evidence
Why are we here?
Who am I?
What is my life’s purpose?
These are BIG questions indeed.
The spiritually transformative work of Life Between Lives (LBL) hypnotherapy began with one man’s dedication and curiosity to search for answers to the great questions about life and beyond. Today, the Michael Newton Institute (MNI), founded by Dr. Michael Newton, and our global network of over 200 LBL Facilitators hold his vision for humanity and carry on his passion for researching the Afterlife and bringing the evolving modality of LBL hypnotherapy to humanity.
Our Vision
For humanity to live the unconditional love and wisdom of Spiritual Consciousness.
Our Mission
To raise personal and collective consciousness, by bringing the healing and wisdom of Life Between Lives to individuals around the globe, reawakening their immortal identity and integrating Spiritual Consciousness.
Who We Are
The Michael Newton Institute is a not-for-profit organization, bringing together a worldwide collective of trained Facilitators to offer Life Between Lives hypnotherapy, as pioneered by Dr. Michael Newton.Dr Michael Newton. We are committed to providing opportunities globally for people to experience their soul state and a reconnection to the wisdom of the After-life / Inter-life.
What We Offer the World
We advocate for the Spiritual Realm, sharing the wisdom received by individuals around the globe through the exploration of their existence between lives by offering:
- Life Between Lives Sessions – Access to LBL sessions for individuals all around the world through our network of members.
- LBL Facilitator Network – Our MNI members are a diverse group of over 200 individuals who offer LBL to clients all around the world in 40 countries and over 25 languages within their own practices.
- LBL Training – Empowering new generations to learn LBL and continue this important work for their own clients. We create and nurture a community of Life Between Lives Facilitators to connect, learn and grow, so they may support their clients.
- Stories of the Afterlife – Our quarterly journal shares the latest LBL cases and information about LBL (public subscriptions welcome).
- Publications – Continued publication of Dr Michael Newtons and the Institutes own books ensure the wisdom of LBL work is accessible to all people. Over 1 million people have enjoyed these books and learnt from others, Life Between Lives spiritually transformative experience, applying the wisdom to bring new insight, awareness and healing to their own lives.
- Research – We continue to explore the afterlife and conduct studies into the therapeutic benefits of LBL.
- Facebook Community – Our thriving social media discussion group has over 8,000 members who discuss the work of Dr Michael Newton, MNI and LBL every day.
You can read about Dr. Newton and the development of the Michael Newton Institute over the last 20 years at History of MNI. The Michael Newton Institute is overseen by a Board of Directors and Volunteer Teams.
Our LBL Facilitator Community
MNI is an organisation of like-minded, yet diverse individuals who are called to help others expand their awareness of their immortal identity furthering Dr Michael Newton’s legacy. Individuals in our LBL facilitator member community can be found in 40 countries around the world.
We understand more than anyone that our higher guidance draws us together for a common purpose. Many feel the call to join the Michael Newton Institute, often inspired by reading our publications, or through a life changing experience in their own Life Between Lives session. MNI is always seeking to grow the community, if you feel drawn you may consider LBL training.
After completing LBL training and certification requirements, certified LBL facilitators join our global membership community offering LBL to their own clients in their independent practices. LBL work can be a spiritually transformative experience for many clients and MNI LBL Facilitators consider the offering of LBL work to others an honour.
Values and Ethics
As LBL Facilitators, and Members of the Michael Newton Institute (MNI) we are:
- Dedicated and passionate about reawakening humanity’s connection to the unconditional love and wisdom of Spiritual Consciousness for healing and personal growth.
- Trusting in the innate wisdom within everyone and All That Is.
- Compassionate to those we serve and each other, seeking to transcend the human condition.
We are a Spiritual based organization. The Michael Newton Institute is committed to maintaining the highest standard of human and spiritual Values and Ethics in delivering our Mission for humanity. Our LBL Facilitators and those in many volunteers in roles throughout our organization commit to following the MNI Code of Ethics in their own practices, or working on behalf of MNI. Our Alliance Hypnotherapy and Alliance Past Life Regression Program partners also commit to these ethical standards, to support our Vision and Mission.
So:
Why are we here?
Who am I?
What is my life’s purpose?
I found one therapist offering these services, and it was her website that provided some plausible answers:
We are here to be exploited by charlatans.
We are considered to be gullible morons.
Our purpose in life is to support quacks.
The costs for the sessions range from 90 to 795 Euros!
