risk
A case report was published of a 35-year-old Chinese man with no risk factors for stroke. He presented with a 2-day history of expressive dysphasia and a 1-day history of right-sided weakness. The symptoms were preceded by multiple sessions of the neck, shoulder girdle, and upper back massage for pain relief in the prior 2 weeks. A CT-scan of the brain demonstrated an acute left middle cerebral artery infarct and left internal carotid artery dissection. The MRI cerebral angiogram confirmed left carotid arterial dissection and intimal oedema of bilateral vertebral arteries. In the absence of other vascular comorbidities and risk factors, massage-induced internal carotid arterial dissection was deemed to be the most likely cause of the near-fatal cerebrovascular event.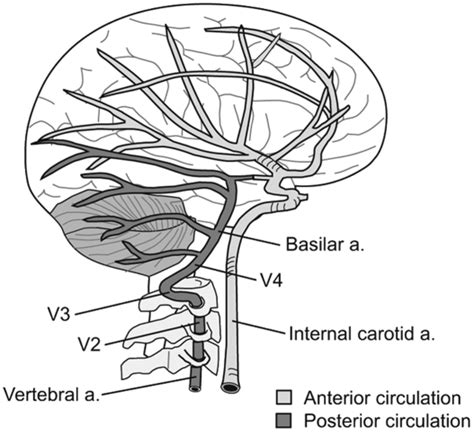
INSIDER reported further details of the case: the patient told the doctors who treated him that he had seen the chiropractor for two weeks before he experienced trouble reading, writing and talking. After experiencing those symptoms for two days and one day of pain on his right side, a friend convinced the patient to consult a neurologist. This led to the hospital admission, the above-named tests, and diagnosis. After three months of therapy and rehab, the patient showed “significant improvement,” according to the doctors.
What remains unclear is the exact nature of the neck treatment that is believed to have caused the arterial dissection. A massage is mentioned but massages have rarely been associated with such problems. Neck manipulations, on the other hand, are the hallmark therapy of chiropractors and have, as I have pointed out regularly, often been reported to cause arterial dissections.
Chiropractors usually deny this fact; alternatively, they claim that only poorly trained practitioners cause these adverse events or that their frequency is exceedingly small. However, without a proper post-marketing surveillance system, this argument is hardly convincing.
 So-called alternative medicine (SCAM) for cancer is the title of my new book. I was informed that it has been published but, in reality, the hard copy might still take a few days until it is available (there were major problems at the proof-reading stage which caused a considerable delay). To give you a flavor of the book, allow me to show you my introduction; here it is:
So-called alternative medicine (SCAM) for cancer is the title of my new book. I was informed that it has been published but, in reality, the hard copy might still take a few days until it is available (there were major problems at the proof-reading stage which caused a considerable delay). To give you a flavor of the book, allow me to show you my introduction; here it is:
In February 2013, my wife and I were in good spirits. I had recently retired from my post at Exeter University, and we were heading off to celebrate Danielle’s round birthday with her family in Brittany. There was just one thing that bothered us: Danielle had recurring abdominal pains. She had seen our GP in England several times about it. The last time, she had received a prescription for some antibiotics. I knew they would not help; her symptoms were not due to an infection.
After our arrival in France, things got worse, and Danielle consulted a gynaecologist at the out-patient clinic of the local hospital. More tests were ordered; an ultrasound showed an abnormality; a subsequent MRI revealed a tumour of the uterus. The gynaecologist advised to operate as soon as possible, and Danielle agreed.
The operation went well, but the gynaecologist, Dr Matthieu Jacquot, was concerned and said he had to be more radical than he had anticipated. The diagnosis was still uncertain until the results from the histology lab were in. A few days later, when we saw Dr Jacquot again, our hopes that all was fine were thoroughly dashed. He explained that Danielle had cancer of the endometrium and laid out the treatment plan which an entire team of oncologists had designed after an in-depth review of her case: a second, much more extensive operation, followed by six sessions of chemotherapy, followed by months of daily radiotherapy, followed by two sessions of brachytherapy.
Dr Jacquot could not have been more empathetic. He explained in detail what consequences all this would have. Danielle’s life would be dominated for the next year by a long series of treatments that were unpleasant to say the least. We were both shocked and close to tears.
Before arriving at a decision, we talked to friends and experts in this area. Opinions differed marginally. Two days later, we had made up her mind: we would stay in Brittany for the entire year and get Danielle treated exactly as Dr Jacquot suggested.
The second operation was much tougher than the first, but Danielle recovered well. Ten days later, she was back in our home and looked after by a nurse who came daily to change the bandages and give injections. On her third visit, the nurse broached the subject of chemotherapy which was scheduled to start soon. She explained how unpleasant it would be and what horrendous side effects Danielle was facing. Then she said: ‘You know, you don’t need to go through all this. They only pump you full with poison. There is a much better approach. Just follow the anti-cancer diet of Dr Schwartz.[1] It is natural and has no side effects. It would surely cure your cancer.’ When Danielle told me about this conversation, I informed the nurse that from now on I would myself take charge of the post-operative care of my wife and that her services were no longer required.
