodological quality of homeopathy trials is lousy.
- The totality of the trial evidence analysed here fails to show that non-individualised homeopathy is effective.
In case you wonder why the authors are not more outspoken about their own findings, perhaps you need to read their statement of conflicts of interest:
Authors RTM, YYYF, PV and AKLT are (or were) associated with a homeopathy organisation whose significant aim is to clarify and extend an evidence base in homeopathy. RTM holds an independent research consultancy contract with the Deutsche Homöopathie-Union, Karlsruhe, Germany. YYYF and AKLT belong to Living Homeopathy Ltd., which has contributed funding to some (but not this current) HRI project work. RTM and PV have no other relationships or activities that could appear to have influenced the submitted work. JRTD had no support from any organisation for the submitted work; in the last 3 years, and for activities outside the submitted study, he received personal fees, royalties or out-of-pocket expenses for advisory work, invitational lectures, use of rating scales, published book chapters or committee membership; he receives royalties from Springer Publishing Company for his book, A Century of Homeopaths: Their Influence on Medicine and Health. JTRD has no other relationships or activities that could appear to have influenced the submitted study.
If one had wanted to add insult to injury, one could have added that, if, despite such conflicts of interest, the overall result of this new review turned out to be not positive, the evidence must be truly negative.
Simply put, in the realm of SCAM, we seem to have two types of people:
- those who don’t care a hoot about evidence;
- those who try their best to follow the evidence.
The first group is replete with SCAM enthusiasts who make their decisions based purely on habit, emotion, intuition etc. They are beyond my reach, I fear. It is almost exclusively the second group for whom I write this blog.
And that could be relatively easy, if the evidence were always accessible, understandable, straight forward, conclusive and convincing. But sadly, in SCAM (as in most other areas of healthcare), the evidence is full of apparent and real contradictions. In this situation, it is often difficult even for experts to understand what is going on; for lay people this must be immeasurably more confusing. Yet, it is the lay consumers who often will take the decision to use or not use this or that SCAM. They therefore need our help.
What can consumers do when they are confronted with contradictory evidence?
How can they distinguish right from wrong?
- Some articles claim that homeopathy works – others say it is just a placebo therapy.
- Some experts claim that chiropractic is safe – others say it can do serious harm.
- Some articles claim that SCAM-practitioners are competent – others say this is not true.
- Some experts claim that SCAM is the future – others stress that it is obsolete.
What can a lay person with no or very little understanding of science do to see through this fog of contradictions?
Let me try to provide consumers with a step by step approach to get closer to the truth by asking a few incisive questions:
- WHERE DID YOU READ THE CLAIM? If it was in a newspaper, magazine, website, etc. take it with a pinch of salt (double the dose of salt, if it’s from the Daily Mail).
- CAN YOU RETRACE THE CLAIM TO A SCIENTIFIC PAPER? This might challenge you skills as a detective, but it is always well-worth finding the original source of a therapeutic claim in order to judge its credibility. If no good source can be found, I advise caution.
- IN WHICH MEDICAL JOURNAL WAS THE CLAIM PUBLISHED? Be aware of the fact that there are dozens of SCAM-journals that would publish virtually any rubbish.
- WHO ARE THE AUTHORS OF THE SCIENTIFIC PAPER? It might be difficult for a lay person to evaluate their credibility. But there might be certain pointers; for instance, authors affiliated to a university tend to be more credible than SCAM-practitioners who have no such affiliations or authors working for a lobby-group.
- WHAT SORT OF ARTICLE IS THE ORIGINAL SOURCE OF THE CLAIM? Is it a proper experimental study or a mere opinion piece? If possible, try to find a good-quality (perhaps even a Cochrane) review on the subject.
- ARE THERE OTHER RESEARCHERS WHO HAVE ARRIVED AT SIMILAR CONCLUSIONS? If the claim is based on just one solitary piece of research or opinion, it clearly weighs less than a consensus of experts.
- DO PUBLICATIONS EXIST THAT DISAGREE WITH THE CLAIM? Even if there are several scientific papers from different teams of researchers supporting the claim, it is important to find out whether the claim is shared by all experts in the field.
Eventually, you might get a good impression about the veracity of the claim. But sometimes you also might end up with a bunch of systematic reviews of which several support, while others reject the claim. And all of them could look similarly credible to your untrained eyes. Does that mean your attempt to find the truth of the matter has been frustrated?
Not necessarily!
In this case, you would probably consider the following options:
- You could do a simple ‘pea count’; this would tell you whether the majority of reviews is pro or contra the claim. However, this might be your worst bet for arriving at a sound conclusion. The quantity of the evidence usually is far less important than its quality.
- If you have no training to judge the quality of a review, you might just go with the most recent and up-to-date review. This, however, would also be fraught with problems, as you can, of course, not be sure that the most recent one is also the least biased assessment.
- Perhaps you can somehow get an impression about the respectability of the source. If, for instance, there is a recent Cochrane review, I advise to go with that one.
- Look up the profession of the authors of the review. The pope is unlikely to condemn Catholicism; likewise, you will find very few homeopaths who are critical of homeopathy, or chiropractors who are critical of chiropractic, etc. I know this is a very crude ‘last resort’ for replacing an authorative evaluation of the claim. But, if that’s all you have, it is better than nothing. Ask yourself who can normally be trusted more, the SCAM-practitioner or lobbyist who makes a living from the claim or an independent academic who has no such conflict of interest?
If all of this does not help you to decide whether a therapeutic claim is trustworthy or not, my advice has always been to reflect on this: IF IT SOUNDS TOO GOOD TO BE TRUE, IT PROBABLY IS.