iridology
Iridology is an assessment technique that involves examining the iris allegedly to identify potential pathological disorders. Despite being practised for centuries, the effectiveness of iris diagnosis as a diagnostic tool remains doubtful, primarily due to limited empirical evidence supporting its claims. Thus, there is a need for scientific studies to test the efficacy of iridology assessment.
This study aimed to determine the sensitivity and specificity of iridology assessment in detecting abnormalities in the female reproductive system.
This cross-sectional observational study included 100 female participants. All participants underwent an iris examination, a clinical assessment, and ultrasonography. The results from these investigations were compared, and sensitivity and specificity rates were calculated using standard formulas.
The study found that iridology assessment demonstrated a sensitivity of 92% and a specificity of 56% in detecting abnormalities within the female reproductive system.
The authors concluded that their findings suggest that iridology assessment may serve as a potentially useful complementary tool for detecting abnormalities in the female reproductive system. However, further research is essential to confirm the effectiveness of this method and to explore its potential benefits and limitations in gynecological diagnosis. Continued scientific investigation is crucial to establish the role of iridology assessment in enhancing gynecological healthcare.
The authors of this study published in “Advances in Integrative Medicine” list the following affiliations:
- Department of Naturopathy, Government Yoga and Naturopathy Medical College, The Tamilnadu Dr. MGR Medical University, Chennai, Tamilnadu, India
- Department of Research, Government Yoga and Naturopathy Medical College, The Tamilnadu Dr. MGR Medical University, Chennai, Tamilnadu, India
- Department of Yoga, Government Yoga and Naturopathy Medical College, The Tamilnadu Dr. MGR Medical University, Chennai, Tamilnadu, India
- Department of Women and Child Care, National Institute of Naturopathy, Pune, Ministry of AYUSH, Government of India, India
I fear that this does not inspire me with confidence. But let’s have a look at the actual study.
The first thing that strikes me is the fact that there are many dozens of abnormalities in the female reproductive system. It seems oddly unscientific that the Indian researchers did not bother to define one single disorder. This gets even weirder when we realize that many of the abnormalities in the female reproductive system are easily recognisable or guessable without any diagnostic procedure upon first encountering the patient.
What I am trying to explain: the iridologists probably used all sorts of clues to guess which group each patient belonged to. In any case, the study is so poorly conceived and described that we really cannot be sure what happened.
But why am I so critical? Perhaps iridology is a useful diagnostic tool after all?
I find this possibility highly unlikely, and here is why:
Iridology was invented by a Hungarian homeopath in the late 19th century who thought to observe changes in the iris of an owl during the recovery of the animal after it had broken a leg. Iridologists believe that the iris is a ‘mirror of our body’. Any relevant abnormality on the right half of the body will reveal itself on the right iris and problems on the left side will show up on the left iris. They assume that the iris is linked via multiple nerve connections to all organs and believe that any bodily malfunction will thus be represented as abnormalities of pigmentation on the iris. These assumptions are not in keeping with basic anatomy or physiology and thus lack plausibility.
Iridologists have produced detailed maps of the iris where each iris is divided in 60 sectors (much like the face of a clock) and each segment is related to an inner organ or bodily function (for instance, heart diseases are thus seen in the left iris somewhere between two and three o’clock). Iridologists either study the iris in situ or they produce high-quality colour photographs of both irides for detailed inspection. Several studies have tested the validity of iridology. My systematic review of these data concluded that “the validity of iridology as a diagnostic tool is not supported by scientific evaluations. Patients and therapists should be discouraged from using this method.”
A final thought: if iridology were a valid diagnostic tool, this would be a scientific sensation, and the study proving it would get published in journals like SCIENCE or NATURE and not in s 3rd class SCAM journal.
I REST MY CASE.
