bogus claims
In so-called alternative medicine (SCAM) – but certainly not just there – we regularly encouter reports about new research results that sound odd, implausible, too good to be true, or outright fantastic (like borne out of fantasy). What should one do with such news? Keep an open mind, yes sure, but what if the news leads us up the garden path? Here is what I usually do and what I recommend you might do as well:
- Check who published the story; some sources are clearly more trustworthy than others (think of ‘Natural News‘, or WDDTY, for instance).
- Try to find other outlets confirming the news; if none can be located, be extra sceptical.
- Identify the origin of the new research; an academic might be more trustworthy that a SCAM practitioner or a commercial firm.
- Find out where the study was originally published; some SCAM journals publish virtually any rubbish (think of EBCAM or JCAM).
- If you are still in doubt and continue to be interested, go on Medline and obtain the original article.
- If it’s behind a pay-wall, email the authors for a copy.
- Check the validity of the paper; this can be rather a big task for someone not trained in critical assessment of scientific papers, but there are certain pointers: in case of a clinical trial, for instance, check whether it was large or small, randomised or not, placebo-controlled or not, blind or not.
- If the findings look suspicious to you, find out more about the researchers: for example, do they have a track record of publishing results that look false-positive (think of M Frass or other members of the ‘ALTERNATIVE MEDICINE HALL OF FAME‘, for instance)?
- Identify studies by other researchers addressing the same research question; have similar findings been published, or do most of the previous investigations contradict the results of the new study?
- Find out who sponsored the new study.
- Look up what the authors declare in terms of conflicts of interest.
- If all of this leaves important questions unanswered, don’t be shy, write to the authors and ask.
When I have gone through all these steps, I usually have a fairly clear impression whether I can trust the research or not. Obviously keeping an open mind about new discoveries is sensible. But please. do remember that charlatans might (and often do) put a lot of BS in your mind, if you open it too wide for too long.
It has been reported that Karnataka’s Deputy Chief Minister, Dr CN Ashwathnarayan, has launched eight products, several of which fall in the category of so-called alternative medicine (SCAM), aimed at mitigating COVID-19, developed by various start-ups at Bangalore Bioinnovation Centre (BBC). Dr CN Ashwathnarayan said the launch of the products shows that Karnataka has emerged as a leading state in developing solutions to fight the COVID 19 pandemic.
Here are short descriptions of the innovations:
- Padma Vitals +: Developed by Innovator start-up Dr. Madan Gopal of Cardiac Design labs,Padma Vitals + is a centralized monitoring system for ECG, respiration, Spo2 and body temperature, which can measure the vitals continuously and the analysis sent through telemetry, with an alerting system embedded in it. The device is much needed for contactless monitoring of patients during COVID 19 Pandemic. The product has been validated at Narayana Hrudayalaya.
- Malli’s Cordytea: Developed by Dr. Moushmi Mondal from Mallipatra Neutraceuticals, this product is an Immunity booster tea prepared from medicinal mushroom – Cordyceps. The mushroom variety grown under laboratory conditions is developed by the Innovator. Cordicepin, an active ingredient is known to have anti-viral properties too. In the COVID 19 times, it will be helpful in boosting the immunity levels. The product has been patented and is approved by FSSAI.
- CD4 Shield : Developed by Dr. Vijay Lanka and his team from Stabicon, this product is a chewable tablet containing curcumin and Vitamin B12. Both the ingredients fight inflammation and infection. The product ensures activation of innate immunity by activating CD4+, CD8+ and IFN 1 to virus specific effect and has immunomodulatory properties. It also reduces cytokine storm in response to viral infection. The product is approved by FSSAI.
- BeamRoti : Developed by Dr. Srinivas from Aspartika, the product is an immunity booster chapati having mixture of herbs recommended by AYUSH ministry. The ingredients have been prepared using supercritical fluid extraction technology to ensure optimum concentration of herbal extract reaches the body. The chapatis are easy to store with good shelf life and Patent application has been filed. The product is approved by FSSAI.
- Immune booster daily drops: Developed by Dr. Srinivas from Aspartika, the product is an immunity booster drop having mixture of herbs recommended by AYUSH ministry. The ingredients have been prepared using supercritical fluid extraction technology to ensure optimum concentration of herbal extract reaches the body by mixing just one drop of the product in a glass of hot water. The product is approved by FSSAI.
- VegPhal – Fruit and Vegetable Sanitizer: Developed by Deepak Bhajantri from Krimmi Biotech, this fruit and vegetable sanitizer is prepared using edible ingredients effective against microbes and removal of pesticides. It is chorine and alcohol free.
- Water Sanitizer – Kitchen Tap: The product is developed by Ravi Kumar from Biofi and is a miniaturized version of UV purifier that can be attached to a water tap and kill 99% of microbes including viruses such as phages.
- nti-Micobial HVAC module: The product is developed by Ravi Kumar from Biofi and is a module that can be fitted to HVAC system to ensure circulating air is sanitized. This is especially useful during COVID 19 times as many enclosed spaces in which AC circulated air may be contaminated. Based on UV-silver titanium dioxide technology, the product is patented and has been validated.
Karnataka is of course a state in the south western region of India. The region has so far about one million COVID-19 cases, while almost 12 000 people have died. One would therefore very much hope that the newly launched innovations can make a difference.
But will they?
As far as the SCAM-related products (e.g. ‘immune boosters’) are concerned, I see no convincing evidence to assume that they are effective. If anyone has information to the contrary, please let me know.
But why not? They can’t do any harm!
Sadly, I am am not so sure. I see the potential for considerable harm from all the useless SCAMs that are being promoted left right and centre for protecting the public against COVID-19. Firstly, there is the financial harm of paying for products that are useless. Secondly, ineffective effords might distract from finding and adhering to efforts that are effective. Thirdly, believing in a SCAM that does not work will create a sense of false security which, in turn, renders consumers more vulnerable to catch the virus.
