death
Muscular dystrophies are a rare, severe, and genetically inherited disorders characterized by progressive loss of muscle fibers, leading to muscle weakness. The current treatment includes the use of steroids to slow muscle deterioration by dampening the inflammatory response. Chinese herbal medicine (CHM) has been offered as adjunctive therapy in Taiwan’s medical healthcare plan, making it possible to track CHM usage in patients with muscular dystrophies. This investigation explored the long-term effects of CHM use on the overall mortality of patients with muscular dystrophies.
A total of 581 patients with muscular dystrophies were identified from the database of Registry for Catastrophic Illness Patients in Taiwan. Among them, 80 and 201 patients were CHM users and non-CHM users, respectively. Compared to non-CHM users, there were more female patients, more comorbidities, including chronic pulmonary disease and peptic ulcer disease in the CHM user group. After adjusting for age, sex, use of CHM, and comorbidities, patients with prednisolone usage exhibited a lower risk of overall mortality than those who did not use prednisolone. CHM users showed a lower risk of overall mortality after adjusting for age, sex, prednisolone use, and comorbidities. The cumulative incidence of the overall survival was significantly higher in CHM users. One main CHM cluster was commonly used to treat patients with muscular dystrophies; it included Yin-Qiao-San, Ban-Xia-Bai-Zhu-Tian-Ma-Tang, Zhi-Ke (Citrus aurantium L.), Yu-Xing-Cao (Houttuynia cordata Thunb.), Che-Qian-Zi (Plantago asiatica L.), and Da-Huang (Rheum palmatum L.).
The authors concluded that the data suggest that adjunctive therapy with CHM may help to reduce the overall mortality among patients with muscular dystrophies. The identification of the CHM cluster allows us to narrow down the key active compounds and may enable future therapeutic developments and clinical trial designs to improve overall survival in these patients.
I disagree!
What the authors have shown is a CORRELATION, and from that, they draw conclusions implying CAUSATION. This is such a fundamental error that one has to wonder why a respected journal let it go past.
A likely causative explanation of the findings is that the CHM group of patients differed in respect to features that the statistical evaluations could not control for. Statisticians can never control for factors that have not been measured and are thus unknown. A possibility in the present case is that these patients had adopted a different lifestyle together with employing CHM which, in turn, resulted in a longer survival.
As we have discussed ad nauseam on this blog, spinal manipulation therapy (SMT) can cause serious adverse events, including spinal epidural hematoma (SEH), an emergency that can cause severe neurological dysfunction. Chinese surgeons have reported three cases of SEH after SMT.
- The first case was a 30-year-old woman who experienced neck pain and numbness in both upper limbs immediately after SMT. Her symptoms persisted after 3 d of conservative treatment, and she was admitted to our hospital. Magnetic resonance imaging (MRI) demonstrated an SEH, extending from C6 to C7.
- The second case was a 55-year-old man with sudden back pain 1 d after SMT, numbness in both lower limbs, an inability to stand or walk, and difficulty urinating. MRI revealed an SEH, extending from T1 to T3.
- The third case was a 28-year-old man who suddenly developed symptoms of numbness in both lower limbs 4 h after SMT. He was unable to stand or walk and experienced mild back pain. MRI revealed an SEH, extending from T1 to T2.
All three patients underwent surgery after failed conservative treatment. Blood clots were found during the operation in case 1 and case 2, and the postoperative pathology confirmed a hematoma. In case three, a vein ruptured during the operation, causing massive bleeding. The three patients recovered to ASIA grade E on day 5, 1 wk, and day 10 after surgery, respectively. All patients returned to normal after 3 mo of follow-up.
