Uncategorized
The new kid on the SCAM block seems to be hydrogen-rich water (HRW). It is pure water infused with hydrogen molecules and can be purchased in pouches and cans or made at home using special, commercially available devices. Health writers and entrepreneurs have been everything but timid in publishing claims about HRW. This is from one of thousands of sites promoting it:
1. Antioxidant And Anti-inflammatory Properties
Studies show that consuming hydrogen-rich water for a few weeks at a time can reduce reactive oxygen metabolites (ROMs) in the bloodstream, which can damage cells while sustaining blood oxidation levels needed to ensure health. The result is a reduction in and inflammation, which effectively reduces cell damage and leads to an improved quality of life. Decreased oxidative stress is also a valuable factor which helps prevent metabolic syndrome and soften the impact of neurodegenerative disease. Hydrogen-rich water, through its power to combat oxidative stress, is a promising remedy for these and other diseases. Its anti-inflammatory properties are already used to treat rheumatoid arthritis, one of the most prominent and debilitating conditions caused by high levels of inflammation in the body.
2. May Treat And Prevent Metabolic Syndrome
Metabolic syndrome, which includes obesity, high cholesterol, high blood pressure, and often causes a range of cardiovascular illnesses, is a rapidly growing problem among American adults. Early studies show that hydrogen-rich water health benefits include staving off metabolic syndrome and reversing negative metabolic symptoms because of its ability to reverse the effects of oxidative stress on the body. In fact, studies have shown that consuming hydrogen-rich water decreases the “bad” cholesterol, also known as serum-LDL cholesterol while improving HDL function — the “good” cholesterol. This effect, in turn, prevents against the development of a number of debilitating cardiovascular issues.
3. Slows The Development Of Neurodegenerative Diseases
By fighting in important brain tissues, hydrogen-rich water fights a key cause of conditions like Parkinson’s disease and , both of which feature cognitive and behavioral impairment and decline. Because it consumes a high level of oxygen, the brain is prone to oxidative stress. Hydrogen-rich water elicits effects in the brain that counter the ability of oxidative stress to kill dopamine cells and damage proteins that maintain cognitive functioning. When used daily by patients of Alzheimer’s, hydrogen-rich water has been shown to restore neural proliferation, thereby inhibiting cognitive decline. Especially promising is the demonstrated ability of H2-rich water consumption to combat cognitive impairment even in its latest stages and to alleviate the harm of brain injury — again, because of its ability to ameliorate oxidative stress on brain tissue. In fact, some researchers recommend daily consumption of hydrogen-rich water as a long-term preventative treatment against dementia and neurodegenerative disease and as a part of a recovery program for brain injury from stroke or surgery.
4. May Treat And Prevent Insulin Resistance And Type 2 Diabetes
Recent studies demonstrate that hydrogen-rich water health benefits include having a normalizing effect on glucose in the body. In combination with powerful antioxidant properties, hydrogen-rich water improves insulin circulation and sensitivity, while also increasing levels of certain compounds that build insulin resistance. The end product is improved glucose metabolism, which can both prevent and slow the development of Type 2 Diabetes Mellitus and insulin resistance.
5. Improves Dental Health
As shown above, oxidative stress causes a number of ailments. One of the most common is dental decay. Fortunately, consuming hydrogen-rich water has been proven to treat conditions associated with dental deterioration, such as periodontal disease, because of its ability to fight oxidative stress, in addition to its effective anti-inflammatory properties. Drinking water containing molecular hydrogen targets periodontal disease at the source by suppressing inflammation in the oral tissue. Hydrogen-rich water also prevents age-related oxidative damage to oral tissue, thereby offsetting dental decay.
6. Combats Muscle Fatigue
One compelling study of male soccer players found that, by consuming hydrogen-rich water before exercise, these athletes could reduce blood lactate levels and improve muscle function during exercise. After exercise, these athletes experienced lower levels of muscle fatigue and were able to recover faster. Because it also treats exercise-induced dehydration, hydrogen-rich water is a promising remedy for athletes. According to Biethan, “more and more athletes are picking up on it” to improve their athletic performance and recovery.
And how does HRW work? What is its mode of action? Nobody seems to know! During the last months, there have been several controlled clinical trials of HRW. Regardless of what condition they address, they all arrived at positive conclusions:
- In conclusion, these results suggest that supplementation with hydrogen-rich water may have a beneficial role in prevention of T2DM and insulin resistance.
- HRW significantly attenuates oxidative stress in CHB patients, but further study with long-term treatment is required to confirm the effect of HRW on liver function and HBV DNA level.
- Two weeks of HRW intake may help to maintain PPO in repetitive sprints to exhaustion over 30 minutes.
