Uncategorized
For more than seven months, the Austrian general practitioner, Dr. Lisa-Maria Kellermayr, received death threats and was verbally attacked by the anti-vaccination cult. She eventually closed her practice, no longer wanted to leave the house, and apparently lost the courage to live. Last Friday, she was found dead in her practice in Seewalchen on Attersee. The public prosecutor’s office in Wels confirmed that there were no signs of foul play. Letters of farewell had been found. It is generally assumed that, in her desperation, Kellermayr took her own life. A friend tweeted: “In the end, she begged for help – from politicians, from the police, from her medical association. It never came. The police and the medical association would mock her. They said Dr Kellermayrjust wants to seek the limelight. Politicians ignored her. Now she is dead.”
The GP had closed her practice at the end of June, only temporarily, she said initially, because she could no longer afford the costs for her security, including a bodyguard. She did not feel sufficiently protected by the police. “For more than 7 months, we have been receiving death threats from the Covid measure opponents and vaccination opponents scene at irregular intervals,” Kellermayr tweeted. Threats went as far as predicting a “massacre” in her practice. In one of the threatening letters, the author described in detail how he would first torture and then murder the doctor and her practice staff.
At the end of July, she closed her practice for good. For the doctor, who loved her profession, it was a terrible decision. “I put so much money and energy into it,” she told ‘Der Spiegel’ just one day before her death. By her own account, she had at that stage invested around 100,000 Euros in security measures.
It is claimed that Kellermayr was badly let down by the Austrian authorities. On Austrian radio, the police even stated that Kellermayr merely sought the limelight to further her career. Now an official complaint has been filed charging the authorities with neglect.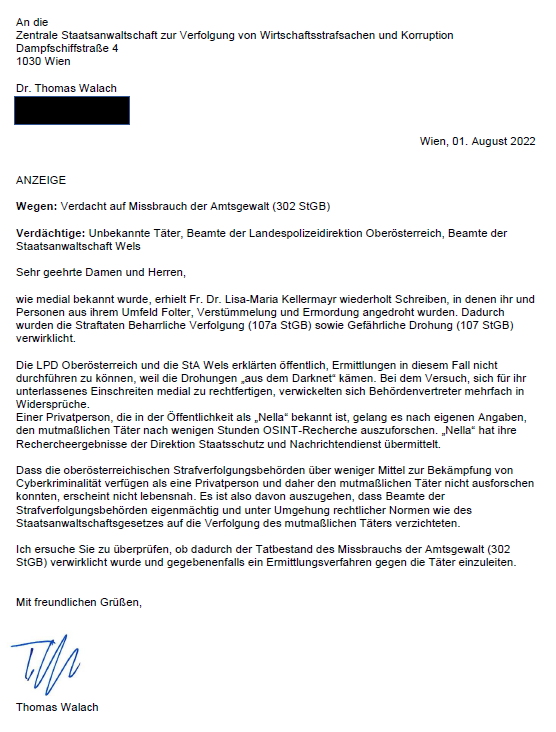
Unbelievably, the despicable agitation of the anti-vaccination cult continues even after Kellermayr’s death. Most of the agitators remain anonymous. But some are also agitating publicly, for instance, on Twitter: Harald Laatsch, an AfD member of parliament in Berlin, wrote that the doctor was a vaccination propagandist and probably “no longer wanted to live with the heavy guilt”.
After Kellermayr’s suicide, well-known German Twitter users are withdrawing from the platform. The Würzburg lawyer Chan-jo Jun turned his back on Twitter last Friday stating: “If I tweet about certain people, I get warnings in my letterbox the next day. I am reaching my limits. I’m now leaving the field to others. Until I find a concept of how an objective exchange can take place in social media.”
Doctor Natalie Grams, a well-known critic of homeopathy, is also closing her Twitter account. She plans to continue her commitment to evidence-based medicine with the help of her podcast, Grams explained in her farewell tweet.
Others reached a different conclusion. Dr. Christian Luebbers tweeted this (my translation): “Of course, I also considered deactivating my account here. However, I came to the conclusion not to do so and continue to educate people about pseudo-medicine and vaccination. I see this as necessary moral courage and will not leave the field to hate.” Personally, I agree with him.
I would like to use the tragic occasion of Dr. Kellermyr’s death as an opportunity for making a plea. It is high time that intolerance, aggression, violence, and hatred stop. Please, let us all calm down and discuss with dignity and respect whatever issues we might have. Please, let this terrible death remind us that we are all human beings. Please, let it be a lesson to all of us.
The DAILY EXPRESS (DE) is not my favorite newspaper – perhaps even the opposite. During the last years, I have often been questioned by journalists on matters relating to so-called alternative medicine (SCAM). I do not recall, however, being interviewed by the DE (I might have forgotten, of course, but it certainly did not happen very often). I was therefore surprised to find that, in the last 13 years (this is as far back as I was able to search), the DE quoted me 22 times. Therefore, I decided to do a quick analysis of these 22 articles rating them (generously) for accuracy on a scale of 0 (totally inaccurate) to 10 (totally accurate).
1. Title (date of publication): Tracking down the safe alternatives (25 March 2008)
Subject: a new regulatory body (the Complementary and Natural Healthcare Council (CNHC)) might help separate the cranks from the credible.
Quote: The CNHC has been described as complementary medicine’s equivalent of the General Medical Council – the body which sets standards for GPs. It will investigate complaints and therapists who fall below expected standards could be struck off. The new organisation has been set up by Prince Charles’s Foundation for Integrated Health and receives part funding from the NHS. The Prince, who is a fan of homeopathy, believes that complementary therapies should have a greater role within the NHS…
Edzard Ernst, the UK’s first professor of complementary medicine, is scathing, describing the £2million cost of founding the CNHC as a waste of money. He says the new body does not challenge the safety or effectiveness of the therapies. “This organisation could give the public false confidence. Some of these therapies can do more harm than good. It will give them a status they don’t deserve.”
My comment (score): The subject matter was relevant. The article seems correct and my comment is true; the CNHC did, in fact, turn out to be a waste of space. (10)
2. Title (date of publication): Chinese Medicine: A risky remedy? (19 May 2008)
Subject: How much do we really know about how they work and could they actually be harmful to our health?
Quote: Traditional Chinese Medicine (TCM) is enjoying a boom with hundreds of shops appearing on high streets. The herbal medicine industry, which includes Chinese medicines, is worth an estimated £200million in the UK as thousands place their faith in ancient remedies for everything from acne to infertility…
Edzard Ernst, professor of complementary medicine at the University of Exeter and co-author of the book Trick Or Treatment: Alternative Medicine On Trial, says: “People think that because something is ancient or natural it must be good. That’s simply not true. Plenty of these medicines have side effects and can be dangerous. “TCMs are grossly under-researched in the UK. China’s research is hard to access and hard to understand. TCMs are frequently contaminated with toxic heavy metals. “This is because of poor quality, because soil is contaminated and supplying procedures are unregulated. The most worrying thing about TCMs is that they are regularly found to contain synthetic prescription drugs, which in extreme cases, taken wrongly, can kill.”
My comment (score): The subject matter was relevant. The article seems correct and my comment is true. (10)
3. Title (date of publication): Alternative treatments face calls for regulation (17 June 2008)
Subject: Alternative medicines must be regulated to protect patients from harm, according to an influential group of experts.
Quote: A government-appointed steering group said it was ridiculous that eight years after regulation was first called for, nothing had been done. And in a report to UK ministers, who have reserved powers on regulating health professionals, they warned it must be introduced “without delay”…
Prof Edzard Ernst, professor of complementary medicine at the University of Exeter, said there was no scientific evidence that homoeopathy works. Homoeopathy is the treatment of disease using minute doses of drugs diluted in water. Prof Ernst and author Simon Singh have pledged to give £10,000 to anyone who could prove, in a scientific way, that these treatments work as well as conventional medicines.