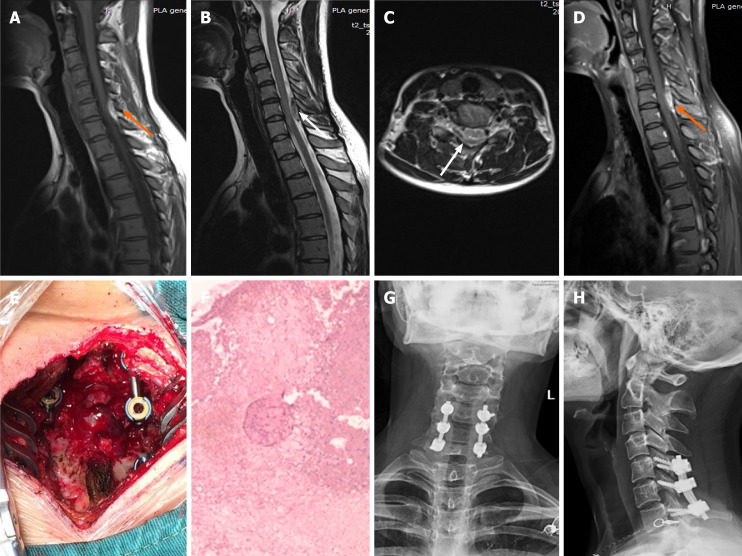
Imaging examinations of case 1. A: T1-weighted preoperative magnetic resonance imaging (MRI) image shows high signal intensity (orange arrow); B and C: Preoperative T2-weighted image shows low signal intensity, and an axial T2-weighted image demonstrates that the hematoma occurred in the posterior region (white arrow); D: Preoperative enhanced MRI suggests an enhanced hematoma signal (orange arrow); E: Intraoperative photograph shows that spinal cord compression has recovered; F: Postoperative pathology suggested a hematoma; G and H: X-ray at the 3-mo follow-up indicated intact internal fixation.
The authors concluded that before proceeding with SMT, each patient should be evaluated in detail and checked for risk factors. In cases where the physical condition changes rapidly, physicians should be alert to the danger and send the patient to the emergency department for a complete MRI examination. We recommend surgery if neurological symptoms appear.
In their paper, the authors also review 15 further cases of SEH that have been previously published. They stress several times in their article that this complication is rare. In my view, this begs the question: how do they know? As there is no post-marketing surveillance of chiropractors or other clinicians doing SMT, I would insist that nobody can be sure about the true incidence of SEH or any other complication after SMT.
Recently, I wrote about the court case of a French naturopath. Last week, the judge has issued his verdict. Miguel Barthéléry was sentenced to a two-year suspended prison term and to a fine of 5 000 Euros. Two cancer patients had died following his treatments and recommendations. Barthéléry was also found guilty of impersonating a doctor and illegally practising medicine. In addition, he was also banned for life from practising as a healthcare professional.
to a two-year suspended prison term and to a fine of 5 000 Euros. Two cancer patients had died following his treatments and recommendations. Barthéléry was also found guilty of impersonating a doctor and illegally practising medicine. In addition, he was also banned for life from practising as a healthcare professional.
The Paris criminal court found that Miguel Barthéléry had deliberately created confusion about his qualifications by presenting himself as a doctor on the internet and in text messages to the two victims. The defendant had claimed to have a doctorate and a post-doctorate from the United States. The judgment “has the consequence of dissuading all those who engage in the same abuses, they are now warned that we can not do anything with the health of people,” said the judge.
The case had begun in February 2019 with the complaint of the companion of a man who had died two months earlier of testicular cancer. Diagnosed in 2016, the patient had not consulted a doctor but had preferred to follow a “health plan” drawn up by the naturopath. It was based on fasting and cures, raw food, and essential oils. Later, the family of a Belgian physiotherapist, who died of uterine cancer at the age of 39, joined the legal case. However, according to Code Source, the Parisien podcast, the case is more extensive, with seven further suspicious deaths of Barthéléry’s patients.
Barthéléry’s lawyer said that the decision “raises questions more generally about the appreciation that we now have of alternative therapeutic practices, which now seem, although not prohibited by law, to be subject to condemnation by the courts.”
Kratom (Mitragyna speciosa, Korth.) is an evergreen tree that is indigenous to Southeast Asia. It is increasingly being used as a recreational drug, to help with opium withdrawal, and as a so-called alternative medicine (SCAM) for pain, erectile dysfunction, as a mood stabilizer, and for boosting energy or concentration. When ingested, Kratom leaves produce stimulant and opioid-like effects (see also my previous post).

