risk
During the coronavirus disease 2019 pandemic, Ayurvedic herbal supplements and homeopathic remedies were promoted as immune boosters (IBs) and disease-preventive agents. This happened in most parts of the world but nowhere more intensely than in India.
The present study examined the clinical outcomes among patients with chronic liver disease who presented with complications of portal hypertension or liver dysfunction temporally associated with the use of IBs in the absence of other competing causes. This Indian single-center retrospective observational cohort study included patients with chronic liver disease admitted for the evaluation and management of jaundice, ascites, or hepatic encephalopathy temporally associated with the consumption of IBs and followed up for 180 days. Chemical analysis was performed on the retrieved IBs.
From April 2020 to May 2021, 1022 patients with cirrhosis were screened, and 178 (19.8%) were found to have consumed complementary and alternative medicines. Nineteen patients with cirrhosis (10.7%), jaundice, ascites, hepatic encephalopathy, or their combination related to IBs use were included. The patients were predominantly male (89.5%). At admission, 14 (73.75%) patients had jaundice, 9 (47.4%) had ascites, 2 (10.5%) presented with acute kidney injury, and 1 (5.3%) had overt encephalopathy. Eight patients (42.1%) died at the end of the follow-up period. Hepatic necrosis and portal-based neutrophilic inflammation were the predominant features of liver biopsies.
Ten samples of IBs, including locally made ashwagandha powder, giloy juice, Indian gooseberry extracts, pure giloy tablets, multiherbal immune-boosting powder, other multiherbal tablets, and the homeopathic remedy, Arsenicum album 30C, were retrieved from our study patients. Samples were analyzed for potential hepatotoxic prescription drugs, known hepatotoxic adulterants, pesticides, and insecticides, which were not present in any of the samples. Detectable levels of arsenic (40%), lead (60%), and mercury (60%) were found in the samples analyzed. A host of other plant-derived compounds, industrial solvents, chemicals, and anticoagulants was identified using GC–MS/MS. These include glycosides, terpenoids, phytosteroids, and sterols, such as sitosterol, lupeol, trilinolein, hydroxy menthol, methoxyphenol, butyl alcohol, and coumaran derivatives.
The authors concluded that Ayurvedic and Homeopathic supplements sold as IBs potentially cause the worsening of preexisting liver disease. Responsible dissemination of scientifically validated, evidence-based medical health information from regulatory bodies and media may help ameliorate this modifiable liver health burden.
The authors comment that Ayurvedic herbal supplements and homeopathic remedies sold as IBs, potentially induce idiosyncratic liver injury in patients with preexisting liver disease. Using such untested advertised products can lead to the worsening of CLD in the form of liver failure or portal hypertension events, which are associated with a high risk of mortality compared to those with severe AH-related liver decompensation in the absence of timely liver transplantation. Severe mixed portal inflammation and varying levels of hepatic necrosis are common findings on liver histopathology in IB-related liver injury. Health regulatory authorities and print and visual media must ensure the dissemination of responsible and factual scientific evidence-based information on herbal and homeopathic “immune boosters” and health supplements to the public, specifically to the at-risk patient population.
Research by the Milner Center for Evolution at the University of Bath, U.K., along with colleagues at the Universities of Oxford and Aberdeen, found that trust in scientists has hugely increased since the COVID-19 pandemic. The study also found that people were more likely to take the COVID-19 vaccine if their trust in the science had increased.
