Monthly Archives: October 2021
Guest post by Emeritus Professor Alastair MacLennan AO, MB ChB, MD, FRCOG, FRANZCOG
The sale and promotion of a therapeutic drug in most countries require rigorous assessment and licencing by that country’s therapeutic regulatory body. However, a new surgical technique can escape such checks and overview unless the technique is subject to local medical ethics review in the context of a research trial. New medical devices in Australia such as carbon dioxide or Er-YAG lasers can be listed on its therapeutic register without critical review of their efficacy and safety. Thermal injury to the postmenopausal vaginal wall in the hope of rejuvenating it has become a lucrative fad for some surgeons outside formal well-conducted clinical trials.
There are many published studies of this technique but the large majority are small, uncontrolled and observational. The few randomised controlled trials using sham controls show a placebo effect and debatable clinical efficacy with limited follow-up of adverse effects. A review of these therapies in July 2020 published by The National Institute for Health and Care Excellence summarised apparent claims for some efficacy in terms of vaginal dryness, dyspareunia, sexual function, and incontinence but noted confounding in the study’s designs such as concurrent breast cancer treatments, local oestrogen therapy and lubricants (!). Most studies had very limited follow up for adverse events but elsewhere the literature has reported burns, infection, increased dyspareunia and scarring. There is no physiological mechanism by which burning atrophic vaginal epithelium will magically rejuvenate it.
A recent well-conducted randomised sham-controlled trial with a 12-month follow-up of Fractional Carbon Dioxide Laser for the treatment of vaginal symptoms associated with menopause has been published in JAMA by Li et al has shown no efficacy for this treatment(2).
At 12 months, there was no difference in overall symptom severity based on a 0-100 scale (zero equals no symptoms), with a reduction in symptom severity of 17.2 in the treatment group compared with 26.6 in the sham group.
The treatment had no impact on quality of life. “Sexual activity rates and quality of sex were not significantly different between the groups at baseline or 12 months”. The study compared 46 paired vaginal wall biopsies, taken at baseline and six months into treatment, and no significant histological improvement with laser was evident.
“The annual cost of laser treatment to the individual for management of vaginal menopausal symptoms was reported to be AUD$2,733, and because there is no demonstrable difference versus sham treatment, it cannot be considered to be cost-effective.”
Although one could still call for more quality sham-controlled randomised trials in different circumstances there is no justification for touting this therapy commercially. Complications following this therapy outside of ethical trials could become the next medico-legal mine-field.
Vaginal atrophy in the years after menopause is almost universal and is primarily due to oestrogen deficiency. The efficient solution is local vaginal oestrogen or systemic hormone replacement therapy. However, the misreporting of the Women’s Health Initiative and Million Women’s Study has created exaggerated fear of oestrogen therapies and thus a market for alternative and often unproven therapies (3). The way forward is education and tailoring of hormonal therapies to minimise risk and maximise efficacy and quality of life and not to resort to quackery.
References
1. https://www.nice.org.uk/guidance/ipg697/documents/overview
2. Li FG, Maheux-Lacroix S, Deans R et al. Effect of Fractional Carbon Dioxide Laser vs Sham Treatment on Symptom Severity in Women With Postmenopausal Vaginal Symptoms A Randomized Clinical Trial. JAMA. 2021;326:1381-1389.
3. MacLennan AH. Evidence-based review of therapies at the menopause. Int J Evid Based Healthc 2009; 7: 112-123.
As we have discussed ad nauseam on this blog, spinal manipulation therapy (SMT) can cause serious adverse events, including spinal epidural hematoma (SEH), an emergency that can cause severe neurological dysfunction. Chinese surgeons have reported three cases of SEH after SMT.
- The first case was a 30-year-old woman who experienced neck pain and numbness in both upper limbs immediately after SMT. Her symptoms persisted after 3 d of conservative treatment, and she was admitted to our hospital. Magnetic resonance imaging (MRI) demonstrated an SEH, extending from C6 to C7.
- The second case was a 55-year-old man with sudden back pain 1 d after SMT, numbness in both lower limbs, an inability to stand or walk, and difficulty urinating. MRI revealed an SEH, extending from T1 to T3.
- The third case was a 28-year-old man who suddenly developed symptoms of numbness in both lower limbs 4 h after SMT. He was unable to stand or walk and experienced mild back pain. MRI revealed an SEH, extending from T1 to T2.
