progress
Nausea and vomiting are common symptoms of patients with advanced cancer. While there is some evidence for acupuncture point stimulation in the treatment of these symptoms for patients having anticancer treatment, there is little for when they are not related to such treatment.
This study aimed to determine whether acupressure at the pericardium 6 sites can help treat nausea and vomiting suffered by palliative care patients with advanced cancer. The researchers conducted a double-blind randomized controlled trial-active versus placebo acupressure wristbands. In-patients with advanced cancer in two specialist palliative care units who fitted either or both of the following criteria were approached: nausea that was at least of moderate severity; vomiting daily on average for the prior 3 days.
A total of 57 patients were randomized to have either active or placebo acupressure wristbands. There was no difference in any of the outcome measures between the two groups:
- change from the baseline number of vomits;
- Visual Analogue Scale for ‘did acupressure wristbands help you to feel better?’;
- the total number of doses of antiemetic medication;
- the need for escalation of antiemetics.
The authors concluded that, in contrast to a previously published feasibility study, active acupressure wristbands were no better than placebo for specialist palliative care in patients with advanced cancer and nausea and vomiting.
When the research into acupuncture for nausea and vomiting began some 20 years ago, the evidence turned out to be encouraging. Later, as the studies became more and more rigorous, many trials failed to confirm the initial findings. Today, the totality of the evidence is far less convincing than it seemed years ago.
This is a phenomenon that can be observed not just in acupuncture research but in many types of treatment:
- Initially, over-enthusiastic researchers become victims of their own optimism.
- These investigators are less into testing hypotheses than into confirming their own wishful thinking.
- Thus, several positive trials emerge.
- These, however, turn out to be methodologically flawed.
- Eventually, the subject might be picked up by real scientists who truly test hypotheses.
- More and more negative studies thus emerge.
- Depending on how many flawed studies were initially published and how critical the authors of systematic reviews are, it can take years until the totality of the evidence depicts the true picture which discloses the initial findings as false-positive.
The message is, I think, clear: poor quality studies have the potential to mislead us for many years. Eventually, however, the self-cleansing ability of science should generate the truth about the value of any treatment. In other words:
poor-quality science is not just useless, it causes long-term harm
and
critical thinking prevents harm
In a previous post, I reported about the ‘biggest ever’, ‘history-making’ conference on integrative medicine. It turns out that it was opened by none other than Prince Charles. Here is what the EXPRESS reported about his opening speech:
Opening the conference, Charles said:
“I know a few people have seen this integrated approach as being in some way opposed to modern medicine. It isn’t. But we need to combine this with a personal approach that also takes account of our beliefs, hopes, culture and history. It builds upon the abilities of our minds and bodies to heal, and to live healthy lives by improving diet and lifestyle.”
Dr. Michael Dixon, Chair of the College of Medicine, said:
“Medicine, as we know it, is no longer affordable or sustainable. Nor is it able to curb the increase in obesity, mental health problems and most long-term diseases. A new medical mindset is needed, which goes to the heart of true healthcare. The advantages and possibilities of social prescription are limitless. An adjustment to the system now will provide a long-term, sustainable solution for the NHS to meet the ever-increasing demand for funding and healthcare professionals.”
_______________________
Charles very kindly acknowledges that not everyone is convinced about his concept of integrated/integrative medicine. Good point your royal highness! But I fear Charles did not quite understand our objections. In a nutshell: it is not possible to cure the many ills of conventional medicine by adding unproven and disproven therapies to it. In fact, it distracts from our duty to constantly improve conventional medicine. And pretending it is all about diet and lifestyle is simply not true (see below). Moreover, it is disingenuous to pretend that diet and lifestyle do not belong to conventional healthcare.
Dr. Dixon’s concern about the affordability of medicine is, of course, justified. But the notion that “the advantages and possibilities of social prescription are limitless” is a case of severe proctophasia, and so is Dixon’s platitude about ‘adjusting the system’. His promotion of treatments like Acupuncture, Alexander Technique, Aromatherapy, Herbal Medicine, Homeopathy, Hypnotherapy, Massage, Naturopathy, Reflexology, Reiki, Tai Chi, Yoga Therapy will not adjust anything, it will only make healthcare less efficient.