- Thus, hydrogen-rich water appeared to alleviate the mFOLFOX6-related liver injury.
- appears that orally administered H2 as a blend of hydrogen-generating minerals might be a beneficial agent in the management of body composition and insulin resistance in obesity.
- Although preliminary, the results of this trial perhaps nominate HRW as an adjuvant treatment for mild-to-moderate NAFLD. These observations provide a rationale for further clinical trials to establish safety and efficacy of molecular hydrogen in NAFLD.
- To conclude, acute pre-exercise supplementation with HRW reduced blood lactate at higher exercise intensities, improved exercise-induced perception of effort, and ventilatory efficiency.
Aprart from producing uniformly positive results, these studies have another common feature: they are methodologically flimsy. Probably the most rigorous trial of HRW was published earlier this year. Perhaps it is worth having a look at it:
An international team of researchers conducted a randomized, double-blinded, placebo-controlled trial in 60 subjects (30 men and 30 women) with metabolic syndrome. An initial observation period of one week was used to acquire baseline clinical data followed by randomization to either placebo or high-concentration HRW (> 5.5 millimoles of H2 per day) for 24 weeks.
High-concentration HRW was prepared via hydrogen-producing tablets (HRW Natural Health Products Inc., New Westminster BC, Canada) while the placebo was prepared as a placebo drink similar in taste, dissolution, and appearance to HRW. Placebo capsules, also donated by HRW Natural Health Products Inc. (New Westminster, BC, Canada), contained identical ingredients to the hydrogen supplement, but instead of metallic magnesium the placebo contained various forms of magnesium salts (i.e. tartrate, malate, chloride) and similar organic acids to prevent any pH buffering effect from the conjugate bases of the alkaline salts.
The participants consumed 1 tablet 3 x daily in 250 mL of 12-18°C water. They were advised to drink the product in one gulp as soon as the tablet finished dissolving on an empty stomach/morning. This method of H2 administration would provide >5.5 millimoles H2/day.
Supplementation with high-concentration HRW significantly reduced blood cholesterol and glucose levels, attenuated serum haemoglobin A1c, and improved biomarkers of inflammation and redox homeostasis as compared to placebo. Furthermore, H2 tended to promote a mild reduction in body mass index and waist-to-hip ratio.
The authors concluded that the results from our study suggest that supplementation with high-concentration HRW produced via H2-producing tablets improves body composition, favorably modulates fatty acid and glucose metabolism, and improves inflammation and redox homeostasis in subjects with metabolic syndrome. Therefore, long-term treatment with high-concentration hydrogen-rich water may be used as an adjuvant therapy to decrease the features of metabolic syndrome. However, a larger prospective clinical trial is warranted to further determine the biological effects of HRW in this subject population.
The authors of this study, which was conducted in Moradabad India and supported by Slovak Research and Development Agency; Scientific grant agency of the Ministry of Education of the Slovak Republic, and by HRW Natural Health Products Inc., have the following affiliations:
- Centre of Experimental Medicine, Institute for Heart Research, Slovak Academy of Sciences, Bratislava, Slovak Republic.
- Molecular Hydrogen Institute, Enoch, UT, USA.
- Hospital and Research Institute, Moradabad, India.
- Era Medical College, Lucknow, India.
- Applied Bioenergetics Lab, Faculty of Sport and PE, University of Novi Sad, Novi Sad, Serbia.
- Faculty of Health Sciences, University of Pécs, Pécs, Hungary.
- Medical Faculty, Pharmacobiochemical Laboratory of 3rd Medical Department, Comenius University Bratislava, Bratislava, Slovakia.
- Laboratory of Pathophysiology, Graduate School of Pharmaceutical Sciences, Kyushu University, Fukuoka, Japan.
- Third Internal Clinic, Faculty of Medicine, Comenius University, Bratislava, Slovakia.
- Center of Nutrition Research, International College of Nutrition, Moradabad, India.
In the last two years, the 1st author of this new trial has published over a dozen expeimental papers on HRW; all of them report positive findings. Whenever I see a treatment that never fails to produce positive results, regardless of the conditions it is applied to, I start asking myself, are these findings not too good to be true?
Am I the only one to smell a rat?
When I started this blog almost precisely 8 years ago, I had no idea that I would take to it. Those who know me personally would probably confirm that I and a blog go about as well together as fire and water. But here we are:
THIS IS POST NUMBER 2000!
Unquestionably, this is a reason to celebrate. And I have decided that I will do this with a ‘homeopathic proving’. If you have followed some of the recent comments, there are some who cannot stop telling me that I must do a proving, otherwise I understand nothing about homeopathy. I have repeatedly replied that I have done my share of provings but they never produced any result. The homeopathy-fans then wanted to have proof of my provings, and I answered that there is no proof. Then they wanted to know the exact details, but I cannot remember them because they were some 35 years ago. Consequently, they imply that I am a liar. This does not bother me much; on the contrary, according to the ‘like cures like’ assumption, this must mean that I am a 100% truthful person. So, I am flattered by their insinuations.
