Monthly Archives: July 2018
I have written about the ethics of pharmacists selling homeopathic preparations pretending they are effective medicines often – not just on this blog, but also in medical journals (see for instance here and here) and in our recent book. So, maybe I should give it a rest?
No!
I believe that the issue is far too important not to remain silent about it.
A recent article in the ‘Australian Journal of pharmacy’ caught my eye. As it makes a new and relevant point, I will quote some short excerpts for you:
One of the greatest criticisms pharmacists face is the ranging of homeopathic products in pharmacies. It is difficult to deny that ranging homeopathic products provides a level of legitimacy to these products that they do not deserve.
Conclusive evidence now exists [1] that homeopathy does not work. This is different from a lack of evidence for an effect; this is specific evidence that shows that this modality cannot and does not provide any of the purported benefits or mechanisms of action.
This evidence for lack of effect is important, due to the ethical responsibilities of pharmacists to provide evidence-based medicine. Specifically, from the Pharmaceutical Society of Australia’s Code of Ethics [2]:
Care Principle 1 g)
Before recommending a therapeutic product, considers available evidence and supports the patient to make an informed choice and only supplies a product when satisfied that it is appropriate and the person understands how to use it correctly.
It is not possible to adhere to this principle while also selling homeopathic and other non-EBM products – it is incumbent on pharmacists to always notify a patient that homeopathic medicines cannot work. Ranging homeopathic products therefore opens a pharmacist up to conflict of interest, where their professional judgement tells them that there is no benefit to a product, yet a patient wishes to purchase it anyway, even when advised not to. Not ranging a product is the only method of preventing this conflict.
Pharmacists may also find themselves in position where the pharmacy they work in ranges homeopathic or other non-EBM products, yet they do not want to be involved in the sale or recommendation of these products. In this situation, it is important to remember that the code of ethics requires that a pharmacist does not undertake any action or role if their judgement determines that this is not the correct course of action.
Integrity Principle 2
A pharmacist only practises under conditions which uphold the professional independence, judgement and integrity of themselves and others.
Professional misconduct
This leads to the professional risk a pharmacist puts themselves in when recommending or selling a product that lacks evidence … any breach of the code of ethics can be the basis of a report to the Pharmacy Board for professional misconduct. If a pharmacist were to be referred to the Pharmacy Board for recommending a non-EBM product, pharmacists will be put in the position of having to justify their decision to supply a product that has no evidence, especially if this supply harms a patient or delays them from accessing effective treatment. In addition, it will not be possible to make a case defending the decision to supply non-EBM products based on pressures from employers wishes, due to Integrity Principle 2.
Clearly, the use of Non-EBM products, including homeopathy, puts consumers at risk due to delayed treatment and the risk of unexpected outcomes. It also puts pharmacists at risk of professional and ethical reprimand. Relying on evidence, and having a working knowledge of how to access and assess this evidence, remains a critical part of the role of pharmacists in all areas of practice.
[1] https://www.nhmrc.gov.au/guidelines-publications/cam02
[2] https://www.psa.org.au/downloads/codes/PSA-Code-of-Ethics-2017.pdf
END OF QUOTE
I find this comment important: we all knew (and I have dwelled on it repeatedly) that pharmacists can put consumers at risk when they sell homeopathic remedies masquerading as medicines (while in truth they are placebos that cure absolutely nothing). What few people so far appreciated, I think, is the fact that pharmacists also put themselves at risk.
Of course, you might say, this is a view from Australia, and it might not apply elsewhere. But I think, because the codes of ethics differ only marginally from country to country, it might well apply everywhere. If that is so, pharmacists across the globe – most of them do sell homeopathics regularly – are in danger of breaking their own codes of ethics, if they recommend or sell homeopathic products. And violating professional ethics must mean that pharmacists are vulnerable to reprimands.
Perhaps we should all go to our next pharmacy, ask for some advice about homeopathy, and test this hypothesis!
The Royal College of Chiropractors (RCC), a Company Limited by guarantee, was given a royal charter in 2013. It has following objectives:
- to promote the art, science and practice of chiropractic;
- to improve and maintain standards in the practice of chiropractic for the benefit of the public;
- to promote awareness and understanding of chiropractic amongst medical practitioners and other healthcare professionals and the public;
- to educate and train practitioners in the art, science and practice of chiropractic;
- to advance the study of and research in chiropractic.
In a previous post, I pointed out that the RCC may not currently have the expertise and know-how to meet all these aims. To support the RCC in their praiseworthy endeavours, I therefore offered to give one or more evidence-based lectures on these subjects free of charge.