All three patients underwent surgery after failed conservative treatment. Blood clots were found during the operation in case 1 and case 2, and the postoperative pathology confirmed a hematoma. In case three, a vein ruptured during the operation, causing massive bleeding. The three patients recovered to ASIA grade E on day 5, 1 wk, and day 10 after surgery, respectively. All patients returned to normal after 3 mo of follow-up.
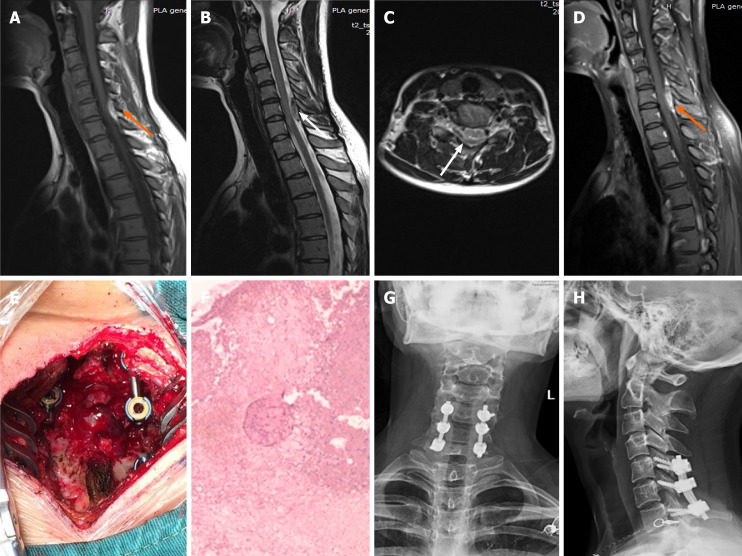
Imaging examinations of case 1. A: T1-weighted preoperative magnetic resonance imaging (MRI) image shows high signal intensity (orange arrow); B and C: Preoperative T2-weighted image shows low signal intensity, and an axial T2-weighted image demonstrates that the hematoma occurred in the posterior region (white arrow); D: Preoperative enhanced MRI suggests an enhanced hematoma signal (orange arrow); E: Intraoperative photograph shows that spinal cord compression has recovered; F: Postoperative pathology suggested a hematoma; G and H: X-ray at the 3-mo follow-up indicated intact internal fixation.
The authors concluded that before proceeding with SMT, each patient should be evaluated in detail and checked for risk factors. In cases where the physical condition changes rapidly, physicians should be alert to the danger and send the patient to the emergency department for a complete MRI examination. We recommend surgery if neurological symptoms appear.
In their paper, the authors also review 15 further cases of SEH that have been previously published. They stress several times in their article that this complication is rare. In my view, this begs the question: how do they know? As there is no post-marketing surveillance of chiropractors or other clinicians doing SMT, I would insist that nobody can be sure about the true incidence of SEH or any other complication after SMT.
Recently, I wrote about the court case of a French naturopath. Last week, the judge has issued his verdict. Miguel Barthéléry was sentenced to a two-year suspended prison term and to a fine of 5 000 Euros. Two cancer patients had died following his treatments and recommendations. Barthéléry was also found guilty of impersonating a doctor and illegally practising medicine. In addition, he was also banned for life from practising as a healthcare professional.
to a two-year suspended prison term and to a fine of 5 000 Euros. Two cancer patients had died following his treatments and recommendations. Barthéléry was also found guilty of impersonating a doctor and illegally practising medicine. In addition, he was also banned for life from practising as a healthcare professional.
The Paris criminal court found that Miguel Barthéléry had deliberately created confusion about his qualifications by presenting himself as a doctor on the internet and in text messages to the two victims. The defendant had claimed to have a doctorate and a post-doctorate from the United States. The judgment “has the consequence of dissuading all those who engage in the same abuses, they are now warned that we can not do anything with the health of people,” said the judge.
The case had begun in February 2019 with the complaint of the companion of a man who had died two months earlier of testicular cancer. Diagnosed in 2016, the patient had not consulted a doctor but had preferred to follow a “health plan” drawn up by the naturopath. It was based on fasting and cures, raw food, and essential oils. Later, the family of a Belgian physiotherapist, who died of uterine cancer at the age of 39, joined the legal case. However, according to Code Source, the Parisien podcast, the case is more extensive, with seven further suspicious deaths of Barthéléry’s patients.
