conflict of interest
Homeopaths believe that their remedies work for every condition imaginable and that naturally includes irritable bowel syndrome (IBS). But what does the evidence show?
The aim of this pilot study was to evaluate the efficacy of individualized homeopathic treatment in patients with IBS. The study was carried out at the National Homeopathic Hospital of the Secretary of Health, Mexico City, Mexico and included 41 patients: 3 men and 38 women, mean age 54 ± 14.89 years, diagnosed with IBS as defined by the Rome IV Diagnostic criteria. Single individualized homeopathics were prescribed for each patient, taking into account all presenting symptoms, clinical history, and personality via repertorization using RADAR Homeopathic Software. The homeopathic remedies were used at the fifty-millesimal (LM) potency per the Mexican Homeopathic Pharmacopoeia starting with 0/1 and increasing every month (0/2, 0/3, 0/6). Severity scales were applied at the beginning of treatment and every month for 4 months of treatment. The evaluation was based on comparing symptom severity scales during treatment.
The results demonstrated that 100% of patients showed some improvement and 63% showed major improvement or were cured. The study showed a significant decrease in the severity of symptom scores 3 months after the treatment, with the pain score showing a decrease already one month after treatment.
The authors state that the results highlight the importance of individualized medicine regimens using LM potency, although the early decrease in pain observed could also be due to the fact that Lycopodium clavatum and Nux vomica were the main homeopathic medicine prescribed, and these medicines contain many types of alkaloids, which have shown significant analgesic effects on pain caused by physical and chemical stimulation.
The authors concluded that this pilot study suggests that individualized homeopathic treatment using LM potencies benefits patients with IBS.
Where to begin?
Let me mention just a few rather obvious points:
- A pilot study is not for evaluating the efficacy, but for testing the feasibility of a definitive trial.
- The study has no control group, therefore the outcome cannot be attributed to the treatment but is most likely due to a mixture of placebo effects, regression towards the mean, and natural history of IBS.
- The conclusions are not warranted.
- The paper was published in the infamous Altern Ther Health Med.
Just to make sure that nobody is fooled into believing that homeopathy might nonetheless be effective for IBS. Here is what the Cochrane review on this subject tells us: no firm conclusions regarding the effectiveness and safety of homeopathy for the treatment of IBS can be drawn. Further high quality, adequately powered RCTs are required to assess the efficacy and safety of clinical and individualised homeopathy for IBS compared to placebo or usual care.
In my view, even the conclusion of the Cochrane review is odd and slightly misleading. The correct conclusion would have been something more to the point:
THE CURRENT TRIAL EVIDENCE FAILS TO INDICATE THAT HOMEOPATHY IS AN EFFECTIVE TREATMENT FOR IBS.
The authors of this review start their paper with the following statement:
Acupuncture has demonstrated effectiveness for symptom management among breast cancer survivors.
This, I think, begs the following question: if they already know that, why do they conduct a systematic review of the subject?
The answer becomes clear as we read thier article: they want to add another paper to the literature that shows they are correct in their assumption.
So, they do the searches and found 26 trials (2055 patients), of which 20 (1709 patients) could be included in the meta-analysis. Unsurprisingly, their results show that acupuncture was more effective than control groups in improving pain intensity [standardized mean difference (SMD) = -0.60, 95% confidence intervals (CI) -1.06 to -0.15], fatigue [SMD = -0.62, 95% CI -1.03 to -0.20], and hot flash severity [SMD = -0.52, 95% CI -0.82 to -0.22]. Compared with waitlist control and usual care groups, the acupuncture groups showed significant reductions in pain intensity, fatigue, depression, hot flash severity, and neuropathy. No serious adverse events were reported related to acupuncture intervention. Mild adverse events (i.e., bruising, pain, swelling, skin infection, hematoma, headache, menstrual bleeding) were reported in 11 studies.
The authors concluded that this systematic review and meta-analysis suggest that acupuncture significantly reduces multiple treatment-related symptoms compared with the usual care or waitlist control group among breast cancer survivors. The safety of acupuncture was inadequately reported in the included studies. Based on the available data, acupuncture seems to be generally a safe treatment with some mild adverse events. These findings provide evidence-based recommendations for incorporating acupuncture into clinical breast cancer symptom management. Due to the high risk of bias and blinding issues in some RCTs, more rigorous trials are needed to confirm the efficacy of acupuncture in reducing multiple treatment-related symptoms among breast cancer survivors.