- the safety of oil pulling is assumed but has not actually been tested;
- the cost-effectiveness of oil pulling is assumed but has not actually been tested;
- efficiency means the quality of achieving the largest amount of useful work using as little energy as possible and is meaningless in this context. I suspect the authors meant “effectiveness” which is also wrong because it is not evidence-based.
In case you want an evidence-based text about oil pulling, I refer you to a previous post of mine which, in fact, refers to my book in which the treatement was discussed together with 201 further modalities:
So, what is oil pulling? It is the use of oil for swishing it around your mouth for alleged health benefits. Here are several short points that might explain it more fully:
- Oil pulling is said to have roots that reach back to ancient Hindu texts. Coconut or sesame oils are usually employed for this therapy.
- The mechanism of action (if there is one at all) is poorly understood, and several theories have been put forward:
Alkali hydrolysis of fat results in saponification or “soap making” process. Since the oils used for oil pulling contain fat, the alkali hydrolysis process emulsifies the fat into bicarbonate ions, normally found in the saliva. Soaps then blend in the oil, increase the surface area of the oil, and thus cleanse the teeth and gums.
A second theory suggests that the viscous nature of the oil inhibits plaque accumulation and adhesion of bacteria.
A third theory holds that the antioxidants present in the oil prevent lipid peroxidation, resulting in an antibiotic-like effect helping in the destruction of microorganisms.
- Oil pulling is recommended to be carried out in the morning on an empty stomach. About 10 ml of oil is swished between the teeth for a duration of approximately 15-20 min and spat out. This ritual should be followed by rinsing and tooth brushing. The practice should be repeated regularly, even three times daily for acute diseases.
- To my surprise, oil pulling has been tested in clinical trials. Some of these investigations seem reasonably sound and suggest that coconut oil pulling reduces potentially harmful bacteria in the mouth.[1] This effect has been shown to lead to a reduction in dental plaque formation[2] , halitosis (bad breath) [3] and gingivitis. [4]
- The evidence for these oral effects is by no means strong, but I have not found studies that show negative results.
- Dentists – even the bizarre species of ‘holistic dentists‘ – do not seem to be balled over by oil pulling (some malicious minds might speculate that this is so because they cannot earn much money with it).
- The claimed benefits of oil pulling are, however, not limited to the oral cavity. It is advocated also for the prevention and treatment of conditions such as headaches, migraines, thrombosis, eczema, diabetes and asthma.[5] Some proponents also claim that oil pulling is a detox therapy. Unsurprisingly, none of these claims are supported by good evidence.
- As long as you don’t swallow the oil, there are no serious risks associated with oil pulling.
So, what is the conclusion? To me, the evidence looks promising as far as oral health is concerned. For all other indication, oil pulling is neither plausible nor evidence-based.
[1] https://www.ncbi.nlm.nih.gov/pubmed/27891311
[2] https://www.ncbi.nlm.nih.gov/pubmed/18408265
[3] https://www.ncbi.nlm.nih.gov/pubmed/21911944
According to chiropractic belief, vertebral subluxation (VS) is a clinical entity defined as a misalignment of the spine affecting biomechanical and neurological function. The identification and correction of VS is the primary focus of the chiropractic profession. The purpose of this study was to estimate VS prevalence using a sample of individuals presenting for chiropractic care and explore the preventative public health implications of VS through the promotion of overall health and function.
A brief review of the literature was conducted to support an operational definition for VS that incorporated neurologic and kinesiologic exam components. A retrospective, quantitative analysis of a multi-clinic dataset was then performed using this operational definition.
The operational definition used in this study included:
- (1) inflammation of the C2 (second cervical vertebra) DRG,
- (2) leg length inequality,
- (3) tautness of the erector spinae muscles,
- (4) upper extremity muscle weakness,
- (5) Fakuda Step test,
- radiographic analysis based on the (6) frontal atlas cranium line and (7) horizontal atlas cranium line.
Descriptive statistics on patient demographic data included age, gender, and past health history characteristics. In addition to calculating estimates of the overall prevalence of VS, age- and gender-stratified estimates in the different clinics were calculated to allow for potential variations.