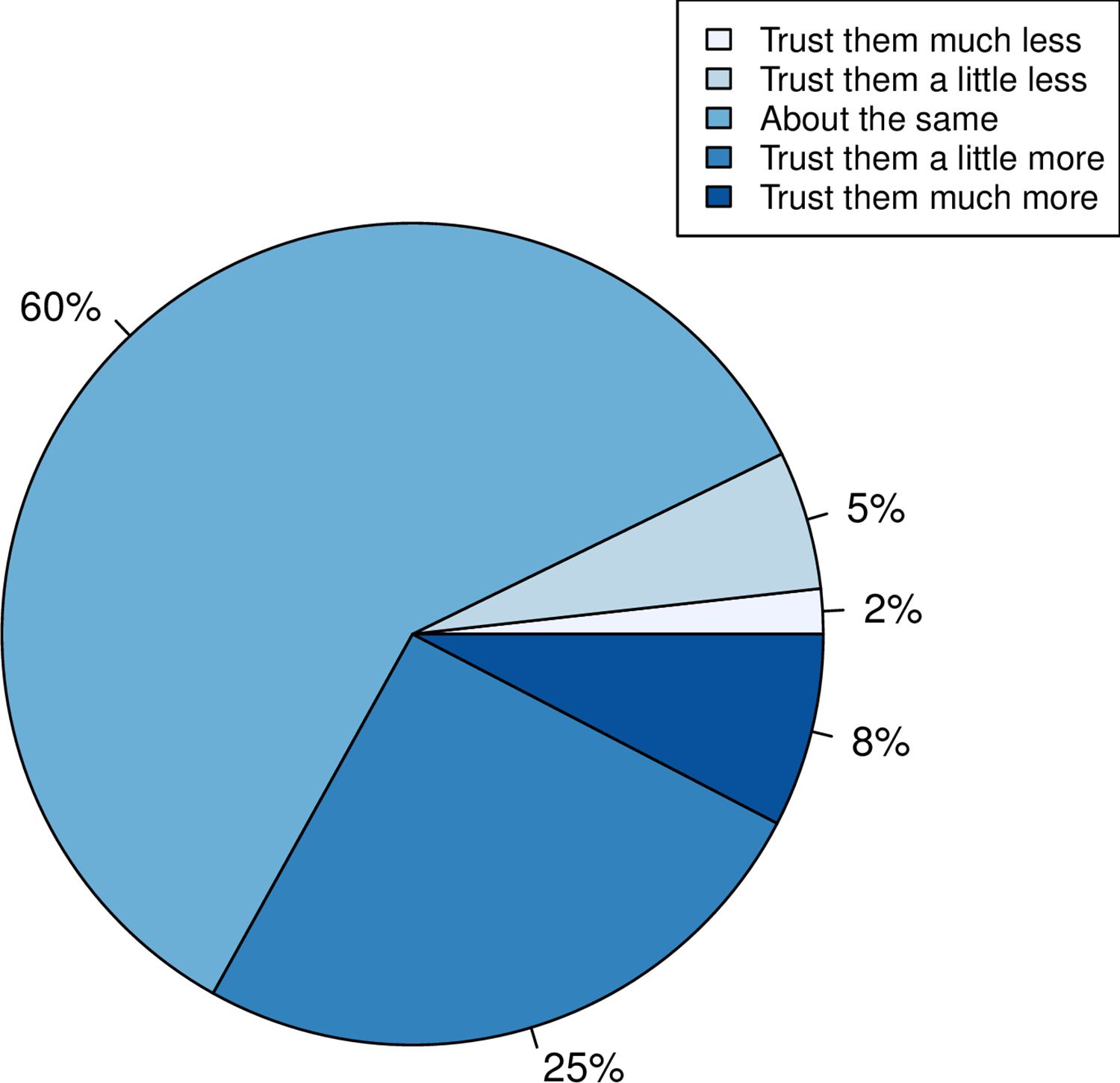
Using data from a survey of more than 2,000 U.K. adults commissioned by the Genetics Society, the team asked individuals whether their trust in scientists had gone up, down, or stayed the same.
- A third of people reported that their trust in scientists had gone up.
- When Pfizer, a company that made COVID-19 vaccines, was used as an example of the pharma industry, more people reported a positive response than when GlaxoSmithKline, a company not associated with the COVID-19 vaccine, was mentioned.
- The researchers also found that people who reported holding a negative view of science before the pandemic had become even more negative.
- People reporting increased trust were most likely to take the COVID-19 vaccine.
- Those preferring not to do so reported a decline in trust.
This is an interesting study with relevance to many discussions we had on this blog. I recommend reading it in full. Here are the abstract and link to the paper:
While attempts to promote acceptance of well-evidenced science have historically focused on increasing scientific knowledge, it is now thought that for acceptance of science, trust in, rather than simply knowledge of, science is foundational. Here we employ the COVID-19 pandemic as a natural experiment on trust modulation as it has enabled unprecedented exposure of science. We ask whether trust in science has on the average altered, whether trust has changed the same way for all and, if people have responded differently, what predicts these differences? We 1) categorize the nature of self-reported change in trust in “scientists” in a random sample of over 2000 UK adults after the introduction of the first COVID vaccines, 2) ask whether any reported change is likely to be real through consideration of both a negative control and through experiment, and 3) address what predicts change in trust considering sex, educational attainment, religiosity, political attitude, age and pre-pandemic reported trust. We find that many more (33%) report increased trust towards “scientists” than report decreased trust (7%), effects of this magnitude not being seen in negative controls. Only age and prior degree of trust predict change in trust, the older population increasing trust more. The prior degree of trust effect is such that those who say they did not trust science prior to the pandemic are more likely to report becoming less trusting, indicative of both trust polarization and a backfire effect. Since change in trust is predictive of willingness to have a COVID-19 vaccine, it is likely that these changes have public health consequences.
The Lightning Process (LP) is a therapy for ME based on ideas from osteopathy, life coaching, and neuro-linguistic programming. LP is claimed to work by teaching people to use their brains to “stimulate health-promoting neural pathways”. One young patient once described it as follows: “Whenever you get a negative thought, emotional symptom, you are supposed to turn on one side and with your arm movements in a kind if stop motion, just say STOP very firmly and that is supposed to cut off the adrenaline response.”