Yes, I agree: this is an uncritical white-wash of the evidence. So, why do I bother to discuss this paper? After all, the acupuncture literature is littered with such nonsense.
Well, to my surprise, the results did contain a little gem after all.
A subgroup analysis of the data indicated that acupuncture showed no significant effects on any of the treatment-related symptoms compared with the sham acupuncture groups.
In other words, this paper confirms what has been discussed repeatedly on this blog (see for instance here, here, and here):
Acupuncture seems to be a placebo therapy!
Acupuncture is usually promoted as a safe therapy. This may be good marketing but, sadly, it is not the truth. About 10% of all patients experience mild to moderate adverse effects such as pain or bleeding. In addition, there are well-documented complications, for instance:
However, there have been few reports of deaths due to pneumothorax after acupuncture treatment, especially focused on electroacupuncture.
Japanese authors recently reported an autopsy case of a man in his 60s who went into cardiopulmonary arrest and died immediately after receiving electroacupuncture. Postmortem computed tomography (PMCT) showed bilateral pneumothoraces, as well as the presence of numerous gold threads embedded subcutaneously. An autopsy revealed two ecchymoses in the right thoracic cavity and a pinhole injury on the lower lobe of the right lung, suggesting that the needles had penetrated the lung. There were marked emphysematous changes in the lung, suggesting that rupture of bullae might also have contributed to bilateral pneumothoraces and fatal outcomes. The acupuncture needles may have been drawn deeper into the body than at the time of insertion due to electrical pulses and muscle contraction, indicating the need for careful determination of treatment indications and technical safety measures, such as fail-safe mechanisms.
This is the first case report of fatal bilateral pneumothoraces after electroacupuncture reported in the English literature. This case sheds light on the safety of electroacupuncture and the need for special care when administering it to patients with pulmonary disease who may be at a higher risk of pneumothorax. This is also the first report of three-dimensional reconstructed PMCT images showing the whole-body distribution of embedded gold acupuncture threads, which is unusual.
One-sided pneumothoraxes are common events after acupuncture. Several hundred cases have been published and the vast majority of such incidents remain unpublished or even unnoticed. These events are not normally life-threatening. If ‘only’ one lung is punctured, the patient may experience breathing difficulties, but in many cases these are temporary and the patient soon recovers.
Yet a bilateral pneumothorax is an entirely different affair. If both lungs malfunction, the patient’s chances of survival are slim unless he/she is close to an intensive care unit.
You might think that it needs an especially ungifted acupuncturist to manage to puncture both lungs simultaneously. I might agree, but we need to consider that acupuncture needles are often inserted in a symmetrical fashion into the patient’s body. This means that, if the therapist puts a needle at one point of the thorax that is close to a lung, he is not unlikely to do the same on the other side.
And how does one prevent such disasters?
Easy:
- train acupuncturists properly,
- avoid needles on the upper thorax,
- or refuse acupuncture altogether.
This study aimed to assess the feasibility of a future definitive trial, with a preliminary assessment of differences between effects of individualized homeopathic (IH) medicines and placebos in the treatment of cutaneous warts.
A double-blind, randomized, placebo-controlled trial (n = 60) was conducted at the dermatology outpatient department of the Homoeopathic Medical College and Hospital, West Bengal. Patients were randomized to receive either IH (n = 30) or identical-looking placebos (n = 30). The primary outcome measures were numbers and sizes of warts; the secondary outcome measure was the Dermatology Life Quality Index (DLQI) questionnaire measured at baseline, and every month up to 3 months. Group differences and effect sizes were calculated on the intention-to-treat sample.
Attrition rate was 11.6% (IH, 3; placebo, 4). Intra-group changes were significantly greater in the IH group than in the placebo group. Inter-group differences were statistically non-significant (all p > 0.05, Mann-Whitney U tests) with small effect sizes, both in the primary outcomes (number of warts after 3 months: IH median [interquartile range; IQR] 1 [1, 3] vs. placebo 1 [1, 2]; p = 0.741; size of warts after 3 months: IH 5.6 mm [2.6, 40.2] vs. placebo 6.3 [0.8, 16.7]; p = 0.515) and in the secondary outcomes (DLQI total after 3 months: IH 4.5 [2, 6.2] vs. placebo 4.5 [2.5, 8]; p = 0.935). Thuja occidentalis (28.3%), Natrum muriaticum (10%), and Sulphur (8.3%) were the most frequently prescribed medicines. No homeopathic aggravations or serious adverse events were reported.
