risk
It has been reported, at the German Medical Congress (DÄT) a year ago, that it was decided to delete the additional title of homeopathy from the model further training regulations of the German Medical Association. And Federal Health Minister Karl Lauterbach (SPD) tweeted applause: “Homeopathy has no place in modern medicine.”
Now the ‘ Bundesverband der Pharmaziestudierenden in Deutschland’ (BPhD), the German Pharmacists Organization, even goes a few steps further. The position paper distinguishes between evidence-based medicine (EBM) and unproven therapeutic methods. According to the BPhD, these include homeopathy, but also anthroposophy, traditional Chinese medicine, and traditional medicines.
Among other things, the BPhD is disturbed by the way homeopathy presents itself as an alternative, because an alternative means “a choice between two equally suitable possibilities” to achieve a goal, and this is not the case. Compared to evidence-based medicine (EBM), homeopathy is a “constructed, illusory concept” and “the principles of homeopathic teachings and principles” are to be rejected as “unscientific”. According to the BPhD, a designation as “alternative” for advertising purposes should no longer be allowed.
They would also like to see a demarcation from naturopathy; the clear distinction between homeopathy and phytopharmacy has been lacking up to now. The advertising attribute “natural” should therefore also be banned in order to prevent equalization in advertising, the position paper states.
Like doctors, pharmacy students point to the lack of proof of efficacy beyond the placebo effect. According to the BPhD, the dogma WER HEILT HAT RECHT, “he who heals is right” would “disregard all processes that work towards healing and glorify the result”. The “gold standard” of EBM – randomized, double-blind studies with placebo control – should in future also have to be fulfilled by homeopathic medicines, experience reports are not sufficient, it continues.
Homeopathic medicines are only registered as medicinal products without indication, which requires neither proof of efficacy nor clinical studies. The BPhD, therefore, demands that a warning be placed on the preparations that they have “no proven efficacy beyond the placebo effect”. Up to now, without this warning, patients have been “deceived about the efficacy”, and there is an “urgent need for detailed public information and counseling on homeopathy since its unjustified reputation poses a danger of not seeking treatment”. The BPhD also demands that the status of homeopathic medicines is withdrawn and that the pharmacy obligation for the preparations is abolished…
“In the health professions, no trivialization of unproven therapeutic procedures should be tolerated, as inadequate counseling or ignorance poses a danger to patients,” the BPhD said.
_________________________
When I first read this article – I translated and shortened it for those who cannot read German- I was truly dazzled. These are the suggestions that I have been making for around 20 years now, not specifically for Germany but for pharmacists in general. For many years, the Germans seemed the least likely to agree with me. But now they seem to be ahead of everyone else in Europe!
How come?
I suspect and hope that our recent initiative might have something to do with it.
Let’s hope that the pharmacists of other countries follow the German example.
On this blog, we have some people who continue to promote conspiracy theories about Covid and Covid vaccinations. It is, therefore, time, I feel, to present them with some solid evidence on the subject (even though it means departing from our usual focus on SCAM).
This Cochrane review assessed the efficacy and safety of COVID‐19 vaccines (as a full primary vaccination series or a booster dose) against SARS‐CoV‐2. An impressive team of investigators searched the Cochrane COVID‐19 Study Register and the COVID‐19 L·OVE platform (last search date 5 November 2021). They also searched the WHO International Clinical Trials Registry Platform, regulatory agency websites, and Retraction Watch. They included randomized controlled trials (RCTs) comparing COVID‐19 vaccines to placebo, no vaccine, other active vaccines, or other vaccine schedules.
A total of 41 RCTs could be included and analyzed assessing 12 different vaccines, including homologous and heterologous vaccine schedules and the effect of booster doses. Thirty‐two RCTs were multicentre and five were multinational. The sample sizes of RCTs were 60 to 44,325 participants. Participants were aged: 18 years or older in 36 RCTs; 12 years or older in one RCT; 12 to 17 years in two RCTs; and three to 17 years in two RCTs. Twenty‐nine RCTs provided results for individuals aged over 60 years, and three RCTs included immunocompromised patients. No trials included pregnant women. Sixteen RCTs had two‐month follow-ups or less, 20 RCTs had two to six months, and five RCTs had greater than six to 12 months or less. Eighteen reports were based on preplanned interim analyses. The overall risk of bias was low for all outcomes in eight RCTs, while 33 had concerns for at least one outcome. 343 registered RCTs with results not yet available were identified.The evidence for mortality was generally sparse and of low or very low certainty for all WHO‐approved vaccines, except AD26.COV2.S (Janssen), which probably reduces the risk of all‐cause mortality (risk ratio (RR) 0.25, 95% CI 0.09 to 0.67; 1 RCT, 43,783 participants; high‐certainty evidence).High‐certainty evidence was found that BNT162b2 (BioNtech/Fosun Pharma/Pfizer), mRNA‐1273 (ModernaTx), ChAdOx1 (Oxford/AstraZeneca), Ad26.COV2.S, BBIBP‐CorV (Sinopharm‐Beijing), and BBV152 (Bharat Biotect) reduce the incidence of symptomatic COVID‐19 compared to placebo (vaccine efficacy (VE): BNT162b2: 97.84%, 95% CI 44.25% to 99.92%; 2 RCTs, 44,077 participants; mRNA‐1273: 93.20%, 95% CI 91.06% to 94.83%; 2 RCTs, 31,632 participants; ChAdOx1: 70.23%, 95% CI 62.10% to 76.62%; 2 RCTs, 43,390 participants; Ad26.COV2.S: 66.90%, 95% CI 59.10% to 73.40%; 1 RCT, 39,058 participants; BBIBP‐CorV: 78.10%, 95% CI 64.80% to 86.30%; 1 RCT, 25,463 participants; BBV152: 77.80%, 95% CI 65.20% to 86.40%; 1 RCT, 16,973 participants).Moderate‐certainty evidence was found that NVX‐CoV2373 (Novavax) probably reduces the incidence of symptomatic COVID‐19 compared to placebo (VE 82.91%, 95% CI 50.49% to 94.10%; 3 RCTs, 42,175 participants).There is low‐certainty evidence for CoronaVac (Sinovac) for this outcome (VE 69.81%, 95% CI 12.27% to 89.61%; 2 RCTs, 19,852 participants).High‐certainty evidence was found that BNT162b2, mRNA‐1273, Ad26.COV2.S, and BBV152 result in a large reduction in the incidence of severe or critical disease due to COVID‐19 compared to placebo (VE: BNT162b2: 95.70%, 95% CI 73.90% to 99.90%; 1 RCT, 46,077 participants; mRNA‐1273: 98.20%, 95% CI 92.80% to 99.60%; 1 RCT, 28,451 participants; AD26.COV2.S: 76.30%, 95% CI 57.90% to 87.50%; 1 RCT, 39,058 participants; BBV152: 93.40%, 95% CI 57.10% to 99.80%; 1 RCT, 16,976 participants).
