insomnia
Insomnia is a prevalent disorder that is associated with substantial impairment. Homeopathy has been proposed as a complementary treatment for insomnia, but its clinical effects remain uncertain.
This systematic review assessed the efficacy, effectiveness, and safety of homeopathic treatments for insomnia. Prospective comparative studies evaluating any homeopathic preparation for insomnia were included. Searches in MEDLINE, EMBASE, seven additional databases, and three trial registries were conducted through August 2025. Risk of bias, intervention complexity, model validity, and pragmatism were assessed using respectively RoB 2, ROBINS-I, iCAT, MVHT, and RITES. Data were synthesized using random-effects meta-analyses, and certainty of evidence was evaluated using GRADE.
Eight randomized controlled trials (RCTs; n = 364 participants) and four non-randomized studies (NRSIs; n = 517) met the inclusion criteria. In adults, sleep quality (MD = −2.6 points; 95% CI −5.5 to 2.6; low certainty) and insomnia severity (MD = −3.2; 95% CI −5.68 to −0.72, moderate certainty) were reported in one RCT each. For total sleep time, the pooled MD of three RCTs was 0.65 hours (95% CI −0.9 to 2.2; low certainty). In children, one open-label RCT suggested a difference in insomnia severity, but certainty of evidence was very low. Adverse events were rarely reported, resulting in low certainty evidence.
The authors concluded that the current evidence is mainly limited by imprecision and risk of bias. The available evidence does not allow firm conclusions regarding the effects of homeopathy for insomnia. High-quality, replicated trials with systematic adverse event monitoring are needed.
15 years ago, I published a similar review entitled “Homeopathy for insomnia and sleep-related disorders: a systematic review of randomised controlled trials” (Focus on Alternative and Complementary Therapies Volume 16(3) September 2011 195–199)). Here is its abstract:
The aim of this review was the critical evaluation of evidence for the effectiveness of homeopathy for insomnia and sleep-related disorders. A search of MEDLINE, AMED, CINAHL, EMBASE and Cochrane Central Register was conducted to find RCTs using any form of homeopathy for the treatment of insomnia or sleep-related disorders. Data were extracted according to predefined criteria; risk of bias was assessed using Cochrane criteria. Six randomised, placebo-controlled trials met the inclusion criteria. Two studies used individualised homeopathy, and four used standardised homeopathic treatment. All studies had significant flaws; small sample size was the most prevalent limitation. The results of one study suggested that homeopathic remedies were superior to placebo; however, five trials found no significant differences between homeopathy and placebo for any of the main outcomes. Evidence from RCTs does not show homeopathy to be an effective treatment for insomnia and sleep-related disorders.
The findings of the two reviews are remarkably similar. For the following reasons, I find this notable:
- One would have hoped that 15 years are a long enough time for clarifying the issue, particularly as insomnia is not an unimportant condition for homeopathy.
- The new review is authored by well-known proponents. It seems unexpected that they (almost) go as far as admitting that the evidence for homeopathy as a treatment for insomnia is not positive.
- We have here, I think, a textbook example of how proponents of homeopathy prettify results that do not confirm their belief.
SO FAR, SO GOOD.
But now consider this: There are two further reviews of the same subject!
The first is entitled “Homoeopathy for insomnia: A meta-analysis of clinical evidence – Journal of Integrated Standardized Homoeopathy“. Here is its abstract:
Objectives: Insomnia is a prevalent sleep disorder characterised by challenges in initiating, maintaining or achieving restorative sleep, resulting in compromised daytime functionality. Traditional therapeutic modalities frequently encompass pharmacological treatments, which may have adverse effects and potential for dependency. Numerous patients pursue alternative methodologies, such as homoeopathy, which is attributed to its personalised, holistic and non-invasive treatment framework. This thorough examination assesses the effectiveness of homoeopathy in promoting better sleep quality and overall wellness in people with insomnia by analysing randomised controlled trials (RCTs).
Material and Methods: This meta-analysis sought to ascertain whether homoeopathy induces a statistically significant enhancement in the management of insomnia, concentrating on aspects of sleep quality, duration and general well-being. All RCTs addressing insomnia treated with homoeopathic interventions were included in this review. All studies were meticulously documented in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Three evaluators independently reviewed and compiled the literature, extracting comprehensive details regarding participants, study designs, therapeutic interventions and follow-up pertaining to homoeopathic treatment. The primary outcome of the investigation was disease assessment based on sleep diary scores, with an additional outcome being the enhancement of quality of life.
Results: The analysis revealed that homoeopathic remedies exhibited statistically significant improvement over placebo in the management of insomnia. The overall pooled effect size, standardised mean difference (random), was −0.60, standard error (random) was 0.42 and confidence interval (random) at 95% ranged from −0.93 to −0.26. The risk of bias was assessed for all studies.