As always in healthcare, even harmless interventions that do not work can become dangerous, as they lead to neglecting effective measures. I shudder to think of how many deaths have been caused by the many SCAM merchants who see the current pandemic as an opportunity.
Numerous so-called alternative medicines (SCAMs) have been touted as the solution for COVID-19. In fact, it is hard to find a SCAM that is not claimed to be useful for corona patients. Crucially, such claims are being made in the complete absence of evidence. A recent paper offers a bibliometric analysis of global research trends at the intersection of SCAM and COVID-19.
SCOPUS, MEDLINE, EMBASE, AMED and PSYCINFO databases were searched on July 5, 2020. All publication types were included, however, articles were only deemed eligible, if they made mention of one or more SCAMs for the potential prevention, treatment, and/or management of COVID-19 or a health issue indirectly resulting from the COVID-19 pandemic. The following eligible article characteristics were extracted: title; author names, affiliations, and countries; DOI; publication language; publication type; publication year; journal (and whether it is TICAM-focused); 2019 impact factor, and TICAMs mentioned.
A total of 296 eligible articles were published by 1373 unique authors at 977 affiliations across 56 countries. The most common countries associated with author affiliation included:
- China,
- the United States,
- India,
- Italy.
Four journals had published more that 10 papers each on the subject:
- Chinese Traditional and Herbal Drugs,
- Journal of Biomolecular Structure & Dynamics,
- Zhongguo Zhongyao Zazhi (China Journal of Chinese Materia Medica),
- Pharmacological Research
The vast majority of articles were published in English, followed by Chinese. Eligible articles were published across 157 journals, of which 33 were SCAM-focused; a total of 120 journals had a 2019 impact factor, which ranged from 0.17 to 60.392. A total of 327 different SCAMs were mentioned across eligible articles, with the most common ones including:
- traditional Chinese medicine (n = 94),
- vitamin D (n = 67),
- melatonin (n = 16),
- phytochemicals (n = 12),
- general herbal medicine (n = 11).

The Canadian author concluded that this study provides researchers and clinicians with a greater knowledge of the characteristics of articles that been published globally at the intersection of COVID-19 and SCAM to date. At a time where safe and effective vaccines and medicines for the prevention and treatment of COVID-19 have yet to be discovered, this study provides a current snapshot of the quantity and characteristics of articles written at the intersection of SCAM therapies and COVID-19.
If anyone repeated the research today, I fear that the number of different SCAMs would have at least doubled. There is simply no form of SCAM that would not have joined the bandwagon of snake-oil salesmen trying to make a quick buck or satisfying their dangerous delusion of a panacea. Today (11/12/2020) my very quick Medline search on just a few SCAMs resulted in the following:
- Herbal medicine: 253
- Dietary supplement: 139
- Acupuncture: 68
- Homeopathy (not mentioned at all above): 20
- Chiropractic: 13
- Naturopathy: 6
One of the most chilling reads during my ‘rough and ready’ trawl through the literature was an article co-authored by a Viennese professor who has featured repeatedly on this blog. Here is its abstract:
Successful homeopathic prescriptions are based on careful individualization of symptoms, either for an individual patient or collectively in the case of epidemic outbreaks. The ongoing COVID-19 pandemic was initially represented as a severe acute respiratory illness, with eventual dramatic complications. However, over time it revealed to be a complex systemic disease with manifestations derived from viral-induced inflammation and hypercoagulability, thus liable to affect any body organ or system. As a result, clinical presentation is variable, in addition to variations associated with several individual and collective risk factors. Given the extreme variability of pathology and clinical manifestations, a single, or a few, universal homeopathic preventive Do not split medicine(s) do not seem feasible. Yet homeopathy may have a relevant role to play, inasmuch as the vast majority of patients only exhibit the mild form of disease and are indicated to self-care at home, without standard monitoring, follow-up, or treatment. For future pandemics, homeopathy agencies should prepare by establishing rapid-response teams and efficacious lines of communication.
The Canadian author of the above paper did not analyse how many of the papers he included would make therapeutic claims. I suspect that the majority did. In this context, one of the clearest indications of how deluded SCAM practitioners tend to be during these difficult times was provided by this paper:
Coronavirus disease 2019 (COVID-19), caused by a new coronavirus, first appeared in late 2019. What initially seemed to be a mild influenza quickly revealed itself as a serious and highly contagious disease, and the planet was soon faced with a significant morbidity and mortality associated with this pathogen. For homeopathy, shunned during its 200 years of existence by conventional medicine, this outbreak is a key opportunity to show potentially the contribution it can make in treating COVID-19 patients. This should be done through performance of impeccably controlled, prospective, randomized clinical trials, with publication of their findings in well-ranked conventional medicine journals. If the homeopathy community fails to take advantage of this rare opportunity, it might wait another century for the next major pandemic.
I must admit, I felt vaguely sick while reading it.
Bloodletting has been used for centuries in many cultures. Its principle, it was assumed, consisted in re-balancing the body’s four humours. Bloodletting had a detrimental effect on most diseases and must have killed millions. It is a good historical example of the harm that ensues, if healthcare adheres to dogma. Today, we know that bloodletting is useful only in rare conditions such as polycythaemia vera or haemochromatosis (and some 30 years ago, a variation of bloodletting, isovolaemic haemodilution, was being discussed as a treatment for circulatory diseases such as intermittent claudication or stroke).
Yet, in so-called alternative medicine (SCAM), there are some practitioners who seem to find it hard to concede that ancient treatments might be not as good as they think. Thus, bloodletting has survived in this realm as a therapy for a wide range of conditions. This study assessed the efficacy of bloodletting therapy (acupoint pricking and cupping) in patients with chronic idiopathic urticaria (CIU) in a randomized, control, parallel-group trial.