Allegedly, the LP teaches individuals to recognize when they are stimulating or triggering unhelpful physiological responses and to avoid these, using a set of standardized questions, new language patterns, and physical movements with the aim of improving a more appropriate response to situations. The LP involves three group sessions on consecutive days where participants are taught theories and skills, which are then practiced through simple steps, posture, and coaching.
Does LP work?
Some think it does, particularly in Norway, it seems.
Proponents of the ‘LP’ in Norway claim that 90% of all ME patients get better after trying it. However, such claims seem to be more than questionable.
- In the Norwegian ME association’s user survey from 2012 with 1,096 participants, 164 ME patients stated that they had tried LP. 21% of these patients experienced improvement or great improvement and 48% got worse or much worse.
- In Norway’s National Research Center in Complementary and Alternative Medicine, NAFKAM’s survey from 2015 amongst 76 patients 8 had a positive effect and 5 got worse or much worse.
- A survey by the Norwegian research foundation, published in the journal Psykologisk, with 660 participants, showed that 62 patients had tried LP, and 5 were very or fairly satisfied with the results.
Such figures seem to reflect the natural history of the condition and may be totally unrelated to LP.
The LP instructors’ claims of a 90% positive effect are used for marketing and for lobbying. Their aim is to influence politicians, health authorities, and welfare and disability benefits authorities. They want to get the LP course approved as part of the public health service.
The company ‘Aktiv Prosess’ was started by LP instructors Live Landmark and Vibeke C. Hammer. In an article in the Norwegian medical journal Tidsskriftet in 2016, Landmark describes her own customer satisfaction survey from 2008 as «generating a hypothesis». Landmark has also written a book about her personal story and holds lectures for medical students, medical doctors, and nurses. Now she is trying to run a clinical trial which, many experts believe, is far from rigorous and set up to produce a positive result.
Positive experiences with LP have received massive media coverage for 15 years. Anecdotes are recycled in the media and give the impression of being a higher number than reality. We rarely hear about those who deteriorated: https://lp-fortellinger.no/ (English language link here).
The NICE guidelines for ME/CFS specifically (and in my view rightly) warn against offering LP to ME patients.
It has been reported that the PLASTIC SURGERY INSTITUTE OF ·UTAH, INC.; MICHAEL KIRK MOORE JR.; KARI DEE BURGOYNE; KRISTIN JACKSON ANDERSEN; AND SANDRA FLORES, stand accused of running a scheme out of the Plastic Surgery Institute of Utah, Inc. to defraud the United States and the Centers for Disease Control and Prevention.
Dr. Michael Kirk Moore, Jr. and his co-defendants at the Plastic Surgery Institute of Utah have allegedly given falsified vaccine cards to people in exchange for their donating $50 to an unnamed organization, one which exists to “liberate the medical profession from government and industry conflicts of interest.” As part of the scheme, Moore and his co-defendants are accused of giving children saline injections so that they would believe they were really being vaccinated.
The co-defendants are Kari Dee Burgoyne, an office manager at the Plastic Surgery Institute of Utah; Sandra Flores, the office’s receptionist; and, strangest of all, a woman named Kristin Jackson Andersen, who according to the indictment is Moore’s neighbor. Andersen has posted copious and increasingly conspiratorial anti-vaccine content on Facebook and Instagram; Dr. Moore himself was a signatory on a letter expressing support for a group of COVID-skeptical doctors whose certification was under review by their respective medical boards. The letter expresses support for ivermectin, a bogus treatment for COVID.
According to the indictment, the Plastic Surgery Center of Utah was certified as a real vaccine provider and signed a standard agreement with the CDC, which among other things requires doctor’s offices not to “sell or seek reimbursement” for vaccines.
Prosecutors allege that, when people seeking falsified vaccine cards contacted the office, Burgoyne, the office manager, referred them to Andersen, Dr. Moore’s neighbor. Andersen, according to the indictment, would ask for the name of someone who’d referred them—it had to be someone who’d previously received a fraudulent vaccine card, per the indictment—then direct people to make a $50 donation to a charitable organization, referred to in the indictment only as “Organization 1.” Each vaccine card seeker was required to put an orange emoji in the memo line of their donation.
After making a donation to the unnamed charitable organization, prosecutors allege, Andersen would send a link to vaccine card seekers to enable them to make an appointment at the Plastic Surgery Institute. With adult patients, Moore would allegedly use a real COVID vaccine dose in a syringe, but squirt it down the drain. Flores, the office’s receptionist, gave an undercover agent a note, reading “with 18 & younger, we do a saline shot,” meaning that kids were injected with saline instead of a vaccine. Prosecutors allege the team thus disposed of at least 1,937 doses of COVID vaccines.