Today, Danielle is cancer-free. Had she listened to the nurse, she would almost certainly no longer be with us. But the lure of a ‘natural’ cancer cure with no side effects is almost irresistible. Faced with a serious diagnosis like cancer, most patients would consider any therapy that promises help without harm. Inevitably, they encounter a myriad of so-called alternative medicines (SCAMs), and many patients give SCAM a try.
In addition to Dr Schwartz’s cancer diet, there are hundreds of SCAMs that specifically target vulnerable cancer patients like Danielle. How can patients not be confused, and who might give them responsible advice? Conventional doctors rarely do. A recent summary of 29 relevant papers concluded that physicians will discuss complementary therapies only when a patient him/herself raises this issue within a consultation.[2] But cancer patients are often too embarrassed to ask about SCAM. Those who are courageous enough usually get short shrift. Many conventional doctors are not just critical about SCAM, but also know very little about the subject.[3]
Patients deserve evidence-based information, instead they often get unhelpful blanket statements from their GPs such as:
- ‘there is no evidence’;
- ‘that’s all rubbish, best to stay well clear of it’;
- ‘if you want to try it, go ahead, it cannot do much harm’.
All of these are untrue. Frustrated by such erroneous platitudes, patients might go on the Internet for help where they are bombarded with uncritical promotion. We investigated the information on SCAM for cancer provided by popular websites and found that they offer information of extremely variable quality. Many endorse unproven therapies and some are outright dangerous.[4] Sadly, the advice patients might glean from newspapers[5] or health-food stores[6] tends to be equally misleading and potentially harmful.
Subsequently, some patients might visit a library and read one of the many books on the subject. If anything, they are even worse. We have repeatedly analysed the contents of consumer guides on SCAM and always concluded that following their recommendations would shorten the life of the reader.[7] To give you a flavour, here are a few titles currently on sale:
- Cancer Medicine from Nature
- Outsmart Your Cancer: Alternative Non-Toxic Treatments That Work
- Cancer Medicine from Nature
- Perfect Guide on How to Cure Breast Cancer Through Curative Approved Alkaline Diets & Herbs
- How to Starve Cancer
- Healing the Prostate: The Best Holistic Methods to Treat the Prostate and Other Common Male-Related Conditions
- Outsmart Cancer: Defeat Cancer With Vitamin B17, Healthy Nutrition and Alternative Medicine
Cancer patients would, of course, all like to ‘outsmart cancer’; they are desperate and vulnerable. In this state of mind, they easily fall victim to anyone who sells false hope at inflated prices. The consequences can be tragic.
In 2016, the actress English Leah Bracknell, for example, raised ~£50 000 to treat her lung cancer in the German ‘Hallwang Private Oncology Clinic’. The SCAMs used there included homeopathy, micronutrients, natural supplements, whole-body hyperthermia, and ozone therapy, none of which cures cancer. If cancer patients fall for bogus treatments, they not just lose their money but also their lives. Leah Bracknell died of her cancer in 2019.[8]
Three basic facts are indisputably clear:
- a high percentage of cancer patients use SCAM,
- misinformation about SCAM is rife,
- misinformation endangers the lives of cancer patients.
It follows that there is an obvious and urgent need for an evidence-based text naming the SCAMs that are potentially harmful and discussing those that might be helpful.
My book is aimed at doing just that.
[1] Dr Laurent Schwartz cancérologue iconoclaste — Guérir du Cancer (guerir-du-cancer.fr)
[2] Stub T, Quandt SA, Arcury TA, et al. Perception of risk and communication among conventional and complementary health care providers involving cancer patients’ use of complementary therapies: a literature review. BMC Complement Altern Med. 2016;16(1):353. Published 2016 Sep 8. doi:10.1186/s12906-016-1326-3
[3] Ziodeen KA, Misra SM. Complementary and integrative medicine attitudes and perceived knowledge in a large pediatric residency program. Complement Ther Med. 2018;37:133-135. doi:10.1016/j.ctim.2018.02.004
[4] Schmidt K, Ernst E. Assessing websites on complementary and alternative medicine for cancer. Ann Oncol. 2004;15(5):733-742. doi:10.1093/annonc/mdh174
[5] Milazzo S, Ernst E. Newspaper coverage of complementary and alternative therapies for cancer–UK 2002-2004. Support Care Cancer. 2006;14(9):885-889. doi:10.1007/s00520-006-0068-z
[6] Mills E, Ernst E, Singh R, Ross C, Wilson K. Health food store recommendations: implications for breast cancer patients. Breast Cancer Res. 2003;5(6):R170-R174. doi:10.1186/bcr636
[7] https://edzardernst.com/2013/09/drowning-in-a-sea-of-misinformation-part-8-books-on-alternative-medicine/
[8] https://edzardernst.com/2019/10/leah-blacknell-1964-2019-another-victim-of-cancer-quackery/
____________________________________________
The publication of this book is perhaps the right occasion to publicly thank two regular and one occasional contributor to this blog. I am grateful to
- Prof. Michael Baum, emeritus professor, for writing the foreword,
- Dr. Julian Money-Kyrle, retired consultant oncologist, for his constructive comments on chapter 1.4,
- Richard Rasker for his corrections and advice on the entire text.