I do not doubt for a minute that doctors are prescribing too many drugs and that we could save huge amounts by reminding patients that they are responsible for their own health while teaching them how to improve it without pills. This is what we learn in medical school! All we need to do is remind everyone concerned. In fact, Charles and his advisor, Michael, could be most helpful in achieving this – but not by promoting a weird branch of healthcare (integrative/integrated medicine or whatever other names they choose to give it) that can only distract from the important task at hand.
Almost 10 years ago, I posted this:
When I decided to become a doctor I, like most medical students, did so mainly to help suffering individuals. When I became a researcher, I felt more removed from this original ideal. Yet I told myself that, by conducting research, I might eventually contribute to a better health care of tomorrow. Helping suffering patients was still firmly on the agenda. But then I realised that my articles in peer-reviewed medical journals somehow missed an important target: in alternative medicine, one ought to speak not just to health care professionals but also to consumers and patients; after all, it is they who often make the therapeutic decisions in this area.
Once I had realised this, I started addressing the general public by writing for The Guardian and other newspapers, giving public lectures and publishing books for a lay audience, like TRICK OR TREATMENT…The more I did this sort of thing, the more I noticed how important this activity was. And when a friend offered to help me set up a blog, I did not hesitate for long.
So, the reason for my enthusiasm for this blog turns out to be the same as the one that enticed me to go into medicine in the first place. I do believe that it is helpful for consumers to know the truth about alternative medicine. Considering the thousands of sources of daily misinformation in this area, there is an urgent need for well-informed, critical information. By providing it, I am sure I can assist people to make better therapeutic decisions. In a way, I am back where I started all those years ago: hoping to help suffering patients in the most direct way my expertise allows.
Helping vulnerable patients often means warning them from dangerous charlatans, and this is precisely what I frequently try to do with this blog. But how successful are my endeavors?
More often than not, I have no idea and can only hope for the best. Sometimes I do get some feedback that is encouraging and motivates me to carry on. Rarely, however, do I witness immediate, tangible success. And this is why the recent story is so remarkable:
- On 6 June, an Australian acquaintance from the FRIENDS OF SCIENCE IN MEDICINE sent me some material about a planned lecture in the UK by someone promoting dangerous quackery.
- I looked into it and published a blog post about it a few hours later.
- A reader then suggested in the comments section of this post alerting the UK press to it.
- Another reader contacted THE TIMES, and I wrote to several other journalists.
- THE TIMES turned out to be interested in the story.
- They did some research and interviewed Michael Marshall from the GOOD THINKING SOCIETY (and myself).
- Today, THE TIMES published an article about the planned event.
- Finally, a kind person made the article available to those who don’t want to pay for it.
The whole thing amounts to superb teamwork, in my view. It shows how like-minded people who do not even all know each other can manage to achieve a respectable result with little more than goodwill and dedication.
A respectable result?
Of course, the optimal result would be to stop Barbara O’Neill’s UK lectures. Let’s hope this is what eventually will happen – and please let me know if you know more.
I know only too well that some readers will interpret this post as pompous and self-congratulatory, but I nevertheless feel like telling my readers that I have become a member of the ACADEMIA EUROPAEA. In case you don’t know what this is, Wikipedia provides the following information:
Membership of the Academia Europaea (MAE) is an award conferred by the Academia Europaea to individuals that have demonstrated “sustained academic excellence”.[2] Membership is by invitation only by existing MAE only and judged during a peer review selection process.[3] Members are entitled to use the post-nominal letters MAE.[4]
New members are announced annually, every year since 1988.[5][6] For a more complete list see Category:Members of Academia Europaea..[7][8][9][10][11] Some Members of the Academia Europaea have received very prestigious awards, medals and prizes, such as:
- The Nobel Prize[12] e.g. Christiane Nüsslein-Volhard (1995, Physiology), Arvid Carlsson (2000, Physiology or Medicine), Paul Nurse (2001, Physiology or Medicine), Tim Hunt (2001, Physiology or Medicine), Kurt Wüthrich (2002, Chemistry), John Sulston (2002, Physiology or Medicine), Sydney Brenner 2002, Physiology or Medicine, Aaron Ciechanover (2004, Chemistry), Roy J. Glauber (2005, Physics), Roger D. Kornberg (2006, Chemistry), Gerhard Ertl (2007, Chemistry), Richard Tol (2007, shared winner of the Nobel Peace Prize), Harald zur Hausen (2008, Physiology or Medicine), Luc Montagnier (2008, Physiology or Medicine), Robert G. Edwards (2010, Physiology or Medicine), John B. Gurdon (2012, Physiology or Medicine), Rita Levi-Montalcini (1986, Physiology)
- The Wolf Prize,[13] e.g. Simon Donaldson (2020), Alexander Beilinson (2018), Peter Zoller (2013), Alain Aspect (2010), Anton Zeilinger (2010), Axel Ullrich (2010), David Baulcombe (2010), Howard Cedar (2008), Albert Fert (2006/2007), Alexander Levitzki (2005), Sergei P. Novikov (2005), Alexander Varshavsky (2001), Saharon Shelah (2001), Vladimir I. Arnold (2001).