Anyway, the occasion of POST NUMBER 2000 calls for Champagne – more precisely, for homeopathic Champagne.
Yes, there is such a remedy
Provings are best carried out with the mother tincture. So, in anticipation of today, my wife and I invited two friends to conduct a proving on a bottle on Dom Perignon 2008. Expensive stuff, I know, but good science has never been cheap.
As we opened the bottle, the excitement reached fever pitch. The bouquet was perfect, the robe elegant, the bubbles fine and steady. As the first drops reached out lips, we were transported to Champagne heaven! Patiently we waited for the first symptoms to show: nothing!
Perhaps it’s a question of dose, I thought and refilled the glassed. Nobody protested.
If anything, the second glass was even better.
We waited.
Then, suddenly, the first symptoms seemed to appear: one of us started giggling without apparent reason. Soon all of us normally very introvert people started laughing, talking, relaxing, being sociable. As a good scientist, I noted all this down to generate a proper drug picture of the remedy.
The third glass was greeted with impatience. At this stage we were in full swing: we laughed, told jokes and had a good time. I carried on making notes discretely, while everyone was enjoying themselves. To my shame, I have to admit that, at that stage, we broke off the Champagne proving by opening and consuming a bottle of red wine.
The next day, I looked at my notes and composed the following drug picture of Champagne:
- unmotivated giggling,
- laughing,
- being sociable,
- telling jokes,
- having a good time,
- being relaxed.
The question that the world of homeopathy is dying to get answered is, of course, what must a patient suffer from to be effectively treated with homeopathic Champagne? Well, thanks to my homoeopathically trained mind and my thoroughly developed scientific method, I am now in a position to answer it: if you patient is happy, sociable, relaxed and generally has a good time, you, dear homeopath, must urgently prescribe homeopathic Champagne to stop all this and turn him into a uptight sociopath who hates life.
PS
I know very well that the success of my blog is due to the interesting comments it receives.
So:
THANKS EVERYONE!
.
A number of German health insurances are offering integrated care contracts for homeopathy (ICCHs) that cover the reimbursement of homeopathy. But the effectiveness and cost-effectiveness of these contracts are highly questionable. Now a team of German researchers evaluated the effectiveness and cost-effectiveness of treatment after an additional enrolment in an ICCH in a comparative, prospective, observational study (sponsored by the health insurance company Techniker Krankenkasse).
The participants in the ICCH (HOM group) were compared with matched (on diagnosis, sex and age) insured individuals (CON group) who received usual care alone. Those insured with either
- migraine or headache,
- allergic rhinitis,
- asthma,
- atopic dermatitis,
- depression
were included. Primary effectiveness outcomes were the baseline adjusted scores of diagnosis-specific questionnaires (e.g. RQLQ, AQLQ, DLQI, BDI-II) after 6 months. Primary cost-effectiveness endpoints were the baseline adjusted total costs from an insurer perspective in relation to the achieved quality-adjusted life years (QALYs). Costs were derived from health claims data and QALYs were calculated based on SF-12 data.
Data from 2524 participants (1543 HOM group) were analysed. The primary effectiveness outcomes after 6 months were statistically significant in favour of the HOM group for:
- migraine or headache (Δ = difference between groups, days with headache: – 0.9, p = 0.042),
- asthma (Δ-AQLQ(S): + 0.4, p = 0.014),
- atopic dermatitis (Δ-DLQI: – 5.6, p ≤ 0.001),
- depression (Δ-BDI-II: – 5.6, p ≤ 0.001).
Only the BDI-II differences reached the minimal clinically important difference.
For all diagnoses, the adjusted mean total costs over 12 months were higher in the HOM group from an insurer perspective, with
- migraine or headache,
- atopic dermatitis,
- depression
suggesting cost-effectiveness in terms of additional costs per QALY gained.
The authors concluded that after an additional enrolment in the ICCH, the treatment of participants with depression showed minimally clinically relevant improvements. From an insurer perspective, treatment with an ICCH enrolment resulted in higher costs over all diagnoses but seemed to be cost-effective for migraine or headache, atopic dermatitis and depression according to international used threshold values. Based on the study design and further limitations, our findings should be considered cautiously and no conclusions regarding the effectiveness of specific treatment components can be made. Further research is needed to overcome limitations of this study and to confirm our findings.