My comment (score): The subject matter was relevant. The article seems a bit confused. My comment seems to be from elsewhere and is out of context. (5)
4. Title (date of publication): Thank you for the music (28 June 2008)
Subject: Nerve disorder fibromyalgia left musician Emily Maguire housebound and in constant pain. As she prepares to play the Glastonbury festival she tells ABIGAIL JACKSON how her love of music pulled her through…
Quote: Dr Peter Fisher from the Royal London Homeopathic Hospital … has claimed to have success in treating fibromyalgia patients with homeopathic remedies. He prescribed ignacia, used as a remedy for numerous complaints from depression and sleeplessness to backache. A month later, Emily says the pain was gone. “I couldn’t believe it,” she says. “I feel so blessed.”
Although Emily is confident that taking ignacia (as well as maintaining a healthy lifestyle) did the trick, there are growing concerns over whether homeopathic remedies have any effect. Last week Edzard Ernst, the UK’s only professor of complementary medicine, offered £10,000 for any proof of a successful homeopathic treatment.
My comment (score): The subject matter is basically a case report which is not very relevant. The article seems confused and goes from the positive effects of music to homeopathy. What the article reports about our £10, 000 challenge is not relevant. (3)
5. Title (date of publication): Charles hit by ‘dodgy’ detox quackery row (11 March 2009)
Subject: Prince Charles was accused yesterday of using “quackery” to exploit gullible people after his Duchy Originals label launched a controversial detox tincture.
Quote: Andrew Baker, chief executive of Duchy Originals… said: “Duchy Herbals Detox Tincture is traded as a food supplement and in accordance with all of the relevant sections of both UK and European food laws. It is a natural aid to digestion and supports the body’s natural elimination processes. It is not – and has never been described as – a medicine, remedy or cure for any disease.”
Prof Ernst said: …“Products like this are a dangerous waste of money. Charles is exploiting gullible people during hard times. It’s outright quackery.” The academic, who has been a professor at Exeter for 15 years, labelled the Prince’s firm “Dodgy Originals”.
My comment (score): The subject matter was relevant, in my view. The article and my comments are both correct. (10)
6. Title (date of publication): Homeopathy: A ‘cure’ that is all in the mind? (11 February 2010)
Subject: Imagine if an electronics store publicly admitted that an entire range of the products it sold didn’t work. It wasn’t that the DVD players were not very good quality, it simply didn’t have any evidence that they played DVDs at all.
Quote: A report published yesterday by the House of Commons Science and Technology Committee said the products were no more effective than a dummy pill and recommended the NHS stop funding them. Back in October last year Paul Bennett, the professional standards director of Boots, appeared in front of the Committee’s inquiry into alternative medicine. When asked if he believed that homeopathic products worked he said: “There is certainly a consumer demand for these products. I have no evidence to suggest they are efficacious.”
Scientists say there is no evidence water has such a memory or that homeopathy works at all beyond a basic placebo effect. “The principles are simply implausible,” says Professor Edzard Ernst, Professor of Complementary Medicine at the Peninsular Medical School in Exeter. “It might be OK that the principle is implausible if the method still worked but rigorous clinical trials have demonstrated that the method doesn’t work. On both levels the result is negative.”
My comment (score): The subject matter was relevant. The article seems correct but my comment seems a bit confusing. (8)
7. Title (date of publication): Acupuncture ‘a waste of time’ for couples trying for a baby (10 March 2010)
Subject: Couples who have acupuncture to boost their chances of becoming parents are wasting their time and money, experts said yesterday.
Quote: New guidelines from the British Fertility Society, which represents fertility clinics, said there was “no evidence” that either acupuncture or traditional Chinese herbal remedies could improve the success rate of In-Vitro Fertilisation.
Edzard Ernst, professor of complementary medicine at the Peninsula Medical School, based at the universities of Exeter and Plymouth, said: “This is a long-overdue clarification. Infertile women have been misled for some time now to think that traditional Chinese medicine can help them getting pregnant. This analysis shows two things very clearly: The totality of the acupuncture trials does not support this notion, and for Chinese herbs, we have no evidence at all. This will help infertile women not to waste their money.”
My comment (score): The subject matter was relevant. The article seems correct and my comment is true. (10)
8. Title (date of publication): Prince Charles’s charity in £150 000 fraud quiz (4 April 2010)
Subject: One of Prince Charles’s charities is being investigated by police amid allegations of a £150,000 fraud.
Quote: The Prince’s Foundation for Integrated Health … which campaigns for the wider use of complementary therapies, has failed to file its annual return. According to the Charity Commission website it is 154 days overdue. A spokesman for the foundation said: “Due to staff and structural changes, there was a delay in preparing the 2008 accounts. While getting these accounts ready for filing, our auditors Kingston Smith questioned some of the transactions. A t their recommendation a complaint has been made to the police. ” … Dr Michael Dixon, medical director for the foundation, said: “We should not abandon patients we cannot help with conventional scientific medicine. If homeopathy is getting results for those patients then of course we should continue to use it.”
The complaint also claimed the foundation’s trustees allowed staff to pursue a “vendetta” against a prominent critic , Edzard Ernst, professor of complementary medicine at Exeter University. Republic accused the foundation of being partly responsible for the imminent closure of Professor Ernst’s department after he publicly attacked its draft guide to complementary medicines as “outrageous and deeply flawed”.
My comment (score): The subject matter was relevant. The article seems correct albeit slightly confusing (the ‘vendetta’ is not really relevant here) the quotes are somewhat beside the point; mine seems copied from elsewhere. (7)
9. Title (date of publication): Prince Charles’s charity amid £300k fraud inquiry (30 April 2010)
Subject: PRINCE Charles’s homeopathy charity has been shut down amid a Scotland Yard investigation into a £300,000 fraud.
Quote: The 49-year-old man was arrested on Monday with a 54-year-old woman, both on suspicion of the same offences, after an investigation into £300,000 of unaccounted funds in the charity’s books.
… while the foundation has enjoyed successes, sometimes working with the Prince’s Duchy Originals company to produce alternative health care products, it has also become embroiled in a series of controversies. Critics have accused it of promoting “unscientific” approaches to health care. In February, MPs on the Commons Science and Technology Committee called for an end to homeopathy treatment on the NHS, arguing there was no evidence to support its effectiveness. Edzard Ernst, professor of complementary medicine at Exeter University, last year described a detox tincture made by Duchy Originals as “outright quackery” and regulators ordered the firm to withdraw misleading advertising claims about the effectiveness of two natural remedies.
My comment (score): The subject matter was relevant. The article seems correct and my comment seems copied from elsewhere and is beside the point. (8)
10. Title (date of publication): ‘Snake oil seller’ Prince Charles cost me my job, claims professor (26 July 2011)
Subject: A university professor, who labelled Prince Charles and other supporters of complementary medicine as “snake-oil salesmen”, last night accused the heir to the throne of costing him his job.
Quote: Edzard Ernst, a consistent critic of Prince Charles and his Duchy Originals food company, is stepping down from his post at Exeter University as Britain’s only professor of complementary medicine after a long-running dispute with the Prince about the merits of alternative therapies. He said: “Almost directly, Prince Charles has managed to interfere in my professional life and almost managed to close my unit.” He blamed Charles, a prominent advocate of alternative therapies such as acupuncture, herbal remedies and homeopathy, for undermining him and leading his bosses to lose faith in him.
A spokeswoman for Charles claimed last night that the Prince was unaware that his private secretary had complained about the professor. She declined to respond to the description of her boss as a “snake-oil salesman”.
My comment (score): The subject matter was relevant. The article seems correct and my comment is true. (10)
11. Title (date of publication): Do detox diets work? (10 January 2012)
Subject: Most of us overdo it during the festive season. No wonder January is the most popular month for detox diets which typically involve drinking pints of water each day, eating a very restricted diet and taking particular supplements.
Quote: The theory is toxins from unhealthy types of food and drink build up in the body and can lead to health problems. Purging these toxins is meant to leave you feeling full of energy and thinner.
The principle of detox goes back to medieval times but it is anti-science, agrees Professor Edzard Ernst, Britain’s first professor of complementary medicine, who works at Peninsula College of Medicine & Dentistry in Exeter. “You can’t overindulge on food and drink, then wave some magic wand,” he says. “The only thing that detox removes is money from your wallet.”