- The Turing Award,[14] e.g. Joseph Sifakis (2007), Adi Shamir (2002).
- The Fields Medal,[15] e.g. Martin Hairer (2014), Elon Lindenstrauss (2010), Stanislav Smirnov (2010), Cédric Villani (2010), Wendelin Werner (2006), Timothy Gowers (1998), Maxim Kontsevich (1998), Jean Bourgain (1994), Pierre-Louis Lions (1994), Simon Donaldson (1986), Enrico Bombieri (1974), Sergei P. Novikov (1970), Michael Atiyah (1966).
- The Lasker Award,[16] e.g. Roy Calne (2012), David Weatherall (2010), John Gurdon (2009), David Baulcombe (2008), Alec Jeffreys (2005), Pierre Chambon (2004), Robert Edwards (2001), Sydney Brenner (2000), Aaron Ciechanover (2000), Alexander Varshavsky (2000).
- The Abel Prize,[17] e.g. Andrew Wiles (2016), Endre Szemerédi (2012), Mikhail Leonidovich Gromov (2009), Jacques Tits (2008), Lennart Carleson (2006), Michael Atiyah (2004).
- The Gödel Prize,[18] e.g. Christos H. Papadimitriou (2012), Johan Hastad (2011, 1994), Alexander Razborov (2007), Noga Alon (2005), László Lovász (2001), Moshe Vardi (2000), Pierre Wolper (2000).
________________________________
The Academia Europaea was founded in 1988, on the initiative of the UK’s Royal Society and other National Academies in Europe. It is a `Not for Profit’ Charity registered in the UK. The Academia Europaea is the only Academy with individual members from the Council of Europe states and from other nations across the world. Currently, there are some 5000 members who cover the full range of academic disciplines.
The objectives of the Academia Europaea are the advancement and propagation of excellence in scholarship in the humanities, law, the economic, social, and political sciences, mathematics, medicine, and all branches of natural and technological sciences anywhere in the world for the public benefit and for the advancement of the education of the public of all ages.
The Academy organizes meetings and workshops, provides scientific and scholarly advice, and publishes the international journal the ‘European Review’ and is associated with Biology Direct. It operates regional knowledge hubs out of Barcelona, Bergen, Budapest, Cardiff, Munich, Tbilisi, and Wroclaw, hosted by Universities and National academies.
_______________________________
I am both proud and thankful that I have been honored in this way.
I have been sent a press release dated 26/5/2022 that might interest some of my readers. As it is in German, I took the liberty of translating it:
The 126th German Medical Congress today in Bremen deleted the additional designation of homeopathy from the further education regulations for doctors (MWBO). The request brought by Bremen delegates was decided by the physician parliament with a large majority.
The Bremen delegates justified their request with the fact that 13 of 17 state medical associations have already deleted the additional designation of homeopathy from their further education regulations. The further education regulation is to create uniform rules for the post-graduate training of doctors. However, there is no longer any question of uniformity if 13 state medical associations do not follow the MWBO.
In the debate, Dr. Johannes Grundmann once again pointed out that it is not a matter of prohibiting people from using homeopathic remedies. “However, it is the task of the medical associations to define and check verifiable learning objectives,” Grundmann said to great applause.