Moderate‐certainty evidence was found that NVX‐CoV2373 probably reduces the incidence of severe or critical COVID‐19 (VE 100.00%, 95% CI 86.99% to 100.00%; 1 RCT, 25,452 participants).
Two trials reported high efficacy of CoronaVac for severe or critical disease with wide CIs, but these results could not be pooled.
mRNA‐1273, ChAdOx1 (Oxford‐AstraZeneca)/SII‐ChAdOx1 (Serum Institute of India), Ad26.COV2.S, and BBV152 probably result in little or no difference in serious adverse events (SAEs) compared to placebo (RR: mRNA‐1273: 0.92, 95% CI 0.78 to 1.08; 2 RCTs, 34,072 participants; ChAdOx1/SII‐ChAdOx1: 0.88, 95% CI 0.72 to 1.07; 7 RCTs, 58,182 participants; Ad26.COV2.S: 0.92, 95% CI 0.69 to 1.22; 1 RCT, 43,783 participants); BBV152: 0.65, 95% CI 0.43 to 0.97; 1 RCT, 25,928 participants). In each of these, the likely absolute difference in effects was fewer than 5/1000 participants.
Evidence for SAEs is uncertain for BNT162b2, CoronaVac, BBIBP‐CorV, and NVX‐CoV2373 compared to placebo (RR: BNT162b2: 1.30, 95% CI 0.55 to 3.07; 2 RCTs, 46,107 participants; CoronaVac: 0.97, 95% CI 0.62 to 1.51; 4 RCTs, 23,139 participants; BBIBP‐CorV: 0.76, 95% CI 0.54 to 1.06; 1 RCT, 26,924 participants; NVX‐CoV2373: 0.92, 95% CI 0.74 to 1.14; 4 RCTs, 38,802 participants).
The authors’ conclusions were as follows: Compared to placebo, most vaccines reduce, or likely reduce, the proportion of participants with confirmed symptomatic COVID‐19, and for some, there is high‐certainty evidence that they reduce severe or critical disease. There is probably little or no difference between most vaccines and placebo for serious adverse events. Over 300 registered RCTs are evaluating the efficacy of COVID‐19 vaccines, and this review is updated regularly on the COVID‐NMA platform (covid-nma.com).
_____________________
As some conspiratorial loons will undoubtedly claim that this review is deeply biased; it might be relevant to add the conflicts of interest of its authors:
- Carolina Graña: none known.
- Lina Ghosn: none known.
- Theodoros Evrenoglou: none known.
- Alexander Jarde: none known.
- Silvia Minozzi: no relevant interests; Joint Co‐ordinating Editor and Method editor of the Drugs and Alcohol Group.
- Hanna Bergman: Cochrane Response – consultant; WHO – grant/contract (Cochrane Response was commissioned by the WHO to perform review tasks that contribute to this publication).
- Brian Buckley: none known.
- Katrin Probyn: Cochrane Response – consultant; WHO – consultant (Cochrane Response was commissioned to perform review tasks that contribute to this publication).
- Gemma Villanueva: Cochrane Response – employment (Cochrane Response has been commissioned by WHO to perform parts of this systematic review).
- Nicholas Henschke: Cochrane Response – consultant; WHO – consultant (Cochrane Response was commissioned by the WHO to perform review tasks that contributed to this publication).
- Hillary Bonnet: none known.
- Rouba Assi: none known.
- Sonia Menon: P95 – consultant.
- Melanie Marti: no relevant interests; Medical Officer at WHO.
- Declan Devane: Health Research Board (HRB) – grant/contract; registered nurse and registered midwife but no longer in clinical practice; Editor, Cochrane Pregnancy and Childbirth Group.
- Patrick Mallon: AstraZeneca – Advisory Board; spoken of vaccine effectiveness to media (print, online, and live); works as a consultant in a hospital that provides vaccinations; employed by St Vincent’s University Hospital.
- Jean‐Daniel Lelievre: no relevant interests; published numerous interviews in the national press on the subject of COVID vaccination; Head of the Department of Infectious Diseases and Clinical Immunology CHU Henri Mondor APHP, Créteil; WHO (IVRI‐AC): expert Vaccelarate (European project on COVID19 Vaccine): head of WP; involved with COVICOMPARE P et M Studies (APHP, INSERM) (public fundings).
- Lisa Askie: no relevant interests; Co‐convenor, Cochrane Prospective Meta‐analysis Methods Group.
- Tamara Kredo: no relevant interests; Medical Officer in an Infectious Diseases Clinic at Tygerberg Hospital, Stellenbosch University.
- Gabriel Ferrand: none known.
- Mauricia Davidson: none known.
- Carolina Riveros: no relevant interests; works as an epidemiologist.
- David Tovey: no relevant interests; Emeritus Editor in Chief, Feedback Editors for 2 Cochrane review groups.
- Joerg J Meerpohl: no relevant interests; member of the German Standing Vaccination Committee (STIKO).
- Giacomo Grasselli: Pfizer – speaking engagement.
- Gabriel Rada: none known.
- Asbjørn Hróbjartsson: no relevant interests; Cochrane Methodology Review Group Editor.
- Philippe Ravaud: no relevant interests; involved with Mariette CORIMUNO‐19 Collaborative 2021, the Ministry of Health, Programme Hospitalier de Recherche Clinique, Foundation for Medical Research, and AP‐HP Foundation.
- Anna Chaimani: none known.
- Isabelle Boutron: no relevant interests; member of Cochrane Editorial Board.
___________________________
And as some might say this analysis is not new, here are two further papers just out:
Objectives To determine the association between covid-19 vaccination types and doses with adverse outcomes of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection during the periods of delta (B.1.617.2) and omicron (B.1.1.529) variant predominance.
Design Retrospective cohort.
Setting US Veterans Affairs healthcare system.
Participants Adults (≥18 years) who are affiliated to Veterans Affairs with a first documented SARS-CoV-2 infection during the periods of delta (1 July-30 November 2021) or omicron (1 January-30 June 2022) variant predominance. The combined cohorts had a mean age of 59.4 (standard deviation 16.3) and 87% were male.
Interventions Covid-19 vaccination with mRNA vaccines (BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna)) and adenovirus vector vaccine (Ad26.COV2.S (Janssen/Johnson & Johnson)).