Kratom contains 7‑hydroxymitragynine, which is active on opioid receptors. The use of kratom carries significant risks, e.g. because there is no standardized form of administration as well as the possibility of direct damage to health and of addiction.
There are only very few clinical trials of Kratom. One small placebo-controlled study concluded that the short-term administration of the herb led to a substantial and statistically significant increase in pain tolerance. And a recent review stated that Kratom may have drug interactions as both a cytochrome P-450 system substrate and inhibitor. Kratom does not appear in normal drug screens and, especially when ingested with other substances of abuse, may not be recognized as an agent of harm. There are numerous cases of death in kratom users, but many involved polypharmaceutical ingestions. There are assessments where people have been unable to stop using kratom therapy and withdrawal signs/symptoms occurred in patients or their newborn babies after kratom cessation. Both banning and failure to ban kratom places people at risk; a middle-ground alternative, placing it behind the pharmacy counter, might be useful.
In Thailand, Kratom had been outlawed since 1943 but now it has become (semi-)legal. Earlier this year, the Thai government removed the herb from the list of Category V narcotics. Following this move, some 12,000 inmates who had been convicted when Kratom was still an illegal drug received amnesty. However, Kratom producers, traders, and even researchers will still require licenses to handle the plant. Similarly, patients looking for kratom-based supplements will need a valid prescription from licensed medical practitioners. Thai law still prohibits bulk possession of Kratom. Users are encouraged to handle only minimum amounts of the herb to avoid getting prosecuted for illegal possession.
In 2018, the US Food and Drug Administration stated that Kratom possesses the properties of an opioid, thus escalating the government’s effort to slow usage of this alternative pain reliever. The FDA also wrote that the number of deaths associated with Kratom use has increased to a total of 44, up from a total of 36 since the FDA’s November 2017 report. In the majority of deaths that the FDA attributes to Kratom, subjects ingested multiple substances with known risks, including alcohol.
In most European countries, Kratom continues to be a controlled drug. In the UK the sale, import, and export of Kratom are prohibited. Yet, judging from a quick look, it does not seem to be all that difficult to obtain Kratom via the Internet.
This shocking paper presents 5 cases of patients with moderate to severe COVID-19 infections, 2 of them hospitalized in the intensive care unit, who were successfully treated with homeopathy. All 5 patients responded to homeopathic treatment in an unexpectedly short time span (in fact, it took up to 8 days), improving both physically and mentally.
The authors concluded that the present case series emphasizes the rapidity of response among moderate to severely ill patients to homeopathic treatment, when conventional medical options have been unable to relieve or shorten the disease. The observations described should encourage use of homeopathy in treating patients with COVID-19 during the acute phase of the disease.
If I hear about patients suffering from a cold, or tennis elbow, or otitis, or back pain, or allergy who responded to homeopathic treatment in an unexpectedly short time span, I tend to giggle and usually consider it a waste of time to explain that the observed outcome most likely is not a RESPONSE to homeopathic treatment but a non-causally related by-product. Correlation is not causation! What caused the outcome was, in fact, the natural history of the condition which would have improved even without homeopathy. To make this even clearer, I sometimes ask the homeopath: HOW DO YOU KNOW THAT THE PATIENT WOULD NOT HAVE IMPROVED EVEN FASTER IF YOU HAD NOT GIVEN HIM THE HOMEOPATHIC REMEDY? This question sometimes (sadly not always) leads to the realization that homeopathy may not have caused the outcome.
But when, in the middle of a pandemic during which millions of people died and continue to die, someone writes in a medical journal that 5 COVID patients responded to homeopathic treatment in an unexpectedly short time span, I feel compelled to disclose the statement as pure, unethical, irresponsible, and dangerous quackery.
The 5 patients with COVID-19 were hospitalized at a tertiary medical center in Jerusalem for moderate to severe
COVID-19-related symptoms. Each of them requested homeopathic treatment in addition to conventional therapy from the hospital’s ‘Center for Integrative Complementary Medicine’. All 5 patients were over 18 years old and had confirmed COVID-19 infection at the time of admission. They received their homeopathic medications as small round pills (globules); no further information about the homeopathic treatment was provided. Similarly, we also do not learn whether some patients who did not receive homeopathy recovered just as quickly (I am sure that worldwide thousands did), or whether some patients who did get homeopathic remedies failed to recover.
