Monthly Archives: July 2020
New German Medicine?
German New Medicine?
What on earth is that?
German New Medicine (GNM) is the creation of Ryke Geerd Hamer (1935-2017), a German doctor. The name is reminiscent of the ‘Neue Deutsche Heilkunde’ created by the Nazis during the Third Reich. Hamer received his medical licence in 1963 but was later struck off because of malpractice. He then continued his practice as a ‘Heilpraktiker’. According to proponents, GNM Therapy is a spoken therapy based on the findings and research of the Germanic New Medicine of Dr.Hamer. On the understanding that every disease is triggered by an isolating and shocking event, GNM Therapy assists in finding the DHS (shocking moment) in our lives that preceded the dis-ease and in turn allowing our bodies to complete its natural healing cycle back to full health. Hamer believed to have discovered the ‘5 laws of nature’:
- The Iron Rule of Cancer
- The two-phased development of disease
- Ontogenetic system of tumours and cancer equivalent diseases
- Ontogenetic system of microbes
- Natures biological meaning of a disease
Hamer also postulated that:
- All diseases are caused by psychological conflicts.
- Conventional medicine is a conspiracy of Jews to decimate the non-Jewish population.
- Microbes do not cause diseases.
- AIDS is just an allergy.
- Cancer is the result of a mental shock.
None of Hamer’s ‘discoveries’ and assumptions are plausible or based on facts, and none of his therapeutic approaches have been shown to be effective.
These days, I do not easily get surprised by what I read about so-called alternative medicine (SCAM), but this article entitled ‘Homoeopathy And New German Medicine: Two German Siblings‘ baffled me greatly. Here are a few short excerpts:
… German New Medicine (GNM) like Homoeopathy is one of the gentle healing methods. As siblings, they have some common features as well as their own unique features. So, let’s explore a unique relationship between these two siblings.
1) Holistic aspect:
Both therapeutic methods are believed in holistic concept of body. The disease condition in Homoeopathy and conflict in GNM are very similar in expression as they are reflecting on mental as well as physical level also. In Homoeopathy, Mind, Body and Soul are one of the important trios to understand the Homoeopathic philosophy. While in GNM, Psyche, Brain, Body are important aspect in learning the GNM. Let’s see these trio in their founder’s language,
• Homoeopathy:
Dr. Hahnemann in his oragnon of medicine, 6th edition mentioned about a unity of materialistic body and vital force. Last lines of aphorism 15 are as follows, “…although in thought our mind separates these two unities into distinct conceptions for the sake of easy comprehension.
• German New Medicine:
Dr. Ryke Geerd Hamer, founder of GNM said that, “The differentiation between psyche, brain and the body is purely academic. In reality, they are one.”
2) Disease origin concept:
• Homoeopathy:
In Homoeopathy, disease originates from the dynamic disturbances and followed by functional and pathological changes.
• German New Medicine:
In GNM, morbid condition starts from conflict in the psyche level and later it reflects on body. The common feature is the disturbance is at the all levels of man.
3) Cause of disease:
• Homoeopathy:
In Homoeopathy, among the web of causations, psyche (mind) is also considers as a cause of disease.
• German New Medicine:
So, in GNM, psyche is playing important role in cause of disease. When Conflict starts, its dynamic effect perceived first at mind level.
4) Individuality:
• Homoeopathy:
In Homoeopathy, diathesis is a predisposition for disease condition. i.e. According to the diathesis every individual suffers with their own individual morbid dispositions. Rheumatic diathesis, gouty diathesis, etc. are the examples of diathesis.
• German New Medicine:
In GNM, every individual suffers from the disease condition after the receiving conflict. It is different and depending upon the type of conflict they are receiving. E.g. lung cancer- death fright conflict, cervical cancer –female sexual conflict…
Conclusion:
Some similarities and with some own characteristics, these two healing methods are developing at a good length in medical science. The main aim of these both methods is – “to serve the suffering humanity in gentle way”…
_____________________
Could it be that the author forgot the most striking similarities between GNM and homeopathy? How about these points:
- There is nothing truly gentle about either methods.
- Both are based on bizarre fantasies, far removed from reality.
- Both pretend to be a panacea.
- Both lack proof of efficacy.
- Both have the potential to kill patients (mostly through neglect).
- Both mislead consumers.
- Both are deeply anti-scientific.
- Both dissuade patients from using evidence-based healthcare.
- Both are in conflict with medical ethics.
- Both have cult-like features.
- Both are far from being recognised by proper healthcare.
- Both have been repeatedly in conflict with the law.
- Both were invented by deludes fanatics.
ANDREW WAKEFIELD has been mentioned on this blog before (see here and here, for instance). He is, of course, the UK doctor who published false data about vaccination and autism in the Lancet, was struck off the medical register, and then moved to the US where he has become the darling of anti-vaxxers of all types, including Donald Trump, chiropractors and homeopaths. More recently, he seems to have become the star and guru of the growing cult opposing a vaccination against COVID-19, even before one has become available.