A total of 1,851 patient records from seven chiropractic clinics in four states were obtained. The mean age of patients was 43.48 (SD = 16.8, range = 18-91 years). There were more females (n = 927, 64.6%) than males who presented for chiropractic care. Patients reported various reasons for seeking chiropractic care, including, spinal or extremity pain, numbness, or tingling; headaches; ear, nose, and throat-related issues; or visceral issues. Mental health concerns, neurocognitive issues, and concerns about general health were also noted as reasons for care. The overall prevalence of VS was 78.55% (95% CI = 76.68-80.42). Female and male prevalence of VS was 77.17% and 80.15%, respectively; notably, all per-clinic, age, or gender-stratified prevalences were ≥50%.
The authors concluded that the results of this study suggest a high rate of prevalence of VS in a sample of individuals who sought chiropractic care. Concerns about general health and wellness were represented in the sample and suggest chiropractic may serve a primary prevention function in the absence of disease or injury. Further investigation into the epidemiology of VS and its role in health promotion and prevention is recommended.
This is one of the most hilarious pieces of ‘research’ that I have recently encountered. The strategy is siarmingly simple:
- invent a ficticious pathology (VS) that will earn you plently of money;
- develop criteria that allow you to diagnose this pathology in the maximum amount of consumers;
- show gullible consumers that they are afflicted by this pathology;
- use scare mongering tactics to convince consumers that the pathology needs treating;
- offer a treatment that, after a series of expensive sessions, will address the pathology;
- cash in regularly while this goes on;
- when the consumer has paid enough, declare that your fabulous treatment has done the trick and the consumer is again healthy.
The strategy is well known amongst practitioners of so-called alternative medicine (SCAM), e.g.:
- Traditional acupuncturists diagnose a ficticious imbalance of yin and yang only to normalise it with numerous acupuncture sessions.
- Naturopaths diagnose ficticious intoxications and treat it with various detox measures.
- Iridologists diagnose ficticious abnormalities of the iris that allegedly indicate organ disstress and treat it with whatever SCAM they can offer.
As they say:
No disease can be more surely, effectively, and profitably treated than a condition that the unsuspecting customer did not have in the first place!
PS
Sadly, such behavior exists in convertional medicine occasionally too, but SCAM relies almost entirely on it.
In 2020, a Swedish team published a study investigating what resolutions people make when they are free to formulate them, whether different resolutions reach differing success rates, and whether it is possible to increase the likelihood of a resolution’s success by administering information and exercises on effective goal setting. Participants (N = 1066) from the general public were randomized into three groups:
- active control,
- some support,
- and extended support.
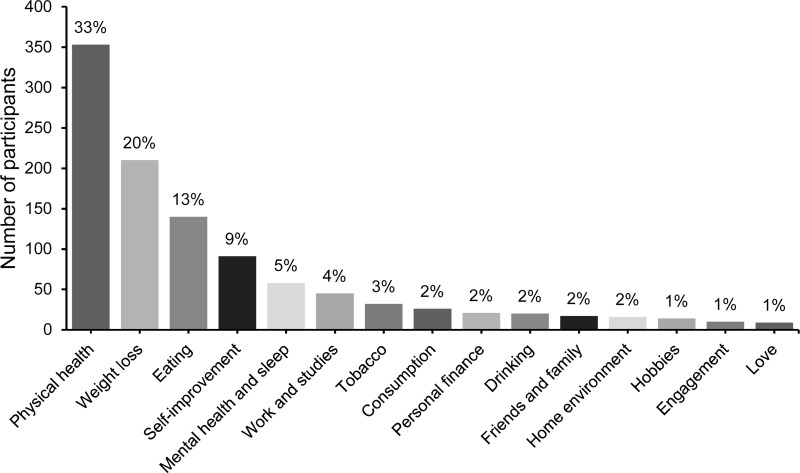
The most popular resolutions regarded physical health, weight loss, and eating habits. At a one-year follow-up, 55% of responders considered themselves successful in sustaining their resolutions. Participants with approach-oriented goals were significantly more successful than those with avoidance-oriented goals (58.9% vs. 47.1%). The group that received some support was exclusively and significantly more successful compared to the other two.