To make matters worse, the authors of this paper state this:
Several conclusions are evident from the cases presented:
1 homeopathy’s effect may be expected within minutes or, at most, hours;
2 contrary to classical homeopathic consultations, which may extend over an hour, correct medications for patients with acute COVID-19 symptoms may be determined in minutes;
3 there were no observable adverse effects to homeopathic treatment of COVID-19;
4 therapy can be administered via telehealth services, increasing safety of treating patients with active infection;
5 patient satisfaction was high; scoring their experience of homeopathic therapy on a 7-point scale, ranging
from “It greatly improved my condition” to “It greatly aggravated my condition,” all 5 patients indicated it
had greatly improved their condition.
The possibility that the outcomes are not causally related to the homeopathic treatment seems to have escaped the authors. The harm that can be done by such an article seems obvious: fans of homeopathy might be misled into assuming that homeopathy is an effective therapy for COVID infections and other serious conditions. It is not hard to imagine that this error would cost many lives.
The authors state in their article that, to the best of their knowledge, this is the first time that a tertiary medical center has permitted homeopathic therapy of patients under treatment for COVID-19-related illness.
I sincerely hope that it is also the last time!
Last week, a naturopath who has been practicing naturopathy for more than three years, appeared in the Paris High Court. He is accused of “illegal practice of medicine” and of “usurpation of the title of doctor” after two of his cancer patients died.
Charles B. was diagnosed with testicular cancer in 2016 but wanted to avoid traditional medicine. In March 2017, he consulted the naturopath, Miguel B., who studied for fourteen years in the United States and has a degree in biochemistry and a doctorate in molecular medicine. He knew that his qualifications did not allow him to practice in France and presented himself as a naturopath. Knowing about his client’s cancer, Miguel B. drew up a health plan for him that included numerous fasts and purges to detox his body.
In the following months, the cancer spreads to the lungs and brain. Charles B. wrote to his naturopath in early February: “Great pain, don’t know what to do”. The naturopath continued his advice: “You should go on a diet, rest and purge in the evening. In court, Charles B.’s father recalled a conversation between his son and Miguel B. during which the latter had said to Charles B.: “It would be a pity if you were to undergo this chemotherapy.” On 22 February 2018, now weighing only 59 kg, Charles B. finally decided to start chemotherapy. But it was already too late, and he died on 18 December 2018, at the age of 41, of a cancer from which more than 98% of patients usually recover. Charles B.’s wife stated that the naturopath had told her husband that he would not need chemotherapy. She believes that the defendant is “responsible and even guilty” of her husband’s death.
The family of another patient of Miguel B. has also joined the case. Catherine F., who had been suffering from cervical cancer, died at the age of 39. She had followed, among other treatments, a fast recommended by the naturopath and was one of 149 further patients whose list was found on a USB stick belonging to the defendant.
The General Chiropractic Council (GCC) regulates chiropractors in the UK, Isle of Man, and Gibraltar to ensure the safety of patients undergoing chiropractic treatment. The GCC sets the standards of chiropractic practice and professional conduct that all chiropractors must meet.

By providing a lengthy ruling in the case of the late John Lawler and his chiropractor, Arlene Scholten, the GCC has recently established new standards for chiropractors working in the UK, Isle of Man, and Gibraltar (see also today’s article in The Daily Mail). If I interpret the GCC’s ruling correctly, a UK chiropractor is henceforth allowed to do all of the following things without fearing to get reprimanded, as long as he or she produces evidence that the deeds were done not with malicious intentions but in a state of confusion and panic:
- Treat a patient with treatments that are contraindicated.
- Fail to obtain informed consent.
- Pose as a real doctor without informing the patient that the practitioner is just a chiropractor who has never been near a medical school.
- Cause the death of a patient by treatment to the neck.
- Administer first aid in a way that makes matters worse.
- Tell lies to the ambulance men who consequently failed to employ a method of transport that would save the patient’s life.