A total of 174 patients with CIU were randomized into three groups:
- group A was treated with bloodletting therapy and ebastine (an anti-histamine),
- group B was treated with placebo treatment (acupoint pseudopricking and cupping) and ebastine,
- group C was treated with ebastine only.
The treatment period lasted 4 weeks. An intention-to-treat analysis was conducted, and the primary outcome was the effective rate of UAS7 score being reduced to 7 or below after treatment phase.
The effective rates at the end of treatment phase were different among the three groups, which were
- 73.7% in group A,
- 45.6% in group B,
- and 42.9% in group C.
Multiple analysis indicated differences between groups A and B (P < 0.0125) and groups A and C (P < 0.0125) and no difference between groups B and C (P > 0.0125). No severe bloodletting therapy-related adverse events were observed.
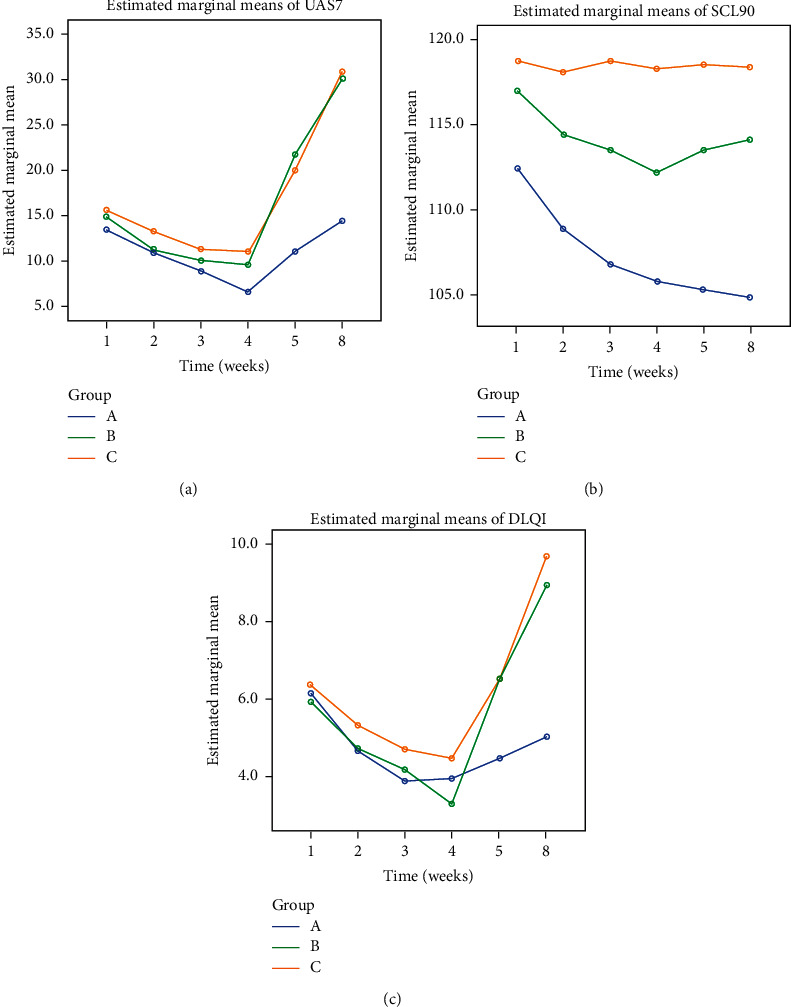
The authors concluded that one month of bloodletting therapy combined with ebastine is clinically beneficial compared with placebo treatment combined with ebastine and treatment with ebastine only. Thus, bloodletting therapy can be an effective complementary treatment in CIU.
Amazed?
Me too!
How on earth might bloodletting help for CIU? Luckily, the authors have an answer to this question:
The clinical feature of urticaria with wheals and pruritus coming and going quickly is the manifestation of wind-evil that lurks in and circulates with blood. Hence, in the treatment of urticaria, dispersing wind is the one of the principle methods, and treating blood before wind is an important procedure because when blood flows fluently , wind-evil will resolve spontaneously. Bloodletting therapy is a direct and effective way of regulating blood.
You see, it’s all perfectly clear!
In this case, the results must be true. And the argument that patients might have known in which treatment group they had ended up (and were thus not blinded) can be discarded.
I was alerted to an interview published in an anthroposophical journal with Prof. Dr. med. Harald Matthes. He is the clinical director of the ‘Gemeinschaftskrankenhauses Havelhöhe‘, a hospital of anthroposophic medicine in Berlin where apparently some COVID-19 patients are presently being treated. Anthroposophic medicine is a medical cult created by the mystic, Rudolf Steiner, about 100 years ago that lacks a basis in science, facts or common sense. Here is the two passages from that interview that I find most interesting (my translation/explanation is below):
Es gibt bisher kein spezifisches Covid-19 Medikament aus der konventionellen Medizin. Remdesivir führt in Studien zu keinem signifikant verbesserten Überleben, sondern lediglich zu einer milden Symptomreduktion. Die anfänglich große Studie vor allem an Universitätskliniken mit Hydrochloroquin und Azithromycin erbrachte sogar eine Steigerung der Todesrate. Daher haben anthroposophische Therapiekonzepte mit Steigerung der Selbstheilungskräfte eine große Bedeutung erfahren. Wichtige anthroposophische Arzneimittel waren dabei das Eisen als Meteoreisen oder als Ferrum metallicum praep., der Phosphor, das Stibium sowie das Cardiodoron® und Pneumodoron®, aber auch Bryonia (Zaunrübe) und Tartarus stibiatus (Brechweinstein). Die Erfolge waren sehr gut, da in Havelhöhe bisher kein Covid-19 Patient verstorben ist, bei einer sonstigen Sterblichkeit von ca. 30% aller Covid-19-Intensivpatienten…
100 Jahre Bazillentheorie und die Dominanz eines pathogenetischen Medizinkonzeptes haben zu der von Rudolf Steiner bereits 1909 vorausgesagten Tyrannei im Sozialen geführt. Der Mensch hat ein Mikrobiom und Virom, das unverzichtbar für seine Immunität ist und von der Quantität mächtiger als der Mensch selbst (Mikrobiom 1014 Bakterien mit ca. 1200 Spezies z.B. im Darm bei nur 1012 Körperzellen).