And what was the reaction?
Nothing!
This might be disappointing, but it is not really surprising. Following the loss of almost all chiropractic credibility after the BCA/Simon Singh libel case, the RCC must now be busy focussing on re-inventing the chiropractic profession. A recent article published by RCC seems to confirm this suspicion. It starts by defining chiropractic:
“Chiropractic, as practised in the UK, is not a treatment but a statutorily-regulated healthcare profession.”
Obviously, this definition reflects the wish of this profession to re-invent themselves. D. D. Palmer, who invented chiropractic 120 years ago, would probably not agree with this definition. He wrote in 1897 “CHIROPRACTIC IS A SCIENCE OF HEALING WITHOUT DRUGS”. This is woolly to the extreme, but it makes one thing fairly clear: chiropractic is a therapy and not a profession.
So, why do chiropractors wish to alter this dictum by their founding father? The answer is, I think, clear from the rest of the above RCC-quote: “Chiropractors offer a wide range of interventions including, but not limited to, manual therapy (soft-tissue techniques, mobilisation and spinal manipulation), exercise rehabilitation and self-management advice, and utilise psychologically-informed programmes of care. Chiropractic, like other healthcare professions, is informed by the evidence base and develops accordingly.”
Many chiropractors have finally understood that spinal manipulation, the undisputed hallmark intervention of chiropractors, is not quite what Palmer made it out to be. Thus, they try their utmost to style themselves as back specialists who use all sorts of (mostly physiotherapeutic) therapies in addition to spinal manipulation. This strategy has obvious advantages: as soon as someone points out that spinal manipulations might not do more good than harm, they can claim that manipulations are by no means their only tool. This clever trick renders them immune to such criticism, they hope.
The RCC-document has another section that I find revealing, as it harps back to what we just discussed. It is entitled ‘The evidence base for musculoskeletal care‘. Let me quote it in its entirety:
The evidence base for the care chiropractors provide (Clar et al, 2014) is common to that for physiotherapists and osteopaths in respect of musculoskeletal (MSK) conditions. Thus, like physiotherapists and osteopaths, chiropractors provide care for a wide range of MSK problems, and may advertise that they do so [as determined by the UK Advertising Standards Authority (ASA)].
Chiropractors are most closely associated with management of low back pain, and the NICE Low Back Pain and Sciatica Guideline ‘NG59’ provides clear recommendations for managing low back pain with or without sciatica, which always includes exercise and may include manual therapy (spinal manipulation, mobilisation or soft tissue techniques such as massage) as part of a treatment package, with or without psychological therapy. Note that NG59 does not specify chiropractic care, physiotherapy care nor osteopathy care for the non-invasive management of low back pain, but explains that: ‘mobilisation and soft tissue techniques are performed by a wide variety of practitioners; whereas spinal manipulation is usually performed by chiropractors or osteopaths, and by doctors or physiotherapists who have undergone additional training in manipulation’ (See NICE NG59, p806).
The Manipulative Association of Chartered Physiotherapists (MACP), recently renamed the Musculoskeletal Association of Chartered Physiotherapists, is recognised as the UK’s specialist manipulative therapy group by the International Federation of Orthopaedic Manipulative Physical Therapists, and has approximately 1100 members. The UK statutory Osteopathic Register lists approximately 5300 osteopaths. Thus, collectively, there are approximately twice as many osteopaths and manipulating physiotherapists as there are chiropractors currently practising spinal manipulation in the UK.
END OF QUOTE
To me this sounds almost as though the RCC is saying something like this:
- We are very much like physiotherapists and therefore all the positive evidence for physiotherapy is really also our evidence. So, critics of chiropractic’s lack of sound evidence-base, get lost!
- The new NICE guidelines were a real blow to us, but we now try to spin them such that consumers don’t realise that chiropractic is no longer recommended as a first-line therapy.
- In any case, other professions also occasionally use those questionable spinal manipulations (and they are even more numerous). So, any criticism of spinal manipulation should not be directed at us but at physios and osteopaths.
- We know, of course, that chiropractors treat lots of non-spinal conditions (asthma, bed-wetting, infant colic etc.). Yet we try our very best to hide this fact and pretend that we are all focussed on back pain. This avoids admitting that, for all such conditions, the evidence suggests our manipulations to be worst than useless.