Main outcome measures Stay in hospital, intensive care unit admission, use of ventilation, and mortality measured 30 days after a positive test result for SARS-CoV-2.
Results In the delta period, 95 336 patients had infections with 47.6% having at least one vaccine dose, compared with 184 653 patients in the omicron period, with 72.6% vaccinated. After adjustment for patient demographic and clinical characteristics, in the delta period, two doses of the mRNA vaccines were associated with lower odds of hospital admission (adjusted odds ratio 0.41 (95% confidence interval 0.39 to 0.43)), intensive care unit admission (0.33 (0.31 to 0.36)), ventilation (0.27 (0.24 to 0.30)), and death (0.21 (0.19 to 0.23)), compared with no vaccination. In the omicron period, receipt of two mRNA doses were associated with lower odds of hospital admission (0.60 (0.57 to 0.63)), intensive care unit admission (0.57 (0.53 to 0.62)), ventilation (0.59 (0.51 to 0.67)), and death (0.43 (0.39 to 0.48)). Additionally, a third mRNA dose was associated with lower odds of all outcomes compared with two doses: hospital admission (0.65 (0.63 to 0.69)), intensive care unit admission (0.65 (0.59 to 0.70)), ventilation (0.70 (0.61 to 0.80)), and death (0.51 (0.46 to 0.57)). The Ad26.COV2.S vaccination was associated with better outcomes relative to no vaccination, but higher odds of hospital stay and intensive care unit admission than with two mRNA doses. BNT162b2 was generally associated with worse outcomes than mRNA-1273 (adjusted odds ratios between 0.97 and 1.42).
Conclusions In veterans with recent healthcare use and high occurrence of multimorbidity, vaccination was robustly associated with lower odds of 30 day morbidity and mortality compared with no vaccination among patients infected with covid-19. The vaccination type and number of doses had a significant association with outcomes.
SECOND EXAMPLE Long COVID, or complications arising from COVID-19 weeks after infection, has become a central concern for public health experts. The United States National Institutes of Health founded the RECOVER initiative to better understand long COVID. We used electronic health records available through the National COVID Cohort Collaborative to characterize the association between SARS-CoV-2 vaccination and long COVID diagnosis. Among patients with a COVID-19 infection between August 1, 2021 and January 31, 2022, we defined two cohorts using distinct definitions of long COVID—a clinical diagnosis (n = 47,404) or a previously described computational phenotype (n = 198,514)—to compare unvaccinated individuals to those with a complete vaccine series prior to infection. Evidence of long COVID was monitored through June or July of 2022, depending on patients’ data availability. We found that vaccination was consistently associated with lower odds and rates of long COVID clinical diagnosis and high-confidence computationally derived diagnosis after adjusting for sex, demographics, and medical history.
_______________________________________
There are, of course, many more articles on the subject for anyone keen to see the evidence. Sadly, I have little hope that the COVID loons will be convinced by any of them. Yet, I thought I should give it nevertheless a try.
In response to yesterday’s post, I received a lengthy comment from ‘Stan’. Several readers have already commented on it. Therefore, I can make my arguments short. In this post, will repeat Stan’s points each followed by my comments (in bold). Here we go:
Seven Reasons Homœopathy is Not Placebo Effect
Sorry, Stan, but your heading is not proper English; I have therefore changed it for the title of this post.
1. Homeopathic remedies work on babies, animals, plants and people in a coma. Biodynamic farmers use homeopathic remedies to repel pests and treat plant diseases. Some organic ranchers rely on homeopathic remedies to treat their herds. Some “placebo by proxy” effect has been shown for children but its doubtful that it could be shown for a herd of cattle or crops in a field. Farmers can’t rely on wishful thinking to stay in business.
As discussed ad nauseam on this blog, homeopathic remedies do not work on babies or animals better than placebos. I don’t know of any studies with “people in a coma” (if you do, Stan, please let me know). The fact that ranchers rely on homeopathy is hilarious but does not prove anything.
2. The correct curative remedy will initially cause a worsening of the condition being cured if it is given in too strong (i.e. too dilute) a dose. A placebo might only cause a temporary improvement of the condition being treated; certainly not an aggravation.
The ‘homeopathic aggravation’ is a myth created by homeopaths. It disappears if we try to systematically research it; see here, for instance.
3. One can do a “proving” of an unknown homeopathic remedy by taking it repeatedly over several days and it will temporarily cause symptoms that one has never experienced previously – symptoms it will cure in a sick person. This is a repeatable scientific experiment used to determine the scope of a new remedy, or confirm the effects of an already proven remedy. A placebo might possibly have an effect if the individual taking it has been “prepared” by being told what they are taking but it likely wouldnt match previously recorded symptoms in the literature.
Homeopathic provings are rubbish and not reproducible when done rigorously; see here.
4. One can treat simple acute (self-limiting) conditions (e.g. minor burns, minor injuries, insect bites, etc.) and see unusually rapid cures with homeopathic remedies. A placebo might only cause a temporary improvement of the condition being treated while taken. Placebos have been found mostly effective in conditions with a strong psychological component like pain.
You mean like using Arnica for cuts and bruises? Sadly, it does not work.
5. One can get homeopathic treatment for long term chronic (non self-limiting) conditions and see a deep lasting cure, as has been documented clinically for a couple centuries. A placebo might only cause a temporary partial improvement of the condition being treated while the placebo is being taken.
You mean like asthma, eczema, or insomnia?
6. There is over 200 years worth of extensive documentation from around the world, of the clinical successes of homeopathy for both acute and chronic conditions of all types. As Dr Hahn has said you have throw out 90% of the evidence to conclude that homeopathy doesnt work. The Sheng et al meta-analysis in 2005 Lancet that was supposedly the death knell of homeopathy used only 8 studies, excluding hundreds of others. Unsurprisingly homeopathy was found wanting. So-called Skeptics see what they want to see in the science. There is relatively little documentation of placebo usage. A few recent studies have been done showing the limited temporary benefits of placebos.
What Hahn wrote is understandably liked by homeopaths but it nevertheless is BS. If you don’t trust me, please rely on independent bodies from across the world.
7. Homeopathic remedies have been shown to have a very weak electromagnetic signature and contain some nano-particles. Some believe this explains their mechanism. An exciting new potential field of research is the subtle cell signalling that has been found to direct the development of stem cells. Scientists have created double-headed planeria worms and this trait has been found to be inherited by their offspring without any change in the genes or epigenetics. Until now we had no idea how a single fertilized ovum could evolve into a complex creature that is bilateral and has multiple cell types. It is possible that the very subtle electromagnetic signature or some other unknown effect of homeopathic remedies is effecting this subtle cell signalling.