My comment (score): The subject matter was relevant. The article seems correct and my comment is true. (10)
12. Title (date of publication): Kevin Sorbo: Three strokes left me fighting for my life (28 February 2012)
Subject: Becoming a key speaker at a medical conference may seem an unlikely part for a Hollywood tough guy. Nevertheless that’s the role Hercules star Kevin Sorbo took after breaking his silence over three life-threatening strokes.
Quote: He made an appointment with his chiropractor. “I had been seeing this guy for eight years and he never cracked my neck,” recalls Kevin. “He knew I didn’t like it.” So he was surprised when the therapist did crack his neck. When he asked him why, the chiropractor responded by saying “I felt you needed it”. Irritated, the star paid his bill and started driving back to the home of his girlfriend, now wife, Sam. “I heard two very loud pops in the back of my head and my vision went crazy. I felt like I was falling backwards and I couldn’t stop. It was like that feeling you get when you stand up too quickly and get dizzy but multiplied by 10,” he says. Kevin managed to drive to Sam’s apartment and despite hearing two more “pops” went on to appear on a TV chat show after his agent insisted he could not pull out at the last minute. “I don’t remember what we discussed. I was on auto-pilot. The entire world was spinning, my head was throbbing. It was the best acting of my life, acting as though I was healthy.”
Whether or not the cracking technique is dangerous is a controversial issue. A study by Professor Edzard Ernst, director of complementary medicine at the UK’s Peninsula Medical School says: “Numerous deaths have occurred after chiropractic manipulations.” He thinks the risks of this treatment by far outweigh its benefit and adds: “In my view a chiropractor should not go near the neck.”
However Haymo Thiel, vice-principal of the Anglo-European College of Chiropractic, says: “There is risk in anything. It would be foolish to say not. But there is a difference between coincidence of timing and causation.”
My comment (score): Even though this is merely a case report, the subject matter seems relevant. The article seems correct and my comments are true. The Thiel comment at the end might serve as a nice example of false balance. (8)
13. Title (date of publication): Menopause: Natural remedies vs HRT (29 January 2013)
Subject: Are natural remedies best for the menopause, or is HRT still the strongest defence against its many unpleasant symptoms?
Quote: Since two major studies called hormone replacement therapy into question a decade ago – raising fears of breast cancer, stroke and heart disease – women confronting the menopause have faced a confusing choice.
“Few of the herbal remedies have been properly studied,” says Edzard Ernst, professor of complementary medicine at the university of Exeter. “Some promising evidence has emerged for black cohosh and red clover, but even these are not as strongly beneficial as HRT.”
My comment (score): The subject matter was relevant. The article seems correct and my comment is true. (10)
14. Title (date of publication): How safe is our herbal medicine? (19 March 2013)
Subject: For many of us hoping to take care of our aches and pains, boost our immune system or improve our mood, herbal remedies are often the first resort. Seen as a healthier and more natural option than conventional medication few of us stop to ask how safe these supplements actually are.
Quote: High street health chain Holland & Barrett is the most recent to fall foul of these rules. In January it was ordered to recall a blend of black cohosh and agnus castus called Flash Fighters which it was selling as a food supplement. A spokesman for the chain confirmed: “The MHRA stated the product’s name implied it could be used to treat ‘hot flushes’.” He added that the store is undergoing the process of having Flash Fighters reclassified under the Traditional Herbal Medicine Registration Scheme (THR).
Professor Edzard Ernst, world’s first professor of complementary medicine, warns: “The notion that natural equals safe can be dangerously misleading.”
My comment (score): The subject matter was relevant. The article seems correct and my comment is true. (10)
15. Title (date of publication): Prince Charles SLAMMED as ‘immoral’ for peddling ‘rubbish’ alternative medicines (18 January 2018)
Subject: Charles is under fire from a renowned scientist who accuses him of being an “immoral snake oil salesman” for promoting alternative medicines in a shocking new book that lambasts the future monarch.
Quote: Professor Edzard Ernst, who previously accused Charles of “selling snake oil”, has now hit out with a new book called “More Harm than Good?” He scalds Charles for being a vocal supporter of homeopathy, lobbying health ministers to set up a register of holistic practitioners and making impassioned speeches at the World Health Assembly and British Medical Association. The authors of the book, Professor Ernst and Dr Kevin Smith, of Abertay University in Dundee, said alternative medicines are “immoral”. Professor Ernst said: “You can’t have alternative medicine just because Prince Charles likes it, because that is not in the best interest of the patients.
My comment (score): The basis for the article was a presentation of a new book at the ‘Science Media Centre’. The book merely mentioned Charles merely in passing. The article and our comments seem correct, however, they were not to focus of our presentation. (7)
16. Title (date of publication): Weight loss pills: Are they actually effective in helping you lose weight? (10 September 2018)
Subject: Weight loss pills claiming to help you lose weight, are widely advertised. But do they actually live up to their claims; are they effective in helping you to lose weight or are they simply a con?
Quote: More than one-third of adults are overweight in England alone, with nearly one-quarter obese, and growing numbers of people are turning to weight loss pills and products as a means to shed excess weight. Many weight loss pills claim to contain herbs or natural substances that speed up metabolism or make you feel full up to discourage you from eating. But according to the NHS, there is little evidence that some products sold by reputable retailers and over the internet actually work, and could even be packed with harmful substances. Even products marketed as ‘guaranteed, clinically-proven and 100 per cent natural’ come with no guarantees, the NHS warned.
Some manufacturers of weight loss products also only focus on positive trials, failing to mention the negative or failed trials. “Manufacturers cherry-pick and only ever mention the positive trials,” said academic physician and researcher Edzard Ernst. “They then also fail to mention the mostly poor quality of their studies. Desperate people are being misled to buy unproven treatments at considerable expense.”
My comment (score): The subject matter was relevant. The article seems correct and my comment is true. (10)
17. Title (date of publication): Prince Charles under fire for becoming patron of 175-year-old homeopathy group (26 June 2019)
Subject: The Prince of Wales has been criticised after being made a patron of a 175-year-old homeopathy group, which supports medical professionals with alternative treatments.
Quote: Charles has long advocated homeopathic medicine, which is seen as an alternative to regular chemical-based treatments. Homeopathy attempts to treat some conditions, including headaches and colds, so the body will get better by itself. But after Charles was accused of being an “immoral snake oil salesman” by a medical professor in 2017, it seems more are lining up to take aim at the future monarch for further endorsement of alternative medicine.
Professor Edzard Ernst, who made the initial criticisms of Charles last year, told the Guardian: “In view of Charles’s long love affair with homeopathy, this news is unsurprising. The question is whether this will change anything about the sharp decline homeopathy has taken in this and several other countries, and whether it will alter the verdicts of dozens of independent organisations which recently have certified it to be a pure placebo therapy.”
My comment (score): The subject matter was relevant. The article seems correct my quotes are borrowed from elsewhere. (7)
18. Title (date of publication): China sparks fresh coronavirus fears by turning to traditional medicine to fight virus (29 June 2020)
Subject: Chinese government papers have revealed that a shocking majority of the country’s cases have been treated with traditional medicine.
Quote: Coronavirus currently has very little universally approved and clinically proven treatments, but scientists have made some discoveries into potentially effective drugs.
Edzard Ernst, a retired UK-based researcher of complementary medicines, said that there is no science behind the recommendation to support it’s usage. He said to Nature: “For TCM there is no good evidence and therefore its use is not just unjustified, but dangerous.”
My comment (score): The subject matter was relevant. The article seems correct my quotes are borrowed from elsewhere. (7)
19. Title (date of publication): Prince Charles fury: Scientist’s shock claim royal ‘treated him like dirt’ exposed (1 July 2020)
Subject: Prince Charles is known to be enthusiastic about alternative medicines and therapies. Yet, Professor Edzard Ernst, who has several times criticised the royal for his influence in the world of pseudo-medicine, once claimed that the prince “silenced” and treated him “like dirt”, a shocking unearthed report revealed.