In September 2020, the Bremen Medical Association had become the first such chamber in Germany to remove homeopathy from its education regulations. The complaint of a Bremen physician against it had subsequently been rejected in two instances. Most recently, the Bremen health insurance was the first to terminate three selective contracts for the remuneration of homeopathic services.
____________________________
I feel that this is a nice victory of reason over unreason. I might even go as far as assuming that our petition of 2021 might have helped a little to bring it about:
Dear President Dr Reinhardt,
Dear Ms Lundershausen,
Mrs Held,
Dear Ms Johna,
We, the undersigned doctors, would like to draw your attention to the insistence of individual state medical associations on preserving “homeopathy” as a component of continuing medical education. We hope that you, by virtue of your office, will ensure a nationwide regulation so that this form of sham treatment [1], as has already happened in other European countries, can no longer call itself part of medicine.
We justify our request by the following facts:
-
- After the landmark vote in Bremen in September 2019 to remove “homeopathy” from the medical training regulations, 10 other state medical associations have so far followed Bremen’s example. For reasons of credibility and transparency, it would be desirable if the main features of the training content taught were not coordinated locally in the future, but centrally and uniformly across the country so that there is no “training tourism”. Because changes to a state’s own regulations of postgraduate training are only binding for the examination committee of the respective state, this does not affect national regulations but is reduced to only a symbolic character without sufficient effects on the portfolio of medical education nationwide.
- Medicine always works through the combination of a specifically effective part and non-specific placebo effects. By insisting on a pseudo-medical methodology – as is “homeopathy” represents in our opinion – patients are deprived of the specific effective part and often unnecessarily deprived of therapy appropriate to the indication. Tragically, it happens again and again that the “therapeutic window of opportunity” for an appropriate therapy is missed, tumors can grow to inoperable size, etc.
- Due to the insistence of individual state medical associations on the “homeopathic doctrine of healing” as part of the medical profession, we are increasingly exposed to the blanket accusation that, by tolerating this doctrine, we are supporting and promoting ways of thinking and world views that are detached from science. This is a dangerous situation, which in times of a pandemic manifests itself in misguided aggression reflected not just in vaccination skepticism and vaccination refusal, but also in unacceptable personal attacks and assaults on vaccinating colleagues in private practice.
Responsible:
Dr. med. Dent. Hans-Werner Bertelsen
Prof. Dr. med. Edzard Ernst
George A. Rausche
_______________________________________
The first reported reactions from politicians are positive, while those of homeopaths are predictably the opposite:
German Health Minister Karl Lauterbach (SPD) expressly welcomed the delegates’ decision, writing via Twitter. “Good medicine stands on the ground of science. For homeopathy, there is no place there. In such a question, one must show one’s colors.”
Paula Piechotta, a Green Party member of parliament, was equally pleased. “… it is good when in times of Fake Facts and right-wing conspiracy theories clarity is provided where clarity is needed. Thank you Ärztetag,” she tweeted.
Michaela Geiger, chairwoman of the German Central Association of Homeopathic Physicians, noted the decision “with astonishment.” Homeopathy has a high acceptance among the population, she claimed.
Anyone who has followed this blog for a while will know that advocates of so-called alternative medicine (SCAM) are either in complete denial about the risks of SCAM or they do anything to trivialize them. Here is a dialogue between a SCAM proponent (P) and a scientist (S) that is aimed at depicting this situation. The conversation is fictitious, of course, but it is nevertheless based on years of experience in discussing these issues with practitioners of various types of SCAM. As we shall see, the arguments turn out to be perfectly circular.
P: My therapy is virtually free of risks.
S: How can you be so sure?
P: I am practicing it for decades and have never seen a single problem.
S: That could have several reasons; perhaps the patients who experience problems did simply not come back.
P: I find this unlikely.
S: I don’t, and I know of reports where patients had serious complications after the type of SCAM you practice.
P: These are isolated case reports. They do not amount to evidence.
S: How do you know they are isolated?
P: They must be isolated because, in the many clinical trials of my therapy available to date, you will not find any evidence of serious adverse effects.
S: That is true, but it has been repeatedly shown that these trials regularly fail to mention side effects altogether.
P: That’s because there aren’t any.