The homeopathic nano-myth is nonsense. And so is the rest of your assumptions.
Every conventional drug has “side effects” that match the symptoms for which it is indicated! Aspirin can cause headaches and fever, ritalin can cause hyperactive effects, radiation can cause cancer. Conventional doctors are just practicing bad homeopathy. They are prescribing Partially similar medicines. If their drugs were homeopathic (i.e. similar) to the patients symptoms on all levels they would be curative. Radiation sometimes does cure cancer instead of just suppressing it per usual.
Even if this were true, what would it prove? Certainly not that homeopathy works!
Dr Hahneman did forbid mixing homeopathy and conventional medicine. In his day doctors commonly used extensive blood letting and extreme doses of mercury. Its not Quite as bad now.
You evidently did not read Hahnemann’s writings.
Just because we dont know how extremely dilute homeopathic remedies work, doesn’t discount that they Do work. Homeopathy seems to fly in the face of Known science. In no way is it irrational or unscientific. There are lots of phenomena in the universe that cant be explained yet, like dark energy and dark matter effects and even consciousness!
Not knowing how a treatment works has not stopped science to test whether it works (e.g. Aspirin). In the case of homeopathy, the results of these endeavors were not positive.
The assumption that the moon is made of cheese also flies in the face of science; do you perhaps think that this makes it true?
The actions of homeopathy can and have been well-explained: they are due to placebo effects.
________________________
Stan, thank you for this entertaining exercise. But, next time, please remember to supply evidence for your statements.
After all these years, I am still fascinated by what proponents of homeopathy try to tell others about their trade. Recently I found a long article in this vein. It is aimed at an audience of HEILPRAKTIKER and their patients. It should therefore be responsible, thorough, and evidence-based (yes, I am an optimist).
“With this article”, the authors state, “we aim to provide a comprehensive overview of homeopathy and help people make informed decisions about their health. Whether you already have experience with homeopathy or simply want to inform yourself, we hope that this article will provide you with valuable insights and information” (my translation).
Here I present to you just the relatively short section dedicated to the ‘pros and cons’ of homeopathy. Here we go:
Advantages of homeopathy:
- Holistic approach: homeopathy considers the human being as a whole and takes into account both physical and emotional aspects. It aims to support individual balance and the body’s self-healing powers.
- Gentle and non-invasive treatment: Homeopathic remedies are usually taken as globules, drops, or tablets and are therefore easy and convenient to use. They rarely cause side effects and are generally well tolerated.
- Individualized treatment: In homeopathy, each patient is considered unique and treatment is based on individual symptoms and characteristics. There is no “one-size-fits-all” solution, but a personalized approach.
- Support for chronic diseases: Homeopathy can be an alternative or complementary treatment for chronic conditions where conventional medicines offer limited relief. It can help improve quality of life and promote overall well-being.
Limitations of homeopathy:
- Placebo effect: Much of the effect of homeopathy is attributed to the placebo effect. It is argued that the improvements patients experience occur because of belief in the efficacy of the remedies and positive expectations, rather than due to a specific effect of the diluted substances.
- Lack of scientific evidence: The scientific evidence for the efficacy of homeopathy is limited and controversial. Many studies have failed to demonstrate benefits beyond the placebo effect. There is a lack of well-conducted randomized controlled trials that clearly show the effectiveness of homeopathy.
- Delay or rejection of conventional treatments: In some cases, the choice of homeopathy as the sole method of treatment may lead to delays in the diagnosis and timely treatment of serious or acute illnesses. It is important that serious illnesses are examined by a doctor and treated appropriately.
- Difficulties in standardization: Homeopathy involves a variety of remedies used in different potencies and dilutions. This makes standardization and the conduct of reproducible studies difficult. There are also controversial debates about whether the dilutions go beyond the extent to which molecules of the original substance are still present.
__________________________
I am sure that you have heard the BS about the alleged advantages of homeopathy often enough. Therefore, I will here not bother to comment on them again. More interesting, in my view, are the limitations of homeopathy, as seen by its proponents. Please allow me, therefore, to discuss them briefly.
- The authors state that “it is argued that the improvements patients experience occur because of belief in the efficacy of the remedies and positive expectations”. This sounds as though this is a mere aberrant opinion or at least an ongoing debate amongst scientists. In fact, it is the scientific consensus supported by tons of evidence.
- This is the same point expressed differently.
- The admission that “the choice of homeopathy as the sole method of treatment may lead to delays in the diagnosis and timely treatment” is yet another way of stating that homeopathy is not effective. What is, however, not expressed clearly enough, in my view, is the fact that homeopathic treatment usually amounts to medical neglect which is unethical and can cause serious harm, in extreme cases even death.
- It is not true that the range of potencies renders “the conduct of reproducible studies difficult”. There are plenty of examples to demonstrate this, for instance, this study. “There are also controversial debates about whether the dilutions go beyond the extent to which molecules of the original substance are still present.” Yes, I did translate this correctly. I am sorry to say that this sentence does make no sense in German or in English.
What I find particularly interesting is that the authors do not mention disadvantages that non-homeopaths would rate as quite important, e.g.:
- The assumptions of homeopathy fly in the face of science.
- Hahnemann strictly forbade homeopathy to be combined with ‘allopathy’ (yet proponents now claim this option to be an advantage).
- Treating a patient with homeopathy violates even the most basic rules of medical ethics.
- Homeopaths have no choice but to lie to their patients on a daily basis.
- Many homeopaths have the nasty habit of advising their patients against using effective treatments, e.g. vaccinations.
- Homeopathy undermines rational thinking in a general way.
In summary, the authors’ “aim to provide a comprehensive overview of homeopathy and help people make informed decisions about their health” has not been reached.
The well-known Dr. Chris van Tulleken recently joined forces with Professor Michael Heinrich and Dr. Anthony Booker from the University College London School of Pharmacy to test a range of herbal products on sale in the UK. They bought over 70 herbal products from various high street stores and internet retailers. Some of the products were ‘THR’ (traditional herbal registration) herbal medicines, and some were marketed as food supplements. They then analyzed their chemistry to see whether each one really contained what the label says. The three popular herbal remedies we tested were:-
- Milk thistle (Silybum marianum),
- Ginkgo (Ginkgo biloba),
- Evening primrose (Oenothera).
