migraine
Migraine affects more than 3 billion people worldwide, impacting mental, social, and economic well-being. Despite a wide range of pharmacological treatments, many patients experience limited relief or adverse effects, prompting interest in integrative approaches such as homoeopathy. This scoping review aimed to systematically explore and map the existing evidence on the role of homoeopathy in the management of migraine.
A comprehensive search was conducted across major databases and search engines, including PubMed, Medscape, Science Direct, Google Scholar, CCRH Homoeopathic Archives, and the AYUSH portal, covering studies published between 1990 and 2024. The search was limited to English or translated studies from peer-reviewed sources, indexed databases, and library publications.
A total of 37 full-text studies were screened. The review focused on
- randomized controlled trials,
- prospective studies,
- and retrospective observational studies
reporting clinical outcomes using validated tools such as VAS Scale, HIT 6, 24-Hr-MQoLQ, MOS SF-36 or MIDAS scores. Case reports, case series, editorials, letters, conference proceedings, and reviews lacking original research were excluded. Study selection, data extraction, and quality verification were independently performed by the reviewers according to PRISMA-ScR guidelines.
- 6 RCTs,
- 6 observational studies,
- 1 correlational study,
- and 1 quasi-experimental study
were included, while 23 were excluded. The centesimal scale was most commonly used, with potencies of 30, 200, and 1M. Among the 14 studies, 11 showed positive results for homoeopathy in reducing migraine frequency, severity, and duration. However, 3 studies found no significant difference between the homoeopathy and placebo groups, indicating potential placebo effects. While most findings are promising, some studies question homoeopathy’s specific effectiveness over placebo.
The Indian authors who are affiliated with various homeopathic institutions concluded that this scoping review highlights the potential role of homoeopathic treatment in the management of migraine as evidenced by previous studies. However, a notable gap in high-quality, well-designed research highlights the need for generating stronger levels of evidence to validate these findings.
That’s funny!
My own assessment, based on 4 RCTs, concluded that this systematic review has not produced compelling evidence to suggest that individualized homeopathic treatment is more effective than placebo in the prevention of migraine or headache attacks. However, due to several caveats (e.g., paucity of RCTs) it seems premature to make final judgment on this matter.
How can we explain this discrepancy?
In my view, there are several options:
- The Indian reviewers included Non-randomised studies and mischaracterised some trials.
- The Indian reviewers failed to take into account the lousy quality of the positive trials.
- The Indian reviewers did not aim to test the effectiveness of homeopathy but wanted to prove it.
In fact, I fear that all of these reasons apply.
And why am I so confident that homeopathy is not useful in the management of migraine? Just think about it: The Indian authors state correctly that “migraine affects more than 3 billion people worldwide, impacting mental, social, and economic well-being”. If it worked, would homeopathy not be the long-established treatment of choice for migraine?
I came across a new systematic review of the herbal remedy, FEVERFEW, as a preventative treatment for migraine. Here is the abstract:
Review just published in ‘The American Journal of Natural Medicines, Facts’
Migraine, a neurological condition, affects approximately 1.1 billion people worldwide, making it the third leading cause of disability. It significantly impacts quality of life and incurs an annual economic burden exceeding $78 billion in the United States. This systematic review and meta-analysis aims to evaluate the efficacy of Feverfew Dietary Supplement in migraine prophylaxis, with migraine frequency considered as the primary outcome. Three trials (n=237) were included in the meta-analysis (MA) of migraine frequency, and an additional three trials were synthesized narratively in the systematic review. In the MA, feverfew showed a non-significant reduction in migraine frequency compared to placebo (Overall effect size, Cohen’s d: -0.19; 95% CI: -0.52 to 0.14; I² = 34%, p = 0.26). These findings suggest that Feverfew might offer some benefit in individual patients, but given the small, non-significant effect size, it should not be recommended as a primary prophylactic agent over established treatments. Feverfew may not be effective as a standalone prophylactic supplement for migraines; however, its potential in combination therapies seems promising and requires further evaluation. Larger trials with standardized parthenolide content and extended durations are necessary to clarify feverfew’s definitive role in migraine prophylaxis.