Personally, I find the RCC-strategy very understandable; after all, the RCC has to try to save the bacon for UK chiropractors. Yet, it is nevertheless an attempt at misleading the public about what is really going on. And even, if someone is sufficiently naïve to swallow this spin, one question emerges loud and clear: if chiropractic is just a limited version of physiotherapy, why don’t we simply use physiotherapists for back problems and forget about chiropractors?
(In case the RCC change their mind and want to listen to me elaborating on these themes, my offer for a free lecture still stands!)
 I am sure we have all seen these colourful tapes that nowadays decorate the bodies of many of our sporting heroes. The tape is supposed to be good for athletic performance – but not just that, it is also promoted for all sorts of health conditions, for instance, low back pain.
I am sure we have all seen these colourful tapes that nowadays decorate the bodies of many of our sporting heroes. The tape is supposed to be good for athletic performance – but not just that, it is also promoted for all sorts of health conditions, for instance, low back pain.
But is it worth the considerable investment?
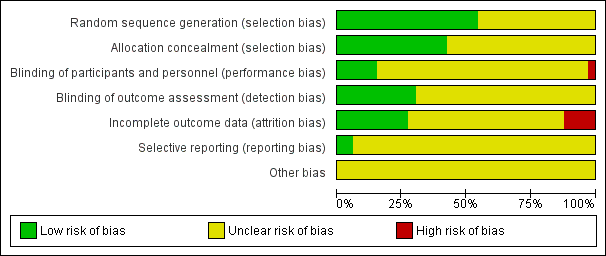
This systematic review investigated the effectiveness of ‘Kinesiology Tape’ (KT) for patients with non-specific low back pain.
The researchers included all randomized controlled trials (RCTs) in adults with chronic non-specific low back pain that compared KT to no intervention or placebo as well as RCTs that compared KT combined with exercise against exercise alone. The methodological quality and statistical reporting of the eligible trials were measured by the 11-item PEDro scale. The quality of the evidence was assessed using the GRADE classification. Pain intensity and disability were the primary outcomes. Whenever possible, the data were pooled through meta-analysis.
 Eleven RCTs were included in this systematic review. Two clinical trials compared KT to no intervention at the short-term follow-up. Four studies compared KT to placebo at short-term follow-up and two trials compared KT to placebo at intermediate-term follow-up. Five trials compared KT combined with exercises or electrotherapy to exercises or spinal manipulation alone. No statistically significant difference was found for most comparisons.
Eleven RCTs were included in this systematic review. Two clinical trials compared KT to no intervention at the short-term follow-up. Four studies compared KT to placebo at short-term follow-up and two trials compared KT to placebo at intermediate-term follow-up. Five trials compared KT combined with exercises or electrotherapy to exercises or spinal manipulation alone. No statistically significant difference was found for most comparisons.
The authors concluded that very low to moderate quality evidence shows that KT was no better than any other intervention for most the outcomes assessed in patients with chronic non-specific low back pain. We found no evidence to support the use of KT in clinical practice for patients with chronic non-specific low back pain.
So, is KT worth the often considerable investment for patients with back trouble?
Or is the current popularity of KT more of a triumph of clever marketing over scientific evidence?
I let you answer this one.
Needle acupuncture in small children is controversial, not least because the evidence that it works is negative or weak, and because small children are unable to consent to the treatment. Yet it is recommended by some acupuncturists for infant colic. This, of course, begs the questions:
- Does the best evidence tell us that acupuncture is effective for infant colic?
- Are acupuncturists who recommend acupuncture for this condition responsible and ethical?
This systematic review and a blinding-test validation based on individual patient data from randomised controlled trials was aimed to assess its efficacy for treating infantile colic. Primary end-points were crying time at mid-treatment, at the end of treatment and at a 1-month follow-up. A 30-min mean difference (MD) in crying time between acupuncture and control was predefined as a clinically important difference. Pearson’s chi-squared test and the James and Bang indices were used to test the success of blinding of the outcome assessors [parents].
The investigators included three randomised controlled trials with data from 307 participants. Only one of the included trials obtained a successful blinding of the outcome assessors in both the acupuncture and control groups. The MD in crying time between acupuncture intervention and no acupuncture control was -24.9 min at mid-treatment, -11.4 min at the end of treatment and -11.8 min at the 4-week follow-up. The heterogeneity was negligible in all analyses. The statistically significant result at mid-treatment was lost when excluding the apparently unblinded study in a sensitivity analysis: MD -13.8 min. The registration of crying during treatment suggested more crying during acupuncture.
The authors concluded that percutaneous needle acupuncture treatments should not be recommended for infantile colic on a general basis.