The last few days, I spent much of my time answering questions from journalists on the subject of Charles lll. [interestingly, almost exclusively journalists NOT writing for UK newspapers]. Unsurprisingly, they all wanted to know about the way Charles managed to close down my research department at Exeter University some 10 years ago.
The story is old and I am a bit tired of repeating it. So, nowadays I often refer people to Wikipedia where a short paragraph sums it up:
Ernst was accused by Prince Charles’ private secretary of having breached a confidentiality agreement regarding the 2005 Smallwood report. After being subjected to a “very unpleasant” investigation by the University of Exeter, the university “accepted his innocence but continued, in his view, to treat him as ‘persona non grata’. All fundraising for his unit ceased, forcing him to use up its core funding and allow its 15 staff to drift away.”[15] He retired in 2011, two years ahead of his official retirement.[10][25] In July 2011, a Reuters article described his “long-running dispute with the Prince about the merits of alternative therapies” and stated that he “accused Britain’s heir-to-the-throne Prince Charles and other backers of alternative therapies on Monday of being ‘snake-oil salesmen’ who promote products with no scientific basis”, and that the dispute “had cost him his job – a claim Prince Charles’s office denied”.[14][26] Ernst is a republican, and has supported Republic, an organisation which campaigns for the abolition of the British monarchy.[27]
Re-reading it yesterday, I noticed that the text is not entirely correct (a full account can be found here). Let me explain:
- There never was a formal confidentiality agreement with signature etc. But I did feel bound to keep the contents of the Smallwood report confidential.
- The investigation by my University was not just ‘very unpleasant’, it was also far too long. It lasted 13 months! I had to take lawyers against my own University!
- In addition, it was unnecessary, not least because a University should simply establish the facts and, if reasonable, defend its professor from outside attacks. The facts could have been established over a cup of tea with the Vice Chancellor in less than half an hour.
- When my department had been destroyed in the process, I retired voluntarily and was subsequently re-employed for half a year to help find a successor. In retrospect, I see this move as a smart ploy by the University to keep me sweet and prevent me from going to the press.
- A successor was never hired; one good candidate was found but he was told that he had to find 100% of the funds to do the job. Nobody of high repute would have found this acceptable, and thus the only good candidate was not even tempted to accept the position.
- The snake oil salesman story is an entirely separate issue (see here) that happened years later.
- It is true that Charles’s office denied that Charles knew about his 1st private secretary writing to my Vice Chancellor asking him to investigate my alleged breach of confidence. However, as Sir Michael Peat started his letter with the words “I AM WRITING … AS THE PRINCE OF WALES’ PRIVATE SECRETARY…, I find this exceedingly hard to believe.
- Even though Charles did a sterling job in trying, I did not become a republican. I do have considerable doubts that Charles will be a good King (his reign might even be the end of the monarchy), and I did help the republican cause on several occasions but I never formally joined any such group (in general, I am not a joiner of parties, clubs or interest groups).
To one of the journalists who recently interviewed me, I explained that I do not in the slightest feel sore, bitter, or angry on a personal level. Going into early retirement suited me perfectly fine, and thanks to that decision I enjoy life to the full. The significance of this story lies elsewhere: Charles’ intervention managed to permanently close the then worldwide-only department that systematically and critically investigated so-called alternative medicine. If you know another, please let me know.
It is not often that I publish a paper with a philosopher in a leading journal of philosophy. In fact, it is the first time, and I am rather proud of it – so much so that I must show my readers (the article is freely available via the link below and I encourage everyone to read the full text) the abstract of our article entitled WHY HOMOEOPATHY IS PSEUDOSCIENCE (Synthese (2022) 200:394):
Homoeopathy is commonly recognised as pseudoscience. However, there is, to date, no systematic discussion that seeks to establish this view. In this paper, we try to fill this gap. We explain the nature of homoeopathy, discuss the notion of pseudoscience, and provide illustrative examples from the literature indicating why homoeopathy fits the
bill. Our argument contains a conceptual and an empirical part.
In the conceptual part, we introduce the premise that a doctrine qualifies as a pseudoscience if, firstly, its proponents claim scientific standing for it and, secondly, if they produce bullshit to defend it, such that, unlike science, it cannot be viewed as the most reliable knowledge on its topic. In the empirical part, we provide evidence that homoeopathy fulfils both criteria. The first is quickly established since homoeopaths often explicitly claim scientificity.