The subject is no doubt interesting: migraine is a common contition that severely reduces quality of life and is difficult to treat or prevent. Thus an effective herbal remedy would be more than welcome. Based on such considerations, my co-workers and I had conducted a Cochrane review which was last updated in 2015. Here is its abstract:
Background: This review is an update of a previously published review in the Cochrane Database of Systematic Reviews on ‘Feverfew for preventing migraine’ (2004, Issue 1). Feverfew (Tanacetum parthenium L.) extract is a herbal remedy, which has been used for preventing attacks of migraine.
Objectives: To systematically review the evidence from double-blind randomised controlled trials (RCTs) assessing the clinical efficacy and safety of feverfew monopreparations versus placebo for preventing migraine.
Search methods: For this updated version of the review we searched CENTRAL, MEDLINE, EMBASE and AMED to January 2015. We contacted manufacturers of feverfew and checked the bibliographies of identified articles for further trials.
Selection criteria: We included randomised, placebo-controlled, double-blind trials assessing the efficacy of feverfew monopreparations for preventing migraine in patients of any age. We included trials using clinical outcome measures, while we excluded trials focusing exclusively on physiological parameters. There were no restrictions regarding the language of publication.
Data collection and analysis: We systematically extracted data on patients, interventions, methods, outcome measures, results and adverse events. We assessed risk of bias using the Cochrane ‘Risk of bias’ tool and evaluated methodological quality using the Oxford Quality Scale developed by Jadad and colleagues. Two review authors (BW and MHP for this update, MHP and EE for the original version) independently selected studies, assessed methodological quality and extracted data. We resolved disagreements concerning evaluation of individual trials through discussion.
Main results: We identified one new study for this update, resulting in six trials (561 patients) meeting the inclusion criteria. Five of the six trials reported on the main outcome, migraine frequency. Although five of the trials were generally of good methodological quality, all studies were either of unclear or high risk of bias with regards to sample size. Pooled analysis of the results was not possible due to the lack of common outcome measures and heterogeneity between studies in terms of participants, interventions and designs.The most recent trial added to this version of the review is rigorous and larger (n = 218), using a stable feverfew extract at a dose determined by a previous dose-finding trial. It reports that feverfew reduced migraine frequency by 1.9 attacks from 4.8 to 2.9 and placebo by 1.3 from to 4.8 to 3.5 per month, resulting in a difference in effect between feverfew and placebo of 0.6 attacks per month. For the secondary outcome measures intensity and duration of migraine attacks, incidence and severity of nausea and vomiting, and global assessment no statistically significant differences were reported. Results of previous trials are not convincing: three trials reporting positive effects of feverfew are all of small sample size (17 to 60 participants), while two rigorous trials (n = 50, 147) did not find significant differences between feverfew and placebo. Only mild and transient adverse events, most commonly gastrointestinal complaints and mouth ulcers, were reported in the included trials.
Authors’ conclusions: Since the last version of this review, one larger rigorous study has been included, reporting a difference in effect between feverfew and placebo of 0.6 attacks per month. This adds some positive evidence to the mixed and inconclusive findings of the previous review. However, this constitutes low quality evidence, which needs to be confirmed in larger rigorous trials with stable feverfew extracts and clearly defined migraine populations before firm conclusions can be drawn. It appears from the data reviewed that feverfew is not associated with any major safety concerns.
The question that I ask myself is this: what exactly does the new review add to the existing knowledge?
I fear, the answer is VERY LITTLE! Arguably, the new review is even less rigorous, transparent, thorough and informative than our paper.
If that is so, why conduct and publish it?