- Keep inaccurate patient records that conceal what treatments were administered.
In previous years, the job of a chiropractor had turned out to be demanding, difficult, and stressful. This was due not least to the GCC’s professional standards which UK chiropractors were obliged to observe. The code of the GCC stated prominently that “our overall purpose is to protect the public.”
All this is now a thing of the past.
The new ruling changed everything. Now, UK chiropractors can relax and can happily pursue their true devotion, namely to keep their bank manager happy, while not worrying too much about the welfare and health of their patients.
In the name of all UK chiropractors, I herewith express my thanks to the GCC for unashamedly protecting first and foremost the interests of their members, while tacitly discarding medical ethics and evidently not protecting the public.
MAKE CHIROPRACTIC GREAT AGAIN!
On 19-30 April 2021 & 1-2 September, 2021 the Professional Conduct Committee of the General Chiropractic Council considered the case of Arleen Scholten, the chiropractor who treated John Lawler, the patient who died after her treatment. Details of the case can be found in the following posts:
- Former chiropractor fined after death of MS patient receiving hyperbaric oxygen therapy
- Death by chiropractic: thoughts about the sad case of Mr Lawler
- The death of Mr Lawler highlights the scandals of chiropractic
- Death by chiropractic neck manipulation? More details on the Lawler case
The Committee considered there had been breaches of the Code, those breaches occurred as a result of Mrs. Scholten’s state of mind at the time and not as a result of a deliberate intention on her part to be inaccurate or misleading. In light of those circumstances, the Committee considered other members of the profession and fully informed members of the public would not consider her failings to be morally reprehensible or deplorable, but rather would consider them regrettable but understandable in the exceptional, albeit tragic, circumstances of this case. The Committee, therefore, agreed with the GCC’s expert witness Mr Brown and did not think Mrs Scholten’s conduct fell far short of the standard required of a registered chiropractor. The Committee was not satisfied, therefore, that her behaviour amounted to unacceptable professional conduct. Accordingly, the Committee found the allegation of UPC not to be well-founded.
How can this be right?
To remind us of the case, here is what I wrote about it previously:
The tragic case of John Lawler who died after being treated by a chiropractor has been discussed on this blog before. Naturally, it generated much discussion which, however, left many questions unanswered. Today, I am able to answer some of them.
- Mr Lawler died because of a tear and dislocation of the C4/C5 intervertebral disc caused by considerable external force.
- The pathologist’s report also shows that the deceased’s ligaments holding the vertebrae of the upper spine in place were ossified.
- This is a common abnormality in elderly patients and limits the range of movement of the neck.
- There was no adequately informed consent by Mr Lawler.
- Mr Lawler seemed to have been under the impression that the chiropractor, who used the ‘Dr’ title, was a medical doctor.
- There is no reason to assume that the treatment of Mr Lawler’s neck would be effective for his pain located in his leg.
- The chiropractor used an ‘activator’ which applies only little and well-controlled force. However, she also employed a ‘drop table’ which applies a larger and not well-controlled force.
I have the permission to publish the submissions made to the coroner by the barrister representing the family of Mr Lawler. The barrister’s evidence shows that:
The chiropractor, Mrs. Scholten, had been accused by the GCC of unacceptable professional conduct. The exact text of the GCC reads as follows :
1. Between 31 July 2017 and 11 August 2017, you provided chiropractic care and
treatment to Patient A at Chiropractic 1st, 68 The Mount, North Yorkshire, YO24 1AR,
(‘the Clinic’).
2. On 11 August 2017 you provided treatment to Patient A which included:
a. a drop technique applied to the thoracic spine;
b. the use of an Activator applied to the thoracic spine;
c. the use of an Activator applied to the cervical spine.
3. Following the drop technique, Patient A indicated he was in discomfort and had lost sensation in his arms and you inappropriately continued treatment.