The authors also provide this further comment: “Our blinding test validated IPD meta-analysis of minimal acupuncture treatments of infantile colic did not show clinically relevant effects in pain reduction as estimated by differences in crying time between needle acupuncture intervention and no acupuncture control. Analyses indicated that acupuncture treatment induced crying in many of the children. Caution should therefore be exercised in recommending potentially painful treatments with uncertain efficacy in infants. The studies are few, the analysis is made on small samples of individuals, and conclusions should be considered in this context. With this limitation in mind, our findings do not support the idea that percutaneous needle acupuncture should be recommended for treatment of infantile colic on a general basis.”
So, returning to the two questions that I listed above – what are the answers?
I think they must be:
- No.
- No.
Most people probably think of acupuncture as being used mainly as a therapy for pain control. But acupuncture is currently being promoted (and has traditionally been used) for all sorts of conditions. One of them is stroke. It is said to speed up recovery and even improve survival rates after such an event. There are plenty of studies on this subject, but their results are far from uniform. What is needed in this situation, is a rigorous summary of the evidence.
The authors of this Cochrane review wanted to assess whether acupuncture could reduce the proportion of people suffering death or dependency after acute ischaemic or haemorrhagic stroke. They included all randomized clinical trials (RCTs) of acupuncture started within 30 days after stroke onset. Acupuncture had to be compared with placebo or sham acupuncture or open control (no placebo) in people with acute ischaemic or haemorrhagic stroke, or both. Comparisons were made versus (1) all controls (open control or sham acupuncture), and (2) sham acupuncture controls.
The investigators included 33 RCTs with 3946 participants. Outcome data were available for up to 22 trials (2865 participants) that compared acupuncture with any control (open control or sham acupuncture) but for only 6 trials (668 participants) comparing acupuncture with sham acupuncture.
When compared with any control (11 trials with 1582 participants), findings of lower odds of death or dependency at the end of follow-up and over the long term (≥ three months) in the acupuncture group were uncertain and were not confirmed by trials comparing acupuncture with sham acupuncture. In trials comparing acupuncture with any control, findings that acupuncture was associated with increases in the global neurological deficit score and in the motor function score were uncertain. These findings were not confirmed in trials comparing acupuncture with sham acupuncture.Trials comparing acupuncture with any control showed little or no difference in death or institutional care or death at the end of follow-up.The incidence of adverse events (eg, pain, dizziness, faint) in the acupuncture arms of open and sham control trials was 6.2% (64/1037 participants), and 1.4% of these patients (14/1037 participants) discontinued acupuncture. When acupuncture was compared with sham acupuncture, findings for adverse events were uncertain.
The authors concluded that this updated review indicates that apparently improved outcomes with acupuncture in acute stroke are confounded by the risk of bias related to use of open controls. Adverse events related to acupuncture were reported to be minor and usually did not result in stopping treatment. Future studies are needed to confirm or refute any effects of acupuncture in acute stroke. Trials should clearly report the method of randomization, concealment of allocation, and whether blinding of participants, personnel, and outcome assessors was achieved, while paying close attention to the effects of acupuncture on long-term functional outcomes.
This Cochrane review seems to be thorough, but it is badly written (Cochrane reviewers: please don’t let this become the norm!). It contains some interesting facts. The majority of the studies came from China. This review confirmed the often very poor methodological quality of acupuncture trials which I have frequently mentioned before.
In particular, the RCTs originating from China were amongst those that most overtly lacked rigor, also a fact that has been discussed regularly on this blog.
For me, by far the most important finding of this review is that studies which at least partly control for placebo effects fail to show positive results. Depending on where you stand in the never-ending debate about acupuncture, this could lead to two dramatically different conclusions:
- If you are a believer in or earn your living from acupuncture, you might say that these results suggest that the trials were in some way insufficient and therefore they produced false-negative results.
- If you are a more reasonable observer, you might feel that these results show that acupuncture (for acute stroke) is a placebo therapy.
Regardless to which camp you belong, one thing seems to be certain: acupuncture for stroke (and other indications) is not supported by sound evidence. And that means, I think, that it is not responsible to use it in routine care.
In the comment section of a recent post, we saw a classic example of the type of reasoning that many alternative practitioners seem to like. In order to offer a service to other practitioners, I will elaborate on it here. The reasoning roughly follows these simple 10 steps:
- My treatment works.
- My treatment requires a lot of skills, training and experience.
- Most people fail to appreciate how subtle my treatment really is.
- In fact, only few practitioners manage do it the way it has to be done.