The process of doing this is an unethical waste of resources, and the habit of publishing redundant papers is irritating and arguably also unethical.
All this would be rather trivial, of course, if not for the fact that this form of science abuse is happening all the time in the realm of so-called alternative medicine. Responsible journal editors and reviewers should remember that they have the duty to prevent it.
Patients with headaches often seek so-called alternative medicine (SCAM), including chiropractic care. Chiropractic spinal manipulation is one of the most commonly used techniques for these patients; however, its effectiveness remains unclear. This systematic review aimed to evaluate the effectiveness of chiropractic spinal manipulation in reducing headache days, episode duration, episode intensity, and medication intake in patients with headaches.
MEDLINE (Pubmed), PEDro, SCOPUS, Cochrane Library and Web of Science databases were searched from inception to April 2024. PICO search strategy was used to identify randomized controlled trials applying chiropractic spinal manipulations versus sham manipulation, no additional intervention, or other conservative non-pharmacological interventions in patients with headaches. Eligible studies and data extraction were conducted independently by two reviewers. Quality of the studies was assessed with Physiotherapy Evidence Database scale, and risk of bias with Cochrane Collaboration tool. Certainty of the evidence was evaluated using GRADE approach.
Eight studies ranging from low to high methodological quality were included. The results were categorized into three subgroups: chiropractic manipulation versus sham, chiropractic manipulation versus control, and chiropractic manipulation versus deep friction massage. Among the five studies comparing chiropractic manipulation to sham, two found a significant reduction in the number of headache days. Of the three studies comparing chiropractic manipulation to another control, one reported a decrease in headache episode duration. No significant differences were observed for any other variable across the subgroups. The certainty of evidence was downgraded to very low.
We concluded that it is uncertain if chiropractic spinal manipulation is more effective than sham, control, or deep friction massage interventions for patients with headaches.
These conclusions might not surprise many readers. Yet, in at least one way, they are quite surprising: the version of the article we submitted to the ‘European Journal of Integrative Medicine’ had a substantially different conclusion; it was as follows:
What happened?
You may well ask!
The journal wanted us to change our conclusion! Because the main authors of our paper needed, for academic reasons, to publish without any further delay, they agreed to the demand. As far as I remember, such a thing is unprecedented in my ~50 years of publishing research in medical journals.
PS
It is also the last time I will have any dealings with the European Journal of Integrative Medicine
This “randomized controlled clinical trial” (has anyone ever seen a randomized trial without a control group? – No, therefore, the correct term is “ramdomized clinical trial (RCT)”) aimed to compare the effectiveness of wet cupping therapy (WCT) and Acupuncture in treating migraine patients. It was conducted between 01.03.2022 and 01.10.2023 in a Traditional and Complementary Medicine Center of a tertiary hospital. Patients diagnosed with migraine were included in the study and randomized into three groups.
- The WCT group received wet cupping 3 times, once a month.
- The acupuncture group received 10 sessions of acupuncture once a week.
- The waiting list group served as the control group.
VAS and MIDAS scales were used for all groups at the beginning and the end of the treatment, and the results were compared.
Initially, 168 patients were enrolled. However, there were some dropouts throughout the study period. In the acupuncture group, 11 patients did not attend subsequent sessions, with one dropout occurring due to adverse effects. In the wet cupping (WCT) group, three patients discontinued their participation following the initial treatment. Ultimately, a total of 153 patients were included.
The findings show that all three groups were similar regarding age and sex. Migraine Disability Assessment Scale (MIDAS) and Visual Analogue Scale (VAS) pain scores decreased significantly in both treatment groups after the applications, while they remained similar for the same period in the control group. Additionally, the post-treatment values of MIDAS and VAS in both the WCT and acupuncture groups were significantly lower compared to controls, while they were similar when compared in between.
The authors concluded that both of these applications were found to be similarly effective in improving disability status and pain intensity in patients with migraine.
I beg to differ!