The authors concluded that New Year’s resolutions can have lasting effects, even at a one-year follow-up.
This is a truly interesting study generating a lot of truly boring resolutions.
Boring is, however, something that we must avoid on this blog. In an attempt of doing just this, I decided to lodge my tongue in my cheek and formulate my very own resolutions for 2023 in relation to so-called alternative medicine (SCAM) and this blog. I shall:
- Never again call a comment or a commentator idiotic.
- Never state that chiropractors, homeopaths, osteopaths, naturopaths, or other SCAM practitioners are unethical charlatans.
- Never claim that subluxations, meridians, vital forces, etc. are pure fantasy.
- Never suggest that the assumptions of homeopathy fly in the face of science.
- Never imply that holism, integrative medicine, etc. are just sales gimmicks for crooks to boost their businesses.
- Never again demonstrate that a study is fraudulent just because its findings are too good to be true.
- Never again utter a critical word about our SCAM-loving sovereign, King Charles.
In case you are puzzled by my resolutions, please consider this: contrary to the above-cited evidence, it has been shown that only 12% of people who make new year’s resolutions will actually keep them. And this brings me to my last (and only realistic) resolution for 2023:
8. I shall not feel tempted to adhere to my New Year’s resolutions.
Research into both receptivity to falling for bullshit and the propensity to produce it have recently emerged as active, independent areas of inquiry into the spread of misleading information. However, it remains unclear whether those who frequently produce bullshit are inoculated from its influence. For example, both bullshit receptivity and bullshitting frequency are negatively related to cognitive ability and aspects of analytic thinking style, suggesting that those who frequently engage in bullshitting may be more likely to fall for bullshit. However, separate research suggests that individuals who frequently engage in deception are better at detecting it, thus leading to the possibility that frequent bullshitters may be less likely to fall for bullshit.
Canadian psychologists conducted three studies (N = 826) attempting to distinguish between these competing hypotheses, finding that frequency of persuasive bullshitting (i.e., bullshitting intended to impress or persuade others) positively predicts susceptibility to various types of misleading information and that this association is robust to individual differences in cognitive ability and analytic cognitive style.
This seems to make sense – at least in the contest of so-called alternative medicine (SCAM). Those promoting bullshit are the ones that fall for bullshit.
Think of Prince Charles, for instance. In his book HARMONY and on many other occasions he insists on promoting homeopathy and other SCAM, like for example iridology, osteopathy or detox. He even advocates homeopathy for animals and he proudly tells us that, on his farms, he has instructed the personnel to give his cows homeopathy. Thus he is a good example of someone who is frequently bullshitting with the intend to impress or persuade others while, at the same time, being highly susceptible to various other types of misleading information, such as iridology.
Charles is a good example because we all know about the alternative bee under the royal bonnet. But he is certainly not alone, quite to the contrary. If you look around you, I am sure you will find that there are no end of bullshitters who fall for bullshit. Before bullshit became a term used even in scientific journals, they used to say ‘one can never kid a kidder’, but the new research by the Canadian psychologists seems to suggest that the assumption is not entirely correct.
Black salve is a paste for external use made from a variable mixture of herbal and non-herbal ingredients. It usually contains bloodroot and/or chaparral and/or zinc chloride which are all ingredients that render the products corrosive. This means black salve destroys living cells that come in contact with it.
Black salve is said to originate from native American tribes who used the paste as a treatment for various conditions. It was adopted by conventional medicine during the Victorian era as a treatment for a range of skin problems, including skin cancers. When effective treatments became available, it became obsolete.
