death
Micronutrient supplements such as vitamin D, vitamin C, and zinc have been used in managing viral illnesses. However, the clinical significance of these individual micronutrients in patients with Coronavirus disease 2019 (COVID-19) remains unclear. A team of researchers conducted this meta-analysis to provide a quantitative assessment of the clinical significance of these individual micronutrients in COVID-19.
They performed a literature search using MEDLINE, Embase, and Cochrane databases through December 5th, 2021. All individual micronutrients reported by ≥ 3 studies and compared with standard-of-care (SOC) were included. The primary outcome was mortality. The secondary outcomes were intubation rate and length of hospital stay (LOS). Pooled risk ratios (RR) and mean difference (MD) with corresponding 95% confidence intervals (CI) were calculated using the random-effects model.
The authors identified 26 studies (10 randomized controlled trials and 16 observational studies) involving 5633 COVID-19 patients that compared three individual micronutrient supplements (vitamin C, vitamin D, and zinc) with SOC.
Vitamin C
Nine studies evaluated vitamin C in 1488 patients (605 in vitamin C and 883 in SOC). Vitamin C supplementation had no significant effect on mortality (RR 1.00, 95% CI 0.62–1.62, P = 1.00), intubation rate (RR 1.77, 95% CI 0.56–5.56, P = 0.33), or LOS (MD 0.64; 95% CI -1.70, 2.99; P = 0.59).

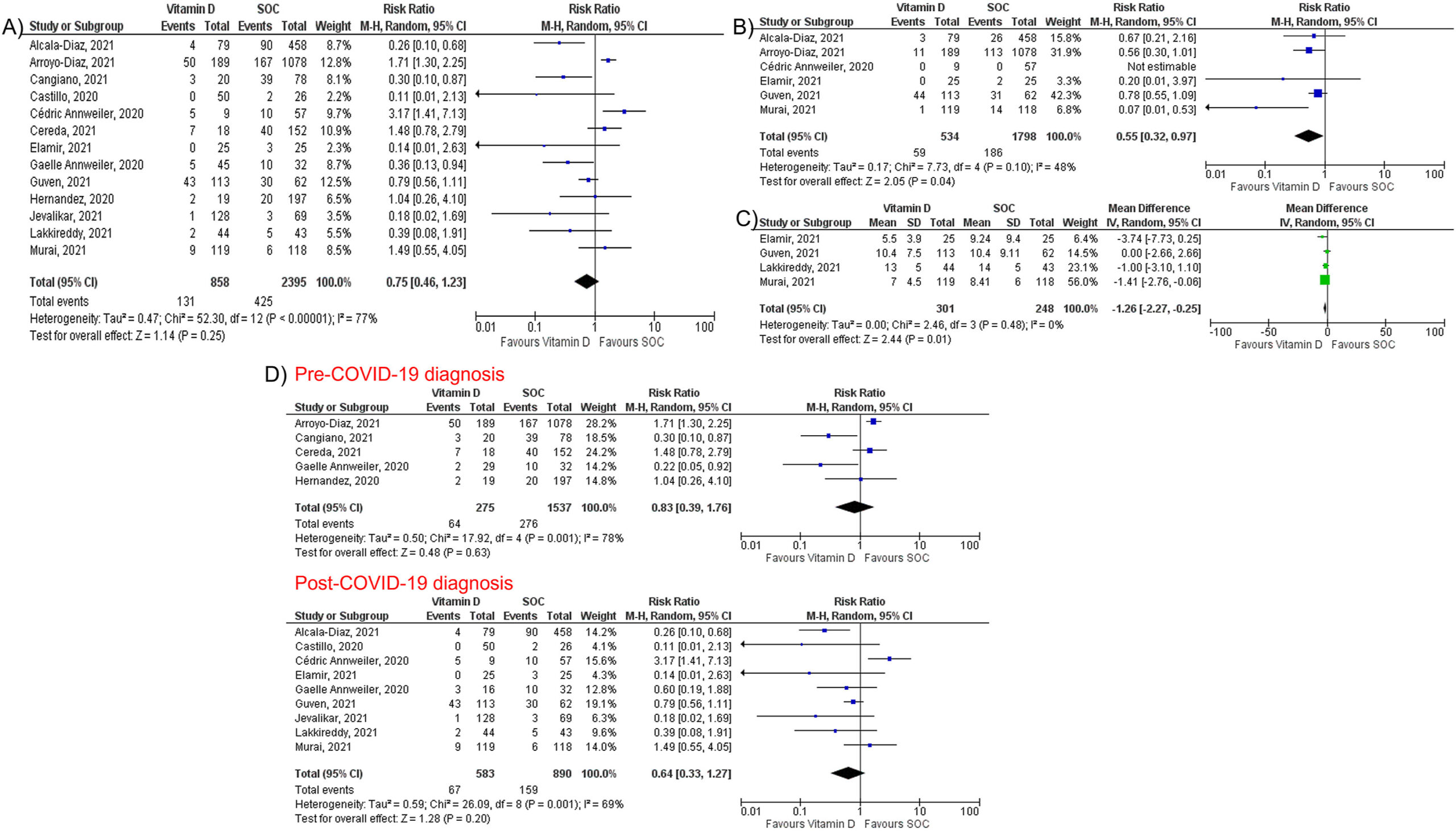
Vitamin D
Fourteen studies assessed the impact of vitamin D on mortality among 3497 patients (927 in vitamin D and 2570 in SOC). Vitamin D did not reduce mortality (RR 0.75, 95% CI 0.49–1.17, P = 0.21) but reduced intubation rate (RR 0.55, 95% CI 0.32–0.97, P = 0.04) and LOS (MD -1.26; 95% CI -2.27, −0.25; P = 0.01). Subgroup analysis showed that vitamin D supplementation was not associated with a mortality benefit in patients receiving vitamin D pre or post COVID-19 diagnosis.