Thank you all.
It has been reported that an Australian naturopath would refuse entry to her business to anyone who has received a COVID-19 vaccine in the past two weeks. In her original Facebook post, Ms. Holland said that vaccinated people would have to wait a minimum of two weeks after vaccination before attending her clinic due to “the shedding of spike proteins” caused by “these experimental treatments”.
Christine Pope, who is on the Australian Traditional Medicine Society (ATMS) board of directors, said she believed the views shared by the Warrnambool naturopath were part of the alternative medicine sector’s “fringe” and didn’t represent the industry. “We’re always very careful to tell our practitioners about posting appropriately and within their scope of practice,” Ms. Pope said. “These sort of comments to me look like they’re outside their scope of practice. We do a lot of training about making sure that you’re posting appropriately within your scope of practice and about things about which you are qualified in. As an association supporting natural medicine practitioners, it’s not really our job to promote or comment on the vaccination program – we’re not public health experts … and this is really outside my scope of practice. But from a public health perspective (vaccination) is the best option we’ve got.”
Sharon Holland, who runs a clinic in Warrnambool, cited on Facebook a number of discredited medical professionals who have become figureheads of the anti-vax and COVID conspiracy movements, including Judy Mikovits, Robert Malone, Peter McCullogh, and J Bart Classen. “Often de-bunked and fact-checked (by whom) can mean silenced,” Ms. Holland wrote. “We still have free speech available to some extent. This is a very emotive and divisive subject so my post was bound to ‘ruffle feathers’.”
The ATMS says its accredited practitioners need to “stay within their scope of practice” and avoid posting about vaccines they haven’t studied. Ms. Pope urged people to lodge a complaint about bogus health claims through the ATMS website or the healthcare complaint commissioner in the appropriate state.
___________________________
This course of events begs several questions. In my view, the most important are:
- Is Sharon Holland an exception, or are many/most naturopaths of her opinion?
- Instructing practitioners about “posting appropriately and within their scope of practice” sounds fine but might miss the point entirely. What really matters are the messages ATMS members orally convey to their patients. Is there any evidence on this issue?
- Surely, the anti-vax sentiments of naturopaths must originate from their education. Is there any evidence as to what they are taught about the subject?
- Is the ATMS going to take action against Ms. Holland and other members who endanger the public with their anti-vax stance?
Former chiropractor Malcolm Hooper, 61, and hyperbaric oxygen therapy provider Oxymed Pty Ltd have been fined following the death of a customer in 2016. They were each convicted of three work safety-related charges, all of failing to ensure a workplace is safe and without risks to health. Hooper was fined $176,750, while the company was fined $550,000. Oxymed was trading as HyperMed at its South Yarra premises in April 2016 when a long-term client with multiple sclerosis and a history of life-threatening seizures came in for treatment. He was later found unconscious in a single-person hyperbaric chamber, taken to hospital, and placed on life support, but died five days later.
The County Court heard that both the company and Hooper had an inadequate system in place for assessing the risks oxygen therapy could pose to clients, and an inadequate system too for developing plans to eliminate or reduce those risks. In her judgment, County Court judge Amanda Fox said HyperMed wasn’t a hospital nor a medical practice and had been described as an “alternative health facility”. Hooper had already been deregistered in 2013 by the national board for chiropractors for misleading and deceptive advertising about the benefits of hyperbaric treatment.
Hyperbaric oxygen therapy involves administering pure oxygen in a pressurised environment, with the heightened air pressure allowing a patients’ lungs to gather much more oxygen than would be possible under normal conditions. The therapy is not based on strong data. A systematic review failed to find good evidence for hyperbaric oxygen therapy as a treatment of multiple sclerosis:
Multiple sclerosis (MS) is a chronic, inflammatory, and degenerative neurological illness with no cure. It has been suggested that Hyperbaric Oxygen Therapy (HBO(2)T) may slow or reverse the progress of the disease. This article summarizes the clinical evidence for the use of HBO(2)T in the treatment of MS. We conducted a literature review focused on the interaction of hyperbaric oxygenation and MS. In particular, we appraised the clinical data regarding treatment and performed a meta-analysis of the randomized evidence using the methodology of the Cochrane Collaboration. We found 12 randomized studies in the area, all of which were performed between 1983 and 1987. A meta-analysis of this evidence suggests there is no clinically significant benefit from the administration of HBO(2)T. The great majority of randomized trials investigated a course of 20 treatments at pressures between 1.75ATA and 2.5ATA daily for 60-120 min over 4 weeks against a placebo regimen. None have tested the efficacy of HBO(2)T against alternative current best practice. No plausible benefit of HBO(2)T on the clinical course of MS was identified in this review. It remains possible that HBO(2)T is effective in a subgroup of individuals not clearly identified in the trials to date, but any benefit is unlikely to be of great clinical significance. There is some case for further human trials in selected subgroups and for prolonged courses of HBO(2)T at modest pressures, but the case is not strong. At this time, the routine treatment of MS with HBO(2)T is not recommended.