Black salve was recently re-discovered by some practitioners of so-called alternative medicine (SCAM) who now recommend it as a natural treatment for various skin conditions, including cancer. Black salve is readily available, for instance, via the Internet. Several national regulators have issued warnings to consumers not to use it. Consumers have little means of telling what is the nature, quality or strength of the black salve they might be purchasing.
No compelling evidence exists that black salve is efficacious for any condition, especially not for any type of skin cancer. Rigorous clinical trials testing its efficacy are not available. A recent review[1] of the published evidence concluded as follows: Black salve is not a natural therapy. It contains significant concentrations of synthetic chemicals. Black salve does not appear to possess tumour specificity with in vitro and in vivo evidence indicating normal cell toxicity. Black salve does appear to cure some skin cancers, although the cure rate for this therapy is currently unknown. The use of black salve should be restricted to clinical research in low risk malignancies located at low risk sites until a better understanding of its efficacy and toxicity is developed. Where a therapy capable of harm is already being used by patients, it is ethically irresponsible not to study and analyse its effects. Although cautionary tales are valuable, black salve research needs to move beyond the case study and into the carefully designed clinical trial arena. Only then can patients be properly informed of its true benefits and hazards.
Due to its erosive nature, black salve burns away the tissue with which it comes into contact. Numerous case reports of the resulting deformations have been published.[2],[3] Many horrendous pictures of patients maimed by their use of black salve are available on the Internet and give a dramatic impression of the harm caused. Black salve is unquestionably a treatment that can cause considerable damage and should be regarded as unsafe. One paper concluded that it is vital that members of the public are aware of the potential effects and toxicity of commercial salve products.[4]
In conclusion, black salve is not of proven efficacy as a treatment of any condition. It is well documented to cause much harm. Its use should be discouraged. Practitioners who employ or recommend it are, in my view, irresponsible to the extreme.
References:
[1] Croaker A, King GJ, Pyne JH, Anoopkumar-Dukie S, Liu L. A Review of Black Salve: Cancer Specificity, Cure, and Cosmesis. Evid Based Complement Alternat Med. 2017;2017:9184034. doi:10.1155/2017/9184034
[2] Ong NC, Sham E, Adams BM. Use of unlicensed black salve for cutaneous malignancy. Med J Aust. 2014;200(6):314. doi:10.5694/mja14.00041
[3] Saltzberg F, Barron G, Fenske N. Deforming self-treatment with herbal “black salve”. Dermatol Surg. 2009;35(7):1152-1154. doi:10.1111/j.1524-4725.2009.01206.x
[4] Lim A. Black salve treatment of skin cancer: a review. J Dermatolog Treat. 2018;29(4):388-392. doi:10.1080/09546634.2017.1395795
Non-validated diagnostic methods, like those in abundant use in alternative medicine, run an unacceptably high risk of producing false positive or false negative diagnoses. The former would be a diagnosis that the patient is, in fact, not suffering from; this enables the charlatan to get rich on treating something that is not even there. The latter would be missing an illness that might even kill the patient. Thus both scenarios are unquestionably harmful.
It is now 21 years ago that I published a review of alternative diagnostic techniques entitled ‘WHICH CRAFT IS WITCHCRAFT?’. Here is the abstract:
The prevalence of complementary medicine in most industrialised countries is impressive and increasing. Discussions of the topic often focus on therapeutic approaches and neglect diagnostic methods specific for complementary medicine. The paper summarises the data available on such “alternative” diagnostics. Scientific evaluations of these are scant, and most techniques have never been properly validated. The ones that have can be demonstrated to be not reproducible, sensitive, or specific. The ones that have not should be regarded as such until shown otherwise by rigorous testing. Therefore it seems that “alternative” diagnostic methods may seriously threaten the safety and health of patients submitted to them. Orthodox doctors should be aware of the problem and inform their patients accordingly.