Zinc
Five studies, including 738 patients, compared zinc intake with SOC (447 in zinc and 291 in SOC). Zinc supplementation was not associated with a significant reduction of mortality (RR 0.79, 95% CI 0.60–1.03, P = 0.08).

The authors concluded that individual micronutrient supplementations, including vitamin C, vitamin D, and zinc, were not associated with a mortality benefit in COVID-19. Vitamin D may be associated with lower intubation rate and shorter LOS, but vitamin C did not reduce intubation rate or LOS. Further research is needed to validate our findings.
Barrie R. Cassileth died on Feb. 26 at an assisted-living home in Beverly Hills, California. I knew about Barrie because she was the 1st author of a most remarkable study published in 1991 in the prestigious NEJM. Here is the abstract:
Background: Cancer treatments without proved efficacy have achieved new levels of popularity, particularly among well-educated patients. The value of these therapies is vigorously debated.
Methods: We compared the length of survival and quality of life in patients who received treatment at a prominent unorthodox cancer clinic in addition to conventional treatment and in matched control patients from an academic cancer center who received only conventional treatment. All the patients had documented extensive malignant disease associated with a predicted median survival time of less than one year. The study sample consisted of 78 pairs of patients matched according to sex, race, age, diagnosis, and time from the diagnosis of metastatic or recurrent disease, who were enrolled over a period of 3 1/2 years. Periodic follow-up (approximately every two months) continued until death.
Results: There was no difference between the two patient groups in length of survival. Median survival for both groups was 15 months (P = 0.22; relative risk, 1.23; 95 percent confidence interval, 0.88 to 1.72). Quality-of-life scores were consistently better among conventionally treated patients from enrollment on.
Conclusions: For this sample of patients with extensive disease and for this particular unorthodox treatment regimen, conventional and unorthodox treatments produced similar results. 
In 1995, I met her for the first time when we both served on an NIH panel, and we kept in contact. When I had flown to Boston for a conference she even drove from New York to see me and have a chat. In 1998, she asked me to come to New York because she needed to discuss something important with me and wanted my advice. It turned out that she had been offered to create the Integrative Medicine Service at Memorial Sloan Kettering Cancer Center in New York sponsored by Laurance Rockefeller. She was very much in two minds about accepting. Her fear was that she would have to become an advocate of alternative medicine. I tried to reassure her and pointed out that I did not exactly turn into an advocate after accepting the Exeter post.
In the end, she accepted and, in the years that followed, we met several times at conferences, became friends, and published a few papers together. I even persuaded her to come to one of our annual conferences at Exeter as a keynote speaker. By then, she had clearly become an advocate of complementary medicine.
What had happened?
Barrie was very keen to differentiate alternative from complementary therapies in cancer care. The former she sharply condemned, while advocating the latter for improving the quality of life of cancer patients. When we discussed these issues, I argued that the ‘alternative versus complementary’ was a somewhat artificial division and that the overlap was large. I also pointed out that some of the complementary treatments she was backing were not based on good evidence. In other words, our views had begun to differ. We remained friends but gradually drifted apart and eventually lost contact.