Matthes explains that, so far, no medication has been demonstrated to be effective against COVID-19 infections. Then he continues: “This is the reason why anthroposophic therapies which increase the self-healing powers have gained great importance”, and names the treatments used in his hospital:
- Meteoric Iron (a highly diluted anthroposophic remedy based on iron from meteors),
- Ferrum metallicum praep. (a homeopathic/anthroposophic remedy based on iron),
- Phosphor (a homeopathic remedy based on phosphor),
- Stibium (a homeopathic remedy based on antimony),
- Cardiodoron (a herbal mixture used in anthroposophical medicine),
- Pneumodoron (a herbal mixture used in anthroposophical medicine containing).
Matthes also affirms (my translation):
“The success has so far been very good, since no COVID-19-patient has died in Havelhöhe – with a normal mortality of about 30% of COID_19 patients in intensive care…
100 years of germ theory and the dominance of a pathogenetic concept of medicine have led to the tyranny in the social sphere predicted by Rudolf Steiner as early as 1909. Humans have a microbiome and virom that is indispensable for their immunity and more powerful in quantity than humans themselves (microbiome 1014 bacteria with about 1200 species e.g. in the intestine with only 1012 somatic cells)…”
_________________
The first 4 remedies listed above are highly diluted and contain no active molecules. The last two are less diluted and might therefore contain a few active molecules but in sub-therapeutic doses. Crucially, none of the remedies have been shown to be effective for any condition.
The germ theory of disease which Matthes mentions is, of course, a bit more than a ‘theory’; it is the accepted scientific explanation for many diseases, including COVID-19.
I have cold sweats when I think of anthroposophical doctors who seem to take it less than seriously, while treating desperately ill COVID-19 patients. If I were allowed to ask just three questions to Matthes, I think, it would be these:
- How did you obtain fully informed consent from your patients, including the fact that your remedies are unproven and implausible?
- If you think your results are so good, are you monitoring them closely to publish them urgently, so that other centres might learn from them?
- Do you feel it is ethical to promote unprovn treatments during a health crisis via a publicly available interview before your results have been formally assessed and published?
Acupuncture-moxibustion therapy (AMT) is a so-called alternative medicine (SCAM) that has been used for centuries in treatment of numerous diseases. Some enthusiasts even seem to advocate it for chemotherapy-induced leukopenia (CIL) The purpose of this review was to evaluate the efficacy and safety of acupuncture-moxibustion therapy in treating CIL.
Relevant studies were searched in 9 databases up to September 19, 2020. Two reviewers independently screened the studies for eligibility, extracted data, and assessed the methodological quality of selected studies. Meta-analysis of the pooled mean difference (MD) and risk ratio (RR) with their respective 95% confidence intervals (CI) were calculated.
Seventeen studies (1206 patients) were included, and the overall quality of the included studies was moderate. In comparison with medical therapy, AMT has a better clinical efficacy for CIL (RR, 1.24; 95% CI, 1.17-1.32; P < 0.00001) and presents advantages in increasing leukocyte count (MD, 1.10; 95% CI, 0.67-1.53; P < 0.00001). Also, the statistical results show that AMT performs better in improving the CIL patients’ Karnofsky performance score (MD, 5.92; 95% CI, 3.03-8.81; P < 0.00001).
The authors concluded that this systematic review and meta-analysis provides updated evidence that AMT is a safe and effective alternative for the patients who suffered from CIL.
A CIL is a serious complication. If I ever were afflicted by it, I would swiftly send any acupuncturist approaching my sickbed packing.
But this is not an evidence-based attitude!!!, I hear some TCM-fans mutter. What more do you want that a systematic review showing it works?
I beg to differ. Why? Because the ‘evidence’ is hardly what critical thinkers can accept as evidence. Have a look at the list of the primary studies included in this review:
- Lin Z. T., Wang Q., Yu Y. N., Lu J. S. Clinical observation of post-chemotherapy-leukopenia treated with ShenMai injectionon ST36. World Journal of Integrated Traditional and Western Medicine. 2010;5(10):873–876. [Google Scholar]
- Wang H. Clinical Observation of Acupoint Moxibustion on Leukopenia Caused by Chemotherapy. Beijing, China: Beijing University of Chinese Medicine; 2011. [Google Scholar]
- Fan J. Y. Coupling of Yin and Yang between Ginger Moxibustion Improve the Clinical Effect of the Treatment of Chemotherapy Adverse Reaction. Henan, China: Henan University of Chinese Medicine; 2013. [Google Scholar]
- Lu D. R., Lu D. X., Wei M., et al. Acupoint injection with addie injection for patients of nausea and vomiting with cisplatin induced by chemotherapy. Journal of Clinical Acupuncture and Moxibustion. 2013;29(10):33–38. [Google Scholar]
- Yang J. E. The Clinical Observation on Treatment of Leukopenia after Chemotherapy with Needle Warming Moxibustion. Hubei, China: Hubei University of Chinese Medicine; 2013. [Google Scholar]
- Fu Y. H., Chi C. Y., Zhang C. Y. Clinical effect of acupuncture and moxibustion on leukopenia after chemotherapy of malignant tumor. Guide of China Medicine. 2014;12(12) [Google Scholar]
- Wang J. N., Zhang W. X., Gu Q. H., Jiao J. P., Liu L., Wei P. K. Protection of herb-partitioned moxibustion on bone marrow suppression of gastric cancer patients in chemotherapy period. Chinese Archives of Traditional Chinese Medicine. 2014;32(12):110–113. [Google Scholar]
- Zhang J. The Clinical Research on Myelosuppression and Quality of Life after Chemotherapy Treated by Grain-Sized Moxibustion. Nanjing, China: Nanjing University of Chinese Medicine; 2014. [Google Scholar]