Apart from all other flaws of this trial, it did not control for placebo effects. Both WCT and acupuncture are invasive treatments that are bound to cause sizeable placebo responses. The waiting list control might account for the natural history of the disease and for regression towards the mean, but it is not a method for allowing for placebo effects. In view of this fundamental limitation of the study, its conclusions should be re-written as follows:
Both of these applications were similarly effective in producing sizeable placebo effects which in turn improved disability status and pain intensity in patients with migraine.
For migraine patients, this means that neither of these therapies are likely to be the best available option.
This update of a systematic review evaluated the effectiveness of spinal manipulations as a treatment for migraine headaches.
Amed, Embase, MEDLINE, CINAHL, Mantis, Index to Chiropractic Literature, and Cochrane Central were searched from inception to September 2023. Randomized clinical trials (RCTs) investigating spinal manipulations (performed by various healthcare professionals including physiotherapists, osteopaths, and chiropractors) for treating migraine headaches in human subjects were considered. Other types of manipulative therapy, i.e., cranial, visceral, and soft tissue were excluded. The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was used to evaluate the certainty of evidence.
Three more RCTs were published since our first review; amounting to a total of 6 studies with 645 migraineurs meeting the inclusion criteria. Meta-analysis of six trials showed that, compared with various controls (placebo, drug therapy, usual care), SMT (with or without usual care) has no superior effect on migraine intensity/severity measured with a range of instruments (standardized mean difference [SMD] − 0.22, 95% confidence intervals [CI] − 0.65 to 0.21, very low certainty evidence), migraine duration (SMD − 0.10; 95% CI − 0.33 to 0.12, 4 trials, low certainty evidence), or emotional quality of life (SMD − 14.47; 95% CI − 31.59 to 2.66, 2 trials, low certainty evidence) at post-intervention. A meta-analysis of two trials showed that compared with various controls, SMT (with or without usual care) increased the risk of adverse effects (risk ratio [RR] 2.06; 95% CI 1.24 to 3.41, numbers needed to harm = 6; very low certainty evidence). The main reasons for downgrading the evidence were study limitations (studies judged to be at an unclear or high risk of bias), inconsistency (for pain intensity/severity), imprecision (small sizes and wide confidence intervals around effect estimates) and indirectness (methodological and clinical heterogeneity of populations, interventions, and comparators).
We cocluded that the effectiveness of SMT for the treatment of migraines remains unproven. Future, larger, more rigorous, and independently conducted studies might reduce the existing uncertainties.
The only people who might be surprised by these conclusions are chiropractors who continue to advertise and use SMT to treat migraines. Here are a few texts by chiropractors (many including impressive imagery) that I copied from ‘X’ just now (within less that 5 minutes) to back up this last statement:
- So many people are suffering with Dizziness and migraines and do not know what to do. Upper Cervical Care is excellent at realigning the upper neck to restore proper blood flow and nerve function to get you feeling better!
- Headache & Migraine Relief! Occipital Lift Chiropractic Adjustment
- Are migraines affecting your quality of life? Discover effective chiropractic migraine relief at…
- Neck Pain, Migraine & Headache Relief Chiropractic Cracks
- Migraine Miracle: Watch How Chiropractic Magic Erases Shoulder Pain! Y-Strap Adjustments Unveiled
- Tired of letting migraines control your life? By addressing underlying issues and promoting spinal health, chiropractors can help reduce the frequency and severity of migraines. Ready to experience the benefits of chiropractic for migraine relief?
- Did you know these conditions can be treated by a chiropractor? Subluxation, Back Pain, Chronic Pain, Herniated Disc, Migraine Headaches, Neck Pain, Sciatica, and Sports Injuries.
- When a migraine comes on, there is not much you can do to stop it except wait it out. However, here are some holistic and non-invasive tips and tricks to prevent onset. Check out that last one! In addition to the other tips, chiropractic care may prevent migraines in your future!