All four people are charged with conspiracy to defraud the United States; conspiracy to convert, sell, convey, and dispose of government property; and conversion, sale, conveyance, and disposal of government property and aiding and abetting.
Throughout the scheme, the group reported the names of all the vaccine seekers to the Utah Statewide Immunization Information System, indicating that the practice had administered 1,937 doses of COVID-19 vaccines, which included 391 pediatric doses. The value of all the doses totaled roughly $28,000. With the money from the $50 vaccination cards totaling nearly $97,000, the scheme was valued at nearly $125,000, federal prosecutors calculated.
“By allegedly falsifying vaccine cards and administering saline shots to children instead of COVID-19 vaccines, not only did this provider endanger the health and well-being of a vulnerable population, but also undermined public trust and the integrity of federal health care programs,” Curt Muller, special agent in charge with the Department of Health and Human Services for the Office of the Inspector General, said in a statement.
_________________________________
I am already baffled by anti-vax attitudes when they originate from practitioners of so-called alternative medicine (SCAM). When they come from real physicians and are followed by real actions, I am just speechless. As I stated many times before: studying medicine does unfortunately not protect you from recklessness, greed, or stupidity.
I have been informed by the publisher, that my book has been published yesterday. This is about two months earlier than it was announced on Amazon. It is in German – yes, I have started writing in German again. But not to worry, I translated the preface for you:
Anyone who falls ill in Germany and therefore needs professional assistance has the choice, either to consult a doctor or a non-medical practitioner (Heilpraktiker).
– The doctor has studied and is licensed to practice medicine; the Heilpraktiker is state-recognized and has passed an official medical examination.
– The doctor is usually in a hurry, while the Heilpraktiker takes his time and empathizes with his patient.
– The doctor usually prescribes a drug burdened with side effects, while the Heilpraktiker prefers the gentle methods of alternative medicine.
So who should the sick person turn to? Heilpraktiker or doctor? Many people are confused by the existence of these parallel medical worlds. Quite a few finally decide in favor of the supposedly natural, empathetic, time-tested medicine of the Heilpraktiker. The state recognition gives them the necessary confidence to be in good hands there. The far-reaching freedoms the Heilpraktiker has by law, as well as the coverage of costs by many health insurances, are conducive to further strengthening this trust. “We Heilpraktiker are recognized and respected in politics and society,” writes Elvira Bierbach self-confidently, the publisher of a standard textbook for Heilpraktiker.
The first consultation of our model patient with the Heilpraktiker of his choice is promising. The Heilpraktiker responds to the patient with understanding, usually takes a whole hour for the initial consultation, gives explanations that seem plausible, is determined to get to the root of the problem, promises to stimulate the patient’s self-healing powers naturally, and invokes a colossal body of experience. It almost seems as if our patient’s decision to consult a Heilpraktiker was correct.
However, I have quite significant reservations about this. Heilpraktiker are perhaps recognized in politics and society, but from a medical, scientific, or ethical perspective, they are highly problematic. In this book, I will show in detail and with facts why.
The claim of government recognition undoubtedly gives the appearance that Heilpraktiker are adequately trained and medically competent. In reality, there is no regulated training, and the competence is not high. The official medical examination, which all Heilpraktiker must pass is nothing more than a test to ensure that there is no danger to the general public. The ideas of many Heilpraktiker regarding the function of the human body are often in stark contradiction with the known facts. The majority of Heilpraktiker-typical diagnostics is pure nonsense. The conditions that they diagnose are often based on little more than naive wishful thinking. The treatments that Heilpraktiker use are either disproven or not proven to be effective.
There is no question in my mind that Heilpraktiker are a danger to anyone who is seriously ill. And even if Heilpraktiker do not cause obvious harm, they almost never offer what is optimally possible. In my opinion, patients have the right to receive the most effective treatment for their condition. Consumers should not be misled about health-related issues. Only those who are well-informed will make the right decisions about their health.
My book provides this information in plain language and without mincing words. It is intended to save you from a dangerous misconception of the Heilpraktiker profession. Medical parallel worlds with the radically divergent quality standard – doctor/Heilpraktiker – are not in the interest of the patient and are simply unacceptable for an enlightened society.
It has been reported that a well-known conservative activist, Kelly Canon, from Arlington, Texas, USA, has tragically died. She was famous for peddling COVID-19 vaccine misinformation. The complications caused by the virus—just a few weeks after attending a “symposium” against the vaccines – have killed her. 
“Another tragedy and loss for our Republican family. Our dear friend Kelly Canon lost her battle with pneumonia today. Kelly will be forever in our hearts as a loyal and beloved friend and Patriot. Gone way too soon We will keep her family in our prayers,” the Arlington Republican Club said in a statement.