Barthéléry’s lawyer said that the decision “raises questions more generally about the appreciation that we now have of alternative therapeutic practices, which now seem, although not prohibited by law, to be subject to condemnation by the courts.”
The bad news for German homeopathy just keeps on coming. As I reported, recent events must be depressing for homeopaths, e.g.:
- A recent investigation disclosed that the German homeopathy cult is at the heart of Germany’s anti-vax movement.
- In July 2021, a German court ruled against a homeopathic HCG remedy.
- In 2020, a German study failed to show that homeopathy is cost-effective.
- In 2019, the attempt by a German homeopathy manufacturer to silence critics backfired spectacularly.
- About 10 years ago, 5 German firms clubbed together supporting a journalist at the tune of Euro 30 000/year to defame me (at the time I was one of the few who regularly informed the public about the evidence on homeopathy). The plot was discovered and published whereupon the journalist committed suicide.
After heated debates in the run-up, the Bavarian Medical Association decided yesterday to ditch the postgraduate education program in homeopathy for its doctors. This means that, of the 17 regional medical associations in Germany, 12 have now discontinued their further education efforts in homeopathy. The ones that have not yet done so are:
- Baden-Württemberg,
- Rhineland-Palatinate,
- Saxony,
- Thuringia,
- Westphalia-Lippe.
In the past months, homeopaths had collected 11,597 signatures in favor of maintaining the additional qualification of homeopathy. The ~ 400 doctors in Bavaria, who have acquired ‘homeopathy’ as an additional title, will be permitted to continue to use it.
The spokesperson of the Information Network Homeopathy, Dr. Christian Lübbers, welcomed the decision of the Medical Association. It was a “landslide victory for patient safety”, he said. The Bavarian regional chairman of the German Central Association of Homeopathic Doctors, Dr. Ulf Riker, regretted the outcome of the vote and added: “We will consider legal steps very seriously.” I would advise against such a step which would only render homeopaths more ridiculous than they already are.
Yes, it’s bad news for German homeopaths – very bad news indeed. Of course, homeopathy fans will claim that it is all a sinister conspiracy against them. Sadly, they are unable to realize that the only driving force behind the long-overdue decline of German homeopathy is the evidence: HOMEOPATHY DOES NOT WORK BEYOND PLACEBO and therefore it has no place in the evidence-based medicine of the 21st century.
One argument that we hear regularly in the comment sections of this blog and elsewhere goes something like this:
“Why worry about a bit of so-called alternative medicine (SCAM like homeopathy or chiropractic, or Reiki, or Bach flower remedies, or detox, etc.)? Why should it bother us? Why not let everyone use what they want? Why not be a bit more tolerant?”
Tolerance is defined as sympathy or indulgence for beliefs or practices differing from or conflicting with one’s own. It is, of course, a quality that normally should be welcomed, taught, and celebrated. So, why not be more tolerant with enthusiasts of pseudoscientific SCAM?
In my view, there are several reasons.
- Ineffective therapies harm patients. The public tends to believe that SCAM is inherently safe. This is, of course, not true – think of chiropractic, for instance. But some treatments seem entirely harmless. Homeopathy might be a good example; its remedies contain nothing and therefore homeopathy can do no harm. Sadly, this is not true either. If a patient uses homeopathy to treat a serious condition, she is likely to harm herself by not treating that condition effectively. In extreme cases, this course of action can be fatal.
- Ineffective therapies are a waste of resources. It seems obvious that the money spent on something that does not work is money wasted. This is true whether we buy a car that is beyond repair or a SCAM that does not work beyond placebo.
- Pseudoscience makes a mockery of evidence-based medicine. If we are tolerant towards useless SCAM and accept that some people make money on, and mislead the public about SCAM, we basically send out a message that evidence is of secondary importance. This would weaken the trust in evidence-based medicine which, in turn, is bound to render healthcare less effective and stand in the way of progress.
- Pseudoscience undermines rationality and one form of irrationality begets another. Perhaps the biggest danger of tolerating promoters of quackery is that this undermines rational thinking far beyond the realm of healthcare. “Those who can make you believe absurdities can make you commit atrocities,” wrote Voltaire. I fear that he might have been correct.