- The negative trials of my treatment are false-negative because they were conducted by incompetent practitioners.
- In any case, for a whole range of reasons, my treatment cannot be pressed into the straight jacket of a clinical trial.
- My treatment is therefore not supported by the type of evidence people who don’t understand it insist upon.
- Therefore, we have to rely on the best evidence that is available to date.
- And that clearly is the experience of therapists and patients.
- So, the best evidence unquestionably confirms that my treatment works.
The case I mentioned above was that of an acupuncturist defending his beloved acupuncture. To a degree, the argument put forward by him sounded (to fellow acupuncturists) reasonable. On closer inspection, however, they seem far less so, perhaps even fallacious. If you are an acupuncturist, you will, of course, disagree with me. Therefore, I invite all acupuncturists to imagine a homeopath arguing in that way (which they often do). Would you still find the line of arguments reasonable?
And what, if you are a homeopath? Then I invite you to imagine that a crystal therapist argues in that way (which they often do). Would you still find the line of arguments reasonable?
And what, if you are a crystal therapist? …
I am not getting anywhere, am I?
To make my point, it might perhaps be best, if I created my very own therapy!
Here we go: it’s called ENERGY PRESERVATION THERAPY (EPT).
I have discovered, after studying ancient texts from various cultures, that the vital energy of our closest deceased relatives can be transferred by consuming their carbon molecules. The most hygienic way to achieve this is to have our deceased relatives cremated and consume their ashes afterwards. The cremation, storage of the ashes, as well as their preparation and regular consumption all have to be highly individualised, of course. But I am certain that this is the only way to preserve their vital force and transfer it to a living relative. The benefits of this treatment are instantly visible.
As it happens, I run special three-year (6 years part-time) courses at the RSM in London to teach other clinicians how exactly to do this. And I should warn you: they are neither cheap nor easy; we are talking of very skilled stuff here.
What! You doubt that my treatment works?
Doubt no more!
Here are 10 convincing arguments for it:
- EPT works, I have 10 years of experience and seen hundreds of cases.
- EPT requires a lot of skills, training and experience.
- Most people fail to appreciate how subtle EPT really is.
- In fact, only few practitioners manage do EPT the way it has to be done.
- The negative trials of EPT are false-negative because they were conducted by incompetent practitioners.
- In any case, for a whole range of reasons, EPT cannot be pressed into the straight jacket of a clinical trial.
- EPT is therefore not supported by the type of evidence people who don’t understand it insist upon.
- Therefore, we have to rely on the best evidence that is available to date.
- And that clearly is the experience of therapists and patients.
- So, the best evidence unquestionably confirms that EPT works.
Convinced?
No?
You do surprise me!
Why then are you convinced of the effectiveness of acupuncture, homeopathy, etc?
“Homeopathic remedies are inherently harmless” this is what many seem to think – homeopathy friends and foes alike. After all, they contain nothing – so, how can it cause harm?
The notion is, of course, not entirely true. Homeopathic remedies can be directly harmful, if:
- they are not highly dilute (low potency) – imagine Arsenic C1;
- they are contaminated with harmful substances – this might happen with poor quality control during the manufacturing process;
- they might not be as dilute as advertised – this too might happen with poor quality control during the manufacturing process.
A reminder that these are not merely theoretical considerations was just published in the shape of a press-release by the US Food and Drug Administration:
King Bio is voluntarily recalling four lots of Aquaflora Candida HP9, Lymph Detox, and Baby Teething liquids to the consumer level. During a routine inspection by the U.S. Food and Drug Administration, the products were found to contain microbial contaminants Pseudomonas Brenneri, Pseudomonas Fluroescens and Burkholderia Multivorans.
Administration or use of drug products with microbial contamination could potentially result in increased infections that may require medical intervention, and could result in infections that could be life threatening to certain individuals. King Bio has not received reports of injury or illness.
The Aquaflora HP9 product is used as a Candida control product. The Lymph Detox product is used for symptoms associated with lymphatic toxicity. The Baby Teething product is used for symptoms of teething pain, irritated gums, delayed teething, etc.
| Product | UPC | Lot Numbers | Expiration Date | Distribution |
|---|---|---|---|---|
| Aquaflora Candida HP9 8 oz. liquid in a carton |
3-57955-80018-7 | 120217R 102017C 101017G 111417C |
12/02/19 10/20/19 10/10/19 11/14/19 |
8,000 bottles nationwide to retail stores and websites |
| King Bio Lymph Detox 2 oz. liquid in a carton |
3-57955-50632-4 | 010118BE | 01/01/20 | 276 bottles nationwide to retail stores and websites |
| King Bio Baby Teething 2 oz liquid in a carton |
020118F | 13 bottles marked NOT FOR RESALE |
King Bio is notifying its distributors and customers by letter and is arranging for return and/or replacement. of all recalled products. Consumers/distributors/retailers that have product which is being recalled should stop using/and contact King Bio prior to returning the product.