Her death was said to be “from COVID-related pneumonia.” Canon had announced on Facebook in November that her employer had granted her a religious exemption for the COVID-19 vaccine. “No jabby-jabby for me! Praise GOD!” she wrote at the time.
Canon had been an outspoken critic of COVID-19 vaccine mandates and pandemic-related restrictions. In one of her final Facebook posts, Canon shared several links to speeches she attended at a “COVID symposium” in Burleson in early December devoted to dissuading people from getting the COVID-19 vaccines that are currently available. The event was organized by God Save Our Children, which bills itself as “a conservative group that is fighting against the use of experimental vaccines on our children.”
Canon had shared similar content on Twitter, where her most recent post was a YouTube video featuring claims that the coronavirus pandemic was “planned” in advance and part of a global conspiracy.
As news of her death spread Tuesday, pro-vaccine commentators flooded her Facebook page with cruel comments and mocking memes, while her supporters unironically praised her for being a “warrior for liberty” to the very end.
___________________________
A religious exemption?
What for heaven’s sake is that?
I feel sad for every death caused by COVID and its complications. If the death is caused by ignorance, it renders the sadness all the more profound.
So-called alternative medicine (SCAM) is widely used in Arabia. One of the commonly used methods is camel urine alone or mixed with camel milk. Camel urine is a liquid by-product of camel metabolism. Urine from camels has been used as prophetic medicine for centuries, being a part of ancient Bedouin practices. Camel urine comes out as a concentrated, viscous syrup because the kidneys and intestines of a camel are very efficient at reabsorbing water. 
Camel urine is consumed and used for treating numerous ailments. Some employ it as a treatment for hair loss, for instance. The camel urine from a virgin camel is priced at twenty dollars per liter, with herders saying that it has curative powers.
A recent paper offers more information:
Camel is one of the important livestock species which plays a major role in the pastoral mode of life by fulfilling basic demands of livelihood. Traditionally, camel urine has been used in the treatment of human diseases. With regard to the health benefits of drinking the urine of camels, it has been proven by modern scientific researches. Camel urine has an unusual and unique biochemical composition that contributes to medicinal values. The chemical composition of camel urine showed the presence of purine bases, hypoxanthine, sodium, potassium, creatinine, urea, uric acid, and phosphates. The nano-particles in the camel’s urine can be used to fight cancer. Camel urine has antimicrobial activity against pathogenic bacteria. Its chemical and organic constituents have also inhibitory properties against fungal growth, human platelets, and parasitic diseases mainly fasciollosis in calves. The healthy status of the liver can be restored through ingestion of diet and minerals in camel urine. Camel urine is used by the camel owners and Bedouins as medicine in different ways. The Bedouin in the Arab desert used to mix camel urine with milk. Recently; the WHO has warned against drinking camel urine due to the modern attempt to limit Outbreaks of Respiratory Syndrome (MRS) in the Middle East. There is no scientific dosage for camel urine to be applied as medicine for different diseases and the ways of camel urine formulation and utilization for the care of patients varies from country to country. Therefore, the purposes of the present review describe the biochemical composition of camel urine will be scientifically extracted and formulated as a therapy rather than drinking raw urine and people’s health impact.
Researchers from the Medical Oncology Department, Comprehensive Cancer Center, King Fahad Medical City, Riyadh, Saudi Arabia wanted to determine whether camel urine shows promise in the treatment of cancer. The aim of their study was to observe cancer patients who insisted on using camel urine and to devise some clinically relevant recommendations.
The authors observed 20 cancer patients (15 male, 5 female) from September 2020 to January 2022 who insisted on using camel urine. They documented the demographics of each patient, the method of administering camel urine, the reasons for refusing conventional treatment, the period of follow-up, and the outcome and side effects.
All the patients had radiological investigations before and after finishing treatment with camel urine. All patients used a combination of camel urine and milk, and treatment ranged from a few days up to 6 months. The average amount of urine/milk consumed was 60 ml/day. No clinical benefit was observed and two patients developed brucellosis. Eleven patients changed their minds and eventually accepted conventional antineoplastic treatments but 7 were too weak to receive further treatment and died from their disease.
The authors concluded that camel urine had no clinical benefits in cancer patients, and may even have caused zoonotic infection. The promotion of camel urine as a traditional medicine should be stopped because there is no scientific evidence to support it.
I fear that, yet again, ‘ancient wisdom’ turns out to be just ‘old bullshit’.
Lower respiratory tract infections (LRTIs) in early childhood are known to influence lung development and lifelong lung health, but their link to premature adult death from respiratory disease is unclear. This analysis aimed to estimate the association between early childhood LRTI and the risk and burden of premature adult mortality from respiratory disease.