S: Not quite, clinical trials should always mention adverse effects, and if there were none, they should mention this too.
P: So, you admit that you have no evidence that my therapy causes adverse effects.
S: The thing is, I don’t need such evidence. It is you, the practitioners of this therapy, who should provide evidence that your treatments are safe.
P: We did! The complete absence of reports of side effects constitutes that evidence.
S: Except, there is some evidence. I already told you that there are several case reports of serious problems.
P: But case reports are anecdotes; they are no evidence.
S: Look, here is a systematic review of all the case reports. You cannot possibly deny that this is a concern.
P: It’s still merely a bunch of anecdotes, nothing more.
S: Only because your profession does nothing about it.
P: What do you think we need to do about it?
S: Like other professions, you need to systematically record adverse effects.
P: How would that help?
S: It would give us a rough indication of the size and severity of the problem.
P: This sounds expensive and complicated to organize.
S: Perhaps, but it is necessary if you want to be sure that your therapy is safe.
P: But we are sure already!
S: No, you believe it, but you don’t know it.
P: You are getting on my nerves with your obsession. Don’t you know that the true danger in healthcare is the adverse effects of pharmaceutical drugs?
S: But these drugs are also effective.
P: Are you saying my therapy isn’t?
S: What I am saying is that the drugs you claim to be dangerous do more good than harm, while this is not at all clear with your SCAM.
P: To me, that is very clear. My therapy helps many and harms nobody!
S: How do you know that it harms nobody?
… At this point, we have gone full circle and we can re-start this conversation from its beginning.
A recent article in LE PARISIEN entitled “L’homéopathie vétérinaire, c’est sans effet… mais pas sans risque” – Veterinary homeopathy is without effect … but not without risk, tells it like it is. Here are a few excerpts that I translated for you.
More than 77% of French people have tried homeopathy in their lifetime. But have you ever given it to your pet? Harmless in most cases, its use can be dangerous when it replaces a treatment whose effectiveness is scientifically proven … from a safety point of view, the tiny granules are indeed irreproachable: their use does not induce any drug interaction or undesirable side effects, nor does it run the risk of overdosing or addiction … homeopathic preparations owe their harmlessness to their lack of proper effects. “Neither in human medicine nor in veterinary medicine, at the current stage, clinical studies of all levels do not provide sufficient scientific evidence to support the therapeutic efficacy of homeopathic preparations”, stated the French Veterinary Academy in May 2021. These conclusions are in line with those of the French Academies of Medicine and Pharmacy, the British Royal College of Veterinary Surgeons, and all the international scientific bodies that have given their opinion on the subject.
Therefore, when homeopathy delays diagnosis or is used in place of proven effective treatments, its use represents a “loss of opportunity” for your pet. The greatest danger of homeopathy is not that the remedies are ineffective, but that some homeopaths believe that their therapies can be used as a substitute for genuine medical treatment,” summarizes a petition to the UK veterinary regulatory body signed by more than 1,000 British veterinarians. At best, this claim is misleading and, at worst, it can lead to unnecessary suffering and death.”
But how can we explain the number of testimonies from pet owners who say that “it works”? “I am very satisfied with the Kalium Bichromicum granules for my cat with an eye ulcer, which is healing very well”… These improvements, real or supposed, can be explained by “contextual effects”, among which the famous placebo effect (which is not specific to humans), your subjective interpretation of his symptoms, or the natural history of the disease.
When these contextual effects are ignored or misunderstood, the spontaneous resolution or reduction of the disease can be wrongly attributed to homeopathy, and thus maintain the illusion of its effectiveness. This confusion is all the more likely because homeopathy owes much of its popularity to its use to treat “everyday ailments”: nausea, allergies, fatigue, bruises, nervousness, etc., which tend to get better on their own with time, or which have a fluctuating expression…
In April 2019, the association published an open letter addressed to the National Council of the Order of Veterinarians, calling on it to take a position on the compatibility of homeopathy with the “ethical and scientific requirements” of the profession. The organization, whose official function is to guarantee the quality of the service rendered to the public by the 20,000 veterinarians practicing in France, issued its conclusions last October. It invited veterinary training centers to remove homeopathy from their curricula, under penalty of having their accreditation withdrawn, and thus their ability to deliver training credits.