- Tian H., Lin H., Zhang L., Fan Z. N., Zhang Z. L. Effective research on treating leukopenia following chemotherapy by moxibustion. Clinical Journal of Chinese Medicine. 2015;7(10):35–38. [Google Scholar]
- Hu G. W., Wang J. D., Zhao C. Y. Effect of acupuncture on the first WBC reduction after chemotherapy for breast cancer. Beijing Journal of Traditional Chinese Medicine. 2016;35(8):777–779. [Google Scholar]
- Zhu D. L., Lu H. Y., Lu Y. Y., Wu L. J. Clinical observation of Qi-blood-supplementing needling for leukopenia after chemotherapy for breast cancer. Shanghai Journal of Acupuncture and Moxibustion. 2016;35(8):964–966. [Google Scholar]
- Chen L, Xu G. Y. Observation on the prevention and treatment of chemotherapy-induced leukopenia by moxibustion therapy. Zhejiang Journal of Traditional Chinese Medicine. 2016;51(8):p. 600. [Google Scholar]
- Mo T., Tian H., Yue S. B., Fan Z. N., Zhang Z. L. Clinical observation of acupoint moxibustion on leukocytopenia caused by tumor chemotherapy. World Chinese Medicine. 2016;11(10):2120–2122. [Google Scholar]
- Nie C. M. Nursing observation of acupoint moxibustion in the treatment of leucopenia after chemotherapy. Today Nurse. 2017;4:93–95. [Google Scholar]
- Wang D. Y. Clinical Research on Post-chemotherapy-leukopenia with Spleen-Kidney Yang Deficiency in Colorectal Cancer Treated with Point-Injection. Yunnan, China: Yunnan University of Chinese Medicine; 2017. [Google Scholar]
- Gong Y. Q, Zhang M. Q, Zhang B. C. Prevention and treatment of leucocytopenia after chemotherapy in patients with malignant tumor with ginger partitioned moxibustion. Chinese Medicine Modern Distance Education of China. 2018;16(21):135–137. [Google Scholar]
- Li Z. C., Lian M. J., Miao F. G. Clinical observation of fuzheng moxibustion combined with wenyang shengbai decoction in the treatment of 80 cases of leukopenia after chemotherapy. Hunan Journal of Traditional Chinese Medicine. 2019;35(3):64–66. [Google Scholar]
Notice anything peculiar?
- The studies are all from China where data fabrication was reported to be rife.
- They are mostly unavailable for checking (why the published adds links that go nowhere is beyond me).
- Many do not look at all like randomised clinical trials (which, according to the authors, was an inclusion criterion).
- Many do not look as though their primary endpoint was the leukocyte count (which, according to the authors, was another inclusion criterion).
Intriguingly, the authors conclude that AMT is not just effective but also ‘safe’. How do they know? According to their own data extraction table, most studies failed to mention adverse effects. And how exactly is acupuncture supposed to increase my leukocyte count? Here is what the authors offer as a mode of action:
I think it is high time that we stop tolerating that the medical literature gets polluted with such nonsense (helped, of course, by journals that are beyond the pale) – someone might actually believe it, in which case it would surely hasten the death of vulnerable patients.
Some consumers believe that research is by definition reliable, and patients are even more prone to this error. When they read or hear that ‘RESEARCH HAS SHOWN…’ or that ‘A RECENT STUDY HAS DEMONSTRATED…’, they usually trust the statements that follow. But is this trust in research and researchers justified? During 25 years that I have been involved in so-called alternative medicine (SCAM), I have encountered numerous instances which make me doubt. In this post, I will briefly discuss some the many ways in which consumers can be mislead by apparently sound evidence (for an explanation as to what is and what isn’t evidence, see here).
ABSENCE OF EVIDENCE
I have just finished reading a book by a German Heilpraktiker that is entirely dedicated to SCAM. In it, the author makes hundreds of statements and presents them as evidence-based facts. To many lay people or consumers, this will look convincing, I am sure. Yet, it has one fatal defect: the author fails to offer any real evidence that would back up his statements. The only references provided were those of other books which are equally evidence-free. This popular technique of making unsupported claims allows the author to make assertions without any checks and balances. A lay person is usually unable or unwilling to differentiate such fabulations from evidence, and this technique is thus easy and poular for misleading us about SCAM.
FAKE-EVIDENCE
On this blog, we have encountered this phenomenon ad nauseam: a commentator makes a claim and supports it with some seemingly sound evidence, often from well-respected sources. The few of us who bother to read the referenced articles quickly discover that they do not say what the commentator claimed. This method relies on the reader beeing easily bowled over by some pretend-evidence. As many consumers cannot be bothered to look beyond the smokescreen supplied by such pretenders, the method usually works surprisingly well.
An example: Vidatox is a homeopathic cancer ‘cure’ from Cuba. The Vidatox website clains that it is effective for many cancers. Considering how sensational this claim is, one would expect to find plenty of published articles on Vidatox. However, a Medline search resulted in one paper on the subject. Its authors drew the following conclusion: Our results suggest that the concentration of Vidatox used in the present study has not anti-neoplastic effects and care must be taken in hiring Vidatox in patients with HCC.
The question one often has to ask is this: where is the line between misleading research and fraud?
SURVEYS
There is no area in healthcare that produces more surveys than SCAM. About 500 surveys are published every year! This ‘survey-mania’ has a purpose: it promotes a positive message about SCAM which hypothesis-testing research rarely does.