Conclusion: This meta-analysis shows that homoeopathic remedies are effective in treating insomnia, but more studies are required for accuracy.
The last review is entitled “Effectiveness of Homeopathic Interventions for Insomnia and Sleep Disorders: A Systematic Review and Meta-Analysis“. Here is its abstract:
Insomnia is a common sleep disorder, and many individuals seek alternative treatments like homeopathy. However, evidence for its effectiveness remains controversial. This systematic review and meta-analysis evaluated the effectiveness of homeopathic interventions for insomnia and sleep-wake disorders. A comprehensive search of PubMed, MEDLINE, CINAHL, and the Cochrane Library was conducted for studies published between 2010 and 2025. We included randomized controlled trials (RCTs) and non-randomized studies involving adults (≥18 years) with primary insomnia receiving any homeopathic intervention compared to placebo, no treatment, or active care. Primary outcomes included validated sleep quality measures (e.g., Pittsburgh Sleep Quality Index (PSQI), Insomnia Severity Index (ISI). Four reviewers independently performed study selection, data extraction, and risk of bias assessment using RoB 2.0 and ROBINS-I. A random-effects meta-analysis was conducted for controlled trials, and a narrative synthesis for non-randomized studies. Certainty of evidence was assessed using Grading of Recommendations, Assessment, Development and Evaluation (GRADE). The search yielded 1304 records; 12 studies (nine RCTs and three non-randomized) met inclusion criteria. Meta-analysis showed a large, statistically significant positive effect of homeopathy on sleep outcomes (SMD = 0.81, 95% CI [0.24, 1.38], p = 0.0055), with substantial heterogeneity (I² = 86.04%) and publication bias (Egger’s test, p = 0.0079). Most studies had high or critical risk of bias, and overall certainty was low. Homeopathic interventions showed a large positive effect on sleep outcomes, but due to high bias, heterogeneity, and publication bias, evidence remains low-certainty and insufficient to support effectiveness. High-quality RCTs are needed.
What should we make of this?
We now have two reviews concluding that there is no good evidence and two implying that homeopathy is effective for insomnia! This clearly demonstrates how easy it is to mislead the public with seemingly rigorous reviews.
I must say, I pity all the interested lay people who are trying to make sense of this mess.
How can they arrive at the best available, most reliable evidence?
We have here, I think, another textbook example; one of how important it is to run reality checks. But surely, we cannot possible ask of a lay person to understand why the last two reviews are badly misleading. What we need is an accessible tool for differentiating the science from the pseudoscience, the reliable from the unreliable.
Unfortunately, such a tool does not exist. But there are a few indicators:
- Is the journal that published the review reputable?
- Are the authors affiliated to reputable institutions?
- Do the authors have a history of critical analysis or one of uncritical promotion?
- Do they explain clearly and provide the essential details of their work?
These are issues that lay people might be able to check relatively easily. The above 4 reviews demonstrate that using them does not always provided an entirely clear cut-off. However, it might give some valuable pointers into the right direction.
Zack Polanski the current Leader of the Green Party of England and Wales, previously worked as a professional “cognitive hypnotherapist”.
My own assessment of hypnotherapy states that is the use of a trance-like state (hypnosis) for therapeutic purposes. It can be traced back to ancient cultures, but more recently Anton Mesmer (1734–1815) introduced hypnotherapy into medicine. Initially Mesmer was highly successful—until a Royal Commission investigated his method of ‘animal magnetism’ and concluded its effects were entirely due to imagination. Hypnotherapy induces in many but not all individuals a state of deep relaxation that is potentially helpful in a range of conditions. Today, there are different schools of hypnotherapy, e.g. Ericksonian hypnotherapy, cognitive behavioural hypnotherapy, curative hypnotherapy. Various different healthcare professionals practise hypnotherapy, including doctors, dentists, psychologists and nurses. Hypnotherapy is used to treat many conditions or symptoms, from pain and stress to irritable bowel syndrome and drug dependency. The evidence from clinical trials is mixed. Most systematic reviews emphasise the often poor-quality of the primary studies, e.g.:
“Hypnosis reduces pain intensity and anxiety ratings in adults undergoing burn wound care. However, because of the limitations discussed, clinical recommendations are still premature.”
“Due to exploratory designs and high risk of bias, the effectiveness of hypnosis or hypnotherapy in stress reduction remains still unclear.”