Normally, I find newly published studies by conducting Medline searches. This one, I found because the insurance company in question, the Techniker Krankenkasse, is already using it for their advertising. No wonder – this is not a scientific study but a clever marketing coup!
THE RESULTS OF THIS ‘STUDY’ WERE CLEAR, EVEN BEFORE THE FIRST PATIENT WAS RECRUITED.
Imagine you are a patient with one of the 5 conditions listed above, and you evidently like homeopathy – so much so that you approach your insurance and ask to get cover for homeopathy at extra cost to yourself. These were the patients of experimental group. They were compared to patients who could not care less about homeopathy and thus did not get this extra cover.
Who do you think claims to feel better in a self-administered questionnaire?
Is there anyone surprised at the findings of this study?
Well, actually I am a little surprised. Not that the results were positive, but that the results were not more positive. With such a monsterous bias built in the ‘study’, I would have expected much larger differences.
And I am surprised about something else too: how come BMC Health Services Research publishes such promotional marketing masquerading as scientific research?
This clever marketing coup can in no way determine the effectiveness of homeopathy. For that, we need RCTs of which there are already plenty; and we all know what they show: the effects of homeopathy are indistinguishable from those of placebo.
This means there is no proven effectiveness. And what did the director of NICE England once tell me?
WHERE THERE IS NO EFFECTIVENESS, THERE CAN ALSO BE NO COST-EFFECTIVENESS!
Across the world, researchers are frantically trying to find a treatment for COVID-19. Thus many trials have been initiated – and some are better than others.
The aim of this study was to develop a new Chinese medicine (CM)-based drug and to evaluate its safety and effect for suppressing acute respiratory distress syndrome (ARDS) in COVID-19 patients.
A putative ARDS-suppressing drug Keguan-1 was evaluated in a randomized, controlled two-arm trial. The two groups were:
- A control therapy receiving alpha interferon inhalation, 50 µg twice daily; and lopinavir/ritonavir, 400 and 100 mg twice daily, respectively.
- The experimental group receiving the control therapy plus Keguan-1 19.4 g twice daily. The new formula was derived from 3 different formulae, Yinqiao Powder (银翘散), Sangju Drink (桑菊饮), and Sanren Decoction (三仁汤), named “Keguan-1” (meaning anti-coronavirus 1 in Chinese) with 7 components: Lonicera japonica Thunb. (Jinyinhua, lot. 19040301) 30 g, Forsythia suspensa (Thunb.) Vahl, (Lianqiao, lot. 19040221) 30 g, Morus alba L. (Sangye, lot. 19045321) 15 g, Chrysanthemum morifolium Ramat. (Juhua, lot. 19040811) 10 g,
Coix lacryma-jobi L. var. mayuen (Roman.) Stapf, Yiyiren, lot. 19025161) 30 g, Fritillaria thunbergii Miq. (Zhebeimu, lot. 19041161) 15 g, and Prunus armeniaca L. var. ansu Maxim. (Kuxingren, lot. 19045591) 9 g. The powder versions of the drugs for the 7 components of Keguan-1 were obtained from Beijing Tcmages Pharmaceutical Co. Ltd. (Beijing, China) and mixed in the defined ratio.
After 2-week treatment, adverse events, time to fever resolution, ARDS development, and lung injury on newly diagnosed COVID-19 patients were assessed.
An analysis of the data from the first 30 participants showed that the control arm and the testing arm did not exhibit any significant differences in terms of adverse events. Based on this result, the study was expanded to include a total of 48 participants (24 cases each arm).
The results show that, compared with the control arm, the experimental group exhibited a significant improvement in time to fever resolution (P=0.035), and a significant reduction in the development of ARDS (P=0.048).
The authors (who almost out-number the patients in the study) concluded that Keguan-1-based integrative therapy was safe and superior to the standard therapy in suppressing the development of ARDS in COVID-19 patients.
The mixture used in this trial is adventurous, to put it mildly (although the authors state that they report the development of a TCM-medicine “We have reported here the development of Keguan-1, a new CM drug that was specifically designed for suppressing ARDS development in patients of COVID-19 and/or of other RDI” they actually do nothing of the sort). The trial design is flimsy, to put it politely. And the conclusion is unjustified, to put it scientifically.
One might even say that – pandemic or not – it is irresponsible to conclude from a sample size of 2 x 24 on the safety and efficacy of any therapy – TCM or not.
Excessive eccentric exercise of inadequately conditioned skeletal muscle results in focal sites of injury within the muscle fibres.  These injuries cause pain which usually is greatest about 72 hours after the exercise. This type of pain is called delayed-onset muscle soreness (DOMS) and provides an accessible model for studying the effects of various treatments that are said to have anaesthetic activities; it can easily be reproducibly generated without lasting harm or ethical concerns.