To establish the second, we dive into the pseudo-academic literature on homoeopathy to provide evidence of bullshit in the arguments of homoeopaths. Specifically, we show that they make bizarre ontological claims incompatible with natural science, illegitimately shift the burden of proof to sceptics, and mischaracterise, cherry-pick, and misreport the evidence. Furthermore, we demonstrate that they reject essential parts of established scientific methodology and use epistemically unfair strategies to immunise their doctrine against recalcitrant evidence.
And here is our conclusion:
At the beginning of the paper, we noted that homoeopathy is commonly named one of the prototypical pseudosciences. However, there has been, to date, no comprehensive discussion as to what makes it a pseudoscience. Moreover, the problem is not trivial since the most well-known and influential demarcation criteria, such as Popper’s falsifiability criterion and Kuhn’s problem-solving criterion, cannot account for it, as we have shown. We have tried to fill this research gap using a novel bullshitology-based approach to the demarcation problem. Following this approach, we have argued that homoeopathy should be regarded as pseudoscience because its proponents claim scientific standing for it and produce argumentative bullshit to defend it, thus violating important epistemic standards central to science.
As numerous of my posts have demonstrated, chiropractic manipulations can cause severe adverse effects, including deaths. Several hundred have been documented in the medical literature. When discussing this fact with chiropractors, we either see denial or we hear the argument that such events are but extreme rarities. To the latter, I usually respond that, in the absence of a monitoring system, nobody can tell how often serious adverse events happen. The resply often is this:
You are mistaken because the Royal College of Chiropractors’ UK-based Chiropractic Patient Incident Reporting and Learning System (CPiRLS) monitors such events adequately.
I have heard this so often that it is time, I feel, to have a look at CPiRLS. Here is what it says on the website:
CPiRLS is a secure website which allows chiropractors to view, submit and comment on patient safety incidents.
Access to CPiRLS
CPiRLS is currently open to all UK-based chiropractors, all ECU members and members of the Chiropractic and Osteopathic College of Australasia. To access the secure area of the CPiRLS website, please click the icon below and insert the relevant CPiRLS username and password when prompted.
In the UK, these can normally be found on your Royal College of Chiropractors’ membership card unless the details are changed mid-year. Alternatively, email [email protected] from your usual email address and we will forward the details.
Alternatively, in the UK and overseas, secure access details can be obtained from your professional association.
National associations and organisations wishing to use CPiRLS, or obtain trial access to the full site for evaluation purposes, should contact The Royal College of Chiropractors at [email protected]
Please click the icon below to visit the CPiRLS site.
Yes, you understood correctly. The public cannot access CPiRLS! When I click on the icon, I get this:
Welcome to CPiRLS
CPiRLS, The Chiropractic Patient Incident Reporting and Learning System – is an online reporting and learning forum that enables chiropractors to share and comment on patient safety incidents.
The essential details of submitted reports are published on this website for all chiropractors to view and add comments. A CPiRLS team identifies trends among submitted reports in order to provide feedback for the profession. Sharing information in this way helps to ensure the whole profession learns from the collective experience in the interests of patients.
All chiropractors are encouraged to adopt incident reporting as part of a blame-free culture of safety, and a routine risk management tool.
CPiRLS is secure and anonymous. There is no known way that anyone reporting can be identified, nor do those running the system seek to identify you. For this security to be effective, you require a password to participate.
Please note that reporting to CPiRLS is NOT a substitute for the reporting of patient safety incidents to your professional association and/or indemnity insurers.
So, how useful is CPiRLS?
Can we get any information from CPiRLS about the incidence of adverse effects?
No!
Do we know how many strokes or deaths have been reported?
No!
Can chiropractors get reliable information from CPiRLS about the incidence of adverse effects?
No, because reporting is not mandatory and the number of reports cannot relate to incidence.
Are chiropractors likely to report adverse effects?
No, because they have no incentive and might even feel that it would give their profession a bad name.
Is CPiRLS transparent?
No!
Is CPiRLS akin to postmarketing surveillance as it exists in conventional medicine?
No!
How useful is CPiRLS?
I think I let my readers answer this question.
Guest post by Ken McLeod
On 07 June 2022, we published an article warning readers of the planned visit to the UK of health crank Barbara O’Neill, ‘A residential health programme that poses “a risk to the health and safety of members of the public.” ‘ We referred to the Prohibition Order that the New South Wales Health Care Complaints Commission has imposed on her:
‘The Commission is satisfied that Mrs O’Neill poses a risk to the health and safety of members of the public and therefore makes the following prohibition order:
Mrs O’Neill is permanently prohibited from providing any health services, as defined in s4 Of the Health Care Complaints Act 1993, whether in a paid or voluntary capacity.’