Evidence-based chiropractic?
MY FOOT!
To date, two open-label clinical trials have indicated that acupuncture may be more effective than standard medication for chronic migraine. However, drawing definitive conclusions from these trials is challenging. Studies employing a double-dummy design can eliminate the placebo effect and offer more unbiased estimates of efficacy.
This double-dummy, single-blind, randomized controlled trial compared the efficacy and safety of acupuncture and topiramate for chronic migraine. Participants, aged 18–65 years and diagnosed with chronic migraine, were randomly assigned (1:1) to receive:
- acupuncture (three sessions/week) plus topiramate placebo (acupuncture group),
- or topiramate (50–100 mg/day) plus sham acupuncture (topiramate group) over 12 weeks.
The primary outcome was the mean change in monthly migraine days during weeks 1–12.
Of 123 screened patients, 60 (mean age 45.8, 81.7% female) were randomly assigned to the acupuncture or topiramate groups. Acupuncture demonstrated significantly greater reductions in monthly migraine days than topiramate. No severe adverse events were reported.
The authors concluded that acupuncture may be safe and effective for treating chronic migraine. The efficacy of 12 weeks of acupuncture was sustained for 24 weeks and superior to that of topiramate. Acupuncture can be used as an optional preventive therapy for chronic migraine.
I beg to differ!
The authors claim that the participants, outcome assessors, and statistical analysts were blinded (masked) to the group allocations. However, the success of patient blinding was not tested. Why?
The authors state that, in the acupuncture group, “twirling, lifting, and thrusting were performed to produce deqi (a sensation of soreness, numbness, distention, or heaviness that indicates effective needling)… In the topiramate group, sham acupuncture was administered on non-effective acupoints, without manual deqi manipulations.” In other words, patients could very easily tell to which group they had been randomised.
This, in turn, means that a placebo effect – possibly enhanced by verbal or non-verbal communication from the (non-blinded) actupuncturists – has most likely caused the observed outcomes. I therefore feel the need to re-phrase the authors’ conclusions:
This study confirms that acupuncture produces a large placebo effect. Whether it has any effects beyond placebo cannot be determined by this study. Until this point has been clarified, acupuncture should not be used as a preventive therapy for chronic migraine.
NICE helps practitioners and commissioners get the best care to patients, fast, while ensuring value for the taxpayer. Internationally, NICE has a reputation for being reliable and trustworthy. But is that also true for its recommendations regarding the use of acupuncture? NICE currently recommends that patients consider acupuncture as a treatment option for the following conditions:
- chronic (long-term) pain
- chronic tension-type headaches
- migraines
- prostatitis symptoms
- hiccups
Confusingly, on a different site, NICE also recommends acupuncture for retinal migraine, a very specific type of migraine that affect normally just one eye with symptoms such as vision loss lasting up to one hour, a blind spot in the vision, headache, blurred vision and seeing flashing lights, zigzag patterns or coloured spots or lines, as well as feeling nauseous or being sick.
I think this perplexing situation merits a look at the evidence. Here I quote the conclusions of recent, good quality, and (where possible) independent reviews:
- Chronic pain: Acupuncture is efficacious for reducing pain in patients with LBP… Further research needs to be done to evaluate acupuncture’s efficacy in these conditions, especially for abdominal pain, as many of the current studies have a risk of bias due to lack of blinding and small sample size.
- Chronic tension-type headaches (TTH): Acupuncture may be an effective and safe treatment for TTH patients. Due to low or very low certainty of evidence and high heterogeneity, more rigorous RCTs are needed to verify the effect and safety of acupuncture in the management of TTH.
- Migraines: Many studies suggest that acupuncture is a safe, helpful and available alternative therapy that may be beneficial to certain migraine patients. Nevertheless, further large-scale RCTs are warranted to further consolidate these findings and provide further support for the clinical value of acupuncture. Despite previous studies that have analyzed the effects of acupuncture on migraine, there is still a need for further investigation to ensure that the incorporation of acupuncture into migraine treatment management will have a positive outcome on patients.