Quote:
Prince Charles for decades has welcomed alternative medicines and therapies to apparently “cure” his ailments. One of the pseudo-sciences most popular with the prince appears to be homeopathy. Homeopathy is the largely discredited practice of treating illness with diluted substances to trigger the body’s own healing mechanisms.
In 2015, Professor Edzard Ernst, claimed he had been “treated like dirt” as a result of Charles trying to “silence” him. Prof Ernst is a staunch critic of using alternative medicines such as homeopathy as a direct means of treatment. He instead champions complementary medicine – the process of using alternative medicines to help alleviate the negative aspects of standard medicines – having held the first complementary medicine post in the world at the University of Exeter. His unscrupulous and rigorous application of evidence-based science and outspoken views found him at loggerheads with Charles.
My comment (score): The subject matter was only marginally relevant. I am pretty sure that I never said Charles treated me like dirt. I did say, however, that my university did treat me like dirt when dealing with the complaint from Charles’s first private secretary, Sir Michael Peat. My comments are borrowed from elsewhere. (4)
20. Title (date of publication): Prince Charles’ ‘plot’ with Andy Burnham for UK healthcare unveiled: ‘He was open to it’ (23 October 2020)
Subject: Prince Charles was once in agreement with Andy Burnham on the future direction of the UK’s healthcare, letters have revealed.
Quote: …this is not the first time Mr Burnham has been caught up in a divisive matter over healthcare. In 2009, the Greater Manchester Mayor was the Health Secretary under then Prime Minister Gordon Brown and was found to be corresponding with the Prince of Wales about the UK healthcare system. Charles has a reputation for being a “meddling” royal, particularly after his so-called ‘black spider memos’ to Government ministers were published in 2015.
Professor of complementary medicine Edzard Ernst told The Guardian in 2015: “The letters demonstrate yet again that Prince Charles relentlessly meddles in UK health politics and thus disrespects his constitutional role. “His arguments in favour of CAM [complementary and alternative medicine] and in particular homeopathy, show a devastating lack of knowledge and understanding; they are ill-informed, invalid and embarrassingly naive – but at the same time they are remarkably persistent.”
My comment (score): The subject matter was relevant. The article seems confusing my quotes are borrowed from elsewhere. (7)
21. Title (date of publication): Meghan Markle warning: Charles’ business blunder exposed amid new career move (17 December 2020)
Subject: Meghan Marle has just moved into the business sector after investing in a start-up – but she should be careful to avoid Prince Charles’ previous industry error which triggered a public outcry.
Quote: The Duchess of Sussex has ventured into the investment sector this week. It was announced that she has invested in Clevr Blends, a California-based sustainable start-up which sells four flavours of instant oat milk lattes. The company says its produce is sustainable, ethically sourced and healthy with organic ingredients, while its shipping materials are 100 percent recyclable.
However, Meghan’s father-in-law was accused of exploiting the public when Britain was still recovering from the recession with his Duchy Originals line. The UK’s first professor of complementary medicine, Edzard Ernst, dubbed the Duchy Originals detox tincture — which was being sold on the market at the time — “outright quackery”. The product, called Duchy Herbals’ Detox Tincture, was advertised as a “natural aid to digestion and supports the body’s elimination processes” and a “food supplement to help eliminate toxins and aid digestion”. The artichoke and dandelion mix cost £10 for a 50ml bottle.
My comment (score): The subject matter seems fairly irrelevant and far-fetched. My quotes belong to a different story. (2)
22. Title (date of publication): Prince Charles rejected by experts before Gwyneth Paltrow’s long Covid row: ‘Witchcraft’ (25 February 2021)
Subject: Prince Charles was rejected by scientists for his views on “witchcraft” alternative medicine well before Gwyneth Paltrow became embroiled in a row over her unapproved treatments for long Covid.
Quote: Gwyneth Paltrow has been urged to stop spreading misinformation by the medical director of NHS England after she suggested on her blog Goop that long Covid could be treated with various alternative medicines. The Hollywood star described how she herself had caught coronavirus and had since suffered with “long-tail fatigue and brain fog”. However, she claimed to have successfully treated it with “intuitive fasting”, herbal cocktails and regular visits to an “infrared sauna”.
The Prince of Wales has been specifically called out for advocating the controversial treatments, too. He was branded an “immoral snake oil salesman” by renowned scientist Professor Edzard Ernst in his book ‘More Harm Than Good?’ Prof Ernst founded the department of Complementary Medicine at the University of Exeter, became the world’s first academic on the subject and has founded two medical journals. Over the years, he has published a lot of critical research exposing methods that lack documentation of efficacy. The expert lambasted Charles for lobbying health ministers to set up a register of holistic practitioners and making impassioned speeches at the World Health Assembly and British Medical Association. He said: “You can’t have alternative medicine just because Prince Charles likes it, because that is not in the best interest of the patients. “The quality of the research is not just bad, but dismal. It ignores harms. There is a whole shelf of rubbish being sold and that is simply unethical.” His co-author, Dr Kevin Smith ‒ a senior lecturer at Abertay University specialising in Complementary and Alternative Medicine and genetics ‒ agreed that these alternative medicines are “immoral”. He added: “We certainly are very worried about the future King being a proponent.
My comment (score): The subject matter seems fairly irrelevant and far-fetched. My quotes belong to a different story. (2)
________________________________________
When I set out doing this analysis, I expected to find rather poor reporting by the DE. Yet, I was pleasantly surprised. Quite a lot of it is good. A few things did nevertheless occur to me:
- I find it remarkable how often Prince Charles is the focus of these stories. Occasionally, my various disputes with Charles were ‘pulled in’ even though they do not really fit into the context of the article.
- It is noticeable, I think, that the quality of the reporting deteriorated quite dramatically over time.
- The DE repeatedly borrows quotes from other publications and even from different stories altogether. This seems to me to be lazy and rather poor journalism.
My point is that there is really no need for lazy or poor journalism on SCAM. Journalists should do their work properly; they can always reach me via the contact option of this blog (I invariably reply swiftly). I feel they owe it to their readers to do at least this minimal and quick amount of effort.
According to his own website , Andreas Kalcker is a biophysical researcher of German origin who has lived most of his life in Spain and for many years has been living in Switzerland where he has investigated and registered several international patents that deal with the therapeutic use of chlorine dioxide for both hypoxia and for inflammation, infection, sepsis and Sars -Cov 2 -Coronavirus.
, Andreas Kalcker is a biophysical researcher of German origin who has lived most of his life in Spain and for many years has been living in Switzerland where he has investigated and registered several international patents that deal with the therapeutic use of chlorine dioxide for both hypoxia and for inflammation, infection, sepsis and Sars -Cov 2 -Coronavirus.
In recent years, he seems to have been particularly active as a snake oil salesman in South America. Argentinian authorities have now charged Andreas Kalcker for promoting toxic bleach (MMS) as a “miracle” medical treatment. Kalcker, alongside several Argentinian nationals, is accused of playing a key role in promoting chlorine dioxide in the country as a cure for various illnesses, including COVID-19, in conferences, books, and on social media.
The charges follow a seven-month-long investigation by the Unidad Fiscal para la Investigación de Delitos contra el Medio Ambiente (UFIMA), which investigates medical crimes in Argentina. The investigation was launched after the August 2020 death of a five-year-old boy in Neuquen, western Argentina, of multiple organ failure consistent with chlorine dioxide poisoning. The child’s parents believed, on the basis of misinformation spread by Kalcker and others, that the substance had the power to ward off COVID-19. An Argentinian judicial source said that Kalcker has been charged with the illegal practice of the medical profession and selling fake medicines. If found guilty of causing a child’s death, Kalcker could serve a prison sentence of up to 25 years.

Apart from Kalcker, four other persons were accused of being responsible for the distribution of chlorine dioxide in Argentina. The Argentine nationals had advertised and sold the substances via the internet – apparently in Kalcker’s name. According to the prosecution, “this distribution would have led to the messages about the ‘improvements’ resulting from the consumption of a substance with serious health consequences, which can even lead to death, being circulated with greater vigor.” The lawyer who started the ball rolling through his complaint is convinced that the parents of the deceased child believed that chlorine dioxide could protect their child from COVID-19 because of the misinformation spread by Kalcker.