“There are still only a relatively small number of studies assessing the use of hypnosis for labour and childbirth. Hypnosis may reduce the overall use of analgesia during labour, but not epidural use. No clear differences were found between women in the hypnosis group and those in the control groups for satisfaction with pain relief, sense of coping with labour or spontaneous vaginal birth. Not enough evidence currently exists regarding satisfaction with pain relief or sense of coping with labour and we would encourage any future research to prioritise the measurement of these outcomes. The evidence for the main comparison was assessed using GRADE as being of low quality for all the primary outcomes with downgrading decisions due to concerns regarding inconsistency of the evidence, limitations in design and imprecision.”
“We have not shown that hypnotherapy has a greater effect on six month quit rates than other interventions or no treatment. The effects of hypnotherapy on smoking cessation claimed by uncontrolled studies were not confirmed by analysis of randomised controlled trials.”
“Current research concerning the efficacy of hypnosis to relieve insomnia is lacking in key methodological elements”
Contrary to what is often claimed, hypnotherapy is not entirely free of adverse effects. It has been associated with the ‘false memory syndrome’ where unpleasant recollections that have never occurred are implanted into the patient’s brain. Hypnotherapy should not be used by patients who suffer from psychoses or personality disorders.
Polanski’s practice was based at a clinic on Harley Street, a London district renowned for private healthcare. His work focused on personal development, confidence building, and body-image issues. Polanski’s hypnotherapy career became a subject of public scrutiny due to a 2013 report by The Sun newspaper, in which it was claimed that during a consultation, Polanski offered to use hypnosis to facilitate breast enlargement. While Polanski later stated the piece was a “misleading” representation of his methods and intended as an experiment in internal self-image, recent investigative reporting has cast doubt on his subsequent narrative.
Although Polanski has frequently asserted that he apologized for the article “the day after” its publication in a BBC radio interview. This claim is, however, contested. In a 2013 interview with BBC Radio Humberside, Polanski reportedly discussed the technique and stated that “the evidence is growing” regarding its efficacy. Independent analysis of the clinical evidence-base for hypnotherapy fails to find good evidence regarding physical outcomes. Similarly, the evidence regarding the efficacy of hypnotherapy for personal development and confidence building is at best varied, with outcomes often depending on the specific application and individual context. My own assessment does not arrive at a positive conclusion.
Polanski has claimed he was misrepresented in the Sun article. Yet, he also wrote in a 2019 blog post that he did not believe the journalist had done a “bad job” or misrepresented him. In that same post, he noted that the coverage led to numerous inquiries from men seeking similar hypnotic treatments for other physical augmentations, all of which he stated he declined.
The “breast enlargement” claim has been frequently cited by political opponents and the media to question Polanski’s judgment and credibility. The story has resurfaced repeatedly during his political campaigns, including through confrontations from members of the public and intense scrutiny during his time as leader.
Polanski maintains that his background in hypnotherapy provides him with unique insights into mental health and communication, which he views as assets in his political role. I would add that, for many of the conditions for which it is promoted, hypnotherapy is not an evidence-based treatment.
Polanski has expressed regret for the “distraction” the story has caused his party, even as critics continue to challenge the consistency of his account regarding the original 2013 events.
Obesity is, as we all know, a huge public health issue. We therefore must no be amazed that the ‘SCAM brigade’ has collectively jumped on this bandwaggon – even auricualar acupressure is being promoted as a solution!
This study aimed to evaluate the impact of auricular acupressure on obesity and sleep quality in middle-aged Korean women. The single-blind, randomized, sham-controlled trial included participants aged 40-65 years with a Body Mass Index (BMI) of 25-34 kg/m 2 , divided into an experimental group (n = 30) and a control group (n = 29).
The intervention involved 8 weeks of auricular acupressure using ear seeds on five acupoints associated with obesity and sleep. Obesity outcomes were assessed using anthropometric indices (body weight, BMI, waist circumference, body fat mass, body fat percentage), while sleep outcomes were evaluated using the Pittsburgh Sleep Quality Index and actigraphy. Measurements were taken thrice: before the intervention, and at 4 and 8 weeks post-intervention start.
The experimental group demonstrated a significant reduction in obesity measures and improvement in sleep quality over time compared to the control group.
The authors suggest that their findings suggest that auricular acupressure may serve as an alternative nursing intervention for managing obesity and improving sleep quality in middle-aged women.
I have to admit that firstly I do not subscribe to ‘HOLIST. NURSE. PRACT.’ and secondly I am not willing to spend my money on buying this article. This means that I only can read the abstract of this paper. Thus my following explanations are speculative [but, as always, I am happy to change my tune once someone shows me that I was wrong].
So, how can a single- [presumably patient-] blind, sham controlled RCT of auricular acupuncture produce a positive result?
Fraud?
Not necessarily!