We showed that O’Neill remains undaunted by such mere technicalities and continues to spruik her nostrums and misinformation, such as that planned for Manna House, Stoke-on-Trent.
One reader did a little bit of digging into O’Neill’s lectures and found something that should alarm anyone; her advocacy of asbestosform Yoni Stones for ‘Balancing Your Hormones.’
So what are ‘Yoni Stones?’ and ‘Why should we be worried?’ we hear you ask. Good questions, so here we go.
0. BACKGROUND:
According to promoters in alternative health industries, ‘Yoni stones,’ also known as ‘Yoni Eggs’ are ‘semi – precious stones carved into the shape of eggs that can be inserted into a woman’s womb space for vaginal wall tightening and energetic cleansing. Yoni Eggs have been used for many decades by the most in-tuned women who know that keeping good vaginal wellness is keeping universal wellness. The more in-tuned a woman is in her femininity the better all her relations will be.’ 1
1. PROMOTION AND SALE:
The following are examples of the promotion and sale of Yoni stones and showing how wrong and dangerous they are.
1.1 ‘La Loba’
A Google search found hundreds of retailers selling them, such as ‘La Loba’ 2 whose website does do not give an address, but are located on the Gold Coast Australia. La Loba sells nephrite jade eggs like this:
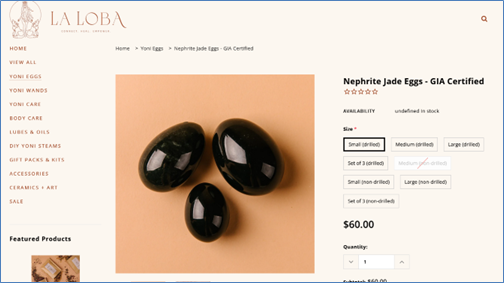
La Loba claim that ‘GIA certified means that it’s certified by the Gemological institute of America to be that specific stone. So you know it’s a real stone that is high quality.’ La Loba makes several claims of therapeutic benefit, like:
‘Yoni Eggs Physical Benefits Pelvic Floor Health Assists with incontinence Increases lubrication Builds sensitivity Helps improve Libido Can be used to prepare for childbirth and to heal post childbirth Helps to prevent and improve prolapse Balances hormones by increasing blood flow to the Yoni Increases orgasmic pleasure for yourself and your partner Spiritual Benefits Healing properties of the chosen crystal are absorbed Builds connection with your Yoni Helps one work through any trauma/stagnant energy held… ‘
Despite the claims of therapeutic benefits, ‘La Loba’ did not display any regulatory approval from the Australian Therapeutic Goods Administration or US Federal Drug Administration, so we can take it as read that Yoni Stones have not been assessed for safety.
1.2 Barbara O’Neill
The most prominent promoter of Yoni Stones is Barbara O’Neill, of Misty Mountain Lifestyle Retreat, of Bellbrook, New South Wales.
The internet, especially YouTube, is alive with hundreds of her videos promoting all sorts of quackery, but today we can limit ourselves to the dozens of videos in which she promotes Yoni Stones, such as the video of Barbara O’Neill conducting a lecture at Living Springs Alabama, USA. This video 5 ‘Balancing Your Hormones’ has been viewed 43,636 times since it was first published on 3 May 2022.
From the video:

In that video, Barbara O’Neill makes claims that are of concern. From the transcript,6 at 00:44:31, she recommends ‘Yoni Stones,’ and at 00:44:44 ‘… ideally, they’re made out of nephrite.’ (See the above screencap of her whiteboard presentation, bottom left-hand corner.) In the transcript she advises that women should insert them daily for several hours at a time over several months, even years. O’Neill describes Yoni Stones at 00:44:35 in the transcript: “The Chinese dynasty developed Yoni stones to help the young concubines be sexually toned for the emperor. But they’re very popular today, and ideally, they’re made out of nephrite. Jade nephrite. Jade is like a green marble. The nephrite jade is heavy and as you’ll see why that’s important in a minute. But it’s also a smooth marble, so there are no crevices.”