Barrie Joyce Rabinowitz was born on April 22, 1938, in Philadelphia. She attended Bennington College in Vermont and spent a summer teaching art in Pownal, Massachusetts. She graduated with a degree in social sciences in 1959, a year after marrying Peter Cassileth. Barrie received a master’s degree in psychology from Albert Einstein University and a Ph.D. in medical sociology in 1978 from the University of Pennsylvania, where Peter Cassileth was an oncologist. As part of her doctoral program, Barrie worked closely with adult leukemia patients. After being hired at Pennsylvania as an assistant professor, she helped establish one of the first palliative cancer care programs in the US. Before accepting the post at Slone-Kettering, she taught at Duke, Harvard, and the University of North Carolina. In 2003, she became the founding president of the Society for Integrative Oncology.
While at Slone-Kettering, Barrie published several excellent books and high-quality studies of complementary medicine. She kept on working well after the normal retirement age. Her last RCT was only published in 2018. Here is the abstract:
Purpose: Approximately 20% of breast cancer survivors develop breast cancer-related lymphedema (BCRL), and current therapies are limited. We compared acupuncture (AC) to usual care wait-list control (WL) for treatment of persistent BCRL.
Methods: Women with moderate BCRL lasting greater than six months were randomized to AC or WL. AC included twice weekly manual acupuncture over six weeks. We evaluated the difference in circumference and bioimpedance between affected and unaffected arms. Responders were defined as having a decrease in arm circumference difference greater than 30% from baseline. We used analysis of covariance for circumference and bioimpedance measurements and Fisher’s exact to determine the proportion of responders.
Results: Among 82 patients, 73 (89%) were evaluable for the primary endpoint (36 in AC, 37 in WL). 79 (96%) patients received lymphedema treatment before enrolling in our study; 67 (82%) underwent ongoing treatment during the trial. We found no significant difference between groups for arm circumference difference (0.38 cm greater reduction in AC vs. WL, 95% CI – 0.12 to 0.89, p = 0.14) or bioimpedance difference (1.06 greater reduction in AC vs. WL, 95% CI – 5.72 to 7.85, p = 0.8). There was also no difference in the proportion of responders: 17% AC versus 11% WL (6% difference, 95% CI – 10 to 22%, p = 0.5). No severe adverse events were reported.
Conclusions: Our acupuncture protocol appeared to be safe and well tolerated. However, it did not significantly reduce BCRL in pretreated patients receiving concurrent lymphedema treatment. This regimen does not improve upon conventional lymphedema treatment for breast cancer survivors with persistent BCRL.
Her contribution to our knowledge about complementary therapies is outstanding, and I am sure that her papers will be cited for decades to come. She will be missed and remembered as an innovator in the field of palliative cancer care.
Barrie had been married three times. Her third husband, Richard Cooper, who was the Director of the Center for the Future of the Healthcare Workforce and a Senior Fellow in the Leonard Davis Institute of Health Economics at the University of Pennsylvania, died in 2016. Barrie is survived by her siblings, Stephen and Ruth Rabinowitz; her daughters, Jodi Cassileth Greenspan and Wendy Cassileth; her son, Gregory Cassileth; and 6 grandchildren.
- COVID vaccinations are not 100% harmless but they generate much more good than harm.
- They are certainly far less dangerous than the disease.
- COVID infections are not ‘just a flu’ but have serious consequences.
The last point was well-documented in a recent Lancet paper. Here is its abstract in full
Mortality statistics are fundamental to public health decision making. Mortality varies by time and location, and its measurement is affected by well known biases that have been exacerbated during the COVID-19 pandemic. This paper aims to estimate excess mortality from the COVID-19 pandemic in 191 countries and territories, and 252 subnational units for selected countries, from Jan 1, 2020, to Dec 31, 2021.
Methods
All-cause mortality reports were collected for 74 countries and territories and 266 subnational locations (including 31 locations in low-income and middle-income countries) that had reported either weekly or monthly deaths from all causes during the pandemic in 2020 and 2021, and for up to 11 year previously. In addition, we obtained excess mortality data for 12 states in India. Excess mortality over time was calculated as observed mortality, after excluding data from periods affected by late registration and anomalies such as heat waves, minus expected mortality. Six models were used to estimate expected mortality; final estimates of expected mortality were based on an ensemble of these models. Ensemble weights were based on root mean squared errors derived from an out-of-sample predictive validity test. As mortality records are incomplete worldwide, we built a statistical model that predicted the excess mortality rate for locations and periods where all-cause mortality data were not available. We used least absolute shrinkage and selection operator (LASSO) regression as a variable selection mechanism and selected 15 covariates, including both covariates pertaining to the COVID-19 pandemic, such as seroprevalence, and to background population health metrics, such as the Healthcare Access and Quality Index, with direction of effects on excess mortality concordant with a meta-analysis by the US Centers for Disease Control and Prevention. With the selected best model, we ran a prediction process using 100 draws for each covariate and 100 draws of estimated coefficients and residuals, estimated from the regressions run at the draw level using draw-level input data on both excess mortality and covariates. Mean values and 95% uncertainty intervals were then generated at national, regional, and global levels. Out-of-sample predictive validity testing was done on the basis of our final model specification.