The case reminds me of that of John Lawler. Mr. Lawlwer’s chiropractor also used a therapy that was not indicated, broke his neck (to put it crudely), and subsequently proved herself more than inept in saving his life. It suggests to me that some chiros may not be trained adequately to deal with emergencies. If that is true, they should perhaps focus less on practice-building courses and more on first aid instructions.
This retrospective electronic medical record data analysis compared the characteristics and outcomes of drug-induced liver injury (DILI) caused by paracetamol and non-paracetamol medications, particularly herbal and dietary supplements. Adults admitted with DILI to the Gastroenterology and Liver Centre at the Royal Prince Alfred Hospital, Sydney (a quaternary referral liver transplantation centre), 2009-2020 were included. The 90-day transplant-free survival and the drugs implicated as causal agents in DILI were extracted from the records.
A total of 115 patients with paracetamol-related DILI and 69 with non-paracetamol DILI were admitted to our centre. The most frequently implicated non-paracetamol medications were:
- antibiotics (19, 28%),
- herbal and dietary supplements (15, 22%),
- anti-tuberculosis medications (6, 9%),
- anti-cancer medications (5, 7%).
The number of non-paracetamol DILI admissions was similar across the study period, but the proportion linked with herbal and dietary supplements increased from 2 of 11 (15%) during 2009-11 to 10 of 19 (47%) during 2018-20 (linear trend: P = 0.011). Despite higher median baseline model for end-stage liver disease (MELD) scores, 90-day transplant-free survival for patients with paracetamol-related DILI was higher than for patients with non-paracetamol DILI (86%; 95% CI, 79-93% v 71%; 95% CI, 60-82%) and herbal and dietary supplement-related cases (59%; 95% CI, 34-85%). MELD score was an independent predictor of poorer 90-day transplant-free survival in both paracetamol-related (per point increase: adjusted hazard ratio [aHR], 1.19; 95% CI, 1.09-3.74) and non-paracetamol DILI (aHR, 1.24; 95% CI, 1.14-1.36).
The authors concluded that, in our single centre study, the proportion of cases of people hospitalised with DILI linked with herbal and dietary supplements has increased since 2009. Ninety-day transplant-free survival for patients with non-paracetamol DILI, especially those with supplement-related DILI, is poorer than for those with paracetamol-related DILI.
A co-author of the paper, specialist transplant hepatologist Dr Ken Liu, was quoted in the Guardian saying he felt compelled to conduct the study because he was noticing more patients with liver injuries from drugs not typically associated with liver harm. “I was starting to see injury in patients admitted with liver injury after using bodybuilding supplements for males or weight loss supplements in females,” he said. “I just decided I better do a study on it to see if my hunch that more of these substances were causing these injuries was true.”
Liu and his colleagues said there needed to be more rigorous regulatory oversight for supplements and other alternative and natural therapies. They also noticed almost half the patients with supplement-induced severe liver injury had non-European ethnic backgrounds. Liu said more culturally appropriate community education about the risks of supplements was needed.
Dr Ken Harvey, public health physician and president of Friends of Science in Medicine, said it was important to note that Liu’s study only examined the most severe cases of supplement-induced liver harm and that the actual rate of harm was likely much higher. “The study only examines severe cases admitted to a specialised liver unit; they cannot be extrapolated to the overall incidence of complementary medicine associated liver injury in Australia,” Harvey said.
The Royal Australian College of General Practitioners, Choice, Friends of Science in Medicine and others have called for an educational statement on the pack and promotional material of medicines making traditional claims, for example saying “This product is based on traditional beliefs and not modern scientific evidence”.
“This was opposed by industry and the TGA,” Harvey said. “But is still needed.”
Pelargonium sidoides, a traditional medicinal plant native to South Africa, is one of the ornamental geraniums that is thought to be effective in treating URTIs. The plant seems to contain a large variety of phytochemicals, including amino acids, phenolic acids, α-hydroxy-acids, vitamins, polyphenols, flavonoids, coumarins, coumarins glucosides, coumarin sulphates and nucleotides. It is mostly used to treat the symptoms of acute bronchitis, common cold and acute rhinosinusitis.
The present study aimed to assess the effectiveness of the liquid herbal drug preparation from the root extracts of Pelargonium sidoides in improving symptoms of uncomplicated upper respiratory tract infections (URTIs). One hundred sixty-four patients with URTI were randomized and given either verum containing the root extracts of Pelargonium sidoides (n = 82) or a matching placebo (n = 82) in a single-blind manner for 7 days. The median total scores of all symptoms (TSS) showed a significant decreasing trend in the group treated with the root extracts derived from Pelargonium sidoides compared to the placebo group from day 0 to day 7 (TSS significantly decreased by 0.85 points in the root extract group compared to a decrease of 0.62 points, p = 0.018). “Cough frequency” showed a significant improvement from day 0 to day 3 (p = 0.023). There was also detected a significant recovery in “sneezing” on day 3 via Brunner-Langer model, and it was detected that the extract administration given in the first 24 h onset of the symptoms had provided a significant improvement in day 0 to day 3 (difference of TSS 0.18 point, p = 0.011).
The authors concluded that Pelargonium sidoides extracts are effective in relieving the symptom burden in the duration of the disease. It may be regarded as an alternative option for the management of URTIs.