Chlorine dioxide is a type of industrial bleaching agent commonly used to treat wood products. Public health authorities around the world have issued warnings about taking the substance, with the US Food and Drugs Administration warning that it can be fatal if taken in large doses. In recent years, a movement originating in a fake Florida “church” has promoted the substance it calls “Miracle Mineral Solution” (MMS), or “Chlorine Dioxide Solution” (CDS), as a cure for a range of illnesses and conditions.
MMS, or the Miracle Mineral Supplement, is a beverage product designed by former aerospace engineer, Jim Humble, who has tested his MMS protocol in Malawi and other parts of Africa. Initially used to treat malaria, the manufacturer claims field-tested success in treating and reversing the effects of AIDS, malaria, hepatitis, herpes, tuberculosis, most cancers, and a host of other diseases.
MMS has been promoted with the help of celebrities and VIPs, including Donald Trump. One of the many websites that advertise MMS states the following about it:
Master Mineral Solution, MMS or WPS Solution – Why has this Product Become so Popular?
Chlorine dioxide is a powerful anti microbial compound that has a long history of use – mostly known for its ability to sanitize drinking water (the last 60 years being the primary chemical used in municipal water supplies). The reason being is that it works, & works well. There are very few pathogens out there in water anywhere in the world that cannot be made potable with the use of this potent little molecule.
I think it goes without saying that MMS has not been shown to be effective against any condition while being very harmful when taken orally by humans.
Patients with fibromyalgia (FM) frequently resort to so-called alternative medicine (SCAM). In particular, osteopathy seems to be common, despite very weak supporting evidence. This study aimed to assess the efficacy of osteopathic manipulation in FM in a randomized clinical trial.
Patients were randomized to osteopathic or sham treatment. Treatment was administered by experienced physical medicine physicians, and consisted of 6 sessions per patient, over 6 weeks. Treatment credibility and expectancy were repeatedly evaluated. Patients completed standardized questionnaires at baseline, during treatment, and at 6, 12, 24, and 52 weeks after randomization. The primary outcome was pain intensity (100-mm visual analog scale) during the treatment period. Secondary outcomes included fatigue, functioning, and health-related quality of life. Intention-to-treat analyses were performed adjusted for credibility, using multiple imputations for missing data.
The ‘real’ treatment consisted of the following maneuvers. The patient was first placed in a prone position. Each vertebra from C7 to L5 was mobilized in a dorsoventral direction by progressive pressure on the spinous process (SP), and in rotation by applying pressure on the lateral surface of the SP (bilaterally). The sacral bone was repeatedly mobilized in nutation–counternutation (5–10 times). The piriformis muscles were progressively stretched. The hip joint was then progressively mobilized in extension combined with abduction and adduction to stretch the adductor, abductor, and flexor muscles (10 times). The shoulders were progressively mobilized, one by one, with a repeated circumduction movement of the glenohumeral joint (10 times). The patient was then placed in a supine position, for the following maneuvers. At the neck, bimanual traction was performed, followed by repeated mobilization in lateral flexion and in rotation (both sides, five times, 3–5 times each). At the shoulders, cranial traction was performed of both arms and then a repeated caudal traction of one arm and then the other, by blocking the clavicle, thereby opening the acromioclavicular and glenohumeral joints (three times). At the hips, repeated tractions were performed on the legs (three times) and the hip joint was mobilized by circumduction movements. Finally, the patient was placed in the lateral decubitus position for mobilization of the lumbar and thoracolumbar spine. Thrust manipulations were allowed at any level, according to the patient’s complaint.
The sham treatment followed the same order, but the maneuvers were stopped halfway through to prevent joint mobilization at the spine. At the hips and shoulders, the stretching techniques were also stopped halfway. The joint techniques were simulated, with no significant mobilization. Thrust manipulation was forbidden.
In total, 101 patients (94% women) were included. Osteopathic treatment did not significantly decrease pain relative to sham treatment (mean difference during treatment: -2.2 mm; 95% confidence interval, -9.1 to 4.6 mm). No significant differences were observed for secondary outcomes. No serious adverse events were observed, despite a likely rebound in pain and altered functioning at week 12 in patients treated by osteopathy. Patient expectancy was predictive of pain during treatment, with a decrease of 12.9 mm (4.4-21.5 mm) per 10 points on the 0-30 scale. Treatment credibility and expectancy were also predictive of several secondary outcomes.
The authors concluded that osteopathy conferred no benefit over sham treatment for pain, fatigue, functioning, and quality of life in patients with FM. These findings do not support the use of osteopathy to treat these patients. More attention should be paid to the expectancy of patients in FM management.
A recent systematic review concluded that the current evidence of manual therapy in patients with FM, based on a very low to moderate quality of evidence, was inconclusive and insufficient to support and recommend the use of manual therapy in this population. To date, only general osteopathic treatment has achieved clinically relevant pain improvement when compared with control.
The new study is by far the most rigorous one to date. This means, I think, that the best available evidence confirms that, in the management of FM,
osteopathy is a placebo therapy.
PS
When I say ‘osteopathy’ I mean the treatments as taught by Andrew Still. US osteopathy practice conventional medicine but everywhere else they adhere more or less strongly to Still’s ideas.
By guest blogger Wolfgang Denzer
Most pseudoscientific studies related to the explanation of the proposed mechanisms of homeopathy used tadpoles, wheat, or watercress as models. Results of these studies, e.g. those by Endler, Baumgartner & Co., were published in dedicated SCAM (So-Called Alternative Medicine) journals where the peers who review manuscripts have a clear tendency to support non-evidence-based studies in particular those that deal with homeopathy. In recent years several papers were published in reputable journals (see below) that purport the efficacy of ultrahigh dilution (UHD). None of these publications relates directly to homeopathy or even uses the term “homeopathy”. One thing the publications have in common is that they were either sponsored by the Russian OOO [sometimes LLC] “npf” Materia Medica Holding or co-authored by staff of that company. Materia Medica Holding produces and markets ultra-high diluted remedies that are called ‘release-active’ drugs (RA-drugs). The company founder rigorously states that their remedies are not homeopathy and that „homeopathy is doomed to have a marginal position in the modern system of therapy“. (see interview link at the end). Already a few years ago Panchin et al. (2018) analyzed several papers that involved Materia Medica Holding in one way or the other and published an article in BMJ Evidence-Based Medicine (Drug discovery today: no molecules required. http://dx.doi.org/10.1136/bmjebm-2018-111121). His remarkable conclusion was as follows: “Surprisingly, these innovative “drugs” contain no active molecules and can be considered a new brand of homeopathy. This indicates one of two possibilities: either we are at the brink of a revolution in medicine or that something went wrong with research published in numerous academic journals.” Of course, the latter assumption is correct.
The difficulty to uncover the use of an ultra-high diluted homeopathic (oops) remedy instead of proper medication published in a study is best shown by having a look at the following publication co-authored by the founder of Materia Medica Holding Oleg I. Epstein and two of his employees:
Pathogenetic approach to the treatment of functional disorders of the gastrointestinal tract and their intersection: results of the Russian observation retrospective program COMFORT (BMC Gastroenterol. 2020; 20: 2. Published online 2019 Dec 31. doi: 10.1186/s12876-019-1143-5).