Exactly 15 years after the publication of this paper, PRINCE CHARLES published his book ‘HARMONY‘ where is covers amongst many other topic also the subject of alternative diagnostics. This is what he tells us about them:
I have also learn from leading experts how we can understand a great deal about the causes of ill health through more traditional methods of diagnosis – for example, through examination of the iris, ears, tongue, feet and pulse, very much the basis of the Indian Ayurvedic system. This is not to say that modern diagnostic techniques do not have a role, but let us not forget what we can gain by using the knowledge and wisdom accumulated over thousands of years by pioneers who did not have access to today’s technology. In fact, an over-reliance can often mean that the subtle signs of imbalance revealed by the examination of the eyes, pulse and tongue are totally missed. Including the fruits of such knowledge, gleaned over 8 000 years of studying the relationship of the human body to the rest of Nature and to the Universe, can but only provide an extra, valuable resource to doctors as they seek to make a full diagnosis. Why persist in denying the immense value of such accumulated wisdom when it can tell us so much about the whole person – mind, body and spirit? Employing the best of the ancient and modern in a truly integrated way is another example of harmony and balance at work.
Charles is talking here about iridology, amongst other methods. Iridologists try to diagnose disease or susceptibility to disease by analysing the colour pattern of a patient’s iris. It happens to be a technique that has repeatedly been put to the test. In 1999, I published a systematic review of the evidence and concluded that the validity of iridology as a diagnostic tool is not supported by scientific evaluations. Patients and therapists should be discouraged from using this method.
Given that the evidence for alternative diagnostic techniques is either negative or absent, why does the heir to the throne advocate using them? Does he not know that he has considerable influence and endangers the health of those who believe him? Why does he call this nonsense valuable? The answer probably is that he does not know better.
There is nothing wrong with Charles’ ignorance, of course. He is not a medic (if he were, his quackery might get him struck off the register!) and does not need to know such things! But, if he is ignorant about certain technicalities, should he write about them? At the very least, when giving such concrete medical advice about diagnostic methods, should he not recruit the expertise of people who do know about such matters?
In Charles’ defence, I should mention that apparently he did ask several physicians for help with his book. Two of those who he acknowledged in HARMONY have been mentioned on this blog before: Mosaraf Ali and Michael Dixon.
I MIGHT BE MISTAKEN, BUT IT SEEMS TO ME THAT CHARLES IS NOT JUST IGNORANT ABOUT MEDICINE BUT ALSO ABOUT THE ART OF CHOOSING EXPERTS.
We used to call it ‘alternative medicine’ (on this blog, I still do so, because I believe it is a term as good or bad as any other and it is the one that is easily recognised); later some opted for ‘complementary medicine’; since about 15 years a new term is en vogue: INTEGRATED MEDICINE (IM).
Supporters of IM are adamant that IM is not synonymous with the other terms. But how is IM actually defined?
One of IM’s most prominent defenders is, of course Prince Charles. In his 2006 address to the WHO, he explained: “We need to harness the best of modern science and technology, but not at the expense of losing the best of what complementary approaches have to offer. That is integrated health – it really is that simple.”
Perhaps a bit too simple?
There are several more academic definitions, and it seems that, over the years, IM-fans have been busy moving the goal post quite a bit. The original principle of ‘THE BEST OF BOTH WORLDS’ has been modified considerably.
- IM is a “comprehensive, primary care system that emphasizes wellness and healing of the whole person…” [Arch Intern Med. 2002;162:133-140]
- IM “views patients as whole people with minds and spirits as well as bodies and includes these dimensions into diagnosis and treatment.” [BMJ. 2001; 322:119-120]
During my preparations for my lecture at the 16th European Sceptics Congress in London last week (which was on the subject of IM), I came across a brand-new (September 2015) definition. It can be found on the website of the COLLEGE OF MEDICINE This Michael Dixon-led organisation can be seen as the successor of Charles’ ill-fated FOUNDATION FOR INTEGRATED HEALTH; it was originally to be called COLLEGE FOR INTEGRATED MEDICINE. We can therefore assume that they know best what IM truly is or aspires to be. The definition goes as follows:
IM is a holistic, evidence-based approach which makes intelligent use of all available therapeutic choices to achieve optimal health and resilience for our patients.