- Prostatitis: This meta-analysis indicated that acupuncture has measurable benefits on CP/CPPS, and security has also been ensured. However, this meta-analysis only included 10 RCTs; thus, RCTs with a larger sample size and longer-term observation are required to verify the effectiveness of acupuncture further in the future.
- Hiccups: All of these studies sought to determine the effectiveness of different acupuncture techniques in the treatment of persistent and intractable hiccups. All four studies had a high risk of bias, did not compare the intervention with placebo, and failed to report side effects or adverse events for either the treatment or control groups.
- Retinal migraine: no evidence
So, what do we make of this? I think that, on the basis of the evidence:
- a positive recommendation for all types of chromic pain is not warranted;
- a positive recommendation for the treatment of TTH is questionable;
- a positive recommendation for migraine is questionable;
- a positive recommendation for prostatitis is questionable;
- a positive recommendation for hiccups is not warranted;
- a positive recommendation for retinal migraine is not warranted.
But why did NICE issue positive recommendations despite weak or even non-existent evidence?
SEARCH ME!
.
The ‘American Heart Association News’ recently reported the case of a 33-year-old woman who suffered a stroke after consulting a chiropractor. I take the liberty of reproducing sections of this article:
Kate Adamson liked exercising so much, her goal was to become a fitness trainer. She grew up in New Zealand playing golf and later, living in California, she worked out often while raising her two young daughters. Although she was healthy and ate well, she had occasional migraines. At age 33, they were getting worse and more frequent. One week, she had the worst headache of her life. It went on for days. She wasn’t sleeping well and got up early to take a shower. She felt a wave of dizziness. Her left side seemed to collapse. Adamson made her way down to the edge of the tub to rest. She was able to return to bed, where she woke up her husband, Steven Klugman. “I need help now,” she said.
Her next memory was seeing paramedics rushing into the house while her 3-year-old daughter, Stephanie, was in the arms of a neighbor. Rachel, her other daughter, then 18 months old, was still asleep. When she woke up in the hospital, Adamson found herself surrounded by doctors. Klugman was by her side. She could see them, hear them and understand them. But she could not move or react.
Doctors told Klugman that his wife had experienced a massive brain stem stroke. It was later thought to be related to neck manipulations she had received from a chiropractor for the migraines. The stroke resulted in what’s known as locked-in syndrome, a disorder of the nervous system. She was paralyzed except for the muscles that control eye movement. Adamson realized she could answer yes-or-no questions by blinking her eyes.
Klugman was told that Adamson had a very minimal chance of recovery. She was put on a ventilator to breathe, given nutrition through a feeding tube, and had to use a catheter. She learned to coordinate eye movements to an alphabet chart. This enabled her to make short sentences. “Am I going to die?” she asked one of her doctors. “No, we’re going to get you into rehab,” he said.
Adamson stayed in the ICU on life support for 70 days before being transferred to an acute rehabilitation facility. She could barely move a finger, but that small bit of progress gave her hope. In rehab, she slowly started to regain use of her right side; her left side remained paralyzed. Therapists taught her to swallow and to speak. She had to relearn to blow her nose, use the toilet and tie her shoes.
She was particularly fond of a social worker named Amy who would incorporate therapy exercises into visits with her children, such as bubble blowing to help her breathing. Amy, who Adamson became friends with, also helped the children adjust to seeing their mother in a wheelchair.