For a typical SCAM survey, a team of enthusiastic researchers might put together a few questions and design a questionnaire to find out what percentage of a group of individuals have tried SCAM in the past. Subsequently, the investigators might get one or two hundred responses. They then calculate simple descriptive statistics and demonstrate that xy % use SCAM. This finding eventually gets published in one of the many third-rate SCAM journals. The implication then is that, if SCAM is so popular, it must be good, and if it’s good, the public purse should pay for it. Few consumers would realise that this conclusion is little more that a fallacious appeal to popularity.
AVOIDING THE QUESTION
Another popular way of SCAM researchers to mislead the public is to avoid the research questions that matter. For instance, few experts would deny that one of the most urgent issues in chiropractic relates to the risk of spinal manipulations. One would therefore expect that a sizable proportion of the currently published chiropractic research is dedicated to it. Yet, the opposite is the case. Medline currently lists more than 3 000 papers on ‘chiropractic’, but only 17 on ‘chiropractic, harm’.
PILOT-STUDIES
A pilot study is a small scale preliminary study conducted in order to evaluate feasibility, time, cost, adverse events, and improve upon the study design prior to performance of a full-scale research project. Yet, the elementary preconditions are not fulfilled by the plethora of SCAM pilot studies that are currently being published. True pilot studies of SCAM are, in fact, very rare. The reason for the abundance of pseudo-pilots is obvious: they can easily be interpreted as showing encouragingly positive results for whatever SCAM is being tested. Subsequently, SCAM proponents can mislead the public by claiming that there are plenty of positive studies and therefore their SCAM is supported by sound evidence.
‘SAFE‘ STUDY-DESIGNS
As regularly mentioned on this blog, there are several ways to design a study such that the risk of producing a negative result is minimal. The most popular one in SCAM research is the ‘A+B versus B’ design. In this study, for instance, cancer patients who were suffering from fatigue were randomised to receive usual care or usual care plus regular acupuncture. The researchers then monitored the patients’ experience of fatigue and found that the acupuncture group did better than the control group. The effect was statistically significant, and an editorial in the journal where it was published called this evidence “compelling”. Due to a cleverly over-stated press-release, news spread fast, and the study was celebrated worldwide as a major breakthrough in cancer-care.
Imagine you have an amount of money A and your friend owns the same sum plus another amount B. Who has more money? Simple, it is, of course your friend: A+B will always be more than A [unless B is a negative amount]. For the same reason, such “pragmatic” trials will always generate positive results [unless the treatment in question does actual harm]. Treatment as usual plus acupuncture is more than treatment as usual alone, and the former is therefore more than likely to produce a better result. This will be true, even if acupuncture is a pure placebo – after all, a placebo is more than nothing, and the placebo effect will impact on the outcome, particularly if we are dealing with a highly subjective symptom such as fatigue.
A more obvious method for generating false positive results is to omit blinding. The purpose of blinding the patient, the therapist and the evaluator of the group allocation in clinical trials is to make sure that expectation is not a contributor to the result. Expectation might not move mountains, but it can certainly influence the result of a clinical trial. Patients who hope for a cure regularly do get better, even if the therapy they receive is useless, and therapists as well as evaluators of the outcomes tend to view the results through rose-tinted spectacles, if they have preconceived ideas about the experimental treatment.
Failure to randomise is another source of bias which can mislead us. If we allow patients or trialists to select or chose which patients receive the experimental and which get the control-treatment, it is likely that the two groups differ in a number of variables. Some of these variables might, in turn, impact on the outcome. If, for instance, doctors allocate their patients to the experimental and control groups, they might select those who will respond to the former and those who don’t to the latter. This may not happen with intent but through intuition or instinct: responsible health care professionals want those patients who, in their experience, have the best chances to benefit from a given treatment to receive that treatment. Only randomisation can, when done properly, make sure we are comparing comparable groups of patients. Non-randomisation can easily generate false-positive findings.
It is also possible to mislead people with studies which do not test whether an experimental treatment is superior to another one (often called superiority trials), but which assess whether it is equivalent to a therapy that is generally accepted to be effective. The idea is that, if both treatments produce similarly positive results, both must be effective. Such trials are called non-superiority or equivalence trials, and they offer a wide range of possibilities for misleading us. If, for example, such a trial has not enough patients, it might show no difference where, in fact, there is one. Let’s consider a simple, hypothetical example: someone comes up with the idea to compare antibiotics to acupuncture as treatments of bacterial pneumonia in elderly patients. The researchers recruit 10 patients for each group, and the results reveal that, in one group, 2 patients died, while, in the other, the number was 3. The statistical tests show that the difference of just one patient is not statistically significant, and the authors therefore conclude that acupuncture is just as good for bacterial infections as antibiotics.
Even trickier is the option to under-dose the treatment given to the control group in an equivalence trial. In the above example, the investigators might subsequently recruit hundreds of patients in an attempt to overcome the criticism of their first study; they then decide to administer a sub-therapeutic dose of the antibiotic in the control group. The results would then seemingly confirm the researchers’ initial finding, namely that acupuncture is as good as the antibiotic for pneumonia. Acupuncturists might then claim that their treatment has been proven in a very large randomised clinical trial to be effective for treating this condition. People who do not happen to know the correct dose of the antibiotic could easily be fooled into believing them.
Obviously, the results would be more impressive, if the control group in an equivalence trial received a therapy which is not just ineffective but actually harmful. In such a scenario, even the most useless SCAM would appear to be effective simply because it is less harmful than the comparator.
A variation of this theme is the plethora of controlled clinical trials in SCAM which compare one unproven therapy to another unproven treatment. Perdicatbly, the results would often indicate that there is no difference in the clinical outcome experienced by the patients in the two groups. Enthusiastic SCAM researchers then tend to conclude that this proves both treatments to be equally effective. The more likely conclusion, however, is that both are equally useless.
Another technique for misleading the public is to draw conclusions which are not supported by the data. Imagine you have generated squarely negative data with a trial of homeopathy. As an enthusiast of homeopathy, you are far from happy with your own findings; in addition you might have a sponsor who puts pressure on you. What can you do? The solution is simple: you only need to highlight at least one positive message in the published article. In the case of homeopathy, you could, for instance, make a major issue about the fact that the treatment was remarkably safe and cheap: not a single patient died, most were very pleased with the treatment which was not even very expensive.