The study deals with a retrospective analysis of the effectiveness of Kolofort, “a release-active drug” produced by Materia Medica Holding. The only statement regarding the composition of the drug reads as follows: “For the treatment of FGID [functional gastrointestinal disorders], the combination of released-active form of antibodies [RAF of Abs] to S-100 protein, TNF-α and histamine (RAF of Abs to S 100, Abs to TNF-α and Abs to H), a pathogenetically targeted drug Kolofort, was developed by the Research and Production Company Materia Medica Holding (LLC NPF” MATERIA MEDICA HOLDING”) Moscow, Russia and introduced into practical medicine. The RAF of Abs in the drug provides an anti-inflammatory, spasmolytic, and anxiolytic effect ” (notations in square brackets by me). The two following paragraphs provide information (and citations of two publications in Russian) related to the clinical trials of Kolofort. At no point in the publication are the concentrations of the active components of Kolofort mentioned! Only a web search provides further information about the composition of Kolofort (see screenshot). The three active ingredients, RAF of Abs to S-100 protein, TNF-α, and histamine, are only present at concentrations of C12, C30, and C200, respectively, i. e. they are absent. Perhaps a better notation for the remedy should be RAF in Abs of histamine, meaning release-active form in absence of histamine.
Judging from the composition of Kolofort no physiological or therapeutical reaction is to be expected. Still the authors claim that “The COMFORT program has demonstrated the positive effect of treatment [with Kolofort] in the majority of patients with IBS and FD and their combination in real clinical practice”. The authors arrived at these results by analyzing a questionnaire that had been specially developed for the assessment of gastrointestinal disorders. The questionnaire is called “7*7” [seven symptoms in seven days], but not further discussed or explained in the publication. Although there exists at least one publication from 2016 where the questionnaire was used to assess symptoms of gastrointestinal ailments (Ivashkin et al. RZHGGK. 2016;3(S):24-33. https://doi.org/10.22416/1382-4376-2016-26-3-24-33) the actual validation was not published until November 2018 (online, print June 2019) which is after the Kolofort study had already terminated (November 01, 2017, through March 30, 2018). Please note that the validation was done by one of the co-authors (V. Ivashkin) of the Kolofort study. There is certainly a good explanation for post-validating a tool used in earlier studies, but I just can’t think of one right now.
There exist several more (if not dozens) of publications by this group of authors that have already been investigated. It appears that the Materia Medica Holding director Oleg I. Epstein is heavily involved in a competition of who is capable of producing the highest number of retracted publications. Here are a few of them:
Retraction: Novel Approach to Activity Evaluation for Release-Active Forms of Anti-Interferon-Gamma Antibodies Based on Enzyme-Linked Immunoassay
The PLOS ONE Editors. Published: May 3, 2018
https://doi.org/10.1371/journal.pone.0197086
Retraction notice to “Efficacy of novel antibody-based drugs against rhinovirus infection: In vitro and in vivo results” [Antiviral Research 142 (2017) 185–192]
https://doi.org/10.1016/j.antiviral.2019.02.010
Retraction notice to “Activity of ultra-low doses of antibodies to gamma-interferon against lethal influenza A(H1N1)2009 virus infection in mice” [Antiviral Research 93 (2012) 219–224]
https://doi.org/10.1016/j.antiviral.2019.02.011
Retraction Note: Release-Active Dilutions of Diclofenac Enhance Anti-inflammatory Effect of Diclofenac in Carrageenan-Induced Rat Paw Edema Model
https://doi.org/10.1007/s10753-013-9705-0
Retraction: Activity of ergoferon against lethal influenza A (H3N2) virus infection in mice
https://www.intmedpress.com/journals/avt/article.cfm?id=3325&pid=48&sType=AVT
Retraction Note: Effects of chronic treatment with the eNOS stimulator Impaza on penis length and sexual behaviors in rats with a high baseline of sexual activity
https://www.nature.com/articles/s41443-020-0321-x
There are probably more retractions out there, but to make it onto the current Retraction Watch Leader Board (https://retractionwatch.com/the-retraction-watch-leaderboard/) a minimum of 25 retractions is required to take over rank 30. You have to work harder Dr. O. I. Epstein!
Last but not least there is an interview with Epstein available online (https://pharmaboardroom.com/interviews/interview-with-oleg-epstein-general-director-materia-medica/) where he claimed that „We proved that we [Materia Medica] are not a homeopathy company, and 1.5 years ago, the Ministry of Public Health decreed that our drugs will no longer be classified as homeopathic.“ Wow! How?
So, what does all this tell us? There exists a pool of authors, somehow connected to Materia Medica Holding, who manage to get articles, that are nothing else but homeopathy in disguise, past the peer review of reputable academic journals. It would be easy to blame the reviewers for their not soo stringent approach. But as the Kolofort paper shows, only in-depth research may actually reveal the truth. Let’s not forget, even the retracted papers made it through to publication and only a later review scrutinized their scientific merit.
It can be assumed that Materia Medica will not stop promoting their remedies through the publication of further studies. There are already publications out there that do not include any company staff as co-authors but were sponsored by the company. Judging from the rate of already retracted paper, reputation does not appear to matter. These authors possibly work along a submission-rejection-resubmission to a different journal approach until a paper gets published.
So far the homeopathy community hasn’t taken much notice of any of the beforementioned studies, most probably for two reasons: nowhere does the term “homeopathy” appear nor were the papers published in SCAM journals but rather in academic journals above the radar of homeopaths. But it can be assumed that in future, if it fits their purpose, such studies will feature among their usual dubious double blindfolded placebo trials.
Keep your eyes open for more of this stuff and please get in touch with the editorial team of the journal concerned if you discover yet another “UHD” or “RAF” publication!
Young Australian journalist Eammon Ashton-Atkinson has survived COVID-19 and two strokes, all in the span of a month. It was reported that the 34-year-old Washington DC-based correspondent had a stroke on his chiropractor’s table after experiencing post-COVID neck pain, and was rushed to hospital. While recovering at home, he had a second stroke, losing his balance and collapsing. 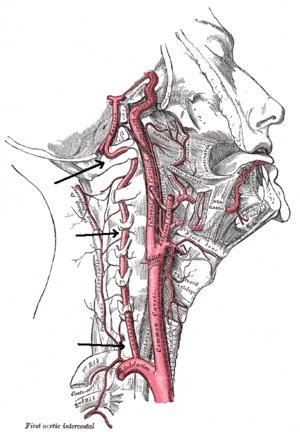
He told his radio channel that the first stroke occurred while he was still on the chiropractor’s bench. He was rushed to hospital where a dissection of an artery supplying the brain (probably the vertebral artery) was diagnosed. His vision was initially severely disturbed and he had ‘pins and needles’ in parts of his body. These symptoms subsided rapidly and he was discharged home to recover. However, while resting at his home in DC, he suffered another stroke. This time a blood clot from the dissection fired into the part of his brain responsible for his balance. He was then readmitted to the hospital and treated against the blood clot. Now he is again back home and hoping to recover fully.
Were the strokes related to COVID, the vaccination, or to the chiropractic treatment? Definitely the latter, explains Eammon Ashton-Atkinson in the interview. It seems that his doctors diagnosing and treating the strokes were clear that the cause of the problems was the manipulation.
“It’s still quite traumatic to talk about,” Eammon Ashton-Atkinson told Jim Wilson. “In some ways, I’m very unlucky, in other ways I’m extremely lucky because I’m talking to you now.”
Chiropractors will surely point out that this is not a properly documented case. Almost every detail that makes a decent case report is missing.
I agree!
And why are cases like these (one might speculate that there are many of them) not adequately documented?
Because there is no post-marketing surveillance of chiropractic.
And who is responsible for establishing one?
The chiropractors, of course!
And why do they not create reliable post-marketing surveillance?
Perhaps because that would disclose the magnitude of the risk; and that would obviously be very bad for business.
Therefore, I suggest that chiropractors finally get their act together and create adequate post-marketing surveillance. Until they have done so, they have no moral right to complain that cases like the one above are not adequately documented.
By guest blogger Hans-Werner Bertelsen
Veronika Hackenbroch wrote in an article for the German news website Der Spiegel about clusters of cases where children were born with severe birth deformities. (1) The only common factor that researchers in the Paediatrics department of the University Medical Center Mainz were able to identify through intensive communication with the mothers was that they had all visited a dentist whilst pregnant. The fetus is particularly sensitive to exogenous stimuli during early pregnancy, which is why this period is also known as the “teratogenetic determination period” (Koberg).