In my view, this is a remarkably good and informative text. How often do homeopathy fans claim IT WORKS FOR ANIMALS AND THUS CANNOT BE A PLACEBO! The truth is that, as we have so often discussed on this blog, homeopathy does not work beyond placebo for animals. This renders veterinary homeopathy:
- a waste of money,
- potentially dangerous,
- in the worst cases a form of animal abuse.
My advice is that, as soon as a vet recommends homeopathy, you look for the exit.
I know, transcutaneous electrical nerve stimulation (TENS) is not really a so-called alternative medicine (SCAM) but it is used by many SCAM practitioners and pain patients. It is, therefore, worth knowing whether it works.
This systematic review investigated the efficacy and safety of transcutaneous electrical nerve stimulation (TENS) for the relief of pain in adults. All randomized clinical trials (RCTs) were considered which compared strong non-painful TENS at or close to the site of pain versus placebo or other treatments in adults with pain, irrespective of diagnosis.
Reviewers independently screened, extracted data, and assessed the risk of bias (RoB, Cochrane tool) and certainty of evidence (Grading and Recommendations, Assessment, Development, and Evaluation). The outcome measures were the mean pain intensity and the proportions of participants achieving reductions of pain intensity (≥30% or >50%) during or immediately after TENS. Random effect models were used to calculate standardized mean differences (SMD) and risk ratios. Subgroup analyses were related to trial methodology and characteristics of pain.
The review included 381 RCTs (24 532 participants). Pain intensity was lower during or immediately after TENS compared with placebo (91 RCTs, 92 samples, n=4841, SMD=-0·96 (95% CI -1·14 to -0·78), moderate-certainty evidence). Methodological (eg, RoB, sample size) and pain characteristics (eg, acute vs chronic, diagnosis) did not modify the effect. Pain intensity was lower during or immediately after TENS compared with pharmacological and non-pharmacological treatments used as part of standard of care (61 RCTs, 61 samples, n=3155, SMD = -0·72 (95% CI -0·95 to -0·50], low-certainty evidence). Levels of evidence were downgraded because of small-sized trials contributing to imprecision in magnitude estimates. Data were limited for other outcomes including adverse events which were poorly reported, generally mild, and not different from comparators.
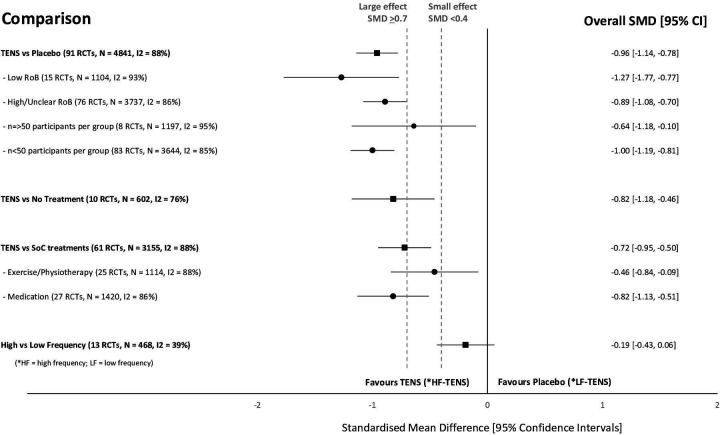
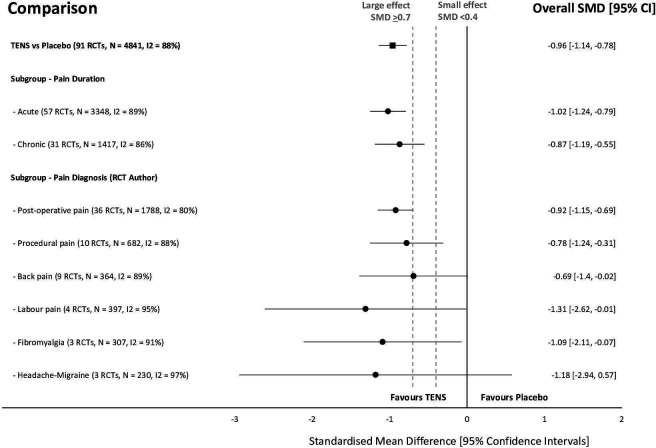
The authors concluded that there was moderate-certainty evidence that pain intensity is lower during or immediately after TENS compared with placebo and without serious adverse events.