These injuries cause pain which usually is greatest about 72 hours after the exercise. This type of pain is called delayed-onset muscle soreness (DOMS) and provides an accessible model for studying the effects of various treatments that are said to have anaesthetic activities; it can easily be reproducibly generated without lasting harm or ethical concerns.
In so-called alternative medicine (SCAM) DOMS is employed regularly to test treatments which are promoted for pain management. Thus several acupuncture trials using this method have become available. Yet, the evidence for the effects of acupuncture on DOMS is inconsistent which begs the question whether across all trials an effects emerges.
The aim of this systematic review therefore was to explore the effects of acupuncture on DOMS. Studies investigating the effect of acupuncture on DOMS in humans that were published before March 2020 were obtained from 8 electronic databases. The affected muscles, groups, acupuncture points, treatment sessions, assessments, assessment times, and outcomes of the included articles were reviewed. The data were extracted and analysed via a meta-analysis.
A total of 15 articles were included, and relief of DOMS-related pain was the primary outcome. The meta-analysis showed that there were no significant differences between acupuncture and sham/control groups, except for acupuncture for DOMS on day 1 (total SMD = -0.62; 95% CI = -1.12∼0.11, P < 0.05) by comparing with control groups.

The authors concluded that acupuncture for DOMS exhibited very-small-to-small and small-to-moderate effects on pain relief for the sham and no acupuncture conditions, respectively. Evidence indicating the effects of acupuncture on DOMS was little because the outcome data during the follow-up were insufficient to perform an effective meta-analysis.
A mere glance at the Forrest plot reveals that acupuncture is unlikely to have any effect on DOMS at all. The very small average effect that does emerge originates mainly from one outlier, the 2008 study by Itoh et al. This trial was published by three acupuncturists from the Department of Clinical Acupuncture and Moxibustion, Meiji University of Integrative Medicine, Kyoto, Japan. It has numerous weaknesses, for instance there are just 10 volunteers in each group, and can therefore be safely discarded.
In essence, this means that there is no good evidence that acupuncture is effective at reducing pain caused by DOMS.
As mentioned already yesterday, NICE published a draft report on pain treatments. The draft is now open to public consultation until 14 September 2020, and some of my readers might want to comment. It suggests that people with chronic primary pain (CPP) should not get pain-medication of any type, but be offered supervised group exercise programmes, some types of psychological therapy, or acupuncture.
No recommendation is made for manual therapy, but a lengthy document evaluates with the subject in some detail. Here are what I consider to be the key passages from its clinical evidence section:
Mixed modality manual therapy versus usual care/acupuncture/dry needling
Pain reduction
Low quality evidence from 2 studies with a total of 52 participants showed no clinically important difference between mixed modality manual therapy and usual care at time points up to 3 months. Low quality evidence from 1 study with a total of 33 participants showed a clinically important benefit of mixed modality manual therapy over usual care at time points after 3 months. Low quality evidence from 1 study with a total of 26 participants showed no clinically important difference between mixed modality manual therapy and acupuncture/dry needling at time points up to 3 months.
Soft tissue technique versus usual care/acupuncture/dry needling
Pain reduction
Low quality evidence from 3 studies with a total of 286 participants showed a clinically important benefit of soft tissue technique over usual care at time points up to 3 months. Very low quality evidence from 2 studies with a total of 115 participants showed a clinically important benefit of acupuncture/dry needling over soft tissue technique at time points up to 3 months.
Manipulation/mobilisation versus usual care/acupuncture/dry needling
Pain reduction
Low quality evidence from 1 study with a total of 30 participants showed a clinically important benefit of manipulation/mobilisation over usual care at time points up to 3 months. Very low quality evidence from 1 study with a total of 24 participants showed no clinically important difference between manipulation/mobilisation and acupuncture/dry needling at time points up to 3 months.
Manual therapy interventions compared with each other
Pain reduction
Moderate quality evidence from 1 study with a total of 63 participants showed a clinically important benefit of mixed modality manual therapy over soft tissue technique at time points up to 3 months. Low quality evidence from 1 study with a total of 63 participants showed a clinically important benefit of mixed modality manual therapy over soft tissue technique at time points after 3 months. Low quality evidence from 1 study with a total of 30 participants showed a clinically important benefit of mixed modality manual therapy over manipulation/mobilisation at time points up to 3 months. Very low quality evidence from 3 studies with a total of 125 participants showed a clinically important benefit of manipulation/mobilisation over soft tissue technique at time points up to 3 months. Low quality evidence from 1 study with a total of 68 participants showed no clinically important difference between manipulation/mobilisation and soft tissue technique at time points after 3 months.
In my view, this is a sound assessment of effectiveness. Nonetheless, I should to mention a few critical points.