Findings
Although reported COVID-19 deaths between Jan 1, 2020, and Dec 31, 2021, totalled 5·94 million worldwide, we estimate that 18·2 million (95% uncertainty interval 17·1–19·6) people died worldwide because of the COVID-19 pandemic (as measured by excess mortality) over that period. The global all-age rate of excess mortality due to the COVID-19 pandemic was 120·3 deaths (113·1–129·3) per 100 000 of the population, and excess mortality rate exceeded 300 deaths per 100 000 of the population in 21 countries. The number of excess deaths due to COVID-19 was largest in the regions of south Asia, north Africa and the Middle East, and eastern Europe. At the country level, the highest numbers of cumulative excess deaths due to COVID-19 were estimated in India (4·07 million [3·71–4·36]), the USA (1·13 million [1·08–1·18]), Russia (1·07 million [1·06–1·08]), Mexico (798 000 [741 000–867 000]), Brazil (792 000 [730 000–847 000]), Indonesia (736 000 [594 000–955 000]), and Pakistan (664 000 [498 000–847 000]). Among these countries, the excess mortality rate was highest in Russia (374·6 deaths [369·7–378·4] per 100 000) and Mexico (325·1 [301·6–353·3] per 100 000), and was similar in Brazil (186·9 [172·2–199·8] per 100 000) and the USA (179·3 [170·7–187·5] per 100 000).
Interpretation
The full impact of the pandemic has been much greater than what is indicated by reported deaths due to COVID-19 alone. Strengthening death registration systems around the world, long understood to be crucial to global public health strategy, is necessary for improved monitoring of this pandemic and future pandemics. In addition, further research is warranted to help distinguish the proportion of excess mortality that was directly caused by SARS-CoV-2 infection and the changes in causes of death as an indirect consequence of the pandemic.
I am posting this in the hope that the many proponents of so-called alternative medicine (SCAM) who deny proven facts about COVID might learn and stop falling victim to proctophasia.
Yes, the fear of nuclear radiation has gripped the minds of many consumers. And who would blame them? We are all frightened of Putin’s next move. There is plenty of uncertainty. But, let me assure you, there is one certainty:
Homeopathy does not help against the effects of nuclear radiation.
But this indisputable fact has never stopped a homeopath.
Many of them are currently trying to persuade us that homeopathy can protect us. Here, for example, is something I found on Twitter:
But there is more, much more. If you go on the Internet, you find dozens of websites making wild claims. Here is just one example:
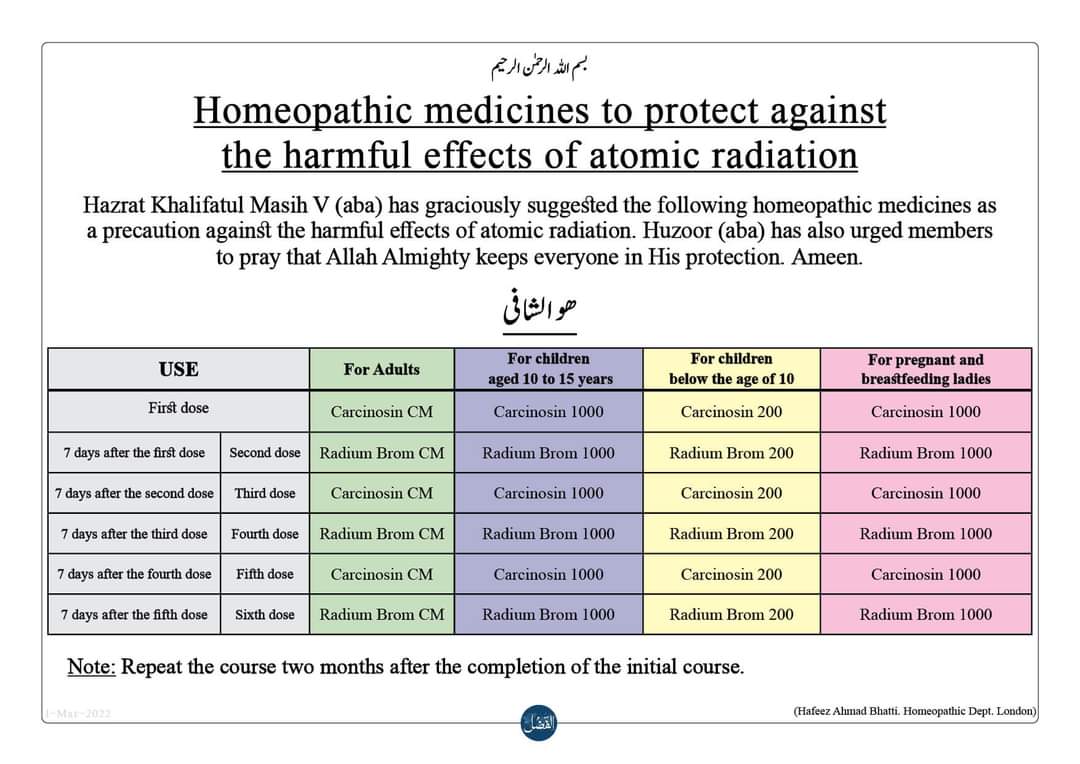
Homeopathic remedies as a preventive for adults
To be taken on an annual or bi-annual basis:
Week 1: Carcinosin in CM potency
Week 2: Radium Bromide in CM potency
Week 3: Carcinosin in CM potency
Week 4: Radium Bromide in CM potency
Week 5: Carcinosin in CM potency
Week 6: Radium Bromide in CM potency
Homeopathic remedies as a preventive for children (13 years old)
100
To be taken on an annual or bi-annual basis:
Week 1: Carcinosin in 1000 potency
Week 2: Radium Bromide in 1000 potency
Week 3: Carcinosin in 1000 potency
Week 4: Radium Bromide in 1000 potency
Week 5: Carcinosin in 1000 potency
Week 6: Radium Bromide in 1000 potency.
___________________________
Ridiculous? YES
Irresponsible? YES
Dangerous? YES
It’s high time to stop this nonsense!