4. During the course of a subsequent 999 telephone call:
a. you told the call handler that Patient A had laid on the adjusting table and you had used the Activator on his midback;
b. you told the call handler that when you were using the Activator on Patient A’s midback he had said his hands had gone numb;
c. you told the call handler that as Patient A was elderly you had never used any manual adjustment on Patient A;
d. you omitted to tell the call handler that you had used a drop technique on Patient A;
e. you omitted to tell the call handler that Patient A had first expressed discomfort following the drop technique;
f. you omitted to tell the call handler that you had treated Patient A’s cervical spine.
5. When paramedics arrived at the Clinic:
a. you told them words to the effect that you had manipulated Patient A’s midback with the use of an Activator;
b. you told them words to the effect that Patient A had first complained of discomfort when you had been using the Activator on his midback;
c. you omitted to tell the paramedics you had used a drop technique on Patient A;
d. you omitted to tell the paramedics that Patient A had first expressed discomfort following the drop technique;
e. you omitted to tell the paramedics that you had treated Patient A’s cervical spine;
f. you demonstrated the force applied by an Activator on one of the paramedic’s arms.
6. In Patient A’s records for 11 August 2017:
a. you recorded that you had used the Activator on Patient A’s thoracic spine at T2/3 level;
b. you recorded that Patient A had directly said his arms felt numb;
c. you omitted to record that you had used a drop technique on Patient A;
d. you omitted to record that you had treated Patient A’s cervical spine.
7. Your comments and omissions as set out above at 4 and/or 5, and/or as recorded at 6 above, were;
a. inaccurate;
b. misleading;
c. dishonest in that you intended to mislead as to the precise details of the treatment you had provided Patient A
Mr Goldring, on behalf of Mrs Scholten, indicated that the following facts were admitted: Particulars 1, 2(a), 4(a), 4(b), 4(c), 4(d), 5(a), 5(b), 5(c), 5(f), 6(a), 6(b), 6(c) and 7(a) and (b), insofar as they related to the aforementioned admitted facts. The Chair therefore announced that those matters were found proved. Later in the proceedings Mr Goldring indicated that 7(a) and 7(b) were not in fact admitted in respect of 4(c) and 6(b), since it was Mrs Scholten’s case that she had not used any manual adjustment on Patient A, (Particular 4(c)) and the record that Patient A had directly said his arms felt numb was accurate, (Particular 6(b)). Accordingly, the Chair formally announced that position.
END OF QUOTES
I am totally baffled by this ruling.
- What about the fact that the chiropractor’s treatment was not even indicated?
- What about the fact that no informed consent was obtained?
- What about the fear that the chiropractor moved her patient after the injury had happened and made an attempt of ‘mouth to mouth’ resuscitation which seems to have aggravated the injury?
- What about the fact that she misled the paramedics which then caused them not to stabilise Mr. Lawlwer’s neck?
Is the GCC truly saying that, as long as a chiropractor panics, all these mistakes can be excused? I am at a complete loss trying to understand the GCC ruling and very much hope that someone can explain it to me.
Acupuncture is usually promoted as a safe therapy. This may be good marketing but, sadly, it is not the truth. About 10% of all patients experience mild to moderate adverse effects such as pain or bleeding. In addition, there are well-documented complications, for instance:
However, there have been few reports of deaths due to pneumothorax after acupuncture treatment, especially focused on electroacupuncture.
Japanese authors recently reported an autopsy case of a man in his 60s who went into cardiopulmonary arrest and died immediately after receiving electroacupuncture. Postmortem computed tomography (PMCT) showed bilateral pneumothoraces, as well as the presence of numerous gold threads embedded subcutaneously. An autopsy revealed two ecchymoses in the right thoracic cavity and a pinhole injury on the lower lobe of the right lung, suggesting that the needles had penetrated the lung. There were marked emphysematous changes in the lung, suggesting that rupture of bullae might also have contributed to bilateral pneumothoraces and fatal outcomes. The acupuncture needles may have been drawn deeper into the body than at the time of insertion due to electrical pulses and muscle contraction, indicating the need for careful determination of treatment indications and technical safety measures, such as fail-safe mechanisms.
This is the first case report of fatal bilateral pneumothoraces after electroacupuncture reported in the English literature. This case sheds light on the safety of electroacupuncture and the need for special care when administering it to patients with pulmonary disease who may be at a higher risk of pneumothorax. This is also the first report of three-dimensional reconstructed PMCT images showing the whole-body distribution of embedded gold acupuncture threads, which is unusual.