These findings are less surprising than they may seem. Already in 2008, we published the following systematic review:
Objective: To critically assess the efficacy of Pelargonium sidoides for treating acute bronchitis.
Data sources: Systematic literature searches were performed in 5 electronic databases: (Medline (1950 – July 2007), Amed (1985 – July 2007), Embase (1974 – July 2007), CINAHL (1982 – July 2007), and The Cochrane Library (Issue 3, 2007) without language restrictions. Reference lists of retrieved articles were searched, and manufacturers contacted for published and unpublished materials.
Review methods: Study selection was done according to predefined criteria. All randomized clinical trials (RCTs) testing P. sidoides extracts (mono preparations) against placebo or standard treatment in patients with acute bronchitis and assessing clinically relevant outcomes were included. Two reviewers independently selected studies, extracted and validated relevant data. Methodological quality was evaluated using the Jadad score. Meta-analysis was performed using a fixed-effect model for continuous data, reported as weighted mean difference with 95% confidence intervals.
Results: Six RCTs met the inclusion criteria, of which 4 were suitable for statistical pooling. Methodological quality of most trials was good. One study compared an extract of P. sidoides, EPs 7630, against conventional non-antibiotic treatment (acetylcysteine); the other five studies tested EPs 7630 against placebo. All RCTs reported findings suggesting the effectiveness of P. sidoides in treating acute bronchitis. Meta-analysis of the four placebo-controlled RCTs suggested that EPs 7630 significantly reduced bronchitis symptom scores in patients with acute bronchitis by day 7. No serious adverse events were reported.
Conclusion: There is encouraging evidence from currently available data that P. sidoides is effective compared to placebo for patients with acute bronchitis.
Meanwhile, P.sidoides has been associated with liver damage, a fact that might dampen our enthusiasm for this remedy. Nevertheless, it seems to me that this plant merits further study.
I recently came across this paper by Prof. Dr. Chad E. Cook, a physical therapist, PhD, a Fellow of the American Physical Therapy Association (FAPTA), and a professor as well as director of clinical research in the Department of Orthopaedics, Department of Population Health Sciences at the Duke Clinical Research Institute at Duke University in North Carolina, USA. The paper is entitled ‘The Demonization of Manual Therapy‘.
Cook introduced the subject by stating: “In medicine, when we do not understand or when we dislike something, we demonize it. Well-known examples throughout history include the initial ridicule of antiseptic handwashing, percutaneous transluminal coronary angioplasty (i. e., balloon angioplasty), the relationships between viruses and cancer, the contribution of bacteria in the development of ulcers, and the role of heredity in the development of disease. In each example, naysayers attempted to discredit the use of each of the concepts, despite having no evidence to support their claims. The goal in each of the aforementioned topics: demonize the concept.”
Cook then discussed 8 ‘demonizations’ of manual therapy. Number 7 is entitled “Causes as Much Harm as Help“. Here is this section in full:
By definition, harms include adverse reactions (e. g., side effects of treatments), and other undesirable consequences of health care products and services. Harms can be classified as “none”, minor, moderate, serious and severe [67]. Most interventions have some harms, typically minor, which are defined as a non-life-threatening, temporary harm that may or may not require efforts to assess for a change in a patient’s condition such as monitoring [67].
There are harms associated with a manual therapy intervention, but they are generally benign (minor). Up to 20 –40 % of individuals will report adverse events after the application of manual therapy. The most common adverse events were soreness in muscles, increased pain, stiffness and tiredness [68]. There are rare occasions of several harms associated with manual therapy and these include spinal or neurological problems as well as cervical arterial strokes [9]. It is critical to emphasize how rare these events are; serious adverse event incidence estimates ranged from 1 per 2 million manipulations to 13 per 10,000 patients [69].
Cook then concludes that “manual therapy has been inappropriately demonized over the last decade and has been associated with inaccurate assumptions and false speculations that many clinicians have acquired over the last decade. This paper critically analyzed eight of the most common assumptions that have belabored manual therapy and identified notable errors in seven of the eight. It is my hope that the physiotherapy community will carefully re-evaluate its stance on manual therapy and consider a more evidence-based approach for the betterment of our patients.
REFERENCES
[9] Ernst E. Adverse effects of spinal manipulation: a systematic review. J R Soc Med 2007; 100: 330–338.doi:10.1177/014107680710000716 [68] Paanalahti K, Holm LW, Nordin M et al. Adverse events after manual therapy among patients seeking care for neck and/or back pain: a randomized controlled trial. BMC Musculoskelet Disord 2014; 15: 77. doi:10.1186/1471-2474-15-77 [69] Swait G, Finch R. What are the risks of manual treatment of the spine? A scoping review for clinicians. Chiropr Man Therap 2017; 25: 37. doi:10.1186/s12998-017-0168-5
_________________________________
Here are a few things that I find odd or wrong with Cook’s text:
- The term ‘demonizing’ seems to be a poor choice. The historical examples chosen by Cook were not cases of demonization. They were mostly instances where new discoveries did not fit into the thinking of the time and therefore took a long time to get accepted. They also show that sooner or later, sound evidence always prevails. Lastly, they suggest that speeding up this process via the concept of evidence-based medicine is a good idea.