The authors concluded that, as regards efficacy, the preliminary study was inconclusive, with a statistically non-significant direction of effect favoring homeopathy. The trial succeeded in showing that an adequately powered definitive trial is both feasible and warranted.
Partly the same group of authors recently published another trial of homeopathy with similar findings. At the time, I commented as follows:
We have come across this terminology before; homeopaths seem to like it. It prevents them from calling a negative trial by its proper name: A NEGATIVE TRIAL. In their view
- a positive trial is a study where homeopathy yields better results than placebo,
- a negative trial is a study where placebo yields better results than homeopathy,
- an inconclusive trial is a study where homeopathy yields results that are not significantly different from placebo.
Is this silly?
Yes, it is completely bonkers!
Is it dishonest?
Yes, in my view, it is.
Why is it done nonetheless?
Perhaps a glance at the affiliations of the authors provides an answer. And here is the list of the affiliations of the trialists of the present cutaneous wart study:
- 1Department of Repertory, D.N. De Homoeopathic Medical College and Hospital, Govt. of West Bengal, Tangra, Kolkata, West Bengal, India.
- 2D.N. De Homoeopathic Medical College and Hospital, Govt. of West Bengal, Tangra, Kolkata, West Bengal, India.
- 3Department of Organon of Medicine and Homoeopathic Philosophy, The Calcutta Homoeopathic Medical College and Hospital, Kolkata, West Bengal, India.
- 4Department of Practice of Medicine, The Calcutta Homoeopathic Medical College and Hospital, Kolkata, West Bengal, India.
- 5Department of Repertory, National Institute of Homoeopathy, Ministry of AYUSH, Govt. of India, Kolkata, West Bengal, India.
- 6Department of Organon of Medicine and Homoeopathic Philosophy, D.N. De Homoeopathic Medical College and Hospital, Govt. of West Bengal, Tangra, Kolkata, West Bengal, India.
- 7Department of Pediatrics, National Institute of Homoeopathy, Ministry of AYUSH, Govt. of India, Salt Lake, Kolkata, West Bengal, India.
- 8Department of Organon of Medicine and Homoeopathic Philosophy, State National Homoeopathic Medical College and Hospital, Lucknow, Uttar Pradesh.
- 9Independent Researcher; Champsara, Baidyabati, Hooghly, West Bengal, India.
- 10Independent Researcher, Shibpur, Howrah, West Bengal, India.
And, as before, this paper also contains this statement:
Conflict of interest statement
None declared.
Pre-hypertension, or stage 1 hypertension as it is also called, is usually defined as a systolic pressure reading between 120 mmHg and 139 mmHg, or a diastolic reading between 80 mmHg and 89 mmHg. It remains a significant public health challenge and appropriate intervention is required to stop its progression to hypertension and cardiovascular diseases.
This double-blind, randomized, two parallel arms, placebo-controlled study tested the effects of individualized homeopathic medicines (IH) against placebo in intervening with the progression of pre-hypertension to hypertension.
Ninety-two patients with pre-hypertension were randomized to receive either IH (n = 46) or identical-looking placebo (n = 46). Both IH or placebo were applied in the mutual context of lifestyle modification (LSM) advice including dietary approaches to stop hypertension (DASH) and brisk exercises.
The primary endpoints were systolic and diastolic blood pressures (SBP and DBP); secondary endpoints were Measure Yourself Medical Outcome Profile version 2.0 (MYMOP-2) scores. All endpoints were measured at baseline, and every month, up to 3 months.
After 3 months of intervention, the number of patients having progression from pre-hypertension to hypertension between groups was similar without any significant differences in between the groups. Reduction in BP and MYMOP-2 scores were also not significantly different. Lycopodium clavatum, Thuja occidentalis and Natrum muriaticum were the most frequently prescribed medicines. No serious adverse events were reported from either group.