The data regarding the workplace exposure limit for mercury is outdated – it is based on information collected about 50 years ago in some cases. Since that time, there have been considerable advances, in particular in the fields of measuring technology and analysis. Unfortunately, these advances have yet to be utilized to provide meaningful figures on exposure to mercury vapour when removing old fillings or drilling into teeth with mercury amalgam fillings for the purpose of acute pain management. In addition to patient protection, the focus when processing existing mercury amalgam fillings is therefore also on occupational health and safety. This has not gone unnoticed by many female employees in dental surgeries that mercury amalgam can pose serious risks to unborn children. For example, a study in Norway reported an increased risk of perinatal death associated with a high number of mercury amalgam fillings. (2)
Sylvia Gabel from the German Association of Medical Professions (Verband medizinischer Fachberufe e.V.) even called for an immediate ban on toxic mercury amalgam: “Vapours pose a danger to dental professionals’ health!”. Mrs Gabel added: “The processing of amalgam in dental surgery releases mercury vapour. As 99 per cent of the dental nurses and hygienists in Germany are female and mercury has harmful effects on both fertility and the unborn child, we are exposed to a particular risk.”(3)
Researchers in Norway documented a considerable increase in the concentration of mercury in the blood after the removal of fillings as far back as 2006. (4) Toxicologists are in unanimous agreement that these peaks, which are the result of inhalation, are extremely harmful and may well have a teratogenetic effect in early pregnancy. (5) Consequently, what I am calling for is this: until such time as we know how high the mercury vapour concentrations are and as long as we “remain in the dark”, we should refrain from removing existing fillings containing mercury and performing dental drilling procedures in women of child-bearing age for ethical reasons so as to exclude the risk of deformities (see Der Spiegel article: “Waren die Schwangeren beim Zahnarzt?”, V. Hackenbroch, 20.09.19). (6)
An immediate ban on the use of mercury amalgam would be advantageous not solely with regard to the exposure to toxins of cancer patients, as the field of “alternative medicine” often recommends expensive, unnecessary and subsequently also very harmful “detox” treatments. (7) A more than questionable business from an ethical perspective: cancer patients are often looking for additional, so-called complementary therapy methods. This often sees them fall into the clutches of healers and doctors, who have no dental expertise but can identify mercury amalgam fillings very easily due to their dark colour. As I myself experienced in a so-called “alternative” dental surgery, the frightened patients, who are often in the middle of chemotherapy cycles, are then informed that they absolutely must have the mercury amalgam removed and then undergo a “detoxification therapy”. Introjects are not spared in the process: “Your body, already devastated by the chemotherapy, should not be subjected to additional chemicals.” Of course, this “detoxification” will be performed (with maximum consideration!) as a “homoeopathic” therapy. I had to observe this very lucrative “business model” often enough – and not once has a cancer patient objected. Once they fall under the charlatan’s spell, patients will allow themselves to be treated with all manner of things. Even live cells. In one patient, a single mother of two, this method triggered a fatal anaphylactic shock. (8) However, cancers and other chronic diseases are not the only reasons that bring patients with mercury amalgam fillings within the reach of dubious individuals with promises of salvation and charlatans. (9) An unfulfilled desire to have children has also led countless desperate women to ask to be parted irrevocably from their mercury-containing fillings. German health insurance companies approve these interventions, which appear logical from a toxicological perspective, and thus contribute not only to the replacement of the fillings but also to the release of mercury vapours and thus toxic peaks resulting from inhalation. Such actions can even have fatal consequences in the early stages of pregnancy.
However, the focus with mercury amalgam is not only on protecting patients from dishonest therapists and unnecessary teratogenetic risks – female staff could also benefit in general. For example, an immediate ban of the use of mercury amalgam could significantly increase job satisfaction among female employees in the dental surgery. According to Sylvia Gabel: “Strike measures were considered in the surgeries continuing use.”(10)
Each new mercury amalgam filling brings with it numerous side effects. It:
- – increases the risk of toxic exposure resulting from inhalation during removal;
- – increases the risk of corrosion products developing in the long term;
- – increases demand in the field of detox beliefs and homoeopathic charlatanry;
- – promotes the conspiracy narrative of “the dangers of conventional medicine”; and, in doing so,
- – often undermines patients’ confidence in treatments appropriate for the indication and, along with it, the often-vital compliance;
- – fills not only the cavity in the tooth but also the charlatans’ pockets.
I believe it is time to give dental health a helping hand with an intelligent combination of contemporary prevention concepts and harmless filling materials. Currently, the political will is merely a small seed. The seed must now germinate and grow.
REFERENCES
1. “Waren die Schwangeren beim Zahnarzt?”, V. Hackenbroch, 20.09.19 2. https://www.zwp-online.info/zwpnews/dental-news/wissenschaft-und-forschung/schwangerschaft-und-amalgam-risiken-bei-hohen-mengen 3. https://www.dzw.de/amalgam-ausstieg-ngo 4. https://pubmed.ncbi.nlm.nih.gov/29320025/
5. Prof. Eschenhagen, Toxicology Hamburg-Eppendorf in personal correspondence dated 23.01.2020 6. Comment dated 05.07. https://onkelmichael.blog/2021/07/03/ist-eine-entfernung-bestehender- amalgam-restaurationen-problemlos-und-bedenkenlos-durchfuhrbar/comment-page-1/? unapproved=4000&moderation-hash=d5b63e66f5045bfa12d829a88eddf1b0#comment- 4000 7. Prof. E. Ernst: https://www.theguardian.com/lifeandstyle/2014/dec/05/detox-myth-health-diet-science-ignorance 8. http://scienceblogs.de/kritisch-gedacht/2012/02/08/insider-bericht/
9. Prof. Jutta Hübner (Oncology, Jena) in personal correspondence dated 21.01.2020
10. Sylvia Gabel in personal correspondence dated 18.06.21
Beer is the main food source of isoxanthohumol, a precursor of 8-prenylnaringenin, the strongest phytoestrogen identified to date. As phytoestrogens are reported to reduce perimenopausal symptoms, this study evaluated if daily moderate consumption of beer with (AB) and without alcohol (NAB) could improve menopausal symptoms and modify cardiovascular risk factors.
A total of 37 postmenopausal women were enrolled in a parallel controlled intervention trial and assigned to three study groups:
- 16 were administered AB (330 mL/day),
- 7 to NAB (660 mL/day),
- 14 were in the control group and received no beer.
After a 6-month follow-up of the 34 participants who finished the trial, both interventions (AB and NAB) significantly reduced the severity of the menopause-related symptoms. Moreover, AB had a beneficial net effect on psychological menopausal discomforts compared to the control group. As the sex hormone profile did not differ significantly between the study groups, the effects of both types of beers (AB and NAB) are attributed to the non-alcoholic fraction of beer. Furthermore, moderate NAB consumption improved the lipid profile and decreased blood pressure in postmenopausal women.
The authors concluded that a daily moderate AB and NAB consumption may provide an alternative approach for postmenopausal women seeking relief from mild to moderate climacteric symptoms. Moreover, NAB was found to have a beneficial effect on LDL-C, ApoA1, and DBP measurements, all known risk factors for cardiovascular disease. However, these results must be considered as preliminary and will require confirmation with larger sample sizes.
The clinical implications of daily moderate AB and NAB consumption have been revealed in this study, but the mechanisms of action and impacts on sex hormones remain unknown. The most effective quantity of beer, with or without alcohol, that can be safely consumed by a postmenopausal woman still needs to be determined, taking into consideration factors such as age, genetics, and ethnicity.
I am impressed and only have this comment: let’s please not forget the male menopause …
and if they ever did a trial, can I please go in group AB?
Germany has long been the ‘Promised Land’ for so-called alternative medicine (SCAM). For many years, about two-thirds of the general population has been reported to be regular SCAM users. Now, this seems about to change. A recent survey found that only one-third of Germans believe that homeopathy works as well as conventional medicine. The verdict on SCAM as a whole is similar: Only 35 percent of respondents would like SCAM to play a role in healthcare in addition to modern medicine. The results originate from an extensive representative survey commissioned by the GWUP and carried out by the KANTAR Institute to sound out attitudes toward esotericism and pseudoscience. The figure below depicts percentage figures of the belief in (from left to right) homeopathy, integrated medicine, spiritual healing, electrosmog, dowsing, clairvoyance, psychokinesis, ghosts, astrology, extra-terrestrials, none mentioned.