There are several falsehoods in this:
1.2.1 There were many dynasties in Imperial China, but none of them were named ‘The Chinese Dynasty.’
1.2.2 No Imperial Chinese dynasty developed Yoni Stones. It’s marketing hype designed to dupe the gullible. Obstetrician -Gynaecologist Dr Jennifer Gunter 7 and archaeologist Professor Sarah Parcak 8 researched that claim by conducting a search of the online databases of four major Chinese art and archaeology collections in the United States. They identified more than 5000 jade objects viewable in online databases. They found that no vaginal jade eggs were identified, and concluded that:
“No evidence was found to support the claim that vaginal jade eggs were used for any indication in ancient Chinese culture.” 9
1.2.3 As for O’Neill’s claim that there are no crevices and are therefore safe, O’Neill says in the transcript at 00:45:13 ‘….There are two holes in the bottom (of the Yoni Stone) so that a woman can insert dental floss for easy extraction….’ So crevices are out but holes are OK?
The Cleveland Health Clinic published an article 10 on July 30, 2021, by Obstetrician – Gynaecologist Dr Suchetha Kshettry, MD, ‘Think Twice Before Putting a Yoni Egg in Your Vagina. She says that ‘Gemstones like jade and onyx are semi-porous, which means there’s space for bacteria to take up residence within them. Semi-porous materials are difficult to fully clean, too, meaning that bacteria may stick around and fester.’ She listed the following hazards:
Ø Persistent bacterial infections;
Ø Irritation, scratches, tears;
Ø Damage to pelvic floor muscles; Ø toxic shock syndrome that can lead to serious health issues and even death.
Dr Kshettry makes it clear that there is no benefit.
That is supported by Obstetrician -Gynaecologist Dr Jennifer Gunter, who has written that Yoni stones do not balance hormones and have all the risks that Dr Kshettry listed above. 11
Further, California officials prosecuted Gwyneth Paltrow and her company Goop for making the same claims as O’Neill. In an out-of-court settlement, Paltrow’s company agreed to pay $US145,000 ($202,000) in civil penalties. 12
1.2.4. More concerning, nephrite jade is notorious as a dangerous asbestiform prismatic tremolite, a mineral composed of microcrystalline tremolite asbestos. Nephrite is a variety of the calcium, magnesium, and iron-rich amphibole minerals tremolite or actinolite, aggregates of which also make up one form of asbestos. The chemical formula for nephrite is Ca2(Mg, Fe)5Si8O22(OH)2. It is one of two different mineral species called jade. In layman’s terms it is ‘asbestos’ and we would think that it is therefore carcinogenic. Strangely enough, while there is plenty of research on the consequences of inhaling asbestos, there seems to be little or no research on the consequences of inserting it into vaginas.
That may be because scientists thought that it was not a productive area of research because they thought nobody would be stupid enough to do that. (How wrong they were.) Nevertheless, in the absence of definitive research showing that inserting asbestos into vaginas is perfectly safe, promoting that is incredibly irresponsible.
All we could find on the subject was the limited research which examined the dangers to people shaping nephrite jade asbestos:
1.2.4.1. Yang HY, Shie RH, Chen PC. Carving of non-asbestiform tremolite and the risk of lung cancer: a follow-up mortality study in a historical nephrite processing cohort. Occup Environ Med. 2013 Dec;70(12):852-7. doi: 10.1136/oemed-2013-101404. Epub 2013 Sep 18. PMID: 24142973; PMCID: PMC3841744. 13
1.2.4.1.1. The researchers found that nephrite processing led to a significantly increased risk of lung cancer.
1.2.4.2. Bailey et al, ‘The Asbestiform and Prismatic Mineral Growth Habit and Their Relationship to Cancer Studies – A Pictorial Presentation.’ 14
If anyone can find research on the effects of inserting asbestos-form Yoni Stones into vaginas, please let us know in the comments.
2. CONCLUSIONS:
2.1 As if the risks of persistent bacterial infections, irritation, scratches, tears, damage to pelvic floor muscles, toxic shock syndrome, serious health issues and death were not bad enough, Barbara O’Neill’s and other health gurus’ and retailers’ recommendations to insert asbestos stones into vaginas for extended lengths of time is reckless and dangerous. And there is no therapeutic benefit in the use of Yoni Stones.
But that’s Standard Operating Procedure in Alt-Med, so that’s all right then.
So what would health regulators make of this? Should they issue a Public Warning to all users, processors, manufacturers, importers and retailers? Watch this space.
1 https://www.yonieggs.com/
2 https://laloba.com.au/collections/yoni-eggs
3 https://laloba.com.au/collections/yoni-eggs/products/nephrite-jade-eggs?_pos=1&_sid=ab4fad37e&_ss=r
4 https://laloba.com.au/blogs/resources
5https://www.youtube.com/watch?v=z7uATPC-7CY. A backup copy is available on request.