The team at UCL used two different methods of analysis to verify the identity of these herbal products and extracts. High-performance thin-layer chromatography (HPTLC) is a sophisticated technique for the analysis of herbal products and is one of the most commonly used methods in the industry. HPTLC analysis creates a chemical fingerprint of the product which the researchers can then compare to an accepted reference standard for the herb. They look for a broad spectrum of ‘marker compounds’ these are the pharmacologically active and/or chemical constituents within a plant that can be used to verify its potency or identity. For complex samples or where additional confirmation is required, researchers often turn to ¹H nuclear magnetic resonance spectroscopy (¹H-NMR) which allows individual samples to be compared in detail against other samples or to the whole group.
In every THR product tested, the product contained what was claimed on the label. However, the food supplements showed a wide range of quality.
- Of the food supplement products labeled as Ginkgo, 8 out of 30 (27%) contained little or no ginkgo extract.
- 36% of the food supplement milk thistle products contained no detectable milk thistle. Although this is quite a small sample size it is still a startling result. Furthermore, in one case of milk thistle, unidentified adulterants suspected to be synthetic compounds were present in place of milk thistle.
- All of the evening primrose food products we tested did contain what the packet claimed.
The researchers concluded that their investigation shows that a regulatory system for herbal products, like the THR scheme, ensures that people have access to safe herbal medicine products. So, if you are considering buying herbal products then do look out for the THR mark– otherwise, you might not just be wasting your money, you might be consuming other, potentially dangerous, ingredients.
_______________________________
This is an interesting investigation. The researchers should be commended for it! However, I disagree with some of their conclusions. Here is why:
- The investigation merely tested the quality of the products and NOT THEIR SAFETY! To claim that the THR ensures access to safe herbal medicines is incorrect. A product might be of adequate quality but can still be unsafe. The THR only implies safety because the herbal has been used for years without problems being noted. This is not the same as ensuring that it is safe. A direct test of safety is usually not available.
- The recommendation to buy a product with a THR mark is also somewhat misleading. It implies that these products are effective. I fail to see convincing evidence that either MILK THISTLE, GINKGO, or EVENING PRIMROSE are effective for any disease or condition. Thus the responsible recommendation should, in my view, be to NOT buy them regardless of whether they are of good quality or not.
It has recently been reported that a 39-year-old woman (a mother-of-three died) died after immersing herself in a river as part of a cold water therapy session. The woman died after paramedics were called to attend a riverside in Derbyshire. The session was run by Kevin O’Neill of ‘Breatheolution’, whose previous clients include Coleen Rooney and actor Stephen Graham. The woman, who was visiting with two friends after paying up to £200 for a two-hour cold water therapy session, was rushed to hospital where she died.

Mr. O’Neill commented: “I am heartbroken. I’ve not slept and I’m finding it hard to process. I cannot stop thinking about her family. It’s tragic.” An inquest is expected to be opened into the woman’s death. East Midlands Ambulance Service said they were called to Bankside, in Bridgemont. “The caller reported a medical emergency,” a spokesperson said. “We sent a paramedic in a fast response car and a double-crewed ambulance. The air ambulance was also in attendance.”
Derbyshire Fire and Rescue Service, which was called to assist the paramedics, has warned people about the dangers of entering open water. “While we cannot and will not comment or speculate on the circumstances and cause of this tragic death, we would like to remind people of the dangers of entering open water and cold water shock,” said group manager Lee Williams.
_____________________
Breatheolution’ has a website where a whole page is dedicated to its leader Kevin O’Neill. I wondered what qualifications Kevin has, but all it tells us about him is this: “I struggled for so long with alcohol and other substance abuse that something had to give, I lost my sister Yvonne in 2019 and I think it was enough trauma to make me think a lot more about my own life”
The website also explains what the cold water sessions are about:
1-2-1 Breath Coaching, practice & Cold water session (river or tank)
2 hours @ £110.00
These sessions are proving popular with those who are not keen on group sessions or just prefer to have a more personal experience. The 2-3 hour sessions will be tailored to you and your breathing and will include potentially life-changing tools and methods to allow you to witness your breathing and physiology differently in the future, its all about feeling and awareness.
Another section of the site is dedicated to celebrities who Kevin seems to have treated. And then there is a video of the treatment. What I did not find anywhere, however, are the conditions that Kevin claims to treat with his cold water therapy.
In any case, it would have been wise for Kevin to read up about the risks of cold water immersion (CWI) before going into business. Perhaps this review would have helped:
In 2012, an estimated 372,000 people (42 per hour) died from immersion, assumed to be drowning. Immersion is the third leading cause of unintentional injury-related death, accounting for 7% of all such deaths (World Health Organization, 2014). These figures are underestimations owing to poor reporting in many Third World countries that have a high number of deaths. The data also do not include life-long morbidity caused by immersion-related injuries, estimated to be a much bigger numerical problem.
There is no strict definition of ‘cold water’. Given that some of the hazardous responses to cold water appear to peak on immersion somewhere between 15 and 10°C, it is reasonable to say that cold water is water <15°C (Tipton et al. 1991). However, the thermoneutral water temperature for a resting naked individual is ∼35°C, so it is possible for individuals to become very cold, with time, on immersion in water below this temperature. The corresponding temperature for those exercising (including shivering) is ∼25°C (Tipton & Golden, 1998).
Historically, the threat associated with CWI was regarded in terms of hypothermia or a reduction in deep body temperature below 35°C. This belief was established as a result of the Titanic disaster and supported by data obtained during maritime conflicts of World War II. However, more recently, a significant body of statistical, anecdotal and experimental evidence has pointed towards other causes of death on immersion. For example, in 1977 a Home Office Report revealed that ∼55% of the annual open water deaths in the UK occurred within 3 m of a safe refuge (42% within 2 m), and two-thirds of those who died were regarded as ‘good swimmers’. This evidence suggests more rapid incapacitation than can occur with whole-body cooling and consequent hypothermia.
The following four stages of immersion have been associated with particular risks (Golden & Hervey, 1981; Golden et al. 1991); the duration of these stages and the magnitude of the responses evoked within them vary significantly, depending on several factors, not least of which is water temperature:
- Initial immersion (first 3 min), skin cooling;
- Short-term immersion (3 min plus), superficial neuromuscular cooling;
- Long-term immersion (30 min plus), deep tissue cooling (hypothermia); and
- Circum-rescue collapse: immediately before, during or soon after rescue.