This is an impressive review, not least because of its rigorous methodology and the large number of included trials. Its results are clear and convincing. In the words of the authors: “TENS should be considered in a similar manner to rubbing, cooling or warming the skin to provide symptomatic relief of pain via neuromodulation. One advantage of TENS is that users can adjust electrical characteristics to produce a wide variety of TENS sensations such as pulsate and paraesthesiae to combat the dynamic nature of pain. Consequently, patients need to learn how to use a systematic process of trial and error to select electrode positions and electrical characteristics to optimise benefits and minimise problems on a moment to moment basis.”
During the last two years, I have written more often than I care to remember about the numerous links between so-called alternative medicine (SCAM) and COVID-19 vaccination hesitancy. For instance:
- A Professor for Integrative and Anthroposophical Medicine claims that severe adverse effects of COVID vaccinations are 40 times more frequent than officially recognized
- What are the reasons for opposing COVID vaccinations?
- A naturopath promoting fake news about COVID vaccinations
- COVID-19 vaccinations: Prof Walach wants to “dampen the enthusiasm by sober facts”
- A change in diet protects us from severe COVID symptoms – REALLY?
- Intelligence, Religiosity, SCAM, Vaccination Hesitancy – are there links?
- Upper Bavaria is struggling with COVID-19, not least due to so-called alternative medicine
- The International Chiropractors Association’s Statement on Vaccination
- Parents’ Willingness to Vaccinate with a COVID-19 Vaccine: strongly influenced by homeopathy
- “The uncensored truth” about COVID-19 vaccines” … as told by some chiro loons
- Ex-doctor Andrew Wakefield: “Better to die as a free man than live as a slave” (and get vaccinated against Covid-19)
- Is this the crown of the Corona-idiocy? Nosodes In Prevention And Management Of COVID -19
- The rejection of so-called alternative medicine is associated with a higher willingness to get vaccinated
Whenever I publish a post on these subjects, some enthusiasts of SCAM argue that, despite all this evidence, they are not really against COVID vaccinations. But who is correct? What proportions of SCAM practitioners are pro or contra? One way to find out is to check how they themselves behave. Do they get vaccinated or not?
Here are some recent data from Canada that seem to provide an answer.
A breakdown of vaccination rates among Canadian healthcare professions has been released, based on data gathered from 17 of B.C.’s 18 regulated colleges. The findings are most revealing:
- dieticians, physicians, and surgeons lead the way, with vaccination rates of 98%,
- occupational therapists were at 97%,
- Chinese medicine practitioners and acupuncturists were at 79%,
- chiropractors at 78%
- naturopaths at 69%.
The provincial health officer Dr. Bonnie Henry said the province is still working with the colleges on how to notify patients about their practitioner’s vaccination status. “We are working with each college on how to build it into professional standards. The overriding principle is patient status,” she told a news conference. “It may be things like when you call to book, you are asked whether you would prefer to see a vaccinated or unvaccinated professional. We are trying to protect privacy and provide agency to make the decision.”
______________________
As far as I am aware, these are unique data. It would be interesting to see additional evidence. If anyone knows about vaccination rates in other countries of acupuncturists, herbalists, homeopaths, osteopaths, Heilpraktiker, etc. I would love to learn more.
Given the high prevalence of burdensome symptoms in palliative care (PC) and the increasing use of so-called alternative medicine (SCAM) therapies, research is needed to determine how often and what types of SCAM therapies providers recommend to manage symptoms in PC.
This survey documented recommendation rates of SCAM for target symptoms and assessed if, SCAM use varies by provider characteristics. The investigators conducted US nationwide surveys of MDs, DOs, physician assistants, and nurse practitioners working in PC.
Participants (N = 404) were mostly female (71.3%), MDs/DOs (74.9%), and cared for adults (90.4%). Providers recommended SCAM an average of 6.8 times per month (95% CI: 6.0-7.6) and used an average of 5.1 (95% CI: 4.9-5.3) out of 10 listed SCAM modalities. Respondents recommended mostly:
- mind-body