The authors concluded that there was a small, but non-significant direction of effect favoring homeopathy, which ultimately rendered the trial as inconclusive.
We have come across this terminology before; homeopaths seem to like it. It prevents them from calling a negative trial by its proper name: A NEGATIVE TRIAL. In their view
- a positive trial is a study where homeopathy yields better results than placebo,
- a negative trial is a study where placebo yields better results than homeopathy,
- an inconclusive trial is a study where homeopathy yields results that are not significantly different from placebo.
Is this silly?
Yes, it is completely bonkers!
Is it dishonest?
Yes, in my view, it is.
Why is it done nonetheless?
Perhaps a glance at the affiliations of the authors provides an answer:
- 1Dept. of Organon of Medicine and Homoeopathic Philosophy, D. N. De Homoeopathic Medical College and Hospital, Kolkata, West Bengal, affiliated to The West Bengal University of Health Sciences, Govt. of West Bengal, India. Electronic address: [email protected].
- 2Dept. of Organon of Medicine and Homoeopathic Philosophy, D. N. De Homoeopathic Medical College and Hospital, Kolkata, West Bengal, affiliated to The West Bengal University of Health Sciences, Govt. of West Bengal, India.
- 3Principal and Administrator D. N. De Homoeopathic Medical College and Hospital, Kolkata, West Bengal, affiliated to The West Bengal University of Health Sciences, Govt. of West Bengal, India.
- 4Dept. of Practice of Medicine, D. N. De Homoeopathic Medical College and Hospital, Kolkata, West Bengal, affiliated to The West Bengal University of Health Sciences, Govt. of West Bengal, India.
- 5Dept. of Practice of Medicine, Mahesh Bhattacharyya Homoeopathic Medical College and Hospital, Howrah, Govt. of West Bengal, affiliated to The West Bengal University of Health Sciences, Govt. of West Bengal, India.
- 6Dept. of Organon of Medicine and Homoeopathic Philosophy, National Institute of Homoeopathy, Block GE, Sector III, Salt Lake, Kolkata 700106, West Bengal, India; affiliated to The West Bengal University of Health Sciences, Govt. of West Bengal, India.
- 7Dept. of Organon of Medicine and Homoeopathic Philosophy, State National Homoeopathic Medical College and Hospital, Lucknow, Govt. of Uttar Pradesh, affiliated to Dr. Bhimrao Ramji Ambedkar University, Agra, Govt. of Uttar Pradesh), India.
- 8Dept. of Repertory, D. N. De Homoeopathic Medical College and Hospital, Kolkata, West Bengal, affiliated to The West Bengal University of Health Sciences, Govt. of West Bengal, India.
Despite these multiple conflicts of interest, the article carries this note:
“Declaration of Competing Interest: None declared.”
In their 2019 systematic review of spinal manipulative therapy (SMT) for chronic back pain, Rubinstein et al included 7 studies comparing the effect of SMT with sham SMT.
They defined SMT as any hands-on treatment of the spine, including both mobilization and manipulation. Mobilizations use low-grade velocity, small or large amplitude passive movement techniques within the patient’s range of motion and control. Manipulation uses a high-velocity impulse or thrust applied to a synovial joint over a short amplitude near or at the end of the passive or physiological range of motion. Even though there is overlap, it seems fair to say that mobilization is the domain of osteopaths, while manipulation is that of chiropractors.
The researchers found:
- low-quality evidence suggesting that SMT does not result in a statistically better effect than sham SMT at one month,
- very low-quality evidence suggesting that SMT does not result in a statistically better effect than sham SMT at six and 12 months.
- low-quality evidence suggesting that, in terms of function, SMT results in a moderate to strong statistically significant and clinically better effect than sham SMT at one month. Exclusion of an extreme outlier accounted for a large percentage of the statistical heterogeneity for this outcome at this time interval (SMD −0.27, 95% confidence interval −0.52 to −0.02; participants=698; studies=7; I2=39%), resulting in a small, clinically better effect in favor of SMT.
- very low-quality evidence suggesting that, in terms of function, SMT does not result in a statistically significant better effect than sham SMT at six and 12 months.