As a result of laboratory-based research, the initial responses to immersion, or ‘cold shock’, were identified as particularly hazardous (Tipton, 1989), accounting for the majority of immersion deaths (Tipton et al. 2014). These deaths have most often been ascribed to drowning, with the physiological responses of a gasp and uncontrollable hyperventilation, initiated by the dynamic response of the cutaneous cold receptors, resulting in the aspiration of the small volume of water necessary to initiate the drowning process (Bierens et al. 2016). Relatively little is known about the minimal rates of change of cold receptor temperature necessary to cause cold shock. The response has been reported to begin in water as warm as 25°C but is easy to suppress consciously at that temperature. In laboratory conditions, the respiratory frequency response (an indication of respiratory drive) peaks on naked immersion in a water temperature between 15 and 10°C, and is no greater on immersion in water at 5°C (Tipton et al. 1991). The corresponding average rates of change of chest skin temperature over the first 20 s of these immersions was 0.42 (water temperature 15°C), 0.56 (water temperature 10°C) and 0.68°C s−1 (water temperature 5°C). This suggests that an average rate of change in chest skin temperature between 0.42 and 0.56°C s−1 on the first 20 s of immersion is sufficient to evoke a maximal respiratory cold shock response.
More recently, it has been suggested (Shattock & Tipton, 2012) that a larger number of deaths than once thought may be attributable to arrhythmias initiated on immersion by the coincidental activation of the sympathetic and parasympathetic division of the autonomic nervous system by stimulation of cutaneous cold receptors around the body [sympathetic activation (cold shock)] and in the oronasal region on submersion or with wave splash [vagal stimulation (diving response)]. This ‘autonomic conflict’ is a very effective way of producing dysrhythmias and arrhythmias even in otherwise young and healthy individuals, particularly, but not necessarily, if a prolonged breath hold is involved in the immersion (Tipton et al. 1994). It seems that predisposing factors, such as long QT syndrome, ischaemic heart disease or myocardial hypertrophy, are necessary for fatal arrhythmias to evolve (Shattock & Tipton, 2012); many of these factors, including drug-induced long QT syndrome, are acquired. Non-fatal arrhythmias could still indirectly lead to death if they cause incapacitation and thereby drowning (Tipton, 2013). The hazardous responses associated with the cold shock response are presented in Fig. 2.
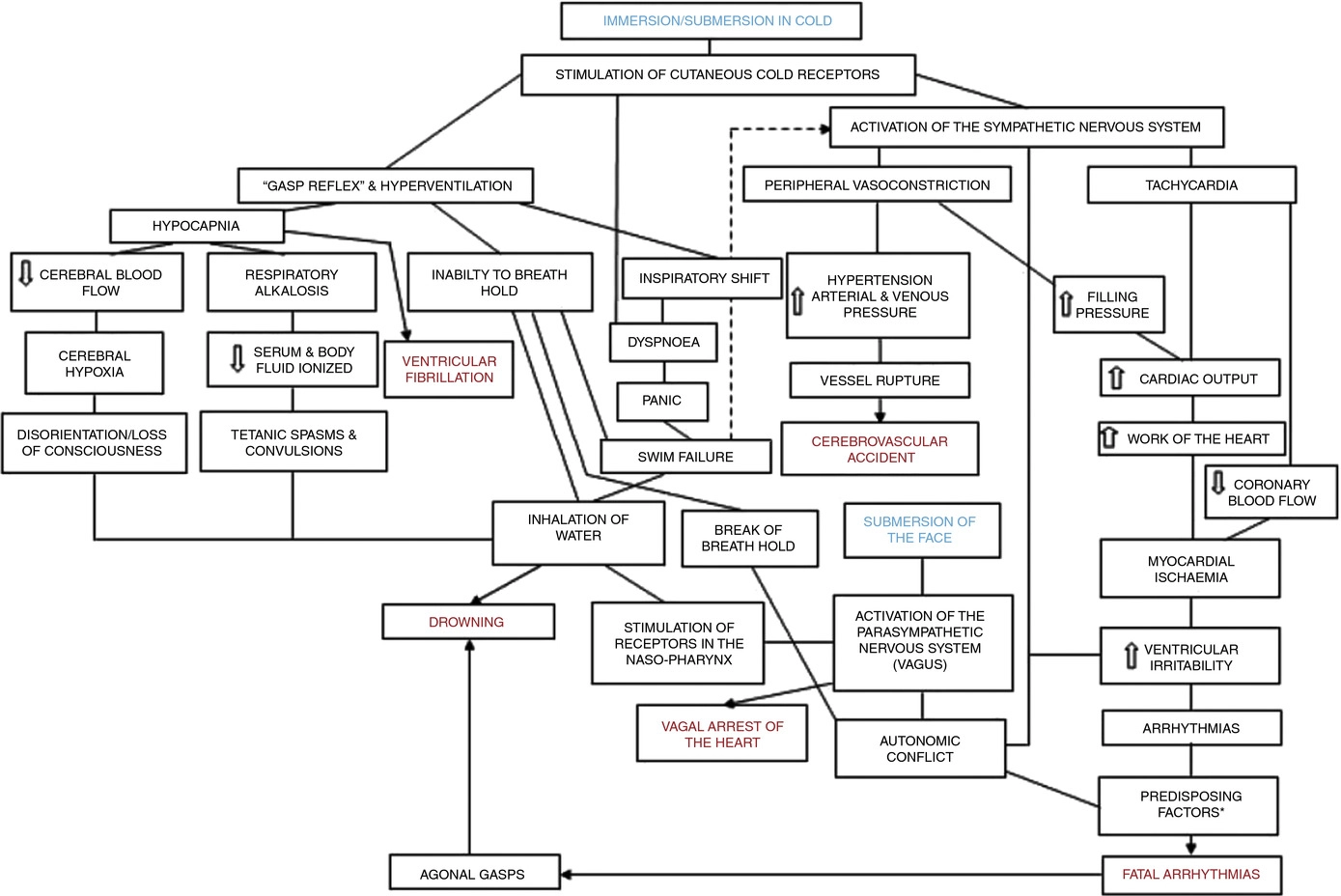
Figure 2. A contemporary view of the initial responses to immersion and submersion in cold water (‘cold shock’)
The problems encountered in short-term immersions are primarily related to physical incapacitation caused by neuromuscular cooling (Castellani & Tipton, 2015). The arms are particularly susceptible because of their high surface area to mass ratio. Low muscle temperatures affect chemical and physical processes at the cellular level. This includes metabolic rate, enzymatic activity, calcium and acetylcholine release and diffusion rate, as well as the series elastic components of connective tissues (Vincent & Tipton, 1988). Maximal dynamic strength, power output, jumping and sprinting performance are related to muscle temperature, with reductions ranging from 4 to 6% per degree Celsius reduction in muscle temperature down to 30°C (Bergh & Ekblom, 1979). At nerve temperatures below ∼20°C, nerve conduction is slowed and action potential amplitude is decreased (Douglas & Malcolm, 1955). Nerve block may occur after exposure to a local temperature of between 5 and 15°C for 1–15 min. This can lead to dysfunction that is equivalent to peripheral paralysis and can, again, result in drowning owing to the inability to keep the airway clear of the water (Clarke et al. 1958; Basbaum, 1973; Golden & Tipton, 2002; Fig. 3).