In my view, tolerance about pseudoscientific, implausible, ineffective, or harmful SCAMs is misplaced. On the contrary, I feel that it is our duty to limit the harm they do to the public, patients, and progress by exposing them for what they are.
I was asked by the ‘Science Media Centre’ (SMC) to provide a short comment on the following press release (which was embargoed until today):
Daily use of cannabidiol (‘CBD’) oil may be linked to lung cancer regression
… The report authors describe the case of a woman in her 80s, diagnosed with non-small cell lung cancer. She also had mild chronic obstructive pulmonary disease (COPD), osteoarthritis, and high blood pressure, for which she was taking various drugs.
She was a smoker, getting through around a pack plus of cigarettes every week (68 packs/year).
Her tumour was 41 mm in size at diagnosis, with no evidence of local or further spread, so was suitable for conventional treatment of surgery, chemotherapy, and radiotherapy. But the woman refused treatment, so was placed under ‘watch and wait’ monitoring, which included regular CT scans every 3-6 months.
These showed that the tumour was progressively shrinking, reducing in size from 41 mm in June 2018 to 10 mm by February 2021, equal to an overall 76% reduction in maximum diameter, averaging 2.4% a month, say the report authors.
When contacted in 2019 to discuss her progress, the woman revealed that she had been taking CBD oil as an alternative self-treatment for her lung cancer since August 2018, shortly after her original diagnosis.
She had done so on the advice of a relative, after witnessing her husband struggle with the side effects of radiotherapy. She said she consistently took 0.5 ml of the oil, usually three times a day, but sometimes twice.
The supplier had advised that the main active ingredients were Δ9-tetrahydrocannabinol (THC) at 19.5%, cannabidiol at around 20%, and tetrahydrocannabinolic acid (THCA) at around 24%.
The supplier also advised that hot food or drinks should be avoided when taking the oil as she might otherwise feel stoned. The woman said she had reduced appetite since taking the oil but had no other obvious ‘side effects’. There were no other changes to her prescribed meds, diet, or lifestyle. And she continued to smoke throughout.
This is just one case report, with only one other similar case reported, caution the authors. And it’s not clear which of the CBD oil ingredients might have been helpful.
“We are unable to confirm the full ingredients of the CBD oil that the patient was taking or to provide information on which of the ingredient(s) may be contributing to the observed tumour regression,” they point out.
And they emphasise: “Although there appears to be a relationship between the intake of CBD oil and the observed tumour regression, we are unable to conclusively confirm that the tumour regression is due to the patient taking CBD oil.”
Cannabis has a long ‘medicinal’ history in modern medicine, having been first introduced in 1842 for its analgesic, sedative, anti-inflammatory, antispasmodic and anticonvulsant effects. And it is widely believed that cannabinoids can help people with chronic pain, anxiety and sleep disorders; cannabinoids are also used in palliative care, the authors add.
“More research is needed to identify the actual mechanism of action, administration pathways, safe dosages, its effects on different types of cancer and any potential adverse side effects when using cannabinoids,” they conclude.
The SMC published three invited comments:
Prof David Nutt, The Edmond J Safra Chair in Neuropsychopharmacology, Imperial College London, said:
“This is one of many such promising single case reports of medical cannabis self-treatment for various cancers. Such case reports are biologically credible given the adaptogenic nature of the endocannabinoid system. A case report itself is not sufficient to give any form of proof that one thing caused the other – we need trials for that. There are some controlled trials already started and more are required to properly explore the potential of medical cannabis in a range of cancers.”
Prof Edzard Ernst, Emeritus Professor of Complementary Medicine, University of Exeter, said:
“Cannabinoids have been shown to reduce the size of prostate cancer tumours in animal models. Previous case reports have yielded encouraging findings also in human cancers. However, case reports cannot be considered to be reliable evidence, and there are currently no data from rigorous clinical trials to suggest that cannabis products will alter the natural history of any cancer.”
Dr Tom Freeman, Senior Lecturer and Director of the Addiction and Mental Health Group, University of Bath, said:
“These results are exciting and very encouraging for this patient. However as a single case study the quality of scientific evidence is low and should not be used to change clinical practice. People with lung cancer should always seek guidance from a healthcare professional when deciding on an appropriate treatment.