This means that SMT has effects that are very similar to placebo (the uncertain effects on function could be interpreted as the result of residual de-blinding due to a lack of an optimal placebo or sham intervention). In turn, this means that the effects patients experience are largely or completely due to a placebo response and that SMT has no or only a negligibly small specific effect on back pain. Considering the facts that SMT is by no means risk-free and that less risky treatments exist, the inescapable conclusion is that SMT cannot be recommended as a treatment of chronic back pain.
Guest post by Norbert Aust and Viktor Weisshäupl
Imagine you recently published an excellent and rigorous trial providing solid evidence that a certain therapy is able to help patients suffering from some inevitably fatal condition. You proved that your therapy is able to significantly prolong the patients’ lifetime, much longer than with the current state-of-the-art therapeutic approach. But the patients not only live considerably longer, but they also do so with a much better quality of life (QoL) and subjective well-being. In short: this therapy marks some progress that would otherwise take years or decades of scientific effort.
And then someone comes forward and points out your data apparently were manipulated. Essential parameters of this trial were modified sometime after data collection was completed, with the patients’ outcome and first analyses available. Thus the results were biased in a certain direction and the critics show that the results as published in your study show characteristics that such manipulations would evoke. After all, this holds an implication of scientific misconduct that could, if verified, ruin your academic reputation more or less completely.
What would you do?
Ignore the preposterous concerns because you know your methods and performance were rigorous and solid? After all, anytime some real academic criticism arises you are ready to prove your findings are well-founded results of accepted scientific methods. Or would you publish data or documents that your critics were too ignorant to find or to understand, and thus to stop such rumours once and for all? Maybe you could even clarify some of the issues raised by those critics, maybe add some follow-up information or data to ensure no more misunderstandings occur. Or would you try to find some clues for a libel lawsuit?
Well, we thought some of the above would happen after we contacted the authors of the recent study on adjunct homeopathy in non-small cell lung cancer. On that date, we forwarded our detailed analysis to the lead author and all the co-authors.
Of course, we even considered the possibility, not very likely though, that we would receive some explanation for the numerous exclusion criteria while other serious conditions that coincide with advanced age did not preclude enrollment. Or an updated CONSORT diagram accounting for the patients excluded. Or some explanation just why the numerous amendments to the protocol were necessary but not important enough to mention them in the published paper.
But nothing of this happened as yet (July 2021). Instead on June 14 and 16, 2021, not two weeks after our messages to the authors, the registration data at ClinicalTrials were updated once again and a new version of the protocol was uploaded [3]. And this update looks pretty much like it is meant to cover up and blur the former data that we based our analysis on. Of course, these data and the former version of the protocol are available still – just one layer further down, and you have to scroll to the bottom of the page to find the small link “history of changes”. Maybe not many visitors will do that.
In contrast to the versions before, now the uploaded data are in line with the study as published, namely, they include a full list of the exclusion criteria and the reduced observation time for QoL, which was the primary outcome. Note: throughout the trial until the end of data assessment those parameters were set with pregnancy as the only exclusion criterion and two years follow up time, only to be amended in the protocol uploaded two months after data collection was complete and analysis presumably was well underway.
In addition, there is a new version of the study protocol, this one dated Feb. 6, 2014. Of course, this protocol is fairly new, in spite of the date it carries. Why would the older version allegedly from January 2011 be uploaded to the register in September 2019, if this more actual version already had existed and was available?
Contrary to the prior version all the clues are removed that would indicate that this document was finished at a much later point in time than given in its date: References to some future software versions that were released years after the protocol was allegedly compiled are dropped. And this strange literature reference “25” that corresponds to the reference list in the final study as published but is pointless in the protocol without any reference list, is removed too. And of course, again contrary to the prior version, the exclusion criteria are identical with the final study as is the shortened follow-up time for QoL.
New to the protocol is a section “Bringing in the patient’s voice”, where the authors disclose how they want to “systematically research the ethical, legal, socio-political, and science theoretical dimensions of homeopathy as in the case of lung cancer (non-small-cell lung carcinoma) exemplified” in some “integral social scientific study”, where some “focus groups” of 4 to 10 participants together with their relatives, friends and caregivers included should be used to study “interactions between individuals, collectively shared and uncontested assumptions, and the emergence of collective meaning”.