Figure 3. The ‘physiological pathways to drowning’ after immersion or submersion in cold water, with possible interventions for partial mitigation (dashed)
Abbreviations: EBA, emergency breathing aid; IS, immersion suit; and LJ, lifejacket. Reproduced with permission, from Tipton (2016b).
Even in ice-cold water, the possibility of hypothermia does not arise for at least 30 min in adults. Hypothermia affects cellular metabolism, blood flow and neural function. In severe hypothermia, the patient will be deeply unconscious. The progressive signs and symptoms (approximate deep body temperature) are shivering (36°C), confusion, disorientation, introversion (35°C), amnesia (34°C), cardiac arrhythmias (33°C), clouding of consciousness (33–30°C), loss of consciousness (30°C), ventricular fibrillation (28°C) and death (25°C) (Bierens et al. 2016). There is great variability between deep body temperature and the signs and symptoms of hypothermia. For example, although the deep body temperature associated with death is often quoted as 25°C, the lowest temperature recorded to date after accidental exposure to cold (air) and with full recovery was 12.7°C in a 28-month-old child (Associated Press, 2014). The coldest adult survivor of CWI followed by submersion had a body temperature of 13.7°C (Gilbert et al. 2000). There is also a large amount of variation in the rate at which people cool on immersion in cold water, owing to a combination of thermal factors (including water temperature and water movement, internal and external insulation) and non-thermal factors (including body size and composition, blood glucose, motion illness, racial and sex differences; Haight & Keatinge, 1973; Gale et al. 1981; White et al. 1992; Mekjavic et al. 2001; Golden & Tipton, 2002).
The most significant practical consequence of hypothermia in water is loss of consciousness; this prevents individuals from undertaking physical activity to maintain a clear airway and avoid drowning. Thus, once again, drowning is often the end-point (Fig. 3).
About 17% of those who die as a result of immersion die immediately before, during or after rescue (Golden et al. 1991). The deaths immediately before rescue are intriguing and probably related to behavioural changes at this time or the relief and psychophysiological alterations associated with imminent rescue, including a reduction in circulating stress hormone concentration and an increase in vagal tone. Death during rescue is most commonly associated with a collapse in arterial pressure when lifted vertical from the water and kept in that position for some time (Golden et al. 1991).
_____________________________
The tragic death of the woman should perhaps remind us that
- there is no SCAM or wellness treatment that is entirely harmless,
- and there are only few ‘would-be gurus’ who know what they are doing.
The German Heilpraktiker (HP), a non-medically trained practitioner of so-called alternative medicine (SCAM), has repeatedly been the subject of my posts. In a nutshell: the profession was created by the Nazis and was originally destined to disappear within one generation. But this did not happen, and today there are ~100 000 HPs who are allowed to treat almost any condition without mandatory training or experience. Many HP schools exist but you can also become an HP without formal training.
Now a report has been published by undercover journalists investigating these HP schools in Germany. Here I have summarized a few crucial passages for you (if you read German, I strongly recommend reading the original article):
There are more than 150 HP schools in Germany. On average, training costs several thousand euros. There is no uniform and state regulation for the training. The curricula are mostly created by the schools themselves.
In addition to medical and psychological content, the schools often offer seminars that are not based on scientific knowledge. The curricula sometimes include courses such as astrology, homeopathy, or so-called quantum healing. HP organizations give indeed training guidelines. However, these are not met by about 83% of the schools.
The students were isolated at the HP school from their environment and urged to break off contact with their families. “Without us you are nothing. That came so often and I then, unfortunately, believed in it, because I was alone. If I had had no one else from school, then I would really have been completely alone,” explains a former student in an interview. “During that time, I also thought for the first time: Are we in some kind of cult here?
The school’s principal rejects the cult accusation: “We have been confronted with the allegation that we are a cult for some time and have always dealt with it very openly because we are not a cult. The principal also denies other accusations made by former students, saying that the allegations of suggestion, coercion, compulsion, or sweeping statements are simply false. He said he would be happy to face them “in a personal conversation outside the public eye to answer their questions.”
In order to get to the bottom of the treatment methods, the reporter also had herself treated by the principal of the school in an undercover self-experiment. In the first session, she determined that the reporter’s sciatica had been passed on to her by her mother, which is why she should sever her ties with her. In the second session, she recommended that she no longer visit her cancer-stricken grandfather. When the principal learned that the ill grandpa was of the zodiac sign Cancer, she concluded, “Cancer gets cancer.” The cancer, she said, was due to the fact that he had done nothing for his soul. And further, the patient runs the risk of adopting the grandfather’s cancer symptoms when she visits him.
The Hamburg health authority, which is listed as a “supervisory authority” on the school’s homepage, explains in response to an inquiry that no official supervision exists for HP schools. To obtain permission for opening a school, no training is necessary. Neither possible training courses nor institutions offering such training courses are regulated by the state.
The journalist also asked the Federal Health Ministry whether it sees the need for action and legal control. The Ministry’s response was evasive: “If necessary,” the HP law should be reformed in the future.
____________________
This is shocking news for many Germans who believe that HPs are well-trained healthcare professionals. However, those who have read my recently published book cannot be surprised. Poor training is only one of a myriad of deficits of HPs. It is time that the government realizes that the current is unacceptable and endangers public health. It is time, in other words, that the government does something about the HP profession.
How often do we hear that chiropractic is safe because numerous trials reported no adverse events? This systematic review tested whether there has been a change in the reporting of adverse events associated with spinal manipulation in randomized clinical trials (RCTs) since 2016.
Databases were searched from March 2016 to May 2022: MEDLINE (Ovid), Embase, CINAHL, ICL, PEDro, and Cochrane Library. Domains of interest (pertaining to adverse events) included: completeness and location of reporting; nomenclature and description; spinal location and practitioner delivering manipulation; methodological quality of the studies and details of the publishing journal. Frequencies and proportions of studies reporting on each of these domains were calculated. Univariable and multivariable logistic regression models were fitted to examine the effect of potential predictors on the likelihood of studies reporting on adverse events.