“The product used by this patient reportedly contained high levels of THC (the intoxicating component of cannabis), and was sourced from outside the UK. This type of product is very different to most CBD oils which predominantly contain CBD. Unlike prescribed medicines, CBD wellness products lack assurance of quality, safety or efficacy and should not be used for medicinal purposes.”
The original paper has now been published and can be found here.
The ‘International Chiropractors Association’ (ICA) has just issued a statement entitled “International Chiropractors Association Affirms Policy on Health Freedom“. On the background of the fact that US President Biden, issued a series of Executive Orders related to mandating federal employees and federal contractors to receive the COVID-19 vaccine, the ICA try to explain their position regarding vaccinations. Here are a few passages from this statement:
…In a world of public health that promotes evidence-based decision making, we see the importance of natural immunity being ignored and replaced with a totalitarian approach of compulsory vaccination. At a time when the Surgeon General says misinformation has become an urgent threat to public health, misinformation is now being used in an attempt to discredit the chiropractic profession, the International Chiropractors Association, and all chiropractic patients who desire to focus on improving health naturally. After enduring 18 months of shutdowns, lockdowns, flattening the curve, masking, limitations of speech on social media; and a cancel culture environment that threatens the basic freedoms our country was founded upon in 1776, ICA will not compromise on the importance of protecting health freedom…
The ICA Policy on Immunization and Vaccination has remained unchanged for almost 50 years and clearly states:
“The International Chiropractors Association recognizes that the use of vaccines is not without risk and questions the wisdom of mass vaccination programs. Chiropractic principles favor the enhancement of natural immunity over artificial immunization.
The ICA supports each individual’s right to select his or her own health care and to be made aware of the possible adverse effects of vaccines upon a human body. In accordance with such principles and based upon the individual’s right to freedom of choice, the ICA is opposed to compulsory programs which infringe upon such rights.
The International Chiropractors Association is supportive of a conscience clause or waiver in compulsory vaccination laws, providing an elective course of action for all regarding immunization, thereby allowing patients freedom of choice in matters affecting their bodies and health.”
The International Chiropractors Association maintains that all healthcare interventions, including the chiropractic adjustment, are associated with some level of risk and that every individual is entitled to be informed of those risks, no matter how insignificant. All individuals must retain the freedom to accept or reject any healthcare product, procedure, or medication including vaccinations. The International Chiropractors Association therefore strongly opposes the use of medical mandates that violate personal sovereignty, violate the principles of informed consent, and constrain the rights of patients to make their own health care choices…
The ICA encourages the recognition that natural efforts to enhance the innate immune system ability to adapt to novel viruses are grounded in science and rejects the notion that the patients’ freedom to rely on naturally acquired immunity is not based upon unscientific beliefs.
The ICA rejects the premise that the chiropractic profession’s long history of promoting health freedom and supporting conscientious exemptions is based upon unscientific or non-mainstream beliefs…
I find this statement clear as mud and have the following questions:
- Do the ICA recommend vaccinations?
- In particular, do they encourage their members to get vaccinated with the COVID-19 vaccines?
- Do they advise to recommend COVID-19 vaccinations to their patients?
- Or do they think that natural immunity is preferable and advise their members and patients accordingly?
- Do they believe that spinal manipulation enhances natural immunity?
- Do they think that spinal manipulations are an effective alternative to COVID-19 vaccinations?
- Do they believe that scientific evidence trumps dogma or vice versa?
- Which of the two should, according to their conviction, must influence the decision-making processes in healthcare?
- If the ICA object to misinformation about COVID, why do they not stop their members from promoting it?
- What makes them think that information about the possible adverse effects of vaccines upon a human body is unavailable?
- If the ICA recognizes the risks of spinal manipulation, why do they not inform the public about them regularly and objectively?
- If the ICA knows about the importance of informed consent, why do not all of their members adhere to it?
- And finally, why do the ICA insist on the term ‘international’ in the name of their organization, if they purely deal with the US situation?
I do not expect the ICA to give me the answers to these questions. But perhaps their Wiki page goes some way towards answering some of them: “… The ICA supports the efforts of the National Vaccine Information Center (NVIC).[13] The NVIC is known for promoting false and misleading information about vaccines, in particular the discredited claim that vaccines cause autism.