- Cook then introduces the principle of risk/benefit balance by entitling the cited section “Causes as Much Harm as Help“. Oddly, however, he only discusses the risks of manual therapies and omits the benefit side of the equation.
- This omission is all the more puzzling since he quotes my paper (his reference [9]) states that “the effectiveness of spinal manipulation for most indications is less than convincing.5 A risk-benefit evaluation is therefore unlikely to generate positive results: with uncertain effectiveness and finite risks, the balance cannot be positive.”
- In discussing the risks, he seems to assume that all manual therapies are similar. This is clearly not true. Massage therapies have a very low risk, while this cannot be said of spinal manipulations.
- The harms mentioned by Cook seem to be those of spinal manipulation and not those of all types of manual therapy.
- Cook states that “up to 20 –40 % of individuals will report adverse events after the application of manual therapy.” Yet, the reference he uses in support of this statement is a clinical trial that reported an adverse effect rate of 51%.
- Cook then states that “there are rare occasions of several harms associated with manual therapy and these include spinal or neurological problems as well as cervical arterial strokes.” In support, he quotes one of my papers. In it, I emphasize that “the incidence of such events is unknown.” Cook not only ignores this fact but states in the following sentence that “it is critical to emphasize how rare these events are…”
Cook concludes that “manual therapy has been inappropriately demonized over the last decade and has been associated with inaccurate assumptions and false speculations …” He confuses, I think, demonization with critical assessment.
Cook’s defence of manual therapy is clumsy, inaccurate, ill-conceived, misleading and often borders on the ridiculous. In the age of evidence-based medicine, therapies are not ‘demonized’ but evaluated on the basis of their effectiveness and safety. Manual therapies are too diverse to do this wholesale. They range from various massage techniques, some of which have a positive risk/benefit balance, to high-velocity, low-amplitude thrusts, for which the risks do not demonstrably outweigh the benefits.
Tinospora cordifolia, a plant used in Ayurvedic medicine, is a widely grown glabrous, deciduous climbing shrub which has been described in traditional medicine texts to have a long list of health benefits. It contains diverse phytochemicals, including alkaloids, phytosterols, glycosides. Preparations utilize the stem and root of the plant which is consumed in the form of capsules, powder, or juice or in an unprocessed form. Its benefits are said to include anti-inflammatory, anti-pyretic properties, anti-viral and anti-cancer, and immune-boosting properties. The latter alleged activity made it popular during the pandemic. Indian researchers recently reported 6 patients who presented with liver injuries after taking Tinospora cordifolia.
Preparations utilize the stem and root of the plant which is consumed in the form of capsules, powder, or juice or in an unprocessed form. Its benefits are said to include anti-inflammatory, anti-pyretic properties, anti-viral and anti-cancer, and immune-boosting properties. The latter alleged activity made it popular during the pandemic. Indian researchers recently reported 6 patients who presented with liver injuries after taking Tinospora cordifolia.
Case 1
A previously healthy 40- year-old male without comorbidities, presented with jaundice of 15 days duration. On persistent probing, he gave a history of consumption of TC plant twigs (10 to 12 pieces) boiled with cinnamon and cloves in half a glass of water, once in two days for 3 months prior to presentation. USG of the abdomen was unremarkable. He underwent a percutaneous liver biopsy which showed features of the hepatocellular pattern of liver injury – with lymphoplasmacytic cell infiltrate, interface hepatitis, and foci of necrosis – suggesting the diagnosis of DILI with autoimmune features. He was managed with standard medical treatment (SMT) which included multivitamins and ondansetron for associated nausea. He was followed up for 5 months till the complete resolution of symptoms and normalization of liver function.
Case 2
A 54- year -old female, with type 2 diabetes mellitus, presented with jaundice for 1 week. A 7-month history of unsupervised consumption of TC plant (1 twig per day), which was boiled and extract consumed – was obtained. Evaluation for cause revealed a positive ANA (1:100), negative ASMA, negative viral markers, and normal IgG. USG features showing a liver with coarse echotexture, spleen of 13.4 cm, and minimal free fluid in the abdomen. A percutaneous liver biopsy showed a mixed pattern of liver injury (hepatocellular and cholestatic) with features of lymphocytic, neutrophilic and eosinophilic infiltrate, prominent interface hepatitis, intracytoplasmic and canalicular cholestasis, and altered architecture. She was managed with SMT. In view of chronicity, she was started on oral prednisolone in a dose of 40 mg which was tapered over a period of 10 weeks following which there was the resolution of her symptoms, improvement in LFTs and she was advised regular follow up.
Case 3
A 38- year-male with Beta-thalassemia minor presented with jaundice of 1-week duration. He gave a history of consumption of 3-4 TC plant twigs – boiled and extract consumed 15 ml/day for 6 months prior to presentation. Work up for the etiology showed a positive ANA (1:100). USG showed hepatomegaly (16 cm) with diffuse fatty infiltration and splenomegaly (17.3 cm). A percutaneous liver biopsy suggested the diagnosis of drug-induced hepatitis with a hepatocellular pattern of liver injury along with moderate lymphocytic infiltrate admixed with plenty of eosinophils and few plasma cells, mild interface hepatitis. He was managed with SMT and followed up until complete resolution of symptoms and LFTs.