But from all of this more or less meaningless but very sciency sounding socio-speak, not a single word found its way into the study. Nothing. So it is pointless to try to figure out what the content of this part of the investigation is all about.
Why then was this chapter added? This “integral social scientific study” was to start after the “third or fourth homeopathic treatment” (But why should patients not be included in this “research” from the very first beginning?). Is it perhaps to give some rationale why the follow-up time for QoL was to end after the third homeopathic treatment?
So what we see, when we look up the study at ClinicalTrials now, is a perfectly matching set of data and a protocol that corresponds to the study as published and looks as if it was published at a time where the trial was underway and the patients were still blinded. If you do not look very closely everything now appears to be perfect.
And here we would like to forward some critique to the register: The purpose of the study register is to prevent not only publication bias but misleading manipulation from happening as well. They do quite a good job in preserving former versions of data and documents and keeping them available to the public. Many national study registers do not offer this service. But you must be of a suspicious mind and of some persistence to actively search and find and check the history of modifications. Thus, a cover-up like the one we are witnessing here might well prove successful. We, therefore, propose to improve the presentation of the registration: If vital amendments occurred that may affect the outcomes – such as protocol changes, extensions of exclusion criteria, modifications of follow-up time – this should be indicated upfront in the study’s record instead of some small hint to “history of changes” at the very bottom of the page.
In conclusion, there appears to be no proof that the results of the study were produced using rigorous scientific methods. And the issues we raised in our report to the authors remain unresolved.
This multicenter, randomized, sham-controlled trial was aimed at assessing the long-term efficacy of acupuncture for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS). Men with moderate to severe CP/CPPS were recruited, regardless of prior exposure to acupuncture. They received sessions of acupuncture or sham acupuncture over 8 weeks, with a 24-week follow-up after treatment. Real acupuncture treatment was used to create the typical de qi sensation, whereas the sham acupuncture treatment (the authors state they used the Streitberger needle, but the drawing looks more as though they used our device) does not generate this feeling.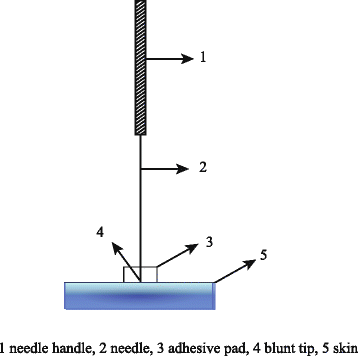
The primary outcome was the proportion of responders, defined as participants who achieved a clinically important reduction of at least 6 points from baseline on the National Institutes of Health Chronic Prostatitis Symptom Index at weeks 8 and 32. Ascertainment of sustained efficacy required the between-group difference to be statistically significant at both time points.
A total of 440 men (220 in each group) were recruited. At week 8, the proportions of responders were:
- 60.6% (95% CI, 53.7% to 67.1%) in the acupuncture group
- 36.8% (CI, 30.4% to 43.7%) in the sham acupuncture group (adjusted difference, 21.6 percentage points [CI, 12.8 to 30.4 percentage points]; adjusted odds ratio, 2.6 [CI, 1.8 to 4.0]; P < 0.001).
At week 32, the proportions were:
- 61.5% (CI, 54.5% to 68.1%) in the acupuncture group
- 38.3% (CI, 31.7% to 45.4%) in the sham acupuncture group (adjusted difference, 21.1 percentage points [CI, 12.2 to 30.1 percentage points]; adjusted odds ratio, 2.6 [CI, 1.7 to 3.9]; P < 0.001).
Twenty (9.1%) and 14 (6.4%) adverse events were reported in the acupuncture and sham acupuncture groups, respectively. No serious adverse events were reported. No significant difference was found in changes in the International Index of Erectile Function 5 score at all assessment time points or in peak and average urinary flow rates at week 8.
The authors concluded that, compared with sham therapy, 20 sessions of acupuncture over 8 weeks resulted in greater improvement in symptoms of moderate to severe CP/CPPS, with durable effects 24 weeks after treatment.
The study was sponsored by the China Academy of Chinese Medical Sciences and the National Administration of Traditional Chinese Medicine. The trialists originate from the following institutions:
- 1Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, China (Y.S., B.L., Z.Q., J.Z., J.W., X.L., W.W., R.P., H.C., X.W., Z.L.).