Adamson changed her dream job from fitness trainer to hospital social worker. She left rehab three and a half months later, still in a wheelchair but able to breathe, eat and use the toilet on her own. She continued outpatient rehab for another year. She assumed her left side would improve as her right side did. But it remained paralyzed. She would need to use a brace on her left leg to walk and couldn’t use her left arm and hand. Still, two years after the stroke, which happened in 1995, Adamson was able to drive with a few equipment modifications…
In 2018, Adamson reached another milestone. She graduated with a master’s degree in social work; she’d started college in 2011 at age 49. “It wasn’t easy going to school. I just had to take it a day at a time, a semester at a time,” she said. “The stroke has taught me I can walk through anything.” …
Now 60, she works with renal transplant and pulmonary patients, helping coordinate their services and care with the rest of the medical team at Vanderbilt University Medical Center. “Knowing that you’re making a difference in somebody’s life is very satisfying. It takes me back to when I was a patient – I’m always looking at how I would want to be treated,” she said. “I’ve really come full circle.”
Adamson has adapted to doing things one-handed in a two-handed world, such as cooking and tying her shoes. She also walks with a cane. To stay in shape, she works with a trainer doing functional exercises and strength training. She has a special glove that pulls her left hand into a fist, allowing her to use a rowing machine and stationary bike….
Adamson is especially determined when it comes to helping her patients. “I work really hard to be an example to them, to show that we are all capable of going through difficult life challenges while still maintaining a positive attitude and making a difference in the world.”
________________________
What can we learn from this story?
Mainly two things, in my view:
- We probably should avoid chiropractors and certainly not allow them to manipulate our necks. I know, chiros will say that the case proves nothing. I agree, it does not prove anything, but the mere suspicion that the lock-in syndrome was caused by a stroke that, in turn, was due to upper spinal manipulation plus the plethora of cases where causality is much clearer are, I think, enough to issue that caution.
- Having been in rehab medicine for much of my early career, I feel it is good to occasionally point out how important this sector often neglected part of healthcare can be. Rehab medicine has been a sensible form of multidisciplinary, integrative healthcare long before the enthusiasts of so-called alternative medicine jumped on the integrative bandwagon.
Migraines are common headache disorders and risk factors for subsequent strokes. Acupuncture has been widely used in the treatment of migraines; however, few studies have examined whether its use reduces the risk of strokes in migraineurs. This study explored the long-term effects of acupuncture treatment on stroke risk in migraineurs using national real-world data.
A team of Taiwanese researchers collected new migraine patients from the Taiwan National Health Insurance Research Database (NHIRD) from 1 January 2000 to 31 December 2017. Using 1:1 propensity-score matching, they assigned patients to either an acupuncture or non-acupuncture cohort and followed up until the end of 2018. The incidence of stroke in the two cohorts was compared using the Cox proportional hazards regression analysis. Each cohort was composed of 1354 newly diagnosed migraineurs with similar baseline characteristics. Compared with the non-acupuncture cohort, the acupuncture cohort had a significantly reduced risk of stroke (adjusted hazard ratio, 0.4; 95% confidence interval, 0.35–0.46). The Kaplan–Meier model showed a significantly lower cumulative incidence of stroke in migraine patients who received acupuncture during the 19-year follow-up (log-rank test, p < 0.001).

The authors concluded that acupuncture confers protective benefits on migraineurs by reducing the risk of stroke. Our results provide new insights for clinicians and public health experts.
After merely 10 minutes of critical analysis, ‘real-world data’ turn out to be real-bias data, I am afraid.
The first question to ask is, were the groups at all comparable? The answer is, NO; the acupuncture group had
- more young individuals;
- fewer laborers;
- fewer wealthy people;
- fewer people with coronary heart disease;
- fewer individuals with chronic kidney disease;
- fewer people with mental disorders;
- more individuals taking multiple medications.
And that are just the variables that were known to the researcher! There will be dozens that are unknown but might nevertheless impact on a stroke prognosis.
But let’s not be petty and let’s forget (for a minute) about all these inequalities that render the two groups difficult to compare. The potentially more important flaw in this study lies elsewhere.