Manual therapy is a very heterogeneous group of interventions. Massage and spinal manipulation, for instance, are very different in almost every respect. It would therefore be more constructive to name the techniques more precisely. Evaluating them together makes little sense to me and is hardly different from an assessment of all pharmacological treatments.
Much more important is the fact that the document lacks an assessment of harms. All I did find was a comment saying ‘THERE WAS NO EVIDENCE OF HARM’. This statement is certainly misleading. Perhaps the clinical trials did not report adverse effects, but this is (as I have often pointed out) because these studies usually defy research ethics by failing to mention them. As we have discussed ad nauseam on this blog (for instance here, here and here), spinal manipulation has regularly been associated with severe harms many times.
As NICE do not suggest to recommend manual therapy for CPP, this is perhaps not so crucial in this particular instance. However, I do believe that, for completeness of the evidence as well as for the credibility of the research, an in-depth assessment of the risks is paramount when it comes to the assessment of any therapy.
ANDREW WAKEFIELD has been mentioned on this blog before (see here and here, for instance). He is, of course, the UK doctor who published false data about vaccination and autism in the Lancet, was struck off the medical register, and then moved to the US where he has become the darling of anti-vaxxers of all types, including Donald Trump, chiropractors and homeopaths. More recently, he seems to have become the star and guru of the growing cult opposing a vaccination against COVID-19, even before one has become available.
Already in March, Wakefield attended an anti-vaxx meeting and told those watching: “One of the main tenets of the marketing of mandatory vaccination has been fear. And never have we seen fear exploited in the way that we do now with the coronavirus infection.”
Citing what he called ‘unambiguous’ evidence that the coronavirus is no more deadly than seasonal flu, and claiming that the pathogen’s death toll had been greatly exaggerated, Wakefield more recently claimed that the crisis had led to ‘a destruction of the economy, a destruction of people and families, and unprecedented violations of health freedom… and it’s all based upon a fallacy’.
The disgraced ex-doctor noted that the COVID-19 pandemic is one big hoax: a cynical plot by pharmaceutical giants — aided by governments, scientists and the media — to force the world to be unnecessarily and dangerously vaccinated. Describing vaccines as ‘intrinsically unsafe’, ex-doctor Wakefield called on free-thinking people to refuse to be vaccinated against Covid-19 if and when a jab becomes available.
‘We have to stand and fight,’ the 63-year-old intoned. ‘As Nelson Mandela said at his trial, there are ideals worth dying for . . . I don’t want to get too dramatic, but better to die as a free man than live as a slave . . . We have to fight to preserve [our] freedom because it will be surely stripped from us in a very short space of time if we don’t.’
Convincing his disciples that he was the victim of a conspiracy by the pharmaceutical industry, medical establishment and media, Wakefield now neatly argues that the same shadowy cabal are lying to the public about coronavirus. Having terrified one generation of parents — leading, some believe, to a spike in measles among children and a number of deaths in countries where a minority have promoted his claims — Wakefield is spreading fear and misinformation again.
And the anti-vaxxers are proving alarmingly successful. It has been estimated that around 60 million people subscribe to anti-vaxx propaganda. It is conceivable therefore that these science-deniers could seriously undermine efforts to tackle the current pandemic effectively.
A reader of this blog reminded me of the fact that I have so far not written anything about VAT (thanks Kathryn) – no, not ‘value added tax’ but Vibroacoustic Sound Therapy. This so-called alternative therapy (SCAM) uses sound and vibrations and is promoted mainly for:
- reducing stress,
- relieving pain,
- improving sleep,
- ‘restoring balance’ (bank balance of the therapist?),
- and enhancing the quality of life.
The VAT frequencies range between 30Hz and 120Hz and are applied directly to the body through a treatment table topped with a water-filled mattress. If you go on the Internet, you will find that there are lots of devices you can buy, if you want to do the therapy at home.
Like so many other SCAMs, VAT is claimed to work with resonant frequency whereby our cells copy vibrations they are exposed to. VAT is said to introduce the healthy vibration of cells into the body. This results in a healthy resonant response in our cells, VAT-proponents claim. Over 100 customized frequencies can be employed to address specific health problems.
Yes, you are right: this is about as genuine as a £4 note.
Those practitioners offering VAT sessions claim that the best results occur with cumulative sessions for between 10 – 12 weeks and recommend a minimum treatment schedule of 8 weeks for the majority of cases, either once or twice per week. In view of the fact that these would-be healthcare professionals want to make a living, this seems almost modest, in my view. But, as they are keen to point out, more chronic conditions require 2-3 times per week.
Any evidence?