This longitudinal observational cohort study used data collected prospectively by the Medical Research Council National Survey of Health and Development in a nationally representative cohort recruited at birth in March 1946, in England, Scotland, and Wales. It evaluated the association between LRTI during early childhood (age <2 years) and death from respiratory disease from age 26 through 73 years. Early childhood LRTI occurrence was reported by parents or guardians. Cause and date of death were obtained from the National Health Service Central Register. Hazard ratios (HRs) and population attributable risk associated with early childhood LRTI were estimated using competing risks Cox proportional hazards models, adjusted for childhood socioeconomic position, childhood home overcrowding, birthweight, sex, and smoking at age 20–25 years. The researchers compared mortality within the cohort studied with national mortality patterns and estimated corresponding excess deaths occurring nationally during the study period.
5362 participants were enrolled in March, 1946, and 4032 (75%) continued participating in the study at age 20–25 years. 443 participants with incomplete data on early childhood (368 [9%] of 4032), smoking (57 [1%]), or mortality (18 [<1%]) were excluded. 3589 participants aged 26 years (1840 [51%] male and 1749 [49%] female) were included in the survival analyses from 1972 onwards. The maximum follow-up time was 47·9 years. Among 3589 participants, 913 (25%) who had an LRTI during early childhood were at greater risk of dying from respiratory disease by age 73 years than those with no LRTI during early childhood (HR 1·93, 95% CI 1·10–3·37; p=0·021), after adjustment for childhood socioeconomic position, childhood home overcrowding, birthweight, sex, and adult smoking. This finding corresponded to a population attributable risk of 20·4% (95% CI 3·8–29·8) and 179 188 (95% CI 33 806–261 519) excess deaths across England and Wales between 1972 and 2019.
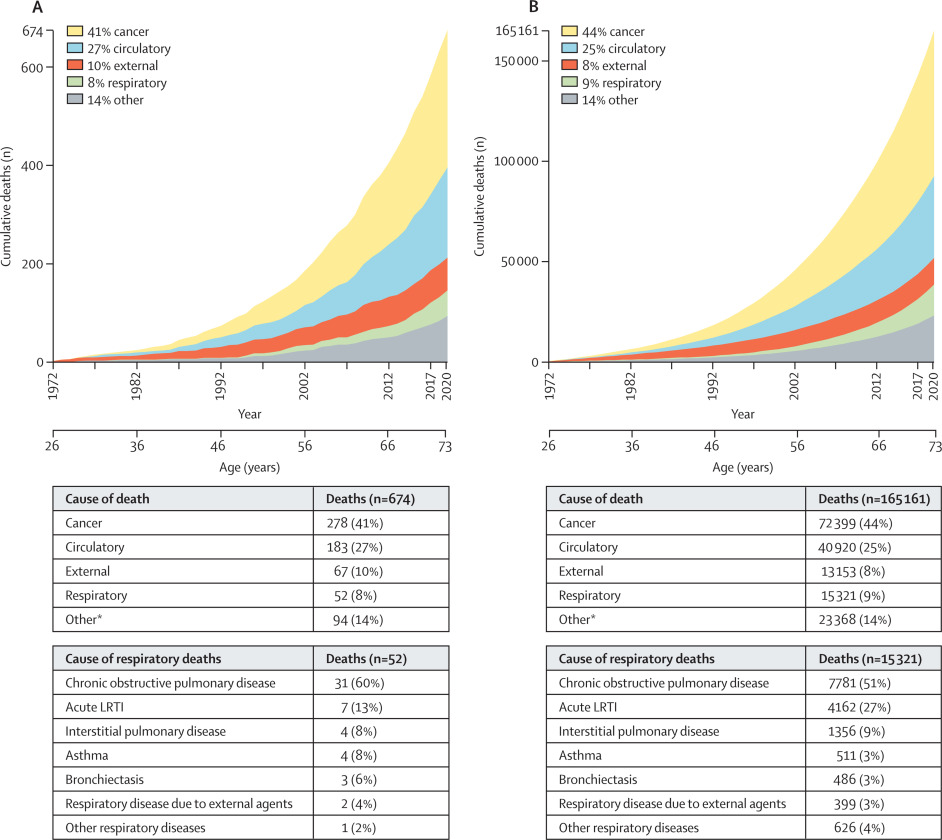
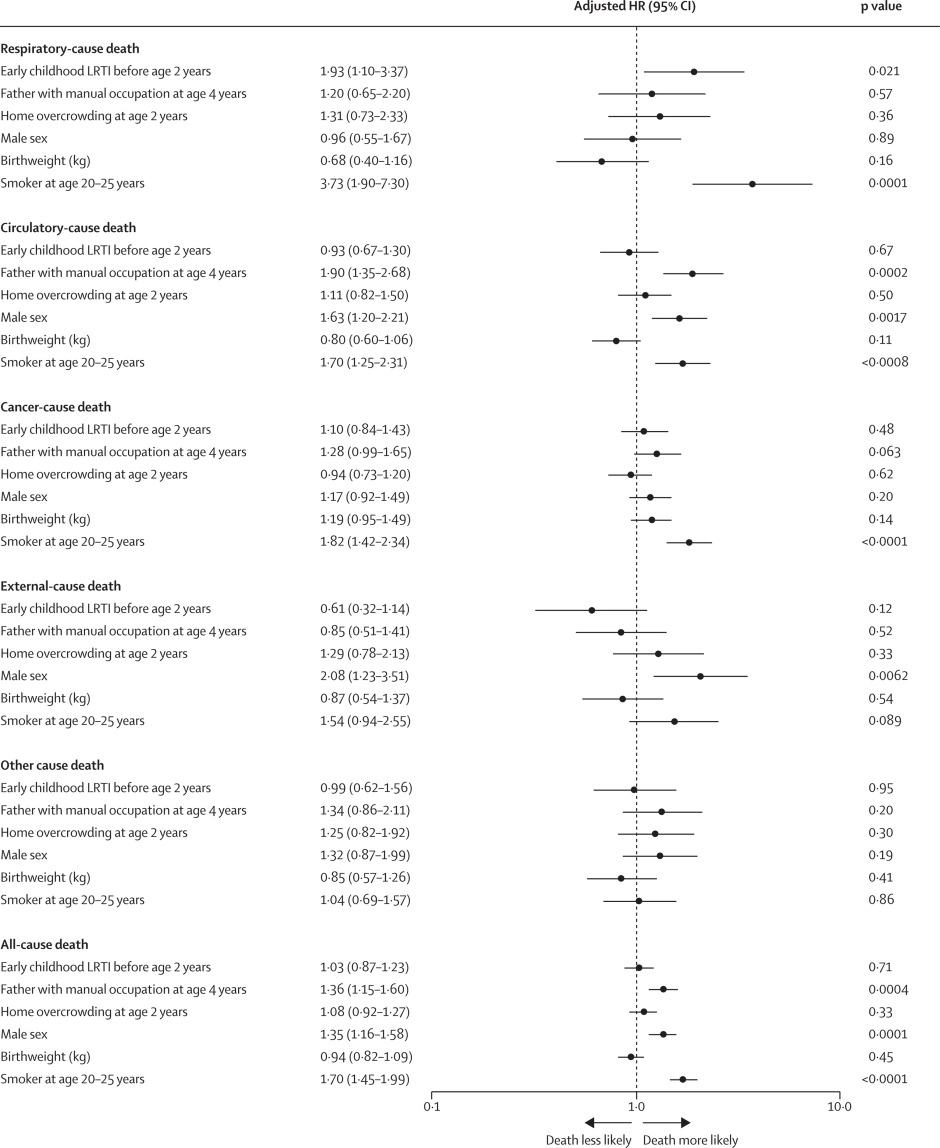
The authors concluded that, in this perspective, life-spanning, nationally representative cohort study, LRTI during early childhood was associated with almost a two times increased risk of premature adult death from respiratory disease, and accounted for one-fifth of these deaths.
What has that got to do with so-called alternative medicine?
Nothing!
Yet, I feel that this study is so remarkable that I need to report on it nonetheless.
What do the findings indicate?
I am not sure. Perhaps they confirm that our genetic makeup is hugely important in determining our health. Thus even the earliest signs of weakness can provide an indication of what might happen in later life.