The ICA’s annual conferences have featured anti-vaccination propaganda. In 2018 Guest Speaker Beau Pierce (Pierce co-produced a series entitled Vaccines Revealed) hosted a session entitled Vaccines Revealed.,[14] and Jeff Hays, known for producing the anti-Vaccine propaganda Vaccines Revealed, was invited to host a session the 2017 ICA Council on Chiropractic Pediatrics Annual Conference. In 2016 the widely discredited anti-vaccination propaganda film VAXXED was shown at a conference sponsored by the ICA’s Council on Chiropractic Pediatrics …”
SAY NO MORE!
Therapeutic touch (TT) is a form of paranormal or energy healing developed by Dora Kunz (1904-1999), a psychic and alternative practitioner, in collaboration with Dolores Krieger, a professor of nursing. TT is popular and practised predominantly by US nurses; it is currently being taught in more than 80 colleges and universities in the U.S., and in more than seventy countries. According to one TT-organisation, TT is a holistic, evidence-based therapy that incorporates the intentional and compassionate use of universal energy to promote balance and well-being. It is a consciously directed process of energy exchange during which the practitioner uses the hands as a focus to facilitate the process.
The question is: does TT work beyond a placebo effect?
This review synthesized recent (January 2009–June 2020) investigations on the effectiveness and safety of therapeutic touch (TT) as a therapy in clinical health applications. A rapid evidence assessment (REA) approach was used to review recent TT research adopting PRISMA 2009 guidelines. CINAHL, PubMed, MEDLINE, Cochrane databases, Web of Science, PsychINFO, and Google Scholar were screened between January 2009-March 2020 for studies exploring TT therapies as an intervention. The main outcome measures were for pain, anxiety, sleep, nausea, and functional improvement.
Twenty-one studies covering a range of clinical issues were identified, including 15 randomized controlled trials, four quasi-experimental studies, one chart review study, and one mixed-methods study including 1,302 patients. Eighteen of the studies reported positive outcomes. Only four exhibited a low risk of bias. All others had serious methodological flaws, bias issues, were statistically underpowered, and scored as low-quality studies. Over 70% of the included studies scored the lowest score possible on the GSRS weight of evidence scale. No high-quality evidence was found for any of the benefits claimed.
The authors drew the following conclusions:
After 45 years of study, scientific evidence of the value of TT as a complementary intervention in the management of any condition still remains immature and inconclusive:
- Given the mixed result, lack of replication, overall research quality and significant issues of bias identified, there currently exists no good quality evidence that supports the implementation of TT as an evidence‐based clinical intervention in any context.
- Research over the past decade exhibits the same issues as earlier work, with highly diverse poor quality unreplicated studies mainly published in alternative health media.
- As the nature of human biofield energy remains undemonstrated, and that no quality scientific work has established any clinically significant effect, more plausible explanations of the reported benefits are from wishful thinking and use of an elaborate theatrical placebo.
TT turns out to be a prime example of a so-called alternative medicine (SCAM) that enthusiastic amateurs, who wanted to prove TT’s effectiveness, have submitted to multiple trials. Thus the literature is littered with positive but unreliable studies. This phenomenon can create the impression – particularly to TT fans – that the treatment works.
This course of events shows in an exemplary fashion that research is not always something that creates progress. In fact, poor research often has the opposite effect. Eventually, a proper scientific analysis is required to put the record straight (the findings of which enthusiasts are unlikely to accept).
In view of all this, and considering the utter implausibility of TT, it seems an unethical waste of resources to continue researching the subject. Similarly, continuing to use TT in clinical settings is unethical and potentially dangerous.
Germany seems to have a significant problem with anti-vaxxers. Today, only 68% of the population has had a COVID vaccination. In the UK and France, these figures are 72% and 75% respectively.
How come?
This study investigated the willingness to vaccinate of parents of minors and people without children who are minors. The investigation was based on a random sample of Germans (telephone survey, n = 2,014, collected between 12 November and 10 December 2020). The evaluation is primarily based on the sub-sample of people with minors in the household (n = 461).
Parents of minors consistently show a lower willingness to be vaccinated with a COVID-19 vaccine than respondents without minors (54.1% vs 71.1%). Fathers show a stronger willingness to be vaccinated than mothers. Furthermore, men are more willing to get their own child vaccinated with a COVID-19 vaccine than are women.