I rarely follow up announcements of new studies of so-called alternative medicine (SCAM). But this one is different. It was so spectacular that almost precisely two years ago I reported about it. Here is what I wrote:
Dr. Dhanunjaya Lakkireddy, a cardiologist at the Kansas City Heart Rhythm Institute in the US, has started a trial of prayer for corona-virus infection. The study will involve 1000 patients with COVID-19 infections severe enough to require intensive care. The four-month study will investigate “the role of remote intercessory multi-denominational prayer on clinical outcomes in COVID-19 patients,” according to a description provided to the National Institutes of Health.
Inclusion Criteria:
- Male or female greater than 18 years of age
- Confirmed positive for COVID-19
- Patient admitted to Intensive Care Unit
Exclusion Criteria:
- Patients admitted to ICU for diagnosis that is not COVID-19 positive
(Not giving informed consent is not listed as an exclusion criterion!)
Half of the patients, randomly chosen, will receive a “universal” prayer offered in five denominational forms, via:
- Buddhism,
- Christianity,
- Hinduism,
- Islam,
- Judaism.
The other 500 patients in the control group will not be prayed for by the prayer group. All the patients will receive the standard care prescribed by their medical providers. “We all believe in science, and we also believe in faith,” Lakkireddy claims. “If there is a supernatural power, which a lot of us believe, would that power of prayer and divine intervention change the outcomes in a concerted fashion? That was our question.”
The outcome measures in the trial are
- the time patients remain on ventilators,
- the number of patients who suffer from organ failure,
- the time patients have to stay in intensive care,
- the mortality rate.
________________________________________
For months, I have now been looking out for the results of this study. It must long be finished now. The results cannot be difficult to analyze. The publication of such a sensational trial should not be a problem. If the findings are positive, even top journals would be keen to publish them. If they are negative, they would still be worth reporting.
So, where are they?
I could not find a trace of them!
Why not?
I was puzzled and became more and more frustrated.
Until I had the obvious idea of looking at the website that reported the above details two years ago. There was the answer to my questions:
“Recruitment Status: Terminated (Due to the low enrollment, this study is closed. Analysis of data is not performed.)”
But how can this be?
What can possibly be the reason for an enrollment that was too low to properly conclude this trial?
- There were certainly enough COVID patients (contrary to what was claimed earlier, the sample size is now given at merely 200).
- Many of these US patients would, of course, be religious and thus welcome some divine intervention.
So, why might such a trial fail? I can only think of two reasons:
- The execution of the trial was sloppy and half-hearted.
- The research question was too daft for participants to consent.
Whatever the reason, I find it sad, possibly even unethical that research funds are being wasted on such nonsense.
PS
The sponsor of this study was the Kansas City Heart Rhythm Institute. The director of the Kansas City Heart Rhythm Institute is Dhanunjaya Lakkireddy, the principal investigator of this trial.