6 Transcript is available at https://www.dropbox.com/s/gwdncg5iwx3a31g/Balancing%20Your%20Hormones%20-%20Barbara%20O%27Neill-%203%20May%202022.mp4-transcript%20%281%29.docx?dl=0
7 https://en.wikipedia.org/wiki/Jen_Gunter
8 https://en.wikipedia.org/wiki/Sarah_Parcak
9 “Vaginal Jade Eggs: Ancient Chinese Practice or Modern Marketing Myth?” Gunter, Jennifer MD*; Parcak, Sarah PhD, Female Pelvic Medicine & Reconstructive Surgery: 1/2 2019 – Volume 25 – Issue 1 – p 1-2, published in Urogynecology – Official Journal of the American Urogynecologic Society. https://journals.lww.com/fpmrs/Abstract/2019/01000/Vaginal_Jade_Eggs__Ancient_Chinese_Practice_or.1.aspx
10 https://health.clevelandclinic.org/are-yoni-eggs-safe/
11 https://drjengunter.com/2017/01/17/dear-gwyneth-paltrow-im-a-gyn-and-your-vaginal-jade-eggs-are-a-bad-idea/
12 https://www.smh.com.au/lifestyle/health-and-wellness/goop-settles-lawsuit-over-purported-benefits-of-jade-eggs-20180906-p5021h.html
13 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3841744/
14 Published 2006. Available on request.
This study aimed to evaluate the efficacy of Persian barley water in controlling the clinical outcomes of hospitalized COVID-19 patients. It was designed as a single-blind, add-on therapy, randomized controlled clinical trial and conducted in Shiraz, Iran, from January to March 2021. One hundred hospitalized COVID-19 patients with moderate disease severity were randomly allocated to receive routine treatment (per local protocols) with or without 250 ml of Persian barley water (PBW) daily for two weeks. Clinical outcomes and blood tests were recorded before and after the study period. Multivariable modeling was applied using Stata software for data analysis.
The length of hospital stay (LHS) was 4.5 days shorter in the intervention group than the control group regardless of history of cigarette smoking (95% confidence interval: -7.22, -1.79 days). Also, body temperature, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and creatinine significantly dropped in the intervention group compared to the control group. No adverse events related to PBW occurred.
The authors from the Department of Traditional Medicine, Shiraz University of Medical Sciences, Shiraz, Iran, concluded that this clinical trial demonstrated the efficacy of PBW in minimizing the LHS, fever, and levels of ESR, CRP, and creatinine among hospitalized COVID-19 patients with moderate disease severity. More robust trials can help find safe and effective herbal formulations as treatments for COVID-19.
I must admit, I did not know about PBW. The authors explain that PBW is manufactured from Hordeum vulgare via a specific procedure. According to recent studies, barley is rich in constituents such as selenium, tocotrienols, phytic acid, catechin, lutein, vitamin E, and vitamin C; these compounds are responsible for their antioxidant and anti-inflammatory properties. Barley grains also have immune-stimulating effects, antioxidant properties, protective effects on the liver and digestive systems, anti-cancer effects, and act to reduce uric acid levels.
But even if these effects would constitute a plausible mechanism for explaining the observed effects (which I do not think they do), the study itself is more than flimsy.
I do not understand why researchers investigating an important issue do not make sure that their study is as rigorous as possible.
- Why not use an adequately large sample size?
- Why not employ a placebo?
- Why not double-blind?
- Why not report the most important outcome, i.e. mortality?
As it stands, nobody will take this study seriously. Perhaps this is a good thing – but perhaps PBW does have positive effects (I know it’s a long shot) and, in this case, a poor-quality study would only prevent an effective therapy come to light.
There is a broad, growing, international consensus that homeopathy is a placebo therapy. Even the Germans who have been notoriously fond of their homeopathic remedies are now slowly beginning to accept this fact. But now, a dispute has started to smolder in Germany’s southwest about further training for doctors in homeopathy. In July, the representative assembly of the Baden-Württemberg Medical Association decided to remove the additional title of homeopathy from the further training regulations of doctors. However, the local health ministry has legal control over the medical association and must therefore review the decision, and the minister (Manne Lucha), a member of the Green Party, has stated that he considers the deletion to be wrong.