Already in March, Wakefield attended an anti-vaxx meeting and told those watching: “One of the main tenets of the marketing of mandatory vaccination has been fear. And never have we seen fear exploited in the way that we do now with the coronavirus infection.”
Citing what he called ‘unambiguous’ evidence that the coronavirus is no more deadly than seasonal flu, and claiming that the pathogen’s death toll had been greatly exaggerated, Wakefield more recently claimed that the crisis had led to ‘a destruction of the economy, a destruction of people and families, and unprecedented violations of health freedom… and it’s all based upon a fallacy’.
The disgraced ex-doctor noted that the COVID-19 pandemic is one big hoax: a cynical plot by pharmaceutical giants — aided by governments, scientists and the media — to force the world to be unnecessarily and dangerously vaccinated. Describing vaccines as ‘intrinsically unsafe’, ex-doctor Wakefield called on free-thinking people to refuse to be vaccinated against Covid-19 if and when a jab becomes available.
‘We have to stand and fight,’ the 63-year-old intoned. ‘As Nelson Mandela said at his trial, there are ideals worth dying for . . . I don’t want to get too dramatic, but better to die as a free man than live as a slave . . . We have to fight to preserve [our] freedom because it will be surely stripped from us in a very short space of time if we don’t.’
Convincing his disciples that he was the victim of a conspiracy by the pharmaceutical industry, medical establishment and media, Wakefield now neatly argues that the same shadowy cabal are lying to the public about coronavirus. Having terrified one generation of parents — leading, some believe, to a spike in measles among children and a number of deaths in countries where a minority have promoted his claims — Wakefield is spreading fear and misinformation again.
And the anti-vaxxers are proving alarmingly successful. It has been estimated that around 60 million people subscribe to anti-vaxx propaganda. It is conceivable therefore that these science-deniers could seriously undermine efforts to tackle the current pandemic effectively.
Glucosamine is currently one of the most popular of all dietary supplements. It is marketed as a treatment for arthritis, and there is some evidence that it is moderately helpful for this indication. But evidence had been accumulating to suggest that glucosamine might have other effects as well. The latest analysis evaluated the associations of regular glucosamine use with all-cause and cause-specific mortality in a large prospective cohort.
This population-based prospective cohort study included 495 077 women and men from the UK Biobank study. Participants were recruited from 2006 to 2010 and were followed up through 2018. The investigators evaluated all-cause mortality and mortality due to cardiovascular disease (CVD), cancer, respiratory and digestive disease. Hazard ratios (HRs) and 95% CIs for all-cause and cause-specific mortality were calculated using Cox proportional hazards models with adjustment for potential confounding variables.
At baseline, 19.1% of the participants reported regular use of glucosamine supplements. During a median follow-up of 8.9 years (IQR 8.3-9.7 years), 19 882 all-cause deaths were recorded, including 3802 CVD deaths, 8090 cancer deaths, 3380 respiratory disease deaths and 1061 digestive disease deaths. In multivariable adjusted analyses, the HRs associated with glucosamine use were 0.85 (95% CI 0.82 to 0.89) for all-cause mortality, 0.82 (95% CI 0.74 to 0.90) for CVD mortality, 0.94 (95% CI 0.88 to 0.99) for cancer mortality, 0.73 (95% CI 0.66 to 0.81) for respiratory mortality and 0.74 (95% CI 0.62 to 0.90) for digestive mortality. The inverse associations of glucosamine use with all-cause mortality seemed to be somewhat stronger among current than non-current smokers (p for interaction=0.00080).
The authors concluded that regular glucosamine supplementation was associated with lower mortality due to all causes, cancer, CVD, respiratory and digestive diseases.
Previous epidemiological investigations indicated that glucosamine use might play a role in prevention of cancer, cardiovascular disease and other diseases. This suggests that the finding is more than the result of a large ‘fishing expedition’ to which epidemiological studies are sadly prone. It we are indeed dealing with a true phenomenon, we should ask by what mechanism these remarkable outcomes might be achieved. It is well documented that glucosamine has powerful anti-inflammatory effects. Therefore it is conceivable that such anti-inflammatory mechanisms are the cause for the observed outcomes.
How do we prove or disprove the hypothesis that glucosamine reduces the mortality of a range of diseases? A reasonable starting point would be to consult the good old Hill criteria of causality:
(1) The strength of association is small to moderate – certainly not strong
(2) The consistency of the findings is quite remarkable; that is unless dozens of epidemiological studies that failed to yield and association were never published.
(3) The specificity of the association with diseases linked to inflammation is also impressive (with the caveat above).
(4) Temporality seems also not a problem, as far as I can see.
(5) Biological gradient needs further testing, I think.
(6) Plausibility is not a problem, since there is a possible mechanism that could explain the findings.
(7) The same applies to coherence.
(8) Experiment is needed, but it is far from easy to conduct clinical trials where mortality is an endpoint.
(9) Analogy is realised through the well-established concept of (cardiovascular) risk factors.