The authors concluded that among parents and especially mothers, a considerable misrepresentation of vaccination risks and frequent beliefs in vaccination conspiracy theories can be observed. Clear and easily understandable information on the effects and side effects of vaccination with a COVID-19 vaccine by relevant institutions and physicians is recommended.
And what has this to do with so-called alternative medicine (SCAM) and homeopathy?
In the results section of the paper, the authors report interesting additional findings (my translation):
In the total sample, a significantly higher willingness to vaccinate is associated with the rejection of “alternative healing methods”. There is also a significant correlation between the attitude towards homeopathy and one’s own willingness to vaccinate: if homeopathy is supported, the willingness to vaccinate is lower. This correlation between the attitude towards homeopathy and willingness to vaccinate is also evident in the sub-sample of parents. Among parents, it is again women who significantly more often have a positive attitude towards homeopathy than men, who more often do not think anything of it.
The authors also report that the parents were asked: “If a vaccine against the coronavirus is approved in Germany, would you get vaccinated?” CERTAINLY NOT was the answer of:
- 41% of homeopathy fans
- 10% of people who thought nothing at all about homeopathy
- 15% of participants who were not fully convinced by homeopathy
Yes, Germany seems to have a problem with the anti-vaccination brigade but it seems that at the heart of it is a problem with a homeopathy cult.
A second look at old research suggested that the recommended dose for vitamin C is far too low. Here is the abstract of the recently published paper:
A double-blind controlled trial initiated in 1944 has led to the common narrative that a 10-mg daily vitamin C intake is adequate to prevent and treat impaired wound healing, and by inference, other collagen-related diseases such as heart disease or stroke. The WHO relies on this narrative to set the recommended nutrient intake for vitamin C. This narrative, however, is based on what is known as the eyeball method of data assessment. The 1944 trial published individual participant data on scar strength providing an opportunity to statistically probe the validity of the 10-mg narrative, something which has not yet been done. The findings show that a vitamin C intake that averages to 10 mg/d over a mean follow-up of 11.5 mo was associated with a 42% weakened scar strength when compared with 80 mg vitamin C intake/d (P < 0.001). The observed dose-response curve between scar strength and vitamin C intake suggests that the daily vitamin C intake needed to prevent collagen-related pathologies is in the range recommended by the National Academy of Medicine and the European Food Safety Authority (75 to 110 mg/d), not the WHO recommendation (45 mg/d). The findings also show that a vitamin C intake that averages to 65 mg/d over a mean follow-up of 6.5 mo failed to restore the normal wound-healing capacity of vitamin C-depleted tissues; such tissues had a 49% weaker scar strength when compared with nondepleted tissues (P < 0.05). Thus, average daily vitamin C intakes ∼50% higher than the WHO recommends may fail to treat existing collagen-related pathologies. It is concluded that the prior lack of statistical analyses of a landmark trial may have led to a misleading narrative on the vitamin C needs for the prevention and treatment of collagen-related pathologies.
The lead author of the recent re-analysis, Professor Philippe Hujoel from the Department of Epidemiology, School of Public Health, University of Washington, Seattle, said: “The vitamin C experiment is a shocking study. They depleted people’s vitamin C levels long-term and created life-threatening emergencies. It would never fly now. The findings of the re-analyses of the Sorby data suggest that the WHO’s recommendation is too low to prevent weak scar strength. Robust parametric analyses of the trial data reveal that an average daily vitamin C intake of 95mg is required to prevent weak scar strength for 97.5 percent of the population. Such a vitamin C intake is more than double the daily 45mg vitamin C intake recommended by the WHO but is consistent with the writing panels for the National Academy of Medicine and (other) countries.”
The original research of 1944 was headed by the British-German biologist and Nobel-prize winner Sir Hans Adolf Krebs. At the time, researchers conducted an experiment that controlled and monitored vitamin C consumption of just 20 volunteers. They were each given varying amounts of vitamin C, which helps the body to produce collagen – and given wounds to observe how quickly their scar tissue healed. The research aimed to ascertain how much vitamin C navy members living off rations is required in order to prevent them from developing scurvy, rather than how much is needed to boost health overall.
Prof Hujoel concluded that: “The failure to reevaluate the data of a landmark trial with novel statistical methods as they became available may have led to a misleading narrative on the vitamin C needs for the prevention and treatment of collagen-related pathologies.”