More likely, I think, is a phenomenon called ‘de-blinding’. For the above trial, this would mean that the control patients were treated with a sham procedure that was deemed to be indistinguishable from the verum by the trialists. But, in fact, patients managed to tell the difference between verum an sham. As the investigators did not check the success of their blinding procedure, they were able to call their study a ‘single-blind trial’, while in reality it was at least partly deblinded. If I am correct, the patients who were treated with the sham intervention fellt cheesed off for not receiving a real therapy and thus kept on eating, while the verum group did as told and controlled their diet a bit better.
In addition, ‘single-blind’, as applied to the patients, means that the therapists were not blinded. As they had a strong interest to generate a positive result, they would have used their verbal and non-verbal communication skills to influence their verum patients to reduce their obesity measures, e.g. by persualding them to excercise more and eat less.
In turn, these mechanisms together had the effect that “the experimental group demonstrated a significant reduction in obesity measures and improvement in sleep quality over time compared to the control group”.
QED
Alternatively, ‘single-blind’ might mean that the therapists were blinded. But, in this particular case, I don’t quite see how this would be possible.
Yes, there is yet another alternative: auricular acupressure might be effective in reducing obesity. If that is so, the current trial does not prove it!
Saffron, the stigmas of Crocus sativus L., has been used extensively in traditional herbal medicine. Since several years, the research interest in this plant is intense. Thus numerous clinical trials of saffron supplements (in contrast to the spice, supplements are affordable [they use different parts of the plant]) have been published. Almost all of them yield positive results (this invariably makes me suspicious!).
The purpose of this 2-arm, 12-wk, parallel-group, randomized, double-blind, placebo-controlled trial was to examine the effects of supplementation with a saffron extract (Affron) on mood and sleep in adults experiencing subclinical depressive symptoms. 202 adults aged 18-70 with depressive symptoms were supplemented with either 28 mg saffron daily or a placebo. Outcome measures included the Depression, Anxiety, and Stress Scale – 21, Sleep Disturbance and Sleep-Related Impairment Scale, World Health Organization-Five Well-Being Scale, and daily depression, stress, and anxiety ratings.
On the primary outcome measure, compared to the placebo, saffron was associated with greater improvements in the Depression, Anxiety, and Stress scale – 21 depression score (β: -2.92 points; 95% confidence interval: -5.13, -0.71 points; Cohen’s d = 0.39). 72% of participants in the saffron group achieved a clinically significant change (a reduction of ≥ 7 points) compared to 54.3% of participants in the placebo group (P = 0.010). However, in the other secondary outcomes, there was no evidence of between-group differences. In exploratory analyses across various strata and assumptions, improvements in sleep disturbances (β: -2.72 points; 95% confidence interval: -4.99, -0.46 points; Cohen’s d = 0.44) were identified in a subset of participants with a greater severity of sleep disturbance. There were no serious adverse reactions reported.
The authors concluded that this study, the largest conducted to date on saffron, provides evidence supporting the beneficial effects of 3 mo of saffron supplementation on depressive symptoms in adults. Large placebo responses were evident in this study, which require consideration in future trials.
As mentioned above, the body of evidence suggesting that saffron is effective for a surprisingly wide range of conditions is impressive. I looked with some skepticism at some of these studies and have to say that many are of decent or even good scientific quality.
Could it be that we have in saffron a plant-based treatment that shows real promise?
WATCH THIS SPACE!
A ‘pragmatic, superiority, open-label, randomised controlled trial’ of sleep restriction therapy versus sleep hygiene has just been published in THE LANCET. Adults with insomnia disorder were recruited from 35 general practices across England and randomly assigned (1:1) using a web-based randomisation programme to either four sessions of nurse-delivered sleep restriction therapy plus a sleep hygiene booklet or a sleep hygiene booklet only. There was no restriction on usual care for either group. Outcomes were assessed at 3 months, 6 months, and 12 months. The primary endpoint was self-reported insomnia severity at 6 months measured with the insomnia severity index (ISI). The primary analysis included participants according to their allocated group and who contributed at least one outcome measurement. Cost-effectiveness was evaluated from the UK National Health Service and personal social services perspective and expressed in terms of incremental cost per quality-adjusted life year (QALY) gained. The trial was prospectively registered (ISRCTN42499563).
Between Aug 29, 2018, and March 23, 2020 the researchers randomly assigned 642 participants to sleep restriction therapy (n=321) or sleep hygiene (n=321). Mean age was 55·4 years (range 19–88), with 489 (76·2%) participants being female and 153 (23·8%) being male. 580 (90·3%) participants provided data for at least one outcome measurement. At 6 months, mean ISI score was 10·9 (SD 5·5) for sleep restriction therapy and 13·9 (5·2) for sleep hygiene (adjusted mean difference –3·05, 95% CI –3·83 to –2·28; p<0·0001; Cohen’s d –0·74), indicating that participants in the sleep restriction therapy group reported lower insomnia severity than the sleep hygiene group. The incremental cost per QALY gained was £2076, giving a 95·3% probability that treatment was cost-effective at a cost-effectiveness threshold of £20 000. Eight participants in each group had serious adverse events, none of which were judged to be related to intervention.