I found plenty of statements arguing that VAT is solidly evidence-based. However, when I searched for it, I failed to locate anything other than uncontrolled studies, pilot studies and promotional articles of VAT. I admit that I did not spend much time looking (it somehow did not seem worth the effort); it is therefore possible that I missed the definitive RCT of VAT. If someone knows of a piece of conclusive evidence, I’d be most thankful to learn about it.
Under the heading ‘Who should not receive vibroacoustic therapy?’ one VAT practitioner listed several contra-indications for VAT:
• Individuals with Pacemakers
• People with very low blood pressure
• People with a DVT, bleeding disorder, or recent surgery
• Individuals who have had a recent psychotic episode
To this list, I would urgently add this: individuals who are capable of critical thinking!!!
I was surprised to see a paper entitled ‘Yogurt Intake Reduces All-Cause and Cardiovascular Disease Mortality‘ in the current issue of the Chinese Journal of Integrative Medicine. My surprise turned into disbelief when I read the abstract. Here it is in its unabbreviated beauty:
Objective
To assess the relationship between yogurt intake and mortality risk from prospective cohort studies.
Methods
The PubMed, EMBASE, and Web of Science databases were searched for all records related to yogurt intake and mortality risk [all-cause or cardiovascular disease (CVD) or cancer mortality] before October 1, 2018. The Newcastle-Ottawa Quality Scale was used to estimate the quality of all eligible articles. The results of the highest and lowest categories of yogurt intake in each study were collected and the effect size was pooled using a random effects model. The dose-response analysis was calculated using the generalized least squares trend estimation model.
Results
Eight eligible cohort studies were included in this meta-analysis. There were 235,676 participants in the 8 studies, and the number of deaths was 14,831. Compared with the lowest category, the highest category of yogurt intake was not significantly related with all-cause mortality [hazard ratio (HR)=0.93; 95% confidence interval (CI): 0.85, 1.01], CVD mortality (HR=0.92; 95% CI: 0.81, 1.03) and cancer mortality (HR=0.97; 95% CI: 0.83, 1.12). These studies were homogenous, since the homogeneity test showed that I2 was 28.7%, 15.1% and 11.8%, respectively. However, yogurt intake ⩾200 g/d was significantly associated with a lower all-cause mortality (HR=0.88; 95% CI: 0.80, 0.96) and CVD mortality (HR=0.87; 95% CI: 0.77, 0.99) in the subgroup analysis. The dose-response analysis showed that yogurt intake of 200 g/d was inversely associated with all-cause mortality (P=0.041, HR=0.95, 95% CI: 0.92, 1.00) and CVD mortality (P=0.009, HR=0.92, 95% CI: 0.86, 0.98), and all of which were linear relationship (P>0.05).
Conclusions
This review provided the evidence regarding yogurt intake can reduce all-cause and CVD mortality. Although some positive findings were identified, more high-quality cohort studies and randomized controlled trials are warranted on a possible protective effect of yoghurt on health.
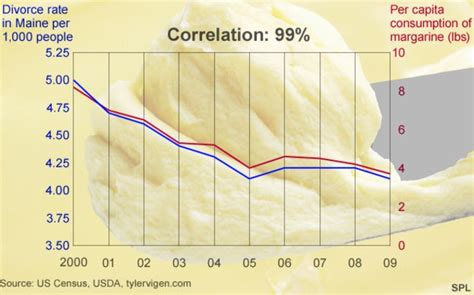
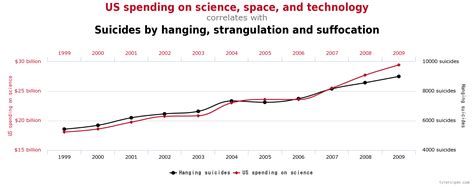

As the above three graphs indicate (and as researchers learn in their first lesson of statistics),
CORRELATION IS NOT CAUSATION.
We all know that, of course – except those of us who work in the so-called alternative medicine (SCAM), it seems – and except the editors of Chinese Journal of Integrative Medicine or the people who do the peer-reviewing for this publication. How else would we explain that a conclusion such as yogurt intake can reduce all-cause and CVD mortality can get published (not to mention the title of the paper)?
But what is the explanation of the intriguing association discovered by the authors of this paper? As far as I can see, there are several possibilities:
- The investigators could be correct, and the link could indeed be causal (in this case, they need to prove it).
- The finding could be coincidental, due to random noise (there are hundreds of epidemiological studies, and they tend to report mainly positive associations [big fishing expeditions really]; thus, it is conceivable that 8 of them found an association where in truth none exists).
- It could be that people who eat a yoghurt tend to not eat a ‘full English’ for breakfast, thus avoiding the harm of unhealthy nutrition)
- Similarly, it might be that yoghurt consumers care more about their health in general (including exercise, body weight, smoking, etc.) than those who shun yoghurt.