Consumers with questions regarding this recall can contact King Bio by 866-298-2740 or e-mail [email protected], Monday – Friday 830am – 430pm, EST. Consumers should contact their physician or healthcare provider if they have experienced any problems that may be related to taking or using this product.
Adverse reactions or quality problems experienced with the use of this product may be reported to the FDA’s MedWatch Adverse Event Reporting program either online, by regular mail or by fax.
- Complete and submit the report Online: http://www.fda.gov/medwatch/report.htm
- Regular Mail or Fax: Download form http://www.fda.gov/MedWatch/getforms.htm or call 1-800-332-1088 to request a reporting form, then complete and return to the address on the pre-addressed form, or submit by fax to 1-800-FDA-0178
END OF QUOTE
KingBio have a website where they disclose their mission statement:
- To provide safe, all-natural medicines without harmful side effects.
- To offer affordable natural medicines that help people overcome common health challenges.
- To achieve the trust and respect of our customers and uphold the best product quality.
- To empower people with the most effective ways to achieve abundant health.
… The FDA classifies homeopathic medicines as pharmaceutical drug products. King Bio is an FDA-registered pharmaceutical manufacturer and is strictly compliant with FDA guidelines and current good manufacturing practices (cGMP). Unlike most pharmaceutical drug products, homeopathic medicine offers gentle symptomatic relief, without recorded harmful side effects.
SAY NO MORE!
Can I tempt you to run a little (hopefully instructive) thought-experiment with you? It is quite simple: I will tell you about the design of a clinical trial, and you will tell me what the likely outcome of this study would be.
Are you game?
Here we go:
_____________________________________________________________________________
Imagine we conduct a trial of acupuncture for persistent pain (any type of pain really). We want to find out whether acupuncture is more than a placebo when it comes to pain-control. Of course, we want our trial to look as rigorous as possible. So, we design it as a randomised, sham-controlled, partially-blinded study. To be really ‘cutting edge’, our study will not have two but three parallel groups:
1. Standard needle acupuncture administered according to a protocol recommended by a team of expert acupuncturists.
2. Minimally invasive sham-acupuncture employing shallow needle insertion using short needles at non-acupuncture points. Patients in groups 1 and 2 are blinded, i. e. they are not supposed to know whether they receive the sham or real acupuncture.
3. No treatment at all.
We apply the treatments for a sufficiently long time, say 12 weeks. Before we start, after 6 and 12 weeks, we measure our patients’ pain with a validated method. We use sound statistical methods to compare the outcomes between the three groups.
WHAT DO YOU THINK THE RESULT WOULD BE?
You are not sure?
Well, let me give you some hints:
Group 3 is not going to do very well; not only do they receive no therapy at all, but they are also disappointed to have ended up in this group as they joined the study in the hope to get acupuncture. Therefore, they will (claim to) feel a lot of pain.
Group 2 will be pleased to receive some treatment. However, during the course of the 6 weeks, they will get more and more suspicious. As they were told during the process of obtaining informed consent that the trial entails treating some patients with a sham/placebo, they are bound to ask themselves whether they ended up in this group. They will see the short needles and the shallow needling, and a percentage of patients from this group will doubtlessly suspect that they are getting the sham treatment. The doubters will not show a powerful placebo response. Therefore, the average pain scores in this group will decrease – but only a little.
Group 1 will also be pleased to receive some treatment. As the therapists cannot be blinded, they will do their best to meet the high expectations of their patients. Consequently, they will benefit fully from the placebo effect of the intervention and the pain score of this group will decrease significantly.
So, now we can surely predict the most likely result of this trial without even conducting it. Assuming that acupuncture is a placebo-therapy, as many people do, we now see that group 3 will suffer the most pain. In comparison, groups 1 and 2 will show better outcomes.
Of course, the main question is, how do groups 1 and 2 compare to each other? After all, we designed our sham-controlled trial in order to answer exactly this issue: is acupuncture more than a placebo? As pointed out above, some patients in group 2 would have become suspicious and therefore would not have experienced the full placebo-response. This means that, provided the sample sizes are sufficiently large, there should be a significant difference between these two groups favouring real acupuncture over sham. In other words, our trial will conclude that acupuncture is better than placebo, even if acupuncture is a placebo.