PPS
When the study was first announced in 2020, it received huge publicity. I, therefore, think that the investigators should have had the decency to also publicly announce that they failed to conclude it.
Yesterday I received the following interesting email: 
Pfizer your God father has now officially released the list ofAdverse events.. it’s huge.. and it’s official…If you guys had half a brainYou would have seen this coming.. calling others quacks..Pfizer clowns need to be hung on a tree just like Judas..
Is this a death threat?
Probably!
Never mind, I am getting used to them.
The first one that I remember came when I was still working at my department in Exeter. We had to call the police who instructed my secretaries how to identify letter bombs without opening them. We had reason to believe that such a device had been posted to me. Not a nice experience!
Since then, death threats have arrived with some regularity.
The one above, however, seems special.
I do not recall advertising the Pfizer vaccine on this blog and elsewhere. It seems therefore that the author (who used the following email address: John <[email protected]>) is more than mildly deranged.
Am I worried? No, not about my safety (but a little about John, I must admit). I have long learned that such aggressions of this nature are a sign that I am probably on the right path. They are, in other words, a victory of reason over unreason.
So, maybe I will start advertising the Pfizer vaccine after all?
The Nobel Prize laureate Luc Montagnier has died at the age of 89.
Montagnier became the hero of the realm of homeopathy when he published findings suggesting that ultra-molecular dilutions are not just pure water but might have some activity. In this context, he has been mentioned repeatedly on this blog. During the years that followed his support for homeopathy, things got from bad to worse, and Montagnier managed to alienate most of the scientific community.
Amongst other things, he became a champion of the anti-vax movement, supported the view that vaccination causes autism, and argued that viral infections including HIV could be cured by diet. During the pandemic, he then claimed that Sars-CoV-2 had originated from a laboratory experiment attempting to combine coronavirus and HIV. On French television, he claimed that vaccination was an “enormous mistake” that would only promote the spread of new variants.
Before Montagnier became a victim of ‘Nobelitis‘, he had a brilliant career as a virologist in his world-famous Paris lab. A co-worker of Montagnier, Barré-Sinoussi, managed to isolate a retrovirus from an AIDS patient in 1983. They called it ‘lymphadenopathy-associated virus’, and concluded that it may be involved in several pathological syndromes, including AIDS.
Meanwhile, in the US, Gallo had identified a family of immunodeficiency retroviruses that he called human T-lymphotropic virus (HTLV). In 1984, Gallo announced that one of these viruses was the cause of AIDS. The US government swiftly patented a blood test for detecting antibodies to it. Thus it became possible to screen for the virus in the blood.
When it became clear that material used in Gallo’s studies included samples that Montagnier had supplied in 1983, one of the fiercest rows in the history of science ensued. Eventually, negotiations between the two governments settled it by resolving that the two scientists should be equally credited. In 2002, Gallo and Montagnier published a joint paper acknowledging each other’s role: Montagnier’s team discovered HIV, and Gallo’s proved it caused AIDS. When Gallo was excluded from the Nobel prize given in 2008 to Montagnier and Barré-Sinoussi, the world of science was stunned. The spectacular dispute between Galo and Montagnier became the subject of a movie and several books.
Montagnier died on 8/2/2022 leaving behind his wife Dorothea and their three children, Anne-Marie, Francine, and Jean-Luc.
Dr Akbar Khan, MD, represents a novel and exciting avenue through which, in this case, a conventionally- trained family physician has come to embrace a broad array of integrative techniques; he witnessed first hand the immense magnitude of safety and efficacy of the practice … Dr Khan describes with frustration the lack of interest displayed by conventional practitioners for safe and effective solutions simply because they come from the realm of natural medicine. “My greatest concern is helping patients.”

From left to right: Douglas Andrews, Akbar Khan, Silvana Marra and Humaira Khan
From left to right: Douglas Andrews, Akbar Khan, Silvana Marra and Humaira Khan[/caption]
An article in the ‘Toronto Sun’, however, tells a very different story. The doctor was found ‘incompetent’ in the treatment of cancer patients. Akbar Khan told one patient she had leukemia when she did not. He told others they were improving under his alternative remedies while their cancer was actually advancing. One of them was a little boy dying of a brain tumor.
Now the Toronto family doctor has been found guilty by the Ontario Physicians and Surgeons Discipline Tribunal of
- incompetence,
- failure to maintain the standard of practice,
- and conduct that’s disgraceful, dishonorable or unprofessional
in his care of a total of 12 patients between 2012 and 2017. “Whether it was ‘snake oil,’ ‘witches’ brew’ or otherwise, whatever it was that Dr. Khan was offering his patients, it was not what he claimed,” concluded the tribunal in its decision. “In doing so, Dr. Khan set aside his obligations as a physician to uphold the College’s CAM and consent policies, and in doing so, he failed his patients.”