OMISSION
A further popular method for misleading the public is the outright omission findings that SCAM researchers do not like. If the aim is that the public believe the myth that all SCAM is free of side-effects, SCAM researchers only need to omit reporting them in clinical trials. On this blog, I have alerted my readers time and time again to this common phenomenon. We even assessed it in a systematic review. Sixty RCTs of chiropractic were included. Twenty-nine RCTs did not mention adverse effects at all. Sixteen RCTs reported that no adverse effects had occurred. Complete information on incidence, severity, duration, frequency and method of reporting of adverse effects was included in only one RCT.
Most trails have many outcome measures; for instance, a study of acupuncture for pain-control might quantify pain in half a dozen different ways, it might also measure the length of the treatment until pain has subsided, the amount of medication the patients took in addition to receiving acupuncture, the days off work because of pain, the partner’s impression of the patient’s health status, the quality of life of the patient, the frequency of sleep being disrupted by pain etc. If the researchers then evaluate all the results, they are likely to find that one or two of them have changed in the direction they wanted (especially, if they also include half a dozen different time points at which these variables are quatified). This can well be a chance finding: with the typical statistical tests, one in 20 outcome measures would produce a significant result purely by chance. In order to mislead us, the researchers only need to “forget” about all the negative results and focus their publication on the ones which by chance have come out as they had hoped.
FRAUD
When it come to fraud, there is more to chose from than one would have ever wished for. We and others have, for example, shown that Chinese trials of acupuncture hardly ever produce a negative finding. In other words, one does not need to read the paper, one already knows that it is positive – even more extreme: one does not need to conduct the study, one already knows the result before the research has started. This strange phenomenon indicates that something is amiss with Chinese acupuncture research. This suspicion was even confirmed by a team of Chinese scientists. In this systematic review, all randomized controlled trials (RCTs) of acupuncture published in Chinese journals were identified by a team of Chinese scientists. A total of 840 RCTs were found, including 727 RCTs comparing acupuncture with conventional treatment, 51 RCTs with no treatment controls, and 62 RCTs with sham-acupuncture controls. Among theses 840 RCTs, 838 studies (99.8%) reported positive results from primary outcomes and two trials (0.2%) reported negative results. The percentages of RCTs concealment of the information on withdraws or sample size calculations were 43.7%, 5.9%, 4.9%, 9.9%, and 1.7% respectively. The authors concluded that publication bias might be major issue in RCTs on acupuncture published in Chinese journals reported, which is related to high risk of bias. We suggest that all trials should be prospectively registered in international trial registry in future.
A survey of clinical trials in China has revealed fraudulent practice on a massive scale. China’s food and drug regulator carried out a one-year review of clinical trials. They concluded that more than 80 percent of clinical data is “fabricated“. The review evaluated data from 1,622 clinical trial programs of new pharmaceutical drugs awaiting regulator approval for mass production. Officials are now warning that further evidence malpractice could still emerge in the scandal.
I hasten to add that fraud in SCAM research is certainly not confined to China. On this blog, you will find plenty of evidence for this statement, I am sure.
CONCLUSION
Research is obviously necessary, if we want to answer the many open questions in SCAM. But sadly, not all research is reliable and much of SCAM research is misleading. Therefore, it is always necessary to be on the alert and apply all the skills of critical evaluation we can muster.
Recent comments on this blog prompted me to look into a very strange therapeutic and diagnostic device used by some practitioners of so-called alternative medicine (SCAM):
The OBERON provides the most unique tool for scanning the various organs and systems of the physical body without having to make a medical or surgical intrusion. Developed by Russian scientists since the early 1990’s, the OBERON is the most revolutionary computer programmed invention available in the world today for analyzing and treating all the body’s organs and functions.
This device scans each organ or tissue on a cellular level. It compares the measurements to a database of thousands of referenced conditions and their diagnosis. OBERON uses a special emitter to modulate the carrier frequency for the cell communication and it uses special sensor trigger readers built into headphones to read the cells own signals.
OBERON finds out how stressed an organ is, and if there are any diseases developing, how much the cells are influenced by a specific disease, and which micro organisms and bacteria are in the area at the time of the scan.
BENEFITS OF THE OBERON:
Rebalances the body so that it can start to heal itself!
Makes intrusive and embarrassing examinations a THING OF THE PAST!!!!
Quick examination (in seconds) with immediate results
Replaces dozens of traditional diagnostic methods.
Finds weaknesses in the skeleton, organs, blood, tissue, etc.
There are no side effects, unpleasantness or injury after treatment
Bio-resonance META-therapy
A print out of the report on findings can be taken at the end of the session…
The method is based on an analysis of the brain stems electromagnetic waves which contain the complete information of the entire organism. This information is read by a sensor. A frequency transmitter aimed at the projection area of the brain stem stimulates this electromagnetic radiation.
Meta- Therapy repairs the organism using a diversity of modulated electromagnetic waves. This treatment stimulates the body’s own functions so that they solve the problem and it stimulates the immune defense and is a very good supplement or alternative to traditional treatment. The patient can follow on the screen how the organ progressively gets better, and afterwards one can take a new measurement showing the improvement…
________________________________________
Sounds fantastic?
Yes, indeed – fantastic as in fantasy!
Almost as much relation to reality as OBERON, king of the fairies in medieval literature.
The modern OBERON device is being used by infamous proponents of integrated medicine like Dr Julian Kenyon who already made an appearance on this blog. On his website, Kenyon published a paper in which he provides details about the OBERON. To a lay person, the sciency text might look like science; however, this impression would be false. The ‘study’ Kenyon mentioned is not on Medline. In fact, Dr Kenyon (former associate of the late George Lewith) has merely 4 Medline-listed papers:
- Physiological and psychological explanations for the mechanism of acupuncture as a treatment for chronic pain. Soc Sci Med. 1984;19(12):1367-78. doi: 10.1016/0277-9536(84)90026-1.PMID: 6085191 Review.