One-sided pneumothoraxes are common events after acupuncture. Several hundred cases have been published and the vast majority of such incidents remain unpublished or even unnoticed. These events are not normally life-threatening. If ‘only’ one lung is punctured, the patient may experience breathing difficulties, but in many cases these are temporary and the patient soon recovers.
Yet a bilateral pneumothorax is an entirely different affair. If both lungs malfunction, the patient’s chances of survival are slim unless he/she is close to an intensive care unit.
You might think that it needs an especially ungifted acupuncturist to manage to puncture both lungs simultaneously. I might agree, but we need to consider that acupuncture needles are often inserted in a symmetrical fashion into the patient’s body. This means that, if the therapist puts a needle at one point of the thorax that is close to a lung, he is not unlikely to do the same on the other side.
And how does one prevent such disasters?
Easy:
- train acupuncturists properly,
- avoid needles on the upper thorax,
- or refuse acupuncture altogether.
Former chiropractor Malcolm Hooper, 61, and hyperbaric oxygen therapy provider Oxymed Pty Ltd have been fined following the death of a customer in 2016. They were each convicted of three work safety-related charges, all of failing to ensure a workplace is safe and without risks to health. Hooper was fined $176,750, while the company was fined $550,000. Oxymed was trading as HyperMed at its South Yarra premises in April 2016 when a long-term client with multiple sclerosis and a history of life-threatening seizures came in for treatment. He was later found unconscious in a single-person hyperbaric chamber, taken to hospital, and placed on life support, but died five days later.
The County Court heard that both the company and Hooper had an inadequate system in place for assessing the risks oxygen therapy could pose to clients, and an inadequate system too for developing plans to eliminate or reduce those risks. In her judgment, County Court judge Amanda Fox said HyperMed wasn’t a hospital nor a medical practice and had been described as an “alternative health facility”. Hooper had already been deregistered in 2013 by the national board for chiropractors for misleading and deceptive advertising about the benefits of hyperbaric treatment.
Hyperbaric oxygen therapy involves administering pure oxygen in a pressurised environment, with the heightened air pressure allowing a patients’ lungs to gather much more oxygen than would be possible under normal conditions. The therapy is not based on strong data. A systematic review failed to find good evidence for hyperbaric oxygen therapy as a treatment of multiple sclerosis:
Multiple sclerosis (MS) is a chronic, inflammatory, and degenerative neurological illness with no cure. It has been suggested that Hyperbaric Oxygen Therapy (HBO(2)T) may slow or reverse the progress of the disease. This article summarizes the clinical evidence for the use of HBO(2)T in the treatment of MS. We conducted a literature review focused on the interaction of hyperbaric oxygenation and MS. In particular, we appraised the clinical data regarding treatment and performed a meta-analysis of the randomized evidence using the methodology of the Cochrane Collaboration. We found 12 randomized studies in the area, all of which were performed between 1983 and 1987. A meta-analysis of this evidence suggests there is no clinically significant benefit from the administration of HBO(2)T. The great majority of randomized trials investigated a course of 20 treatments at pressures between 1.75ATA and 2.5ATA daily for 60-120 min over 4 weeks against a placebo regimen. None have tested the efficacy of HBO(2)T against alternative current best practice. No plausible benefit of HBO(2)T on the clinical course of MS was identified in this review. It remains possible that HBO(2)T is effective in a subgroup of individuals not clearly identified in the trials to date, but any benefit is unlikely to be of great clinical significance. There is some case for further human trials in selected subgroups and for prolonged courses of HBO(2)T at modest pressures, but the case is not strong. At this time, the routine treatment of MS with HBO(2)T is not recommended.
The case reminds me of that of John Lawler. Mr. Lawlwer’s chiropractor also used a therapy that was not indicated, broke his neck (to put it crudely), and subsequently proved herself more than inept in saving his life. It suggests to me that some chiros may not be trained adequately to deal with emergencies. If that is true, they should perhaps focus less on practice-building courses and more on first aid instructions.