Imagine a group of people who receive some extra medical attention – such as acupuncture – over a long period of time, administered by a kind and caring therapist; imagine you were one of them. Don’t you think that it is likely that, compared to other people who do not receive this attention, you might feel encouraged to look better after your health? Consequently, you might do more exercise, eat more healthily, smoke less, etc., etc. As a result of such behavioral changes, you would be less likely to suffer a stroke, never mind the acupuncture.
SIMPLE!
I am not saying that such studies are totally useless. What often renders them worthless or even dangerous is the fact that the authors are not more self-critical and don’t draw more cautious conclusions. In the present case, already the title of the article says it all:
Acupuncture Is Effective at Reducing the Risk of Stroke in Patients with Migraines: A Real-World, Large-Scale Cohort Study with 19-Years of Follow-Up
My advice to researchers of so-called alternative medicine (SCAM) and journal editors publishing their papers is this: get your act together, learn about the pitfalls of flawed science (most of my books might assist you in this process), and stop misleading the public. Do it sooner rather than later!
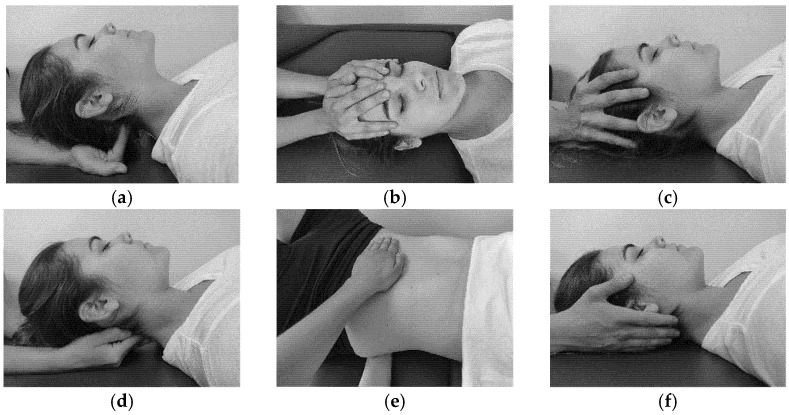
The aim of this study was to evaluate the effectiveness of craniosacral therapy on different features in migraine patients.
Fifty individuals with migraine were randomly divided into two groups (n = 25 per group):
- craniosacral therapy group (CTG),
- sham control group (SCG).
The interventions were carried out with the patient in the supine position. The CTG received a manual therapy treatment focused on the craniosacral region including five techniques, and the SCG received a hands-on placebo intervention. After the intervention, individuals remained supine with a neutral neck and head position for 10 min, to relax and diminish tension after treatment. The techniques were executed by the same experienced physiotherapist in both groups.
The analyzed variables were pain, migraine severity, and frequency of episodes, functional, emotional, and overall disability, medication intake, and self-reported perceived changes, at baseline, after a 4-week intervention, and at an 8-week follow-up.
After the intervention, the CTG significantly reduced pain (p = 0.01), frequency of episodes (p = 0.001), functional (p = 0.001) and overall disability (p = 0.02), and medication intake (p = 0.01), as well as led to a significantly higher self-reported perception of change (p = 0.01), when compared to SCG. The results were maintained at follow-up evaluation in all variables.
The authors concluded that a protocol based on craniosacral therapy is effective in improving pain, frequency of episodes, functional and overall disability, and medication intake in migraineurs. This protocol may be considered as a therapeutic approach in migraine patients.
Sorry, but I disagree!
And I have several reasons for it:
- The study was far too small for such strong conclusions.
- For considering any treatment as a therapeutic approach in migraine patients, we would need at least one independent replication.
- There is no plausible rationale for craniosacral therapy to work for migraine.
- The blinding of patients was not checked, and it is likely that some patients knew what group they belonged to.
- There could have been a considerable influence of the non-blinded therapists on the outcomes.
- There was a near-total absence of a placebo response in the control group.
Altogether, the findings seem far too good to be true.