The authors concluded that brief nurse-delivered sleep restriction therapy in primary care reduces insomnia symptoms, is likely to be cost-effective, and has the potential to be widely implemented as a first-line treatment for insomnia disorder.
I am frankly amazed that this paper was published in a top journal, like THE LANCET. Let me explain why:
The verum treatment was delivered over four consecutive weeks, involving one brief session per week (two in-person sessions and two sessions over the phone). Session 1 introduced the rationale for sleep restriction therapy alongside a review of sleep diaries, helped participants to select bed and rise times, advised on management of daytime sleepiness (including implications for driving), and discussed barriers to and facilitators of implementation. Session 2, session 3, and session 4 involved reviewing progress, discussion of difficulties with implementation, and titration of the sleep schedule according to a sleep efficiency algorithm.
This means that the verum group received fairly extensive attention, while the control group did not. In other words, a host of non-specific effects are likely to have significantly influenced or even entirely determined the outcome. Despite this rather obvious limitation, the authors fail to discuss any of it. On the contrary, that claim that “we did a definitive test of whether brief sleep restriction therapy delivered in primary care is clinically effective and cost-effective.” This is, in my view, highly misleading and unworthy of THE LANCET. I suggest the conclusions of this trial should be re-formulated as follows:
The brief nurse-delivered sleep restriction, or the additional attention provided exclusively to the patients in the verum group, or a placebo-effect or some other non-specific effect reduced insomnia symptoms.
Alternatively, one could just conclude from this study that poor science can make it even into the best medical journals – a problem only too well known in the realm of so-called alternative medicine (SCAM).
Electroacupuncture (EA) is often advocated for depression and sleep disorders but its efficacy remains uncertain. The aim of this study was, therefore, to “assess the efficacy and safety of EA as an alternative therapy in improving sleep quality and mental state for patients with insomnia and depression.”
A 32-week patient- and assessor-blinded, randomized, sham-controlled clinical trial (8-week intervention plus 24-week follow-up) was conducted from September 1, 2016, to July 30, 2019, at 3 tertiary hospitals in Shanghai, China. Patients were randomized to receive
- EA treatment and standard care,
- sham acupuncture (SA) treatment and standard care,
- standard care only as control.
Patients in the EA or SA groups received a 30-minute treatment 3 times per week (usually every other day except Sunday) for 8 consecutive weeks. All treatments were performed by licensed acupuncturists with at least 5 years of clinical experience. A total of 6 acupuncturists (2 at each center; including X.Y. and S.Z.) performed EA and SA, and they received standardized training on the intervention method before the trial. The regular acupuncture method was applied at the Baihui (GV20), Shenting (GV24), Yintang (GV29), Anmian (EX-HN22), Shenmen (HT7), Neiguan (PC6), and SanYinjiao (SP6) acupuncture points, with 0.25 × 25-mm and 0.30 × 40-mm real needles (Wuxi Jiajian Medical Device Co, Ltd), or 0.30 × 30-mm sham needles (Streitberger sham device [Asia-med GmbH]).
For patients in the EA group, rotating or lifting-thrusting manipulation was applied for deqi sensation after needle insertion. The 2 electrodes of the electrostimulator (CMNS6-1 [Wuxi Jiajian Medical Device Co, Ltd]) were connected to the needles at GV20 and GV29, delivering a continuous wave based on the patient’s tolerance. Patients in the SA group felt a pricking sensation when the blunt needle tip touched the skin, but without needle insertion. All indicators of the nearby electrostimulator were set to 0, with the light switched on. Standard care (also known as treatment as usual or routine care) was used in the control group. Patients receiving standard care were recommended by the researchers to get regular exercise, eat a healthy diet, and manage their stress level during the trial. They were asked to keep the regular administration of antidepressants, sedatives, or hypnotics as well. Psychiatrists in the Shanghai Mental Health Center (including X.L.) guided all patients’ standard care treatment and provided professional advice when a patient’s condition changed.