Case 4
A 62- year-old female with type 2 diabetes mellitus, presented with complaints of malaise, reduced appetite and yellowish discoloration of urine, eyes, and skin with abdominal distension for 15 days. She confirmed consumption of commercially available syrup containing TC plant – 15 ml/day, every alternate day for a month, prior to the onset of her symptoms. Investigations revealed a positive ANA (1:320) and ASMA. Imaging showed hepatomegaly and ascites. A trans-jugular liver biopsy suggested a diagnosis of autoimmune hepatitis suggested by lymphoplasmacytic infiltrate with eosinophils and neutrophils, as well as interface hepatitis. There was also cirrhosis suggested by marked lobular disarray, pseudo-glandular transformation, and bridging hepatic fibrosis. She was treated with standard medical therapy including a low salt diet and diuretics for ascites and started on oral prednisolone 40 mg per day. She initially showed clinical improvement and improving trends of LFTs. However, on tapering of steroids, she came back with increasing ascites and oliguria and succumbed to hepato-renal syndrome around 120 days from the first presentation.
Case 5
A 56- year-old female with hypothyroidism presented with yellowish discoloration of urine and eyes. A short, 3-week history of consumption of TC plant boiled extract of 1 twig, 2 to 3 days/week was obtained. Standard investigations for etiology were negative except for a high serum IgG of 2570 mg/dl. The auto-immune markers were negative. USG showed mild ascites, nodular liver, and spleen of 12.3 cm. A trans-jugular liver biopsy showed lymphoplasmacytic infiltrate admixed with plasma cells and eosinophils, moderate interface hepatitis, fibrosis, and altered architecture suggestive of auto-immune cirrhosis. SMT and tapering doses of prednisolone starting with 40 mg orally over 6 weeks led to the resolution of symptoms with the improvement of LFT. She was continued on a maintenance dose of steroids and advised to close follow-up.
Case 6
A 56- year-old female, with hypothyroidism presented with jaundice of 20 days duration. History of TC plant formulation in the form of commercially available tablets – 1 pill a day, for 3 months prior to presentation was obtained. Routine evaluation for the cause of liver injury showed a weakly positive ASMA and a high serum IgG (2045 mg/dl). ANA was negative. USG showed diffuse heterogeneous echotexture of liver and normal-sized spleen. A percutaneous liver biopsy showed chronic hepatitis with lymphoplasmacytic infiltrate, interface hepatitis with significant bridging fibrosis suggesting the possibility of autoimmune hepatitis. She was managed with SMT, leading to complete symptomatic and biochemical resolution. There was no relapse of hepatitis after stopping TC and a follow-up of 2 months.
The authors believe that the liver injury seen in these patients was caused by autoimmune-like hepatitis due to consumption of TC, or the unmasking of latent chronic auto-immune liver disease. Most drug-induced autoimmune liver injuries are an acute idiosyncratic reaction which was also supported by the fact that one patient taking the drug for only 3 weeks on alternate days.
Spinal manipulation therapy (SMT) is widely used worldwide to treat musculoskeletal and many other conditions. The evidence that it works for any of them is weak, non-existent, or negative. What is worse, SMT can – as we have discussed so often on this blog – cause adverse events some of which are serious, even fatal.
Spinal epidural hematoma (SEH) caused by SMT is a rare emergency that can cause neurological dysfunction. Chinese researchers recently reported three cases of SEH after SMT. 
- The first case was a 30-year-old woman who experienced neck pain and numbness in both upper limbs immediately after SMT. Her symptoms persisted after 3 d of conservative treatment, and she was admitted to our hospital. Magnetic resonance imaging (MRI) demonstrated an SEH, extending from C6 to C7.
- The second case was a 55-year-old man with sudden back pain 1 d after SMT, numbness in both lower limbs, an inability to stand or walk, and difficulty urinating. MRI revealed an SEH, extending from T1 to T3.
- The third case was a 28-year-old man who suddenly developed symptoms of numbness in both lower limbs 4 h after SMT. He was unable to stand or walk and experienced mild back pain. MRI revealed an SEH, extending from T1 to T2.
All three patients underwent surgery after failed conservative treatment and all recovered to ASIA grade E on day 5, 1 wk, and day 10 after surgery, respectively. All patients returned to normal after 3 mo of follow-up.
The authors concluded that SEH caused by SMT is very rare, and the condition of each patient should be evaluated in full detail before operation. SEH should be diagnosed immediately and actively treated by surgery.
These cases might serve as an apt reminder of the fact that SMT (particularly SMT of the neck) is not without its dangers. The authors’ assurance that SEH is VERY RARE is a little puzzling, in my view (the paper includes a table with all 17 previously published cases). There is, as we often have mentioned, no post-marketing surveillance, surgeons only see those patients who survive such complications long enough to come to the hospital, and they publish such cases only if they feel like it. Consequently, the true incidence is anyone’s guess.
As pointed out earlier, the evidence that SMT might be effective is shaky for most indications. In view of the potential for harm, this can mean only one thing:
The risk/benefit balance for SMT is not demonstrably positive.