5399 records were identified by the electronic searches, of which 154 (2.9%) were included in the analysis. Of these, 94 (61.0%) reported adverse events with only 23.4% providing an explicit description of what constituted an adverse event. Reporting of adverse events in the abstract has increased (n=29, 30.9%) while reporting in the results section has decreased (n=83, 88.3%) over the past 6 years. Spinal manipulation was delivered to 7518 participants in the included studies. No serious adverse events were reported in any of these studies.
The authors concluded as follows: while the current level of reporting of adverse events associated with spinal manipulation in RCTs has increased since our 2016 publication on the same topic, the level remains low and inconsistent with established standards. As such, it is imperative for authors, journal editors and administrators of clinical trial registries to ensure there is more balanced reporting of both benefits and harms in RCTs involving spinal manipulation.
This article is clearly relevant to our discussions about adverse events after spinal manipulation. However, I find it far too uncritical. This might be due to the affiliations of some of the authors:
- Integrative Spinal Research Group, Department of Chiropractic Medicine, University Hospital Balgrist and University of Zurich, Zurich, Switzerland.
- Department of Chiropractic, Faculty of Medicine, Health and Human Sciences, Macquarie University, Sydney, New South Wales, Australia.
Interestingly, the authors stated that they have no conflict of interest. Also interesting is the fact that they do not cite our paper from 2012. I, therefore, take the liberty of doing it:
Objective: To systematically review the reporting of adverse effects in clinical trials of chiropractic manipulation.
Data sources: Six databases were searched from 2000 to July 2011. Randomised clinical trials (RCTs) were considered, if they tested chiropractic manipulations against any control intervention in human patients suffering from any type of clinical condition. The selection of studies, data extraction, and validation were performed independently by two reviewers.
Results: Sixty RCTs had been published. Twenty-nine RCTs did not mention adverse effects at all. Sixteen RCTs reported that no adverse effects had occurred. Complete information on incidence, severity, duration, frequency and method of reporting of adverse effects was included in only one RCT. Conflicts of interests were not mentioned by the majority of authors.
Conclusions: Adverse effects are poorly reported in recent RCTs of chiropractic manipulations.
In percentage terms the results are similar. What is very different is that the authors of the new paper merely lament that the level remains low and inconsistent with established standards, while we make it clear in the abstract that adverse effect reporting is poor and in the paper identify this deficit as a violation against research ethics and thus as a form of scientific misconduct.
In view of all this, let me re-phrase the last sentence of the authors’ conclusion:
it is imperative for authors, journal editors, and administrators of clinical trial registries to ensure that researchers adhere to accepted ethical standards and that scientific misconduct no longer gets published.
Following the death from cancer of a 14-year-old Carinthian girl, the Klagenfurt public prosecutor’s office has launched an investigation against the girl’s parents. In February this year, the 14-year-old was taken to a hospital in Graz, Austria, where she died a few days later from cancer. The hospital filed charges because the tumor had been treated incorrectly with so-called alternative medicine (SCAM).
Investigations are underway on suspicion of torturing or neglecting underage, younger, or defenseless persons. Currently, the accused and witnesses are being questioned. The parents’ lawyer, Alexander Todor-Kostic, stated that the accusations were without any basis and claimed that the 14-year-old girl had decided of her own free will against being treated with chemotherapy and surgery. The parents respected this, allowed her alternative treatment methods, and acted in accordance with the applicable legal situation.
The girl had developed cancer the previous year that was not detected. Instead of seeing conventional oncologists for a reliable diagnosis and effective treatments, the parents consulted private doctors. Instead of chemotherapy, radiation, and surgery, the girl had deliberately chosen “alternative treatments” herself, the lawyer stressed.
Even though the case has been reported in several Austrian papers, I did not succeed in finding further details about it. In particular, it is unclear what type of cancer the girl had been suffering from and what type of SCAMs she received.
The Austrian skeptic Christian Kreil commented: “Sugar pills in the pharmacies, homeopathic advanced training for doctors, a proliferation of energetics offering every conceivable bullshit … the dead girl is the logical result of this esoteric foolishness covered by politics and chambers.”
I am afraid that he might have a point here: as we have discussed repeatedly on this blog, Austria is currently particularly prone to misinformation about SCAM. Here are a few examples of previous blog posts on this subject:
- Austrian osteopaths seem to violate legal, ethical and moral rules and conventions
- An open letter to the President of the Austrian Medical Association aims to stop medical quackery
- Has the ‘Vienna Medical Association’ taken leave of its senses?
- When politicians become snake-oil salesmen
- Michael Frass’ research into homeopathy for cancer: “numerous breaches of scientific integrity”
- A well-known opponent of vaccination has died of COVID after self-treatment with MMS
- The case of a boy tortured to death with homeopathy
- A truly perplexing homeopath – is it time for an official investigation?
Misinformation about SCAM can be lethal. This is one of the reasons why responsible information is so very important.
Seventeen years after S.K. lost his thyroid gland to cancer, he was promised a miracle by Kyung Chun Oh, an acupuncturist based in the Toronto area: acupuncture could regrow the vital organ. Oh told his patient it would only work if S.K. stopped the thyroid medication he’d been on since his surgery in 2003.
Within just a few months the patient had to be admitted to hospital with a life-threatening case of hypothyroidism. His thyroid had not regenerated. “It was fortunate that the patient did not die,” a college panel wrote in a disciplinary decision, suspending Oh’s license for 12 months. “Telling the patient that he should not take his thyroid medication was irresponsible and had disastrous repercussions.”
The panel found that Oh had engaged in professional misconduct in multiple ways:
- he had provided unnecessary treatment,
- he had failed to advise his patient to consult a medical doctor when he learned that S.K. was suffering
from symptoms that he knew or ought to have known indicated an urgent medical problem, - he had treated a condition that he ought to have known that he did not have the knowledge, skills, or judgment to treat,
- he had failed to keep records in accordance with the standards of the profession,
- he had falsified a record relating to his practice,
- he had made a claim about a treatment that could not be supported by reasonable professional opinion (the claim that acupuncture combined with cessation of thyroid medicine could regrow a surgically removed thyroid gland, and the claim that S.K.’s thyroid gland was regrowing).
This is clearly an extreme incidence of misconduct and one would hope that such cases occur only rarely. But looking at the points listed above, I get the feeling that similar yet less severe cases of misconduct happen regularly in the practices of SCAM practitioners:
- most so-called alternative medicine (SCAM) treatments are unnecessary,
- SCAM practitioners refer patients only rarely to doctors,
- SCAM practitioners often treat conditions that they fail to understand adequately,
- SCAM practitioners frequently make unreasonable claims.