Khan is the founder of the Medicor Cancer Centres, which offer “unique non-toxic approaches to cancer treatment.” He treated terminally-ill patients with the unproven treatments that he called “SAFE Chemotherapy” billed as “lifesaving” and more effective than conventional chemo.
There was insufficient science and evidence to support the conclusion that “SAFE chemotherapy” works, or that it can help people in the way that Dr. Khan claims it can, and he should not have used it,” the tribunal found. Yet, Khan never told his patients it wasn’t working. According to the college’s summary: “Therapy stopped only when his patients either could not afford it any longer, their condition had deteriorated to such a degree that they could not tolerate it, they were so ill that they were admitted to hospital, or they died.”
According to the tribunal, Khan’s patients paid (US)$4,200 for one cycle of “SAFE chemotherapy”, and they received between five to 24 cycles of it. One of the most heartbreaking cases involved Khan’s treatment of a six-year-old boy with brain cancer. In 2017, his parents rejected treating him with lifesaving chemo and radiation and transferred his care to Khan, who prescribed Dichloroacetate (DCA) — which is a medication usually used for metabolic disorders, and not a proven cancer treatment. When a follow-up MRI showed their son’s tumor had grown and progressed to his spine, Khan told them it must be wrong and “his current therapy is actually working very well!” The boy died in 2018.
In another disturbing case, Khan used an “unapproved” test to diagnose a 59-year-old woman with acute leukemia — and informed her by email. He treated the devastated woman with honokol, a biological extract from magnolia bark, and Low Dose Naltrexone (LDN) — both of which are “not informed by evidence and science,” and “not the appropriate treatment for this patient’s presumed cancer.” Khan referred her to an oncologist who performed a bone marrow biopsy and then gave her the good news: “You do not have cancer. You’ve never had cancer. Go home and enjoy your life.” Yet, Khan insisted the oncologist was wrong. “We were frankly shocked that instead of reassuring Ms. B that her ordeal of worrying that she had leukemia could come to a close, Dr. Khan insisted to Ms. B that indeed, she did still have leukemia and urged her to keep taking LDN ‘to keep this under control,’” the tribunal wrote. “In short, Dr. Khan gave Ms. B a diagnosis that she did not have, for which he sold her a remedy that she did not need, which — as per evidence and science — turned out to be no remedy at all.”Khan’s response to the newspaper: “Since the legal process is still ongoing with the CPSO, I know my lawyer Marie Henein would not like me to comment at this time. Perhaps in the near future, I will be able to share with you another side to the story. If so, I will contact you.”
A penalty hearing has yet to be scheduled.
In case you are interested, here is a short CV of Dr. Khan:
| 2019 | FAAO – Fellow of the American Academy of Ozone Therapy |
| 2018 | Certified medical ozone therapy doctor (general ozone therapy, basic ProlozoneTM therapy and advanced ProlozoneTM therapy), certified by the American Academy of Ozone Therapy |
| 2018 | IMD, Integrative Medical Doctor (Board of Integrative Medicine) DHS, Doctor of Humanitarian Service (Board of Integrative Medicine) |
| 1994 | CCFP, Certificant of the College of Family Physicians of Canada (University of Toronto). |
| 1992 | MD, Doctor of Medicine (University of Toronto). |
On this blog, I have been regularly discussing the risks of so-called alternative medicine (SCAM). In particular, I have often been writing about the risks of chiropractic spinal manipulations.
Why?
Some claim because I have an ax to grind – and, in a way, they are correct: I do feel strongly that consumers should be warned about the risks of all types of SCAM, and when it comes to direct risks, chiropractic happens to feature prominently.
But it’s all based on case reports which are never conclusive and usually not even well done.
This often-voiced chiropractic defense is, of course, is only partly true. But even if it were entirely correct, it would beg the question: WHY?
Why do we have to refer to case reports when discussing the risks of chiropractic? The answer is simple: Because there is no proper system of monitoring its risks.
And why not?