THANK YOU FOR DOING THIS THOUGHT EXPERIMENT WITH ME.
Now I can tell you that it has a very real basis. The leading medical journal, JAMA, just published such a study and, to make matters worse, the trial was even sponsored by one of the most prestigious funding agencies: the NIH.
Here is the abstract:
___________________________________________________________________________
Musculoskeletal symptoms are the most common adverse effects of aromatase inhibitors and often result in therapy discontinuation. Small studies suggest that acupuncture may decrease aromatase inhibitor-related joint symptoms.
Objective:
To determine the effect of acupuncture in reducing aromatase inhibitor-related joint pain.
Design, Setting, and Patients:
Randomized clinical trial conducted at 11 academic centers and clinical sites in the United States from March 2012 to February 2017 (final date of follow-up, September 5, 2017). Eligible patients were postmenopausal women with early-stage breast cancer who were taking an aromatase inhibitor and scored at least 3 on the Brief Pain Inventory Worst Pain (BPI-WP) item (score range, 0-10; higher scores indicate greater pain).
Interventions:
Patients were randomized 2:1:1 to the true acupuncture (n = 110), sham acupuncture (n = 59), or waitlist control (n = 57) group. True acupuncture and sham acupuncture protocols consisted of 12 acupuncture sessions over 6 weeks (2 sessions per week), followed by 1 session per week for 6 weeks. The waitlist control group did not receive any intervention. All participants were offered 10 acupuncture sessions to be used between weeks 24 and 52.
Main Outcomes and Measures:
The primary end point was the 6-week BPI-WP score. Mean 6-week BPI-WP scores were compared by study group using linear regression, adjusted for baseline pain and stratification factors (clinically meaningful difference specified as 2 points).
Results:
Among 226 randomized patients (mean [SD] age, 60.7 [8.6] years; 88% white; mean [SD] baseline BPI-WP score, 6.6 [1.5]), 206 (91.1%) completed the trial. From baseline to 6 weeks, the mean observed BPI-WP score decreased by 2.05 points (reduced pain) in the true acupuncture group, by 1.07 points in the sham acupuncture group, and by 0.99 points in the waitlist control group. The adjusted difference for true acupuncture vs sham acupuncture was 0.92 points (95% CI, 0.20-1.65; P = .01) and for true acupuncture vs waitlist control was 0.96 points (95% CI, 0.24-1.67; P = .01). Patients in the true acupuncture group experienced more grade 1 bruising compared with patients in the sham acupuncture group (47% vs 25%; P = .01).
Conclusions and Relevance:
Among postmenopausal women with early-stage breast cancer and aromatase inhibitor-related arthralgias, true acupuncture compared with sham acupuncture or with waitlist control resulted in a statistically significant reduction in joint pain at 6 weeks, although the observed improvement was of uncertain clinical importance.
__________________________________________________________________________
Do you see how easy it is to deceive (almost) everyone with a trial that looks rigorous to (almost) everyone?
My lesson from all this is as follows: whether consciously or unconsciously, SCAM-researchers often build into their trials more or less well-hidden little loopholes that ensure they generate a positive outcome. Thus even a placebo can appear to be effective. They are true masters of producing false-positive findings which later become part of a meta-analysis which is, of course, equally false-positive. It is a great shame, in my view, that even top journals (in the above case JAMA) and prestigious funders (in the above case the NIH) cannot (or want not to?) see behind this type of trickery.
The fact that many SCAM-practitioners are latent or even overt anti-vaxxers has often been addressed on this blog. The fact that the anti-vaccination guru, Andrew Wakefield, has his fingers deep in the SCAM-pie is less well appreciated.
In case you forgot who Wakefield is, let me remind you. As a gastroenterologist at the London Royal Free Hospital, he published evidence in the Lancet (1998) suggesting that the MMR vaccination was a cause of autism. It was discovered to be fraudulent. In 2010, a statutory tribunal of the GMC found three dozen charges proved, including 4 counts of dishonesty and 12 counts involving the abuse of developmentally delayed children. Consequently, he was struck off the register and lives in the US ever since where he, amongst many other things, enjoys lecturing to homeopaths and chiropractors about the dangers of vaccination.