- Is electrodermal testing as effective as skin prick tests for diagnosing allergies? A double blind, randomised block design study. BMJ. 2001 Jan 20;322(7279):131-4. doi: 10.1136/bmj.322.7279.131.PMID: 11159567 Free PMC article. Clinical Trial.
- Randomised double-blind trial on the immediate effects of naloxone on classical Chinese acupuncture therapy for chronic pain. Acupunct Electrother Res. 1983;8(1):17-24. doi: 10.3727/036012983816715064.PMID: 6135300 Clinical Trial.
- Food sensitivity, a search for underlying causes. Case study of 12 patients. Kenyon JN.Acupunct Electrother Res. 1986;11(1):1-13. doi: 10.3727/036012986816359238.PMID: 2872775
And what about other researchers? Aren’t there ANY decent studies of the OBERON?
Not as far as I can see (if anyone does know of peer-reviewed research, please let me know).
So, what is the conclusion?
My conclusion is this:
There is no evidence that the OBERON does anything useful other than putting money in the bank accounts of those charlatans who use or manufacture it.
And what does that make Kenyon and all the other SCAM practitioners using the OBERON or similar devices?
I leave it to you to decide.
The Center for Science in the Public Interest*** (CSPI) announced its agreement with Boiron to improve the labeling on the homeopathic products manufactured by Boiron and sold under the Boiron or other private label brands. The agreement covers the labeling for over 50 homeopathic products.
On Boiron’s Oscillococcinum and two similar products, Boiron will substantially increase the prominence of the words “Homeopathic Medicine” on the front of the box and the disclaimer on the back of the box that says the product’s uses have not been evaluated by the Food and Drug Administration (FDA). These changes will make it easier for consumers to identify that the products are homeopathic products, and are not FDA approved over-the-counter medicines.
For all of the other homeopathic products manufactured by Boiron, consumers will receive much more information on the packages. In addition to increasing the prominence of the words “Homeopathic Medicine,” a new disclaimer in large and contrasting font will be added to the back of the package (endorsed by the American Association of Homeopathic Pharmacists) stating: “Claims based on traditional homeopathic practice, not accepted medical evidence, and not FDA evaluated.”…
“The labeling changes that Boiron has agreed to on all the products covered by the agreement will help consumers more clearly identify that these are homeopathic products and are not FDA approved over-the-counter medicines that have been scientifically proven to be safe and effective,” said CSPI litigation director Lisa Mankofsky. “In addition, the vast majority of the covered homeopathic products will bear a disclaimer clarifying that they are based on traditional homeopathic practice, not accepted medical evidence, and not FDA evaluated. We think that consumers will find this labeling change important when choosing a remedy. We encourage other manufacturers to similarly make their labels more transparent and clear for consumers.”
Bravo!
Clearly a step into the right direction!
But it’s a small step only. It is a long way short of what Dylan Evans suggestied in his book ‘Placebo‘, first published in 2004:
Warning: this product is a placebo. It will work only if you believe in homeopathy, and only for certain conditions such as pain and depression. Even then, it is not likely to be as powerful as orthodox drugs. You may get fewer side-effects from this treatment than from a drug, but you will probably also get less benefit.
***The Center for Science in the Public Interest is perhaps the oldest independent, science-based consumer advocacy organization with an impressive record of accomplishments and a clear and ambitious agenda for improving the food system to support healthy eating.
There is some encouraging evidence regarding the positive influence of vitamin D on COVID-19. But is it convincing? Is it causal? As always, it is worth looking at the totality of the reliable evidence.
In this systematic review and meta-analysis, the researchers analyze the association between vitamin D deficiency and COVID-19 severity. They conducted an analysis of the prevalence of vitamin D deficiency and insufficiency in people with the disease. Five online databases—Embase, PubMed, Scopus, Web of Science, ScienceDirect and pre-print Medrevix were searched. The inclusion criteria were observational studies measuring serum vitamin D in adult and elderly subjects with COVID-19. The main outcome was the prevalence of vitamin D deficiency in severe cases of COVID-19.
The researchers identified 1542 articles and 27 met their inclusion criteria. The results show that
- vitamin D deficiency was not associated with a higher chance of infection by COVID-19,
- severe cases of COVID-19 present 64% more vitamin D deficiency compared with mild cases,
- vitamin D concentration insufficiency increased hospitalization and mortality rates,
- There was a positive association between vitamin D deficiency and the severity of the disease.
The authors concluded that the results of the meta-analysis confirm the high prevalence of vitamin D deficiency in people with COVID-19, especially the elderly. We should add that vitamin D deficiency was not associated with COVID-19 infection. However, we observed a positive association between vitamin D deficiency and the severity of the disease. From this perspective, evaluating blood vitamin D levels could be considered in the clinical practice of health professionals. Moreover, vitamin D supplementation could be considered in patients with vitamin D deficiency and insufficiency, if they have COVID-19. However, there is no support for supplementation among groups with normal blood vitamin D values with the aim of prevention, prophylaxis or reducing the severity of the disease.
These are interesting findings, no doubt. They relate to associations, as the authors repeatedly stress in the text of the paper. They do not, however, signify cause and effect relationships. The principal outcome of this research should be a hypothesis that subsequently needs testing in clinical trials.
So, why on earth did the authors chose that seriously misleading title of their paper? It clearly implies a causal effect; and this can only be verified by conducting clinical trials. One such study has been published (as discussed here) and it concluded that administration of calcifediol may improve the clinical outcome of subjects requiring hospitalization for COVID-19.
My conclusion: it seems well worth conducting more and more rigorous clinical trials.