Whatever the meaning, I find this study fascinating and hope you agree.
During the last few days, several journalists have asked me about ayahuasca. Apparently, Harry Windsor said in an interview that it changed his life! However, the family of a young woman who took her own life after using ayahuasca has joined campaigners condemning his comments. Others – including myself – claim that Harry is sending a worrying message talking about his ‘positive’ experience with ayahuasca, saying it ‘brought me a sense of relaxation, release, comfort, a lightness that I managed to hold on to for a period of time’.
So, what is ayahuasca?
This paper explains it quite well:
Ayahuasca is a hallucinogen brew traditionally used for ritual and therapeutic purposes in Northwestern Amazon. It is rich in the tryptamine hallucinogens dimethyltryptamine (DMT), which acts as a serotonin 5-HT2A agonist. This mechanism of action is similar to other compounds such as lysergic acid diethylamide (LSD) and psilocybin. The controlled use of LSD and psilocybin in experimental settings is associated with a low incidence of psychotic episodes, and population studies corroborate these findings. Both the controlled use of DMT in experimental settings and the use of ayahuasca in experimental and ritual settings are not usually associated with psychotic episodes, but little is known regarding ayahuasca or DMT use outside these controlled contexts. Thus, we performed a systematic review of the published case reports describing psychotic episodes associated with ayahuasca and DMT intake. We found three case series and two case reports describing psychotic episodes associated with ayahuasca intake, and three case reports describing psychotic episodes associated with DMT. Several reports describe subjects with a personal and possibly a family history of psychosis (including schizophrenia, schizophreniform disorders, psychotic mania, psychotic depression), nonpsychotic mania, or concomitant use of other drugs. However, some cases also described psychotic episodes in subjects without these previous characteristics. Overall, the incidence of such episodes appears to be rare in both the ritual and the recreational/noncontrolled settings. Performance of a psychiatric screening before administration of these drugs, and other hallucinogens, in controlled settings seems to significantly reduce the possibility of adverse reactions with psychotic symptomatology. Individuals with a personal or family history of any psychotic illness or nonpsychotic mania should avoid hallucinogen intake.