What does all this actually mean?
It means, I think, that glucosamine could well have clinical effects that go far beyond easing the pain of arthritis. However, we cannot be sure. Once again, it boils down to the need of robust clinical trial data. The subject certainly seems important enough to consider this option.
On his website, Phillip Hughes – D. Hom (Med), M.A.R.H, describes himself as follows:
In the early 1990’s my life was turned upside-down by a prolapsed disk in my back, putting me in traction in a hospital for 6 weeks! The doctor’s prognosis was poor, leaving me with little hope of full mobility, and no choice but to seek treatment elsewhere.
I decided on Homeopathy, and after treatment I experienced real change in my condition within a month, and was completely well within 3 months. I was so inspired by this I decided to study Homeopathy myself – and in 1994 I enrolled at the Hahnemann College of Homeopathy in London, qualifying in 1998.
After qualifying I set up my first clinic in Waterloo, Liverpool. I also became a senior lecturer at the Hahnemann College of Homeopathy, and founder of the Liverpool branch of the Hahnemann College.
I then moved my clinic to College Road Crosby, when I took up the role of secretary of Homeopathic Medical Association (since resigned). It was during this time that my wife Rosa found a lump in her breast, motivating us again to seek safer and alternative treatments, this time using Thermography. We now run Thermography and Homeopathic clinics side by side.
I had never heard of Mr Hughes until yesterday, when it was reported that he had treated a Sean Walsh, a young musician, for Hodgkin lymphoma that had initially been controlled with chemotherapy, but had later returned. Here is an excerpt from the sad story:
Sean was having scans at a clinic – Medical Thermal Imaging – run by a couple called Philip and Rosa Hughes. Philip Hughes, a homeopath, had previously told Sean’s parents he’d successfully treated Rosa for breast cancer. Dawn [Sean’s girlfriend] went along to Sean’s first appointment. “Phil was just talking all about how damaging chemotherapy is, you know, on the human body… saying, ‘I’ve had lots of people come to my clinic, but by the time I get them, they’re shot with all this chemotherapy, so I can’t help them … And then he was talking all about how you can change your diet, which can reverse cancer. He’d said that Rosa had developed breast cancer. She’d had a lump in her breast, and she decided not to do hospital treatment, and she was going to, you know, reverse the cancer herself. So obviously Sean’s listening to this thinking, ‘Well, if one person’s done it, and then I’m hearing other little stories off them, I can do this’. Sean’s scans did carry a disclaimer, stating that thermography does not see or diagnose cancer and recommending further clinical investigation. But the scan results seemed reassuring – and Sean was convinced his cancer had gone. ‘Medical Thermal Imaging’ describe their scans as “100% safe and radiation-free”.
To find out more about the service the Hughes were offering, a BBC reporter went to the clinic where Sean had his scans, posing as a patient who’d found a lump. They were seen by Rosa Hughes, who had provided scans for Sean. Rosa told our reporter that when she went to the breast clinic to have her lump investigated, she should have an ultrasound rather than a mammogram. This is a transcript of what she said: “Not a mammogram, because you’re going to get radiated, and it’s going to squash… and the amount of women that have had their tumours, the tumour burst, that spreads cancer.”
[The BBC] asked cancer specialist Prof Andrew Wardley, of Manchester’s Christie Hospital, to review the medical claims Rosa Hughes made to our reporter. “That’s preposterous. You don’t burst tumours, they are solid. You do squash the breast down to do a mammogram, it is unpleasant but it’s a short-term thing. You do not spread cancer by doing a mammogram, that’s a complete fallacy.” Rosa and Philip Hughes say they “utterly reject” the allegation that they gave Mr Walsh inappropriate advice. They added they had “consistently made clear” that thermography can only be used alongside other tests, such as MRIs or mammograms.
At first Sean believed he had cured his own cancer. But tragically Sean was wrong. Gradually his health declined, until he was rushed to hospital in Liverpool where medical staff found he had multiple tumours in his stomach and chest. He did eventually receive chemotherapy but it was too late.
Sean died in January 2019.
On Philip Hughes’ website, he advertises his services with the help of several testimonials from happy customers. Here is one of them:
In November 2000, I had an aggressive Sarcoma Tumour removed along with my left lung. Shortly after surgery I was referred to Weston Park Hospital, Sheffield for ‘follow up’ treatments where I was offered both chemotherapy and radiotherapy. At around the same time, I first visited Waterloo Homeopathic Clinic on a friends recommendation. After this initial introduction to Homeopathy I began ti educate myself about my condition and possible treatments. Consequently I considered chemotherapy to be a crude option and decided to refuse it. However, the frightening thought of this aggressive tumour returning encourages me to go ahead with a six week course of radiotherapy as a precaution alongside Homeopathic treatment. Accordingly this holistic approach resulted in my immune system being boosted by Homeopathy and my body prepared for this medical treatment. Leading up to the radiotherapy and during the six weeks of treatments, I took a rang of Homeopathic remedies. Radium Brom, in my opinion, was undoubtedly the input that enabled me to go through an intense course of treatment daily and continue my healthy recovery. I didn’t miss a days work and finished a half marathon only three weeks after completing the radiotherapy. I have since remained in good health and all checks been clear.