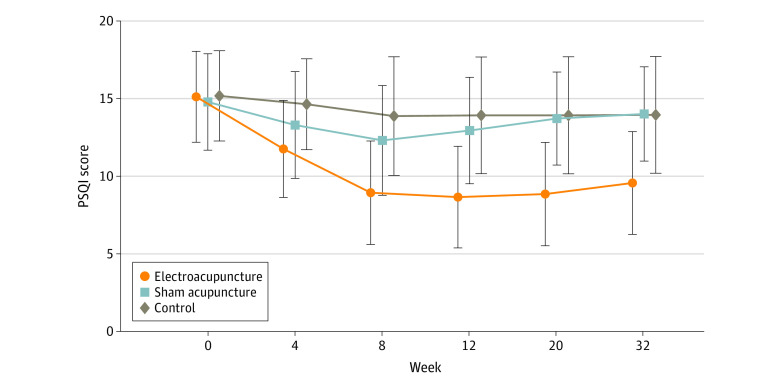
The primary outcome was change in Pittsburgh Sleep Quality Index (PSQI) from baseline to week 8. Secondary outcomes included PSQI at 12, 20, and 32 weeks of follow-up; sleep parameters recorded in actigraphy; Insomnia Severity Index; 17-item Hamilton Depression Rating Scale score; and Self-rating Anxiety Scale score.
Among the 270 patients (194 women [71.9%] and 76 men [28.1%]; mean [SD] age, 50.3 [14.2] years) included in the intention-to-treat analysis, 247 (91.5%) completed all outcome measurements at week 32, and 23 (8.5%) dropped out of the trial. The mean difference in PSQI from baseline to week 8 within the EA group was -6.2 (95% CI, -6.9 to -5.6). At week 8, the difference in PSQI score was -3.6 (95% CI, -4.4 to -2.8; P < .001) between the EA and SA groups and -5.1 (95% CI, -6.0 to -4.2; P < .001) between the EA and control groups. The efficacy of EA in treating insomnia was sustained during the 24-week postintervention follow-up. Significant improvement in the 17-item Hamilton Depression Rating Scale (-10.7 [95% CI, -11.8 to -9.7]), Insomnia Severity Index (-7.6 [95% CI, -8.5 to -6.7]), and Self-rating Anxiety Scale (-2.9 [95% CI, -4.1 to -1.7]) scores and the total sleep time recorded in the actigraphy (29.1 [95% CI, 21.5-36.7] minutes) was observed in the EA group during the 8-week intervention period (P < .001 for all). No between-group differences were found in the frequency of sleep awakenings. No serious adverse events were reported.
The result of the blinding assessment showed that 56 patients (62.2%) in the SA group guessed wrongly about their group assignment (Bang blinding index, −0.4 [95% CI, −0.6 to −0.3]), whereas 15 (16.7%) in the EA group also guessed wrongly (Bang blinding index, 0.5 [95% CI, 0.4-0.7]). This indicated a relatively higher degree of blinding in the SA group.
The authors concluded that, in this randomized clinical trial of EA treatment for insomnia in patients with depression, quality of sleep improved significantly in the EA group compared with the SA or control group at week 8 and was sustained at week 32.
This trial seems rigorous, it has a sizable sample size, uses a credible placebo procedure, and is reported in sufficient detail. Why then am I skeptical?
- Perhaps because we have often discussed how untrustworthy acupuncture studies from China are?
- Perhaps because I fail to see a plausible mechanism of action?
- Perhaps because the acupuncturists could not be blinded and thus might have influenced the outcome?
- Perhaps because the effects of sham acupuncture seem unreasonably small?
- Perhaps because I cannot be sure whether the acupuncture or the electrical current is supposed to have caused the effects?
- Perhaps because the authors of the study are from institutions such as the Shanghai Municipal Hospital of Traditional Chinese Medicine, the Department of Acupuncture and Moxibustion, Huadong Hospital, Fudan University, Shanghai,
- Perhaps because the results seem too good to be true?
If you have other and better reasons, I’d be most interested to hear them.
Yes, Today is ‘WORLD SLEEP DAY‘ and you are probably in bed hoping this post will put you back to sleep.
I’ll do my best!
This study aimed to synthesise the best available evidence on the safety and efficacy of using moxibustion and/or acupuncture to manage cancer-related insomnia (CRI).
The PRISMA framework guided the review. Nine databases were searched from its inception to July 2020, published in English or Chinese. Randomised clinical trials (RCTs) of moxibustion and or acupuncture for the treatment of CRI were selected for inclusion. The methodological quality was assessed using the method suggested by the Cochrane collaboration. The Cochrane Review Manager was used to conduct a meta-analysis.
Fourteen RCTs met the eligibility criteria; 7 came from China. Twelve RCTs used the Pittsburgh Sleep Quality Index (PSQI) score as continuous data and a meta-analysis showed positive effects of moxibustion and or acupuncture (n = 997, mean difference (MD) = -1.84, 95% confidence interval (CI) = -2.75 to -0.94, p < 0.01). Five RCTs using continuous data and a meta-analysis in these studies also showed significant difference between two groups (n = 358, risk ratio (RR) = 0.45, 95% CI = 0.26-0.80, I 2 = 39%).