- 2Key Laboratory of Chinese Internal Medicine of Ministry of Education, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China (Y.L.).
- 3ThedaCare Regional Medical Center – Appleton, Appleton, Wisconsin (K.Z.).
- 4Hengyang Hospital Affiliated to Hunan University of Chinese Medicine, Hengyang, China (Z.Y.).
- 5The First Hospital of Hunan University of Chinese Medicine, Changsha, China (W.Z.).
- 6Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou, China (W.F.).
- 7The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, China (J.Y.).
- 8West China Hospital of Sichuan University, Chengdu, China (N.L.).
- 9China Academy of Chinese Medical Sciences, Beijing, China (L.H.).
- 10Yantai Hospital of Traditional Chinese Medicine, Yantai, China (Z.Z.).
- 11Shaanxi Provincial Hospital of Traditional Chinese Medicine, Xi’an, China (T.S.).
- 12The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, China (J.F.).
- 13Beijing Fengtai Hospital of Integrated Traditional and Western Medicine, Beijing, China (Y.D.).
- 14Xi’an TCM Brain Disease Hospital, Xi’an, China (H.S.).
- 15Dongfang Hospital Beijing University of Chinese Medicine, Beijing, China (H.H.).
- 16Luohu District Hospital of Traditional Chinese Medicine, Shenzhen, China (H.Z.).
- 17Guizhou University of Traditional Chinese Medicine, Guiyang, China (Q.M.).
These facts, together with the previously discussed notion that clinical trials from China are notoriously unreliable, do not inspire confidence. Moreover, one might well wonder about the authors’ claim that patients were blinded. As pointed out above, the real and sham acupuncture were fundamentally different: the former did generate de qi, while the latter did not! A slightly pedantic point is my suspicion that the trial did not test the efficacy but the effectiveness of acupuncture, if I am not mistaken. Finally, one might wonder what the rationale of acupuncture as a treatment of CP/CPPS might be. As far as I can see, there is no plausible mechanism (other than placebo) to explain the effects.
So, is the evidence that emerged from the new study convincing?
No, in my view, it is not!
In fact, I am surprised that a journal as reputable as the Annals of Internal Medicine published it.
A case report was published of a 35-year-old Chinese man with no risk factors for stroke. He presented with a 2-day history of expressive dysphasia and a 1-day history of right-sided weakness. The symptoms were preceded by multiple sessions of the neck, shoulder girdle, and upper back massage for pain relief in the prior 2 weeks. A CT-scan of the brain demonstrated an acute left middle cerebral artery infarct and left internal carotid artery dissection. The MRI cerebral angiogram confirmed left carotid arterial dissection and intimal oedema of bilateral vertebral arteries. In the absence of other vascular comorbidities and risk factors, massage-induced internal carotid arterial dissection was deemed to be the most likely cause of the near-fatal cerebrovascular event.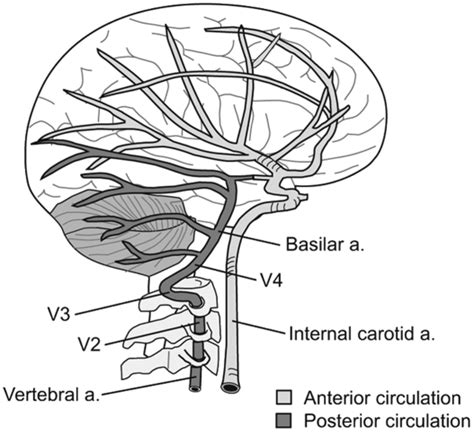
INSIDER reported further details of the case: the patient told the doctors who treated him that he had seen the chiropractor for two weeks before he experienced trouble reading, writing and talking. After experiencing those symptoms for two days and one day of pain on his right side, a friend convinced the patient to consult a neurologist. This led to the hospital admission, the above-named tests, and diagnosis. After three months of therapy and rehab, the patient showed “significant improvement,” according to the doctors.
What remains unclear is the exact nature of the neck treatment that is believed to have caused the arterial dissection. A massage is mentioned but massages have rarely been associated with such problems. Neck manipulations, on the other hand, are the hallmark therapy of chiropractors and have, as I have pointed out regularly, often been reported to cause arterial dissections.