I have said it often, but it seems I have to say it again: the homeopathic remedy might be harmless, but the homeopath isn’t!
PS
The BBC documentary provides many more details about Sean and another of Mr Hughes’ patients. It also shows some rare footage from the inside of the Gerson clinic in Mexico where Sean went for a while. Very sad but well worth watching!!!
Anyone who has followed the comments’ section of this blog knows that science communicators don’t always have it easy. In fact, they have to endure regular attacks. Now, this phenomenon has (as far as I know, for the first time) been investigated systematically.
The objective in this survey was to establish a taxonomy of common negative experiences encountered by those communicating medical science, and suggest guidelines so that they may be circumvented. A total of 142 prominent medical science communicators (defined as having >1000 Twitter followers and experience communicating medical science on social and traditional media platforms) were invited to take part in the survey. One hundred and one responses could be analysed.
The results show that:
- 92% of the participants has experienced abusive behaviour (91.9%), including persistent harassment (69.3%) and physical violence and intimidation (5.9%).
- 39% had received vexatious complaints to their employers, professional bodies or legal intimidation.
- 62% reported negative mental health sequelae due to public outreach, including depression, anxiety and stress.
- 20% had been obligated to seek police advice or legal counsel due to actions associated with their outreach work.
- the majority targeted with vexatious complaints felt supported by their employer/professional body and 32% reported neutral, poor or non-existent support.
Here is a selection of the responses from the participants:
- Accusations—including by one Senator—that [we are] uncaring, dismissive, neglectful, arrogant, or paid by pharma companies when advocating for vaccines. (Misrepresentation)
- I find my expertise is questioned—this often seems to be when men find it difficult to accept women with intelligence and qualifications. Sexist insults are a typical go-to response. (Discreditation)
- The worst one that hurt me professionally and personally was that activists gathered my emails using [Freedom of Information Requests] and handed chosen packets of them with a story to different reporters. (Misrepresentation/Discreditation/Dubious Amplification)
- Persistent negative comments on twitter; usually it doesn’t last long but it can feel very intense while it’s happening! (Intimidation)
- I have been served with a SLAPP lawsuit in order to silence my outreach work. Frequently receive harassing emails, malicious comments made on blog. (Malicious Complaints)
- Social media co-ordinated intimidation, implied threats of legal action (for defamation). Mocking, undermining, condescension and attacks for being an industry shill, although. I am just a patient advocate. Being called a liar, that I never had cancer, that I deserved cancer due to my attitude, that I have been mutilated by conventional medical treatment, and that I am no longer a woman (having had mastectomy for cancer). That my cancer will return and I deserve that. (Dubious Amplification/Misrepresentation/Discreditation)
- I have had anti-vaccine organizations and individuals attempt to prevent my public appearances and have been the subject of numerous online smear campaigns accusing me of being ‘a shill for Big Pharma’ etc. (Discreditation/Dubious Amplification)
- Those who attack me very frequently try to do it by targeting me at my job, sending bogus complaints to my bosses and the university. From my observation, that is the go-to attack, the first thing these groups do. (Malicious Complaints)
- I had to contact the police, who visited the person who was harassing me. I also involved social services. We bought a CCTV to monitor our front door after a strange envelope was hand delivered. The person involved has targeted several people before and continues to target individuals who advocate vaccination. (Intimidation)
- Abuse and accusations of corruption are the most common adverse reaction I get. Sometimes a particular group petition one’s employer and try to create trouble for them. I have been lucky in the past when this happened to have had supportive universities who appreciate my outreach work. I have in the past had slightly unhinged individuals writing rambling, implicitly threatening letters to my office which ultimately required police intervention. (Discreditation/Malicious Complaints/Intimidation)
- The worst are gendered insults (being called a cunt, etc.) and rape/death threats. I have had one empty legal threat that was widely publicized. (Intimidation/Malicious Complaints)
- Regular threats to sue for defamation. (Malicious Complaints)
- Attempts to get me fired, public records act requests for emails, verbal attacks on my children. (Malicious Complaints, Intimidation)
- One of the most unpleasant things is that certain people or groupings will use very underhanded tactics to respond to perceived criticism. If they can’t refute the science, it isn’t uncommon for them to go after you personally, alleging all manner of things to anyone who’ll listen; that you’re incompetent, or unethical, or perverted. It seems they throw things wildly to see what sticks, but it can be extraordinarily unpleasant to endure. (Dubious Amplification/Discreditation)
- My main concern has been obsessed individuals who declare their enmity and seem to be unconstrained by civil norms. (Intimidation)
- Homeopathy advocates looked up my LinkedIn profile and called my employer to complain about my comments on the radio. My employer did not support me and I ended up having to stop the activity I had been planning. (Misrepresentation/Malicious Complaints)
- Being threatened with physical violence. (Intimidation)
- A delusional supporter of [an individual] I wrote about accused me and my lawyer of stalking him and killing his in-laws. He sent accusing emails to the faculty of my school and all the police departments in my state. [They] also accused me of being a terrorist and complained about me to the FBIs Terrorism Joint Task Force. That gave me many nervous, sleepless nights. (Discreditation/Malicious Complaints)