The authors concluded that the meta-analyses demonstrated that moxibustion and or acupuncture showed a positive effect in managing CRI. Such modalities could be considered an add-on option in the current CRI management regimen.
Even at the risk of endangering your sleep, I disagree with this conclusion. Here are some of my reasons:
- Chinese acupuncture trials invariably are positive which means they are as reliable as a 4£ note.
- Most trials were of poor methodological quality.
- Only one made an attempt to control for placebo effects.
- Many followed the A+B versus B design which invariably produces (false-) positive results.
- Only 4 out of 14 studies mentioned adverse events which means that 10 violated research ethics.
Sorry to have disturbed your sleep!
Acupuncture is a veritable panacea; it cures everything! At least this is what many of its advocates want us to believe. Does it also have a role in supportive cancer care?
Let’s find out.
This systematic review evaluated the effects of acupuncture in women with breast cancer (BC), focusing on patient-reported outcomes (PROs).
A comprehensive literature search was carried out for randomized controlled trials (RCTs) reporting PROs in BC patients with treatment-related symptoms after undergoing acupuncture for at least four weeks. Literature screening, data extraction, and risk bias assessment were independently carried out by two researchers. The authors stated that they followed the ‘Preferred Reporting Items for Systematic Review and Meta-Analyses’ (PRISMA) guidelines.
Out of the 2, 524 identified studies, 29 studies representing 33 articles were included in this meta-analysis. The RCTs employed various acupuncture techniques with a needle, such as hand-acupuncture and electroacupuncture. Sham/placebo acupuncture, pharmacotherapy, no intervention, or usual care were the control interventions. About half of the studies lacked adequate blinding.
At the end of treatment (EOT), the acupuncture patients’ quality of life (QoL) was measured by the QLQ-C30 QoL subscale, the Functional Assessment of Cancer Therapy-Endocrine Symptoms (FACT-ES), the Functional Assessment of Cancer Therapy–General/Breast (FACT-G/B), and the Menopause-Specific Quality of Life Questionnaire (MENQOL), which depicted a significant improvement. The use of acupuncture in BC patients lead to a considerable reduction in the scores of all subscales of the Brief Pain Inventory-Short Form (BPI-SF) and Visual Analog Scale (VAS) measuring pain. Moreover, patients treated with acupuncture were more likely to experience improvements in hot flashes scores, fatigue, sleep disturbance, and anxiety compared to those in the control group, while the improvements in depression were comparable across both groups. Long-term follow-up results were similar to the EOT results. Eleven RCTs did not report any information on adverse effects.
The authors concluded that current evidence suggests that acupuncture might improve BC treatment-related symptoms measured with PROs including QoL, pain, fatigue, hot flashes, sleep disturbance and anxiety. However, a number of included studies report limited amounts of certain subgroup settings, thus more rigorous, well-designed and larger RCTs are needed to confirm our results.
This review looks rigorous on the surface but has many weaknesses if one digs only a little deeper. To start with, it has no precise research question: is any type of acupuncture better than any type of control? This is not a research question that anyone can answer with just a few studies of mostly poor quality. The authors claim to follow the PRISMA guidelines, yet (as a co-author of these guidelines) I can assure you that this is not true. Many of the included studies are small and lacked blinding. The results are confusing, contradictory and not clearly reported. Many trials fail to mention adverse effects and thus violate research ethics, etc., etc.
The conclusion that acupuncture might improve BC treatment-related symptoms could be true. But does this paper convince me that acupuncture DOES improve these symptoms?
No!
Bach flower remedies were invented in the 1920s by Dr. Edward Bach (1886-1936), a doctor homeopath who had previously worked in the London Homeopathic Hospital. They have since become very popular in Europe and beyond. Bach flower remedies are clearly inspired by homeopathy; however, they are not the same because they do not follow the ‘like cures like’ principle and are they potentized. They are manufactured by placing freshly picked specific flowers or parts of plants in water which is subsequently mixed with alcohol, bottled, and sold. Like most homeopathic remedies, they are highly dilute and thus do not contain therapeutic amounts of the plant printed on the bottle.
The aim of this new randomized, double-blind, placebo-controlled trial was to compare the efficacy of flower therapy for the treatment of anxiety in overweight or obese adults with that of a placebo. The authors examined improvement in sleep patterns, reduction in binge eating, and change in resting heart rate (RHR).
The study included 40 participants in the placebo group and 41 in the intervention group. Participants were of both genders, from 20 to 59 years of age, overweight or obese, with moderate to high anxiety. They were randomized into two groups:
- one group was treated with Bach flower remedies (BFR) (bottles containing 30 mL of 30% hydro-brandy solution with two drops each of Impatiens, White Chestnut, Cherry Plum, Chicory, Crab Apple, and Pine), purchased from Healing® Flower Essences (São Paulo, Brazil)
- the other group was given a placebo (same solution without BFR).