Chiropractors claim it is because the risks are non-existent or very rare or only minor or negligible compared to the risks of other therapies. This, I fear, is false. But how can I substantiate my fear? Perhaps by listing a few posts I have previously published on the direct risks of chiropractic spinal manipulation. Here is a list (probably not entirely complete):
- Chiropractic manipulations are a risk factor for vertebral artery dissections
- Vertebral artery dissection after chiropractic manipulation: yet another case
- The risks of (chiropractic) spinal manipulative therapy in children under 10 years
- A risk-benefit assessment of (chiropractic) neck manipulation
- The risk of (chiropractic) spinal manipulations: a new article
- New data on the risk of stroke due to chiropractic spinal manipulation
- The risks of manual therapies like chiropractic seem to out-weigh the benefits
- One chiropractic treatment followed by two strokes
- An outstanding article on the subject of harms of chiropractic
- Death by chiropractic neck manipulation? More details on the Lawler case
- Severe adverse effects of chiropractic in children Another serious complication after chiropractic manipulation; best to avoid neck manipulations altogether, I think
- Ophthalmic Adverse Effects after Chiropractic Neck Manipulation
- Is chiropractic treatment safe?
- Cervical artery dissection and stroke related to chiropractic manipulation
- We have an ethical, legal and moral duty to discourage chiropractic neck manipulations
- Cerebral Haemorrhage Following Chiropractic ‘Activator’ Treatment
- Vertebral artery dissection after chiropractic manipulation: yet another case
- Horner Syndrome after chiropractic spinal manipulation
- Phrenic nerve injury: a rare but serious complication of chiropractic neck manipulation
- Chiropractic neck manipulation can cause stroke
- Chiropractic and other manipulative therapies can also harm children
- Complications after chiropractic manipulations: probably rare but certainly serious
- Disc herniation after chiropractic
- Evidence for a causal link between chiropractic treatment and adverse effects
- More on the risks of spinal manipulation
- The risk of neck manipulation
- “As soon as the chiropractor manipulated my neck, everything went black”
- Spinal epidural haematoma after neck manipulation
- New review confirms: neck manipulations are dangerous
- Top model died ‘as a result of visiting a chiropractor’
- Another wheelchair filled with the help of a chiropractor
- Spinal manipulation: a treatment to die for?
Of course, one can argue about the conclusiveness of this or that case report, but I feel that the collective evidence discussed in these posts makes my point abundantly clear:
chiropractic spinal manipulation is not safe.
People often say WHAT’S THE HARM?
Why not let Prince Charles promote any nonsense he likes?
Let him be!
He means well!
He is not harming anyone!
I think this attitude is not correct. Charles’s advocacy of quackery is by no means harmless. This is one of the points I have been trying to make repeatedly, most recently in my biography of Charles.
And there are plenty of examples for this; just think of the Gerson therapy (a whole chapter in the said book). Another, less obvious example is homeopathy. Charles has promoted homeopathy during all his adult life. When he fell ill with COVID in the early phase of the pandemic, the realm of homeopathy predictably decided that he recovered so well because he homeopathic treatment. A report dated 7 April 2020, for example, is quite clear about it:
British Crown Prince Charles has been “101 per cent” cured of COVID-19 using Ayurveda and Homeopathy treatment, Union Minister of State for AYUSH Shripad Naik … “I am proud that the Ministry which I head, managed to cure such a great man, there is no greater credit than this. He may have some problem (admitting to it) because the system in his country does not give recognition to Ayurveda. He may have felt he would violate rules, that is why his refusal to admit is obvious,” Naik told a local cable news channel in an interview late on Monday. “I believe 101 per cent, that he has been cured (using Ayurveda and Homeopathy),” Naik also said.
On April 2, Naik had told a press conference in Goa, that Prince Charles had been cured of COVID-19 after seeking treatment from a Bengaluru-based alternative treatment resort, SOUKYA International Holistic Health Centre’ run by a doctor Isaac Mathai. A day after his statement, Clarence House, the official residence of Prince Charles had said that the claim was incorrect and that the royal “followed the medical advice of the National Health Service in the UK and nothing more”. The royal had been diagnosed COVID-19 positive last month.
Naik in the cable TV interview on Monday continued to insist that Ayurveda and Homeopathy had indeed cured the Prince and that it was a “victory” for Indian traditional medicine systems. Naik also said that there was no need to disbelieve the doctor Isaac Mathai, who cured Prince Charles. “The man (Dr. Mathai) himself is saying this. He is a doctor, an owner of a resort, he is trustworthy, when he says this, it is a victory of our Indian system,” Naik said.
The royal denial had little effect; Indian officials had persuaded themselves and key decision-makers that Charles’s case was proof for homeopathy’s effectiveness against COVID. Consequently, homeopathy was widely used for that purpose. As a result, millions of Indians deemed themselves sufficiently protected (possibly not taking other measures seriously). And the rest is history: in the summer of 2020, about 1000 Indians per day were reported to have died of COVID (the number of unreported deaths was estimated to be even higher).
The point I am trying to make is this: the promotion of quackery by a ‘VIP’ can have dramatic unforeseen consequences, even if (like in Charles’s case) a direct cause-effect relationship is impossible to prove.