- Death threats received, employer unhelpful, sorted myself. (Intimidation)
- I haven’t experienced many negative encounters because I would say I am only lightly involved in public engagement. However the reason I don’t become more heavily involved in this area is fear of this kind of abuse and vexatious complaints to my employer or regulatory body. (Malicious Complaints)
The authors concluded as follows: The question of how we best communicate health science in the modern era is an area where more research is urgently required, especially on the role of social media, and optimum ways physicians, researchers and other public-facing figures can promote good medical science and mitigate falsehoods. The suggestions herein ought to be taken as a starting point, with discussion evolving as improved evidence materialises. There are wider problems implicit in all this that those communicating science cannot tackle in isolation; social media regulation particularly is a serious issue, both in regard to the spreading of misinformation/disinformation, and with respect to procedures preventing the potential weaponisation of social media platforms. Social media platforms must ultimately be made answerable to regulatory oversight, just as every other important aspect of life is; claims of innocence are unconvincing when their business model is so clearly dependent on advertising engagement at the cost of lives. The problem of poor reporting and false balance in conventional media outlets also must be considered, and there is significant scope for scientists and doctors to contribute to policy in these areas. There is ample evidence that physicians and scientists have an important role to play in combatting health disinformation, as has recently been argued by one of the authors in relation to vaccination for British Medical Journal opinion. But equally, it is crucial that those engaging in this vital work have the requisite support from their institutions, so that deleterious consequences of laudable outreach work might be circumvented. It is increasingly clear that disinformation about medicine and illness has become ubiquitous, with severe consequences for both our collective health and public understanding of medical science. Scientists and physicians must be at the vanguard of the pushback against these dangerous falsehoods—our societal well-being depends on it.
_______________________________________
This is an important paper, in my view. It is well worth reading in full.
I know many scientists who will no longer engage in science communication (other than publishing their papers and attending conferences) because they had one or two bad experiences. I certainly had hundreds of bad (some very bad) experiences, but I have taken the opposite decision.
Thus I started this blog, authored several books aimed at the consumer, give public lectures, etc. I have done this for many years despite the lack of support from my university and sometimes despite the opposite of support from my peers.
Why?
Why do I work tirelessly trying to inform consumers about so-called alternative medicine (SCAM)?
Because, in view of the plethora of (often dangerous) misinformation, it is hugely important to get the word out to the men and women in the street. I pity the ones who regularly allege that I do all this because of the money I earn from such activity (on the whole, it costs me money). In fact, I do what I do because I hope it might
- stimulate rational thought,
- help people to make wise therapeutic decisions,
- make a small contribution to public health,
- and perhaps occasionally even save a life.
And the threats which I continue to receive merely indicate that I might be doing this job well, and prove how important the task really is.
There has been plenty of research into the factors that determine the usage of so-called alternative medicine (SCAM). Yet, so far, not a single truly powerful predictor has been identified. The aim of this study was therefore to identify the most important predictors of the use and approval of CAM. The researchers performed a canonical correlation analysis on all 3480 records from the 2012 German General Social Survey (ALLBUS) with the lifetime use and opinion of SCAM as the dependent variables.
 Approval of paranormal practices such as fortune-telling, dowsing or spiritualism explained 32% of the variance in the dependent canonical variate “approval of SCAM”, while sociodemographic variables explained only 2%. Experience with paranormal practices explained 17% of the variance in the dependent canonical variate “experience with SCAM”, and sociodemographic variables explained 10% of the variance. Traditional religiosity, attitudes towards science and post-materialist values showed no relevant correlations with the dependent canonical variates.
Approval of paranormal practices such as fortune-telling, dowsing or spiritualism explained 32% of the variance in the dependent canonical variate “approval of SCAM”, while sociodemographic variables explained only 2%. Experience with paranormal practices explained 17% of the variance in the dependent canonical variate “experience with SCAM”, and sociodemographic variables explained 10% of the variance. Traditional religiosity, attitudes towards science and post-materialist values showed no relevant correlations with the dependent canonical variates.
The authors concluded that paranormal beliefs and related measures are the most important known predictors of the use and approval of SCAM. Experience with paranormal practices not only indicates paranormal beliefs but also explains experience with SCAM that cannot be explained by approval of SCAM. Female gender and higher socioeconomic status predict experience with SCAM without predicting approval of SCAM, but their influence should not be overstated.
Let’s not worry for the moment about the fact that most of the methods employed here to quantify the variables in question were not adequately validated. Let’s instead just assume that the reported findings are reliable and real. In this case, we must ask what do these correlations mean?