In turn, this leads to the conclusion that patients should think twice before having SMT and should inquire about other therapeutic options that have a more positive risk/benefit balance. Similarly, the therapists proposing SMT to a patient have the ethical and moral duty to obtain fully informed consent which includes information about the risk/benefit balance of SMT and other options.
Ever wondered what homeopathy truly is?
Who better to ask than Boiron?
On their website, Boiron (the largest manufacturer of homeopthics) explains:
Homeopathy is a therapeutic method that uses natural substances to relieve symptoms. It derives from the Greek words homeo, meaning “similar,” and pathos, meaning “suffering” (such as the pathology of a disease). Homeopathy operates on a “like cures like” principle that has been used empirically for more than 200 years and continues to be confirmed in pharmacological research and clinical studies.
What this means is a person suffering from symptoms can be treated by microdoses of a substance capable of producing similar symptoms in a healthy person. It is said that homeopathic medicines stimulate the body’s physiological reactions that restore health. This is accomplished with a very low risk of side effects due to the use of microdoses.
Homeopathy in Action
An example of how homeopathic medicines work is the similarity of symptoms between allergies and chopping onions. When you cut into an onion, your eyes will water and your nose runs. If similar symptoms appear after contact with pollen or a pet, the homeopathic medicine most appropriate to treat these symptoms is made from a tiny amount of onion. Instead of masking symptoms, the medicine sends the body a signal to help it rebalance and heal.
The Benefits of Homeopathy and You
A natural choice. The active ingredients in homeopathic medicines are made from diluted extracts of plants, animals, minerals, or other raw substances found in nature.
For everyday use. Similar to other over-the-counter (OTC) medicines, homeopathic medicines can be used to relieve symptoms of a wide range of common health conditions such as allergies, coughs, colds, flu, stress, arthritis pain, muscle pain, and teething.
Safe and reliable. Homeopathy has been used for more than 200 years, building a remarkable safety record and generating a great body of knowledge. Homeopathic medicines do not mask symptoms, are not contraindicated with pre-existing conditions, and are not known to interact with other medications or supplements, making them one of the safest choices for self-treatment.
Rigorous standards. Homeopathic medicines are manufactured according to the highest standards, complying with U.S. Food and Drug Administration regulations and the Homeopathic Pharmacopoeia of the United States (HPUS).
More choices and preferences. Homeopathic medicines are available in a variety of dosage forms such as gels, ointments, creams, syrups, eye drops, tablets, and suppositories.
_________________________
Are you pleased with this explanation?
No?
One must not be too harsh with Boiron and forgive them their errors; a powerful conflict of interest might have clouded their views. Therefore, I shall now take the liberty to edit and update their text ever so slightly.
Homeopathy is an obsolete method that used all sorts of substances in the misguided hope to relieve symptoms. The word derives from the Greek words homeo, meaning “similar,” and pathos, meaning “suffering” (such as the pathology of a disease). Homeopathy was alleged to operate on a “like cures like” principle that had been used empirically for more than 200 years but was refuted by pharmacological research, clinical studies and more.
What it suggested was that a person suffering from symptoms might be treated by the absence of a substance capable of producing similar symptoms in a healthy person. It was said that homeopathic medicines stimulate the body’s physiological reactions that restore health. These assumptions proved to be erroneous.
Homeopathy in Action
An example of how homeopathic medicines were supposed to work is the similarity of symptoms between allergies and chopping onions. When you cut into an onion, your eyes will water and your nose runs. If similar symptoms appear after contact with pollen or a pet, the homeopathic medicine most appropriate to treat these symptoms was assumed to be made with the memory of an onion. These ideas were never proven and had no basis in science.
The Alleged Benefits of Homeopathy
A natural choice. The active ingredients in homeopathic medicines were often made from diluted extracts of plants, animals, minerals, or other raw substances found in nature. The appeal to nature is, however, misleading: firstly the typical remedy did not contain anything; secondly, some remedies were made from synthetic substances (e. g. Berlin wall) or no substances (e. g. X-ray).
For everyday use. Similar to other over-the-counter (OTC) medicines, homeopathic medicines were promoted to relieve symptoms of a wide range of common health conditions such as allergies, coughs, colds, flu, stress, arthritis pain, muscle pain, and teething. These claims could never be verified and are therefore bogus.
Safe and reliable. Homeopathy had been used for more than 200 years. During all these years, no reliable safety record or body of knowledge had been forthcoming. Homeopathic medicines do not mask symptoms, are not contraindicated with pre-existing conditions, and are not known to interact with other medications or supplements. In fact, they have no effects whatsoever beyond placebo.
Rigorous standards. Homeopathic medicines were said to be manufactured according to the highest standards, complying with U.S. Food and Drug Administration regulations and the Homeopathic Pharmacopoeia of the United States (HPUS). This guaranteed that they were devoid of any active ingredient and made them pure placebos.
More choices and preferences. Homeopathic medicines were available in a variety of dosage forms such as gels, ointments, creams, syrups, eye drops, tablets, and suppositories. This means they offered a range of placebos to chose from.
In case, Boiron feels like adopting my updated, evidence-based version of their text, I am sure we can come to an agreement based on an adequate fee.