In other words, ayahuasca can lead to serious side effects. They include vomiting, diarrhea, paranoia, and panic. Ayahuasca can also interact with many medications, including antidepressants, psychiatric medications, drugs used to control Parkinson’s disease, cough medicines, weight loss medications, and more. Those with a history of psychiatric disorders, such as schizophrenia, should avoid ayahuasca because this could worsen their psychiatric symptoms. Additionally, taking ayahuasca can increase your heart rate and blood pressure, which may result in dangerous consequences for those who have a heart condition.
Thus ayahuasca is an interesting albeit dangerous herb (in most countries it is illegal to possess or consume it). Currently, it is clearly under-researched, which means we know very little about its potential benefits and even less about the harm it can do.
Considering this, one would think that any half-intelligent person with loads of influence would not promote or encourage its use – but, sadly, it seems that one would be mistaken.
The ‘keto diet’ is a currently popular high-fat, low-carbohydrate diet; it limits the intake of glucose which results in the production of ketones by the liver and their uptake as an alternative energy source by the brain. It is said to be an effective treatment for intractable epilepsy. In addition, it is being promoted as a so-called alternative medicine (SCAM) for a wide range of conditions, including:
- weight loss,
- cognitive and memory enhancement,
- type II diabetes,
- cancer,
- neurological and psychiatric disorders.
Now, it has been reported that the ‘keto diet’ may be linked to higher levels of cholesterol and double the risk of cardiovascular events. In the study, researchers defined a low-carb, high-fat (LCHF) diet as 45% of total daily calories coming from fat and 25% coming from carbohydrates. The study, which has so far not been peer-reviewed, was presented Sunday at the American College of Cardiology’s Annual Scientific Session Together With the World Congress of Cardiology.
“Our study rationale came from the fact that we would see patients in our cardiovascular prevention clinic with severe hypercholesterolemia following this diet,” said Dr. Iulia Iatan from the Healthy Heart Program Prevention Clinic, St. Paul’s Hospital, and University of British Columbia’s Centre for Heart Lung Innovation in Vancouver, Canada, during a presentation at the session. “This led us to wonder about the relationship between these low-carb, high-fat diets, lipid levels, and cardiovascular disease. And so, despite this, there’s limited data on this relationship.”
The researchers compared the diets of 305 people eating an LCHF diet with about 1,200 people eating a standard diet, using health information from the United Kingdom database UK Biobank, which followed people for at least a decade. They found that people on the LCHF diet had higher levels of low-density lipoprotein and apolipoprotein B. Apolipoprotein B is a protein that coats LDL cholesterol proteins and can predict heart disease better than elevated levels of LDL cholesterol can. The researchers also noticed that the LCHF diet participants’ total fat intake was higher in saturated fat and had double the consumption of animal sources (33%) compared to those in the control group (16%). “After an average of 11.8 years of follow-up – and after adjustment for other risk factors for heart disease, such as diabetes, high blood pressure, obesity, and smoking – people on an LCHF diet had more than two times higher risk of having several major cardiovascular events, such as blockages in the arteries that needed to be opened with stenting procedures, heart attack, stroke, and peripheral arterial disease.” Their press release also cautioned that their study “can only show an association between the diet and an increased risk for major cardiac events, not a causal relationship,” because it was an observational study, but their findings are worth further investigation, “especially when approximately 1 in 5 Americans report being on a low-carb, keto-like or full keto diet.”
I have to say that I find these findings not in the slightest bit surprising and would fully expect the relationship to be causal. The current craze for this diet is concerning and we need to warn consumers that they might be doing themselves considerable harm.
Other authors have recently pointed out that, within the first 6-12 months of initiating the keto diet, transient decreases in blood pressure, triglycerides, and glycosylated hemoglobin, as well as increases in HDL and weight loss may be observed. However, the aforementioned effects are generally not seen after 12 months of therapy. Despite the diet’s favorable effect on HDL-C, the concomitant increases in LDL-C and very-low-density lipoproteins (VLDL) may lead to increased cardiovascular risks. And another team of researchers has warned that “given often-temporary improvements, unfavorable effects on dietary intake, and inadequate data demonstrating long-term safety, for most individuals, the risks of ketogenic diets may outweigh the benefits.”