The authors seem to think that their results are quite extraordinary and require elaborate explanations. I find the findings utterly unsurprising and think they are almost self-explanatory: SCAM use/approval and the belief in the paranormal are linked because, to a very large degree, SCAM is part of the paranormal. The two are associated via a common denominator: lack of rationality and critical thinking.
George Lakhovsky, a Russian-born scientist, believed to have found out that every cell of the human body has its own frequency. Healthy cells emit a frequency radiation, he claimed, and whenever a part of the body gets damaged, inflamed or ill, the resonance of those cells become less intense. When pathogens, bacteria, microbes take over, they disrupt the healthy cells with their harmful frequency, Lakhovsky thought.
Based on these notions, Lakhovsky constructed a device capable of generating a field of frequencies in a very broad spectrum. He argued that, if one would place a sick person or an affected body part in this frequency spectrum, those diseased cells would recognize their own frequency, tune in and would start resonating in their own, healthy frequency again. Thus the illness would disappear, Lakhovsky thought.
He felt it should be possible to halt and even cure degenerative diseases like cancer in this way. After a long time of experimenting unsuccessfully, he called Nicola Tesla for help. Tesla had the blueprints for the oscillator machine ready for use. Their multi-wave oscillator was said to activate healing processes and cured most cases of cancer, leukaemia, osteoporosis etc.
An important part of Lakhovsky’s work took place in 1920-1930. In France, Italy, England and Germany multiple of Lakhovsky’s machines were operating. But then they slowly started disappearing again. Many people said the reason for this was that the quick results provided by the machines made the hospitals unnecessary and no profits could be made by them.
The Second World War put an end to much of Lakhovsky’s work. While visiting the US, Lakhovsky was struck by a car and died under mysterious circumstances aged 72.
________________________________________
Is this intriguing story the script of a bizarre film?
No, it is a true – well, partly true – story which I have taken from this article by a therapist who, like many others, uses Lakhovsky’s oscillator for treating patients (and sells potions, some of which cost well over Euro 1 000!). Another article by a practitioner offering this treatment claims that the oscillator is effective for the following indications:
- vitalising cells,
- activation of the body’s own healing powers,
- anti-ageing,
- wellness,
- improving general well-being,
- pain reduction,
- detox,
- rejuvenation of skin,
- improvement of visual aspect of the skin.
The article further assures us that the treatment is totally free of side-effects and can be used as an adjunctive therapy for almost any disease.
Yet another website advertises the therapy as follows: Have you lost a loved one to cancer? Georges Lakhovsky had a 98% success rate in treating fatal cancers over an 11-year period. Today we celebrate a 50% five-year survival rate.
And this is what Wikipedia tells us about the Lakhovsky oscillator (depicted in the photo above, together with its inventor): The main circuit basically consists of concentric rings forming electrical dipole antennas having capacitive gaps opposing each other by 180° (called Lakhovsky antennas). The circuit is fed with high voltage, high frequency, impulses from a generator, usually a Tesla coil. If set up correctly, the unit is supposed to create a broad band frequency spectrum of low amplitude, consisting of much more substantially lower and higher frequencies, from 1 Hz to 300 GHz, than those of the exciting generator, usually several 100 kHz to a few MHz from a Tesla transformer or several kilohertz from an induction coil. But the power of this broad band noise spectrum is very low. In order to create more harmonics and sub-harmonics, an additional spark gap on the secondary side has been found in some devices, being mounted directly on the antenna, or being mounted in parallel to the secondary coil…
In an attempt to find out whether the machine works, I have searched for published, peer-reviewed clinical evidence on the Lakhovsky oscillator. I was unable to find any. If any of my readers are aware of any evidence, please let me know.
The Society of Homeopaths (SoH) is the UK’s professional organisation of ‘lay-homeopaths’, therapists who treat patients without having studied medicine. They prefer the term ‘professional homeopathy’, but there is little professional about them, it seems. The SoH has a long track record of endangering public health by promoting anti-vaxx nonsense.
A few months ago, it was reported that Linda Wicks, chair of the Society of Homeopaths (S0H), has shared a series of petitions claiming that childhood immunisations are unsafe. Mrs Wicks also posted a petition supporting Andrew Wakefield, the disgraced former doctor who falsely linked the MMR vaccine to autism claiming that the scientific establishment’s rejection of his flawed research was ‘the greatest lie ever told’.
In 2018, I pointed out that the SoH was violating its own code of ethics. At the time, two new members were appointed to the Society’s Public Affairs (PAC) and Professional Standards (PSC) committees, and both were promoting the deeply anti-vaxx CEASE therapy.
![]()
Today, THE TELEGRAPH reports that Sue Pilkington, the SoH’s ‘Head of Standards’, has been promoting anti-vaxx propaganda online. On April 14, she posted anti-vaxx content made by the ‘Children’s Health Defense’ – an organisation accused by NBC News last year as being one of the largest global creators of spreading misinformation’. The page advised that any new vaccine could trigger “lethal” immune reactions.