All patients were instructed to orally ingest the solutions by placing four drops directly in the mouth four times a day for 4 weeks.
The primary outcome was anxiety (State-Trait Anxiety Inventory [STAI]). Secondary outcomes were sleep (Pittsburgh Sleep Quality Index [PSQI]), binge eating (Binge Eating Scale [BES]), and RHR (electrocardiogram).
Multivariate analysis showed significant reductions in scores for the following variables in the intervention group when compared with the placebo group: STAI (β = −0.190; p < 0.001), PSQI (β = −0.160; p = 0.027), BES (β = −0.226; p = 0.001), and RHR (β = −0.07; p = 0.003).
The authors concluded that anxiety symptoms, binge eating, and RHRs of the individuals treated with flower therapy decreased, and their sleep patterns improved when compared with those treated with the placebo.
Did the alcohol in the verum preparation had a relaxing effect? No, I was teasing. The amount would have been too small and the effect would have been the same in both groups. But what could have caused the observed outcome? I have to admit that I have no idea.
I read the study several times and could not find a major flaw. Hence it must have been the flower remedy that caused the positive outcome? No, I am teasing again. I find this impossible to imagine. These remedies contain nothing that might explain the results and all previous systematic reviews of all the available trials have all reached a negative conclusion. Before I seriously consider the option that flower remedies are more than placebos, I would like to see an independent replication.
Reflexology (originally called ‘zone therapy’ by its inventor) is a manual technique where pressure is applied to the sole of the patient’s foot. Reflexology is said to have its roots in ancient cultures. Its current popularity goes back to the US doctor William Fitzgerald (1872-1942) who did some research in the early 1900s and thought to have discovered that the human body is divided into 10 zones each of which is represented on the sole of the foot. Reflexologists thus drew maps of the sole of the foot where all the body’s organs are depicted. Numerous such maps have been published and, embarrassingly, they do not all agree with each other as to the location of our organs on the sole of our feet. By massaging specific zones which are assumed to be connected to specific organs, reflexologists believe to positively influence the function of these organs.
So, does reflexology do more good than harm?
The aim of this review was to conduct a systematic review, meta-analysis, and metaregression to determine the current best available evidence of the efficacy and safety of foot reflexology for adult depression, anxiety, and sleep quality.
Twenty-six studies could be included. The meta-analyses showed that foot reflexology intervention significantly improved adult depression, anxiety, and sleep quality. Metaregression revealed that an increase in total foot reflexology time and duration can significantly improve sleep quality.
The authors concluded that foot reflexology may provide additional nonpharmacotherapy intervention for adults suffering from depression, anxiety, or sleep disturbance. However, high quality and rigorous design RCTs in specific population, along with an increase in participants, and a long-term follow-up are recommended in the future.
Sounds good!
Finally a so-called alternative medicine (SCAM) that is backed by soild evidence!
Or perhaps not?
Here are a few concerns that lead me to doubt these conclusions:
- Most of the primary studies were of poor methodological quality.
- Most studies failed to mention adverse effects.
- Very few studies controlled for placebo effects.
- There was evidence of publication bias (negative studies tended to remain unpublished).
- Studies published in languages other than English were not considered.
- The authors fail to point out that a foot massage is, of course, agreeable (and thus may relieve a range of symptoms), but reflexology with all its weird assumptions is less than plausible.
- Many of the studies located by the authors were excluded for reasons that are less than clear.
The last point seems particularly puzzling. Our own trial, for instance, was excluded because, according to the review authors, it did not include relevant outcomes. However, our method secion makes it clear that the primary focus for this study was the subscores for anxiety and depression, which comprise four and seven items, respectively. As it happens, our study was negative.
Also cuirous is the fact that the authors did not mention our own 2011 systematic review of reflexology:
Reflexology is a popular form of complementary and alternative medicine (CAM). The aim of this update is to critically evaluate the evidence for or against the effectiveness of reflexology in patients with any type of medical condition. Six electronic databases were searched to identify all relevant randomised clinical trials (RCTs). Their methodological quality was assessed independently by the two reviewers using the Jadad score. Overall, 23 studies met all inclusion criteria. They related to a wide range of medical conditions. The methodological quality of the RCTs was often poor. Nine high quality RCTs generated negative findings; and five generated positive findings. Eight RCTs suggested that reflexology is effective for the following conditions: diabetes, premenstrual syndrome, cancer patients, multiple sclerosis, symptomatic idiopathic detrusor over-activity and dementia yet important caveats remain. It is concluded that the best clinical evidence does not demonstrate convincingly reflexology to be an effective treatment for any medical condition.
I wonder why!