This may sound good to many who are not bothered or unable to think critically. It oozes political correctness and might therefore even impress some politicians. But, on closer scrutiny, it turns out to be little more than offensive nonsense. I feel compelled to publish a short analysis of it. I will do this by highlighting and criticising the important implications of this definition one by one.
1) IM is holistic
Holism has always been at the core of any type of good health care. To state that IM is holistic misleads people into believing that conventional medicine is not holistic. It also pretends that medicine might become more holistic through the addition of some alternative modalities. Yet I cannot imagine anything less holistic than diagnosing patients by merely looking at their iris (iridology) or assuming all disease stems from subluxations of the spine (chiropractic), for example. This argument is a straw-man, if there ever was one.
2) IM is evidence-based
This assumption is simply not true. If we look what is being used under the banner of IM, we find no end of treatments that are not supported by good evidence, as well as several for which the evidence is squarely negative.
3) IM is intelligent
If it were not such a serious matter, one could laugh out loud about this claim. Is the implication here that conventional medicine is not intelligent?
4) IM uses all available therapeutic choices
This is the crucial element of this definition which allows IM-proponents to employ anything they like. Do they seriously believe that patients should have ALL AVAILABLE treatments? I had thought that responsible health care is about applying the most effective therapies for the condition at hand.
5) IM aims at achieving optimal health
Another straw-man; it implies that conventional health care professionals do not want to restore their patients to optimal health.
In my lecture, which was not about this definition but about IM in general, I drew the following six conclusions:
- Proponents of IM mislead us with their very own, nonsensical terminology and definitions.
- They promote two main principles: use of quackery + holism.
- Holism is at the heart of all good medicine; IM is at best an unnecessary distraction.
- Using holism to promote quackery is dishonest and counter-productive.
- The integration of quackery will render healthcare not better but worse.
- IM flies in the face of common sense and medical ethics; it is a disservice to patients.
Ignaz von Peczely (1826-1911), a Hungarian physician, got the idea for iridology (or iris-diagnosis) more than a century ago, after seeing streaks in the iris of a man he was treating for a broken leg, and similar phenomena the iris of an owl whose leg von Peczely had broken many years before. He subsequently became convinced that his method was able to distinguish between healthy organs and those that are overactive, inflamed, or distressed. Iridology became internationally known when US chiropractors began adopting this method in their clinical practice. In the United States, most insurance programs do not cover iridology but, in some European countries, they often do. In Germany, for instance, 80% of the Heilpraktiker (non-medically qualified health practitioners) practice iridology.
Iridologists claim to be able to diagnose the health status of an individual, medical conditions or predispositions to disease through abnormalities of pigmentation in the iris. The popularity of iridology renders it necessary to ask whether this method is valid.
The aim of my systematically review from 1999 was to critically evaluate all available, reliable tests of iridology as a diagnostic tool. Four case control studies were included; these are investigations where iridologists are asked to tell by looking at the iris of individuals whether that person does or does not have a certain condition. The majority of these studies suggested that iridology is not a valid diagnostic method. Back then, I concluded that “the validity of iridology as a diagnostic tool is not supported by scientific evaluations. Patients and therapists should be discouraged from using this method.”
Since the publication of my article, several further studies have emerged:
One German team conducted a study investigating the applicability of iridology as a screening method for colorectal cancer. Digital color slides were obtained from both eyes of 29 patients with histologically diagnosed colorectal cancer and from 29 age- and gender-matched healthy control subjects. The slides were presented in random order to acknowledged iridologists without knowledge of the number of patients in the two categories. The iridologists correctly detected 51.7% and 53.4%, respectively, of the patients’ slides; therefore, the likelihood was statistically no better than chance. Sensitivity was, respectively, 58.6% and 55.2%, and specificity was 44.8% and 51.7%. The authors’ conclusion was blunt: “Iridology had no validity as a diagnostic tool for detecting colorectal cancer in this study.”