Chiropractors usually deny this fact; alternatively, they claim that only poorly trained practitioners cause these adverse events or that their frequency is exceedingly small. However, without a proper post-marketing surveillance system, this argument is hardly convincing.
I was alerted the these Chiropractic Paediatric Courses. After studying the material, I was truly stunned. Now that I have recovered, I feel I should share it with you:
Chiropaeds Australia is an approved and accredited provider of the Diplomate of Australian College of Chiropractic Paediatrics program.
Diplomate of Australian College of Chiropractic Paediatrics Offered for the first time in 2013, the Diplomate program is a two-year chiropractic paediatric course. This course is ideal for the family chiropractor wanting to improve his or her knowledge in chiropractic paediatrics. The emphasis is on conditions and management issues which are commonly seen by the family chiropractor.
The course is structured around 20 four-week modules over two years. Each module consists of required reading, exercises and at the end of each four-week module there is a six-hour seminar. Each six-hour seminar will reinforce the reading and develop the practical and management skills needed to feel confident in providing optimal chiropractic care for children…
Registration post 31 December – $AUD 6050 (includes GST) This covers the cost of all materials and seminars but does not include any books or texts you may decide to purchase.
To provide you with an impression of the content of the modules, I have chosen three of them. Here they are:

Module 7
Neurological assessment of the infant
1. Neurological examination of the infant (Infanib)
2. Motor issues: diagnosis and chiropractic management
a. Gross motor developmental delay
b. Hyper/ hypotonia
c. Cerebral palsy
It is only by knowing how to assess the infant’s neurological system that you can start to fully appreciate and understand the immense impact of the subluxation. The information covered in this module allows you to demonstrate to your parents the impact the subluxation has on their infant’s nervous system. As a result your subluxation diagnosis, treatment and management with infants will be enhanced. We look at muscle function issues which occur in this age group with particular emphasis on gross motor developmental delay and hyper/hypotonia.
Module 8
Neurological assessment of the pre-schooler and the school aged child
1. Gross motor function
2. Fine motor function
3. Cerebellar function
4. Assessment of higher cognitive functions
5. Visual processing
6. Auditory processing
7. Language development
Syndrome management
1. Auditory processing syndromes
2. Visual processing syndromes
Chiropractic has a major role to play in treating and managing children with learning difficulties. Crucial to optimal outcomes is an ability to fully assess and determine the particular issues and neurological problems your patient experiences. This module is very practical: you will learn how to accurately test cortical and cerebellar function in preschool and school aged children to a very advanced level. Being able to perform extensive testing of learning ability in children will assist you to accurately find and monitor their learning difficulties. The interplay of higher cortical function, cerebellar function and the subluxation is explored and the impact of your consultation assessment routine on the subluxation is addressed. Management of learning difficulties is emphasised.
Module 11
The child’s ear, nose and throat
1. Acute otitis media
2. Chronic otitis media
3. Serous otitis media
4. Nose and throat issues with children
5. Tonsillitis, epiglottitis, coup and neck abscesses
Chiropractors have a key role to play in the treatment and management of otitis media along with other conditions associated with recurrent viral infection as well as decreased or imbalanced immune system function. We cover the diagnosis of each condition along with chiropractic treatment and management, including the interaction of the subluxation and the immune system. Nutritional management is also covered. Key management issues are explored and literature based knowledge is provided to allow you to educate you patient’s parents. This fosters improved compliance with your care and permits you to expand the boundaries of your chiropractic care of children.
____________________________________
I wonder whether some chiropractor feels like defending this outright charlatanry.
I know of no evidence to assume that chiropractors can provide effective care for children. I see, however, many reasons to fear that they may cause considerable harm. I also see no reason to take a profession seriously that tolerates or even supports such extreme quackery.
I have expressed these concerns often enough, e.g.:
- The effectiveness of chiropractic spinal manipulations/mobilisation for children is unproven. TIME TO STOP TREATING KIDS!
- Chiropractic for kids: a ‘complete disregard for the evidence and scientific facts’
- Chiropractic for kids: a pack of offensive lies
- Chiropractic spinal care for children is dangerous, unwarranted and must cease immediately
- Don’t let a chiropractor near your kids!
- Chiro for kids? No!
In my view, it is high time to stop this dangerous nonsense.