And how do we decide which explanation applies? The answer is simple: by doing proper research and drawing appropriate conclusions from it.
Perhaps something like this?
Background: Although a link between regular yogurt consumption and mortality appears plausible, data are sparse and have yielded inconsistent results.
Objectives: We examined the association between regular yogurt consumption and risk of all-cause and cause-specific mortality among US women and men.
Methods: A total of 82,348 women in the Nurses’ Health Study and 40,278 men in the Health Professionals Follow-Up Study without a history of cardiovascular disease (CVD) and cancer in 1980 (women) or 1986 (men) were followed up until 2012. Yogurt consumption was assessed by updated validated FFQs.
Results: During 3,354,957 person-years of follow-up, 20,831 women and 12,397 men died. Compared with no yogurt consumption, the multivariable-adjusted HRs (95% CIs) of mortality were 0.89 (0.86, 0.93), 0.85 (0.81, 0.89), 0.88 (0.84, 0.91), and 0.91 (0.85, 0.98) for ≤1-3 servings/mo, 1 serving/wk, 2-4 servings/wk, and >4 servings/wk in women (P-trend = 0.34), respectively. For men, the corresponding HRs (95% CIs) were 0.99 (0.94, 1.03), 0.98 (0.91, 1.05), 1.04 (0.98, 1.10), and 1.05 (0.95, 1.16), respectively. We further noted inverse associations for cancer mortality (multivariable-adjusted HR comparing extreme categories: 0.87; 95% CI: 0.78, 0.98; P-trend = 0.04) and CVD mortality (HR: 0.92; 95% CI: 0.79, 1.08; P-trend = 0.41) in women, although the latter was attenuated in the multivariable-adjusted model. Replacement of 1 serving/d of yogurt with 1 serving/d of nuts (women and men) or whole grains (women) was associated with a lower risk of all-cause mortality, whereas replacement of yogurt with red meat, processed meat (women and men), and milk or other dairy foods (women) was associated with a greater mortality.
Conclusions: In our study, regular yogurt consumption was related to lower mortality risk among women. Given that no clear dose-response relation was apparent, this result must be interpreted with caution.
_________________________
I rest my case.
I started my full-time research into so-called alternative medicine (SCAM) at Exeter in 1993. It became soon clear to me that the most urgent subject to investigate was the safety of SCAM. Safety is more important than efficacy for treatments that are already out there. My decision to prioritise safety quickly led to the bewilderment of the SCAM community. They pointed out that SCAM was safe and that the true risks in healthcare were with conventional medicine. Belief was strong, but data were scarce.
My counter arguments therefore were:
- Safety is too important a subject to leave it to belief, and we need evidence.
- SCAM is hugely popular and it was my ethical duty to provide data on safety.
The SCAM community were unconvinced by my logic. But that did not stop me.
In the course of dozens of investigations, we then found that adverse effects of SCAM do exist and some can be quite dramatic. Again, I was told that this might be so, but the real dangers surely lie elsewhere, namely in conventional medicine.
Meanwhile, I began to find that, while the direct risks of SCAM were real, the indirect risks were much more important. During virtually every talk I gave and in most papers I published, I started including this message:
EVEN A HARMLESS SCAM WILL BECOME LIFE-THREATENING, IF IT IS USED AS AN ALTERNATIVE TO CONVENTIONAL CARE FOR A SERIOUS CONDITION.
Even though the statement seems quite clear, it does not really capture the complexity of the issues involved. Let’s take (yet again) the example of homeopathy (because it is one of the most clear-cut cases).
The remedy is normally harmless; after all it contains nothing. Therefore, there are no or very few adverse effects. If a patient is naïve enough to use homeopathy in an attempt to cure a life-threatening condition, it is hardly the fault of homeopathy – at least this is what some defenders of the homeopathic realm claim. So why blame homeopathy?
Indeed, this could be unfair, because then we would have to say that water is dangerous because you can easily kill yourself with it.
But the water companies do not recommend abusing water for suicidal purposes!
And homeopaths do unquestionably recommend homeopathy for serious conditions!
So, it is not the remedy and not homeopathy itself that makes it dangerous. What makes it risky is the combination of two things:
- the inertness of the remedy
- the unsubstantiated claims that are being made for it.
The two together create a potentially deadly mixture. Without false claims, nobody could classify homeopathy as life-threatening. Due to the plethora of false claims, nobody can reasonably deny that it is.
What follows is simple, I think: one would only need to stop the claims. Subsequently, homeopathy – and many other forms of SCAM – could be classified as harmless (yes, I know, this is purely theoretical because in practice this will never happen). They would still be ineffective, of course, but safety was and is the priority.