A study from South Africa aimed to determine the efficacy of iridology in the identification of moderate to profound sensorineural hearing loss in adolescents. A controlled trial was conducted with an iridologist, blind to the actual hearing status of participants, analysing the irises of participants with and without hearing loss. Fifty hearing impaired and fifty normal hearing subjects, between the ages of 15 and 19 years, controlled for gender, participated in the study. An experienced iridologist analysed the randomised set of participants’ irises. A 70% correct identification of hearing status was obtained with a false negative rate of 41% compared to a 19% false positive rate. The respective sensitivity and specificity rates therefore were 59% and 81%. The authors of this investigation concluded that “iridological analysis of hearing status indicated a statistically significant relationship to actual hearing status (P < 0.05). Although statistically significant sensitivity and specificity rates for identifying hearing loss by iridology were not comparable to those of traditional audiological screening procedures.”
A further German study investigated the value of iridology as a diagnostic tool in detecting some common cancers. One hundred ten subjects were enrolled; 68 subjects had histologically proven cancers of the breast, ovary, uterus, prostate, or colorectum, and 42 were cancer-free controls. All subjects were examined by an experienced practitioner of iridology, who was unaware of their medical details. He was allowed to suggest up to five diagnoses for each subject and his results were then compared with each subject’s medical diagnosis to determine the accuracy of iridology in detecting malignancy. Iridology identified the correct diagnosis in only 3 cases (sensitivity, 0.04). The authors concluded that “iridology was of no value in diagnosing the cancers investigated in this study.”
Based on these results it is impossible, I think, to claim that iridology is a valid or useful diagnostic tool. As there is no anatomical or physiological basis for its assumptions, iridology is not biologically plausible. Furthermore, the available clinical evidence does not support its validity as a diagnostic tool. In other words, iridology is bogus. This statement is in sharp contract to the information consumers receive about the method on uncounted websites, books, articles, etc. One website picked at random provides the following information:
The iris reveals changing conditions of every part and organ of the body. Every organ and part of the body is represented in the iris in a well defined area. In addition, through various marks, signs, and discoloration in the iris, nature reveals inherited weaknesses and strengths.
By means of this art / science, an iridologist (one who studies the coloration and fiber structure of the eye) can tell an individual his/her inherited and acquired tendencies towards health and disease, his current condition in general, and the state of every organ in particular.
Iridology cannot detect a specific disease, but, can tell an individual if they have over or under activity in specific areas of the body. For example, an under-active pancreas might indicate a diabetic condition.
Another source claims:
The underlying platform of iridology is that that eyes act as a ‘window’ to a person’s health & well being. This ‘window’ enables the practitioner to see whether areas or organs within the body are healthy, inflamed or ‘over active’. It also enables them to assess a person’s past/ possible future health problems & consider if the patient has a susceptibility to certain diseases. It is important to understand that iridology is simply a method of diagnosis & analysis.
You may well think that none of this really matters. Who cares whether iridology is bogus or not! I would argue that it does matter. Bogus methods cost money that could be better spent elsewhere. More importantly, false positive and false negative diagnoses generated by bogus diagnostic methods can put lives at risk.
But there is a more general and perhaps more crucial point here: alternative medicine is an area where people far too easily get away with ignoring the published evidence and scientific consensus. In the last two decades, I have seen many alternative modalities getting scientifically dis-proven; not in a single such instance can I remember that the corresponding alternative practitioners and their professional organisations took any notice of this fact, and not once did I notice that their practice had changed.
If research is systematically ignored, it becomes a useless appendix. More importantly, progress is then stifled to the detriment of all our best interests.