Since Trump, who seems to share Wakefield’s anti-vaxx stance, has become president of the US, Wakefield has managed to creep back in the limelight. The Guardian recently reported: At one of President Trump’s inaugural balls in January last year, he was quoted as contemplating the overthrow of the (pro-vaccine) US medical establishment in words that brought to mind Trump himself. “What we need now is a huge shakeup at the Centers for Disease Control and Prevention (CDC) – a huge shakeup. We need that to change dramatically.”

In the US, Wakefield also founded the ‘Autism Media Channel’ which makes videos alleging a causal link between autism and the MMR vaccine. The film ‘Vaxxed’ was thus directed by Wakefield. It was put forward to premiere at the 2016 Tribeca film festival by Robert De Niro, the father of an autistic child. It alleges a cover-up of the alleged link between MMR and autism by the CDC – the institute Wakefield said needed a shake-up at the Trump inaugural ball. After much discussion, De Niro fortunately withdrew the film.
Wakefield’s private life has also seem significant changes. He is reported to have recently left his wife who had supported him throughout the debacle in the UK and is now ‘deliciously in love’ with the super-model and entrepreneur Elle Macpherson . Brian Burrowes, 48, who edited ‘Vaxxed’ was reported stating that he and Macpherson had begun dating after they were both guests at the ‘Doctors Who Rock‘ Awards in November last year. This event was to honour alternative medicine practitioners, with Macpherson handing out an award and Wakefield receiving one. Other awardees included Del Bigtree and Billy DeMoss DC.
Wakefield’s legacy in Europe is the recurrence of measles due to persistent doubts in vaccination safety. This regrettable phenomenon is fuelled by Wakefield’s multiple activities, including face-book, twitter and you-tube. Social media has provided an alternative to the “failings of mainstream media”, Wakefield was quoted in the Guardian saying – another phrase that could have come from a tweet by the US president himself. “In this country, it’s become so polarised now … No one knows quite what to believe,” Wakefield said. “So, people are turning increasingly to social media.”
And this is what I said about this strategy in today’s Times: “Such anti-vaccination propaganda is hugely harmful. It prompts many families to shun immunisations which means firstly they are unprotected, and secondly we as a people might lose herd immunity. The result is what we currently see throughout Europe: epidemics are threatening the lives of millions. It is in my view irresponsible for any institution to get involved in the anti-vaxx cult, particularly for universities who really should know better.”
We have previously seen that SCAM-use is associated with shorter survival of cancer patients. A new article now confirms this notion.
The investigators wanted to find out what patient characteristics are associated with use of SCAM for cancer and what is the association of SCAM with treatment adherence and survival. They thus compared the overall survival between patients with cancer receiving conventional treatments with or without SCAM and the adherence to treatment and characteristics of patients in both groups.
Their retrospective observational study used data from the National Cancer Database on 1 901 815 patients from 1500 Commission on Cancer–accredited centers across the United States who were diagnosed with nonmetastatic breast, prostate, lung, or colorectal cancer between January 1, 2004, and December 31, 2013. Patients were matched on age, clinical group stage, Charlson-Deyo comorbidity score, insurance type, race/ethnicity, year of diagnosis, and cancer type. Overall survival, adherence to treatment, and patient characteristics were the study endpoints.
The cohort comprised 1 901 815 patients with cancer (258 patients in the SCAM group and 1 901 557 patients in the control group). In the main analyses following matching, 258 patients were in the SCAM group, and 1032 patients were in the control group. Patients who chose SCAM did not have a longer delay to initiation of conventional therapies, but had higher refusal rates of surgery, radiotherapy, and hormone therapy. Use of SCAM was associated with poorer 5-year overall survival compared with no SCAM (82.2% [95% CI, 76.0%-87.0%] vs 86.6% [95% CI, 84.0%-88.9%]; P = .001) and was independently associated with greater risk of death (hazard ratio, 2.08; 95% CI, 1.50-2.90) in a multivariate model that did not include treatment delay or refusal. However, there was no significant association between SCAM and survival once treatment delay or refusal was included in the model.
The authors concluded that patients who received CM were more likely to refuse additional CCT, and had a higher risk of death. The results suggest that mortality risk associated with CM was mediated by the refusal of CCT.
This new evidence confirms previous papers: SCAM-use is associated with shorter survival of cancer patients. As it is based on a large sample size, its results are more compelling. They indicate that it is not SCAM per se, but the attitude of SCAM-users to conventional therapies that is the cause of the effect. As I have said and written hundreds of times: the most serious risk of SCAM is not a direct but an indirect one: the risk of neglecting effective therapies. Essentially, this means that better information targeted at vulnerable patients must be the way forward (one of the main ambitions of this blog, I hasten to add).