In a further deepening of the conflict, it has been reported that the chairwoman of the Green Party, Lena Schwelling, considers the ongoing controversy over homeopathy to be exaggerated and wants to preserve people’s freedom of choice. She said she agrees with Health Minister Manne Lucha that naturopathy and homeopathy are important issues for many people. “There is freedom of choice of doctor and therapy in this country. And if people want to choose it, I think they should be allowed to do so.” She also said continuing education for homeopathy for physicians should remain.
Schwelling spoke out against omitting homeopathy from the benefits catalog of the statutory health insurance funds, as demanded by the German Liberal Party, for example: “We are talking about about 0.003 percent of the total costs of the statutory health insurance funds, which flow into homeopathic medicines and treatments. If you saw that as a homeopathic medicine, that would also be at the detection limit, that’s how little money it is. It’s so diluted and so little in this overall budget that it’s not worth arguing about. That’s why I’m very surprised at the crusade some are waging against the issue of homeopathy.”
Recently, a dispute has been smoldering in the southwest about continuing education for homeopathy. The representative assembly of the Baden-Württemberg Medical Association decided in July to remove the additional title of homeopathy from the continuing education regulations. The local health minister, Lucha, has legal oversight of the medical association and must review the amendment statute. However, the minister has already stated that he believes the deletion is wrong.
In response, Schwelling stated it is a “normal process” for the ministry to review what the medical association has proposed. He added that it was perfectly clear that “further training in homeopathy is additional training and does not replace medical studies. Of course, homeopathic doctors also prescribe antibiotics when indicated. An important point why homeopathy should remain in the canon is that you then have the established control mechanisms, for example, in further education.”
Osteopathic tradition in the cranial field (OCF) postulates that the primary respiratory mechanism (PRM) relies on the anatomical links between the occiput and sacrum. Few studies investigated this relationship with inconsistent results. No studies investigated the occiput-sacrum connection from a neurophysiological perspective.
This study aims to determine whether the sacral technique (ST), compared to the compression of the fourth ventricle (CV4) technique, can affect brain alpha-band power (AABP) as an indicator of a neurophysiological connection between the occiput and sacrum.
Healthy students, 22-30 years old for men and 20-30 years old for women, were enrolled in the study and randomized into eight intervention groups. Each group received a combination of active techniques (CV4 or ST) and the corresponding sham techniques (sham compression of the fourth ventricle [sCV4] or sham sacral technique [sST] ), organized in two experimental sessions divided by a 4 h washout period. AABP was continuously recorded by electroencephalogram (EEG) of the occipital area in the first 10 min of resting state, during each intervention (active technique time) and after 10 min (post-active technique time), for a total of approximately 50 min per session. Analysis was carried out utilizing a repeated-measure ANOVA within the linear general model framework, consisting of a within-subject factor of time and a within-subject factor of treatment (CV4/ST).
Forty healthy volunteers (mean age ± SD, 23.73±1.43 years; range, 21-26 years; 16 male and 24 female) were enrolled in the study and completed the study protocol. ANOVA revealed a time × treatment interaction effect statistically significant (F=791.4; p<0.001). A particularly high increase in mean AABP magnitude was recorded during the 10 min post-CV4, compared to both the CV4 and post-sCV4 application (p<0.001). During all the times analyzed for ST and sST application, no statistically significant differences were registered with respect to the resting state.
The authors concluded that the ST does not produce immediate changes on occipital AABP brain activity. CV4, as previous evidence supported, generates immediate effects, suggesting that a different biological basis for OCF therapy’s connection between the head and sacrum should be explored.
Why on earth should a different biological mechanism be explored? Why not conclude that OCF and its assumptions are pure nonsense?
The answer to these questions is not difficult to find: the authors are from the ‘Istituto Superiore di Osteopatia, Milan, Italy’! One can understand that, at this institution, people are unlikely to agree with my conclusion that OCF is based on absurd concepts and does not merit further research.
In a previous post, I explained that anthroposophic education was founded by Steiner in 1919 to serve the children of employees of the Waldorf-Astoria cigarette factory in Stuttgart, Germany. Pupils of Waldorf or Steiner schools, as they are also frequently called, are encouraged to develop independent thinking and creativity, social responsibility, respect, and compassion.
Waldorf schools implicitly infuse spiritual and mystic concepts into their curriculum. Like some other alternative healthcare practitioners – for instance, doctors promoting integrative medicine, chiropractors, homeopaths, and naturopaths – doctors of anthroposophic medicine tend to advise against childhood immunizations. For this and other reasons, Waldorf schools have long attracted criticism.