“It is a good sign for health care if two-thirds of the population reject dubious cures. The experience from the pandemic shows that we can only fight diseases with science and modern medicine,” stated Amardeo Sarma, chairman of GWUP. “I am pleased with the result because it also underlines the impact of our educational work. I’m convinced that we’re helping people make important decisions, removing uncertainty and, not least, preventing suffering caused by incorrect treatments.”
“As a physician, I am pleased when more and more people are concerned with their health and critically question promises of healing,” said Dr. Natalie Grams. “For me, the declining approval of homeopathy means that it is worthwhile to publicly stand by science and not be muzzled by industry interests. Fewer homeopathics mean more good medicine for patients that really works.”
This sounds like good news indeed. Yet, I think, we need to be careful and avoid jumping to conclusions because prevalence surveys are often not as reliable as they seem.
1) They frequently lack a clear definition of what is being surveyed. There is no generally accepted definition of alternative medicine, and even if the researchers address specific therapies, they run into huge problems. Take integrated medicine, for instance – some see this as alternative medicine, while others would, of course, argue that it is the integration of social and health care. Or take homeopathy – many consumers confuse it with herbal medicine.
2) The questionnaires used for such surveys are rarely validated. Essentially, this means that we cannot be sure they evaluate what we think they evaluate. We all know that the way we formulate a question can determine the answer. There are many potential sources of bias here, and they are rarely taken into consideration. It is therefore not surprising that different surveys report different prevalences. In Indonesia, for instance, an increase in SCAM use has been reported associated with the pandemic.
3) The typical survey has a low response rate; sometimes the response rate is not even provided or remains unknown even to the investigators. This means we do not know how the majority of patients/consumers who received but did not fill the questionnaire would have answered. Often there is good reason to suspect that those who have a certain attitude did respond, while those with a different opinion did not. This self-selection process is likely to produce misleading findings.
4) The typical survey has a long list of questions and reports only those results that the investigators find interesting or pleasing. Such selective reporting can introduce a significant bias that may not be detectable for the reader of the report.
I am sure the new survey is not seriously affected by any of these drawbacks. After all, it is from the GWUP, the Society of the Scientific Study of Para-Sciences. If they are not able to do good science, who is?
My most frequently cited paper was published by Angelo Izzo and myself in 2001. It has so far been cited 1612 times. Here is its abstract:
Despite the widespread use of herbal medicines, documented herb-drug interactions are sparse. We have reviewed the literature to determine the possible interactions between the seven top-selling herbal medicines (ginkgo, St John’s wort, ginseng, garlic, echinacea, saw palmetto and kava) and prescribed drugs. Literature searches were performed using the following databases: Medline (via Pubmed), Cochrane Library, Embase and phytobase (all from their inception to July 2000). All data relating to herb-drug interactions were included regardless of whether they were based on case reports, case series, clinical trials or other types of investigation in humans. In vitro experiments were excluded. Data were extracted by the first author and validated by the second author. 41 case reports or case series and 17 clinical trials were identified.
The results indicate that St John’s wort (Hypericum perforatum) lowers blood concentrations of cyclosporin, amitriptyline, digoxin, indinavir, warfarin, phenprocoumon and theophylline; furthermore it causes intermenstrual bleeding, delirium or mild serotonin syndrome, respectively, when used concomitantly with oral contraceptives (ethinylestradiol/desogestrel), loperamide or selective serotonin-reuptake inhibitors (sertaline, paroxetine, nefazodone). Ginkgo (Ginkgo biloba) interactions include bleeding when combined with warfarin, raised blood pressure when combined with a thiazide diuretic and coma when combined with trazodone. Ginseng (Panax ginseng) lowers blood concentrations of alcohol and warfarin, and induces mania if used concomitantly with phenelzine. Garlic (Allium sativum) changes pharmacokinetic variables of paracetamol, decreases blood concentrations of warfarin and produces hypoglycaemia when taken with chlorpropamide. Kava (Piper methysticum) increases ‘off periods in Parkinson patients taking levodopa and can cause a semicomatose state when given concomitantly with alprazolam. No interactions were found for echinacea (Echinacea angustifolia, E. purpurea, E. pallida) and saw palmetto (Serenoa repens).
In conclusion, interactions between herbal medicines and synthetic drugs exist and can have serious clinical consequences. Healthcare professionals should ask their patients about the use of herbal products and consider the possibility of herb-drug interactions.
The article was so successful that the journal ‘DRUGS’ asked us to publish an update. As the journal is highly respected we obliged with pleasure; here is the abstract of the update of 2009:
The concomitant use of herbal medicines and pharmacotherapy is wide spread. We have reviewed the literature to determine the possible interactions between seven popular herbal medicines (ginkgo, St John’s wort, ginseng, garlic, echinacea, saw palmetto and kava) and conventional drugs. Literature searches were performed using MEDLINE, Cochrane Library and EMBASE and we identified 128 case reports or case series, and 80 clinical trials. Clinical trials indicate that St John’s wort (Hypericum perforatum), via cytochrome P450 (CYP) and/or P-glycoprotein induction, reduces the plasma concentrations (and/or increases the clearance) of alprazolam, amitriptyline, atorvastatin, chlorzoxazone, ciclosporin, debrisoquine, digoxin, erythromycin, fexofenadine, gliclazide, imatinib, indinavir, irinotecan, ivabradine, mephenytoin, methadone, midazolam, nifedipine, omeprazole, oral contraceptives, quazepam, simvastatin, tacrolimus, talinolol, verapamil, voriconazole and warfarin. Case reports or case series suggest interactions of St John’s wort with adrenergic vasopressors, anaesthetics, bupropion, buspirone, ciclosporin, eletriptan, loperamide, nefazodone, nevirapine, oral contraceptives, paroxetine, phenprocoumon, prednisone, sertraline, tacrolimus, theophylline, tibolone, tryptophan, venlafaxine and warfarin. Ginkgo (Ginkgo biloba) decreases the plasma concentrations of omeprazole, ritonavir and tolbutamide. Clinical cases indicate interactions of ginkgo with antiepileptics, aspirin (acetylsalicylic acid), diuretics, ibuprofen, risperidone, rofecoxib, trazodone and warfarin. Ginseng (Panax ginseng) may interact with phenelzine and warfarin. Kava (Piper methysticum) increases the clearance of chlorzoxazone (a CYP2E1 substrate) and may interact with alprazolam, levodopa and paroxetine. Garlic (Allium sativum) interacts with chlorpropamide, fluindione, ritonavir and warfarin; it also reduces plasma concentrations of chlorzoxazone (a CYP2E1 probe). Echinacea might affect the clearance of caffeine (a CYP1A2 probe) and midazolam (a CYP3A4 probe). No interactions have been reported for saw palmetto (Serenoa repens). Numerous interactions between herbal medicines and conventional drugs have been documented. While the significance of many interactions is uncertain, several interactions, particularly those with St John’s wort, may have serious clinical consequences.
Angelo Izzo is a lovely man and a highly skilled pharmacologist. He came to my department in 2000 as a guest researcher (on his own funds) and worked with us for several months. This is how the 2001 paper was created. After he returned to his native Naples, Italy, he became a professor of pharmacology with a special interest in plant pharmacology. He has published many further important papers and, together with his Italian colleagues, a most useful book entitled ‘Phytotherapy: A Quick Reference to Herbal Medicine‘. I warmly recommend it to anyone interested in herbal medicine.
The subject of herb-drug interactions is in my view hugely important. When Angelo and I first approached it in 2001, it was woefully under-researched; in that year, there were just 37 Medline-listed papers on the subject. This has now increased very significantly; since 2011 there are about 150 articles on the topic each year. It is tempting to think that Angelo (and I) had a tiny influence on this positive development.