In a separate post on Facebook, Pilkington shared a post that describes vaccines as “poison” – alongside medical advice declaring that no child should be vaccinated, if any member of their family has a skin disorder. Pilkington also tried to contact Health Secretary Matt Hancock, attempting to share with him a video of content from an American comedian claiming that it’s ‘realistic’ for vaccines to cause autism.
As though this were not enough nonsense, Pilkington also promotes homeopathy as a solution to the current epidemic. On her homeopathy business website, she has section on coronavirus which states the following: “The current primary homeopathic remedy advised for Coronavirus (2019-nCoV) symptoms is Gelsemium with a possible following remedy of Eupatorium Perforatum, Bryonia or Belladonna depending on how the symptoms progress”. Other homeopathic remedies are in common use for people with influenza and pneumonia, according to Pilkington, these do not “prevent viruses” but may “reduce the severity and length of illness”. She also claims that homeopathy has a “great track record of success in epidemics” – referencing both the Spanish influenza pandemic and the bird flu pandemic.
“In our opinion, the Professional Standards Authority (PSA) has a simple choice to make: remove the SoH and their uninformed vaccination paranoia from the register, or continue to allow homeopaths to make these dangerous claims with the tacit approval of the PSA.” said Michael Marshall, projector director of the Good Thinking Society.
A government health spokesperson was quoted in today’s TELEGRAPH article stating this: “Vaccine misinformation in any form – book, film, website or otherwise – is completely unacceptable.” The spokesperson added that NICE does not recommend homeopathy for the treatment of any health condition and noted that vaccines “save lives and are a foundation of public health.”
A reader of this blog reminded me of the fact that I have so far not written anything about VAT (thanks Kathryn) – no, not ‘value added tax’ but Vibroacoustic Sound Therapy. This so-called alternative therapy (SCAM) uses sound and vibrations and is promoted mainly for:
- reducing stress,
- relieving pain,
- improving sleep,
- ‘restoring balance’ (bank balance of the therapist?),
- and enhancing the quality of life.
The VAT frequencies range between 30Hz and 120Hz and are applied directly to the body through a treatment table topped with a water-filled mattress. If you go on the Internet, you will find that there are lots of devices you can buy, if you want to do the therapy at home.
Like so many other SCAMs, VAT is claimed to work with resonant frequency whereby our cells copy vibrations they are exposed to. VAT is said to introduce the healthy vibration of cells into the body. This results in a healthy resonant response in our cells, VAT-proponents claim. Over 100 customized frequencies can be employed to address specific health problems.
Yes, you are right: this is about as genuine as a £4 note.
Those practitioners offering VAT sessions claim that the best results occur with cumulative sessions for between 10 – 12 weeks and recommend a minimum treatment schedule of 8 weeks for the majority of cases, either once or twice per week. In view of the fact that these would-be healthcare professionals want to make a living, this seems almost modest, in my view. But, as they are keen to point out, more chronic conditions require 2-3 times per week.
Any evidence?
I found plenty of statements arguing that VAT is solidly evidence-based. However, when I searched for it, I failed to locate anything other than uncontrolled studies, pilot studies and promotional articles of VAT. I admit that I did not spend much time looking (it somehow did not seem worth the effort); it is therefore possible that I missed the definitive RCT of VAT. If someone knows of a piece of conclusive evidence, I’d be most thankful to learn about it.
Under the heading ‘Who should not receive vibroacoustic therapy?’ one VAT practitioner listed several contra-indications for VAT:
• Individuals with Pacemakers
• People with very low blood pressure
• People with a DVT, bleeding disorder, or recent surgery
• Individuals who have had a recent psychotic episode
To this list, I would urgently add this: individuals who are capable of critical thinking!!!
I was surprised to see a paper entitled ‘Yogurt Intake Reduces All-Cause and Cardiovascular Disease Mortality‘ in the current issue of the Chinese Journal of Integrative Medicine. My surprise turned into disbelief when I read the abstract. Here it is in its unabbreviated beauty:
Objective
To assess the relationship between yogurt intake and mortality risk from prospective cohort studies.
Methods
The PubMed, EMBASE, and Web of Science databases were searched for all records related to yogurt intake and mortality risk [all-cause or cardiovascular disease (CVD) or cancer mortality] before October 1, 2018. The Newcastle-Ottawa Quality Scale was used to estimate the quality of all eligible articles. The results of the highest and lowest categories of yogurt intake in each study were collected and the effect size was pooled using a random effects model. The dose-response analysis was calculated using the generalized least squares trend estimation model.