Now it has been reported that the district government of Münster has withdrawn the school permit of a Waldorf school in Rheine, Germany, because of “serious deficiencies in the teaching operation”. For the 71 children, school operation ends with the start of the fall vacations at the beginning of October, as the district government announced on Tuesday. Already since the end of 2020 there had been numerous complaints. The school board had not succeeded in eliminating the deficiencies, a proper operation is currently and prospectively not guaranteed.
The list of problems described by the district government is long: there were repeated violations in the health protection of children. A spokesman for the district government said that there had been massive and repeated violations of Corona’s protective measures. In addition, there was a risk of accidents in the playground. The school board had also been unable to stop the misconduct of individual teachers, the district government criticized. “In addition, there is an insufficient supply of teachers, school organizational deficits and a massively disturbed school peace,” it said.
In the end, the basis of trust required for continued operation of the school was no longer given, so the school permit had to be revoked for the sake of the children. “This is an absolutely exceptional case,” the spokesman said. It is presumably the first case under the jurisdiction of the Münster district government, he added.
Developing interventions against age-related memory decline and for older adults experiencing neurodegenerative disease is perhaps one of the greatest challenges of our generation. Spermidine supplementation has shown beneficial effects on brain and cognitive health in animal models, and there has been preliminary evidence of memory improvement in individuals with subjective cognitive decline.
This randomized, double-masked, placebo-controlled phase 2b trial was aimed at determining the effect of longer-term spermidine supplementation on memory performance and biomarkers in this at-risk group. The study was a monocenter trial carried out at an academic clinical research center in Germany. Eligible individuals were aged 60 to 90 years with subjective cognitive decline who were recruited from health care facilities as well as through advertisements in the general population.
One hundred participants were randomly assigned (1:1 ratio) to 12 months of dietary supplementation with either a spermidine-rich dietary supplement extracted from wheat germ (0.9 mg spermidine/d) or placebo (microcrystalline cellulose). Eighty-nine participants (89%) successfully completed the trial. The primary outcome was change in memory performance from baseline to 12-month postintervention assessment (intention-to-treat analysis), operationalized by mnemonic discrimination performance assessed by the Mnemonic Similarity Task. Secondary outcomes included additional neuropsychological, behavioral, and physiological parameters. Safety was assessed in all participants and exploratory per-protocol, as well as subgroup, analyses were performed.
A total of 100 participants (51 in the spermidine group and 49 in the placebo group) were included in the analysis (mean [SD] age, 69 [5] years; 49 female participants [49%]). Over 12 months, no significant changes were observed in mnemonic discrimination performance (between-group difference, -0.03; 95% CI, -0.11 to 0.05; P = .47) and secondary outcomes. Exploratory analyses indicated possible beneficial effects of the intervention on inflammation and verbal memory. Adverse events were balanced between groups.
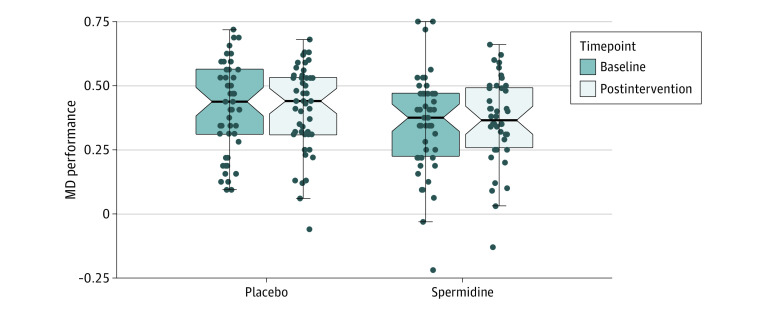
The authors concluded that in this randomized clinical trial, longer-term spermidine supplementation in participants with subjective cognitive decline did not modify memory and biomarkers compared with placebo. Exploratory analyses indicated possible beneficial effects on verbal memory and inflammation that need to be validated in future studies at higher dosage.
The absence of an effect might have, according to the authors, two reasons.
- The daily dose of 0.9 mg spermidine might not have been sufficient to achieve strong effects on memory function and biomarkers in cognitively healthy older individuals.
- The supplementation with dietary spermidine might not act as a memory booster, but rather prevent age-related memory impairment and development of AD, a possibility supported by evidence from animal studies.
I am tempted to add a third one: spermidine might not be effective at all for this indication (or any other condition)!