Results
Eight eligible cohort studies were included in this meta-analysis. There were 235,676 participants in the 8 studies, and the number of deaths was 14,831. Compared with the lowest category, the highest category of yogurt intake was not significantly related with all-cause mortality [hazard ratio (HR)=0.93; 95% confidence interval (CI): 0.85, 1.01], CVD mortality (HR=0.92; 95% CI: 0.81, 1.03) and cancer mortality (HR=0.97; 95% CI: 0.83, 1.12). These studies were homogenous, since the homogeneity test showed that I2 was 28.7%, 15.1% and 11.8%, respectively. However, yogurt intake ⩾200 g/d was significantly associated with a lower all-cause mortality (HR=0.88; 95% CI: 0.80, 0.96) and CVD mortality (HR=0.87; 95% CI: 0.77, 0.99) in the subgroup analysis. The dose-response analysis showed that yogurt intake of 200 g/d was inversely associated with all-cause mortality (P=0.041, HR=0.95, 95% CI: 0.92, 1.00) and CVD mortality (P=0.009, HR=0.92, 95% CI: 0.86, 0.98), and all of which were linear relationship (P>0.05).
Conclusions
This review provided the evidence regarding yogurt intake can reduce all-cause and CVD mortality. Although some positive findings were identified, more high-quality cohort studies and randomized controlled trials are warranted on a possible protective effect of yoghurt on health.
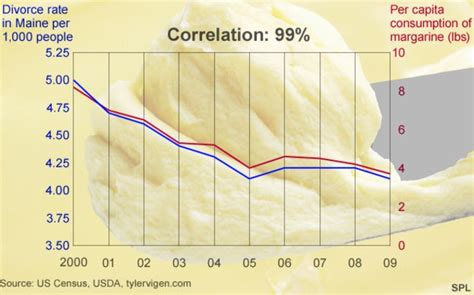
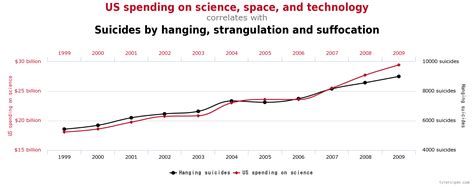

As the above three graphs indicate (and as researchers learn in their first lesson of statistics),
CORRELATION IS NOT CAUSATION.
We all know that, of course – except those of us who work in the so-called alternative medicine (SCAM), it seems – and except the editors of Chinese Journal of Integrative Medicine or the people who do the peer-reviewing for this publication. How else would we explain that a conclusion such as yogurt intake can reduce all-cause and CVD mortality can get published (not to mention the title of the paper)?
But what is the explanation of the intriguing association discovered by the authors of this paper? As far as I can see, there are several possibilities:
- The investigators could be correct, and the link could indeed be causal (in this case, they need to prove it).
- The finding could be coincidental, due to random noise (there are hundreds of epidemiological studies, and they tend to report mainly positive associations [big fishing expeditions really]; thus, it is conceivable that 8 of them found an association where in truth none exists).
- It could be that people who eat a yoghurt tend to not eat a ‘full English’ for breakfast, thus avoiding the harm of unhealthy nutrition)
- Similarly, it might be that yoghurt consumers care more about their health in general (including exercise, body weight, smoking, etc.) than those who shun yoghurt.
And how do we decide which explanation applies? The answer is simple: by doing proper research and drawing appropriate conclusions from it.
Perhaps something like this?
Background: Although a link between regular yogurt consumption and mortality appears plausible, data are sparse and have yielded inconsistent results.
Objectives: We examined the association between regular yogurt consumption and risk of all-cause and cause-specific mortality among US women and men.
Methods: A total of 82,348 women in the Nurses’ Health Study and 40,278 men in the Health Professionals Follow-Up Study without a history of cardiovascular disease (CVD) and cancer in 1980 (women) or 1986 (men) were followed up until 2012. Yogurt consumption was assessed by updated validated FFQs.
Results: During 3,354,957 person-years of follow-up, 20,831 women and 12,397 men died. Compared with no yogurt consumption, the multivariable-adjusted HRs (95% CIs) of mortality were 0.89 (0.86, 0.93), 0.85 (0.81, 0.89), 0.88 (0.84, 0.91), and 0.91 (0.85, 0.98) for ≤1-3 servings/mo, 1 serving/wk, 2-4 servings/wk, and >4 servings/wk in women (P-trend = 0.34), respectively. For men, the corresponding HRs (95% CIs) were 0.99 (0.94, 1.03), 0.98 (0.91, 1.05), 1.04 (0.98, 1.10), and 1.05 (0.95, 1.16), respectively. We further noted inverse associations for cancer mortality (multivariable-adjusted HR comparing extreme categories: 0.87; 95% CI: 0.78, 0.98; P-trend = 0.04) and CVD mortality (HR: 0.92; 95% CI: 0.79, 1.08; P-trend = 0.41) in women, although the latter was attenuated in the multivariable-adjusted model. Replacement of 1 serving/d of yogurt with 1 serving/d of nuts (women and men) or whole grains (women) was associated with a lower risk of all-cause mortality, whereas replacement of yogurt with red meat, processed meat (women and men), and milk or other dairy foods (women) was associated with a greater mortality.
Conclusions: In our study, regular yogurt consumption was related to lower mortality risk among women. Given that no clear dose-response relation was apparent, this result must be interpreted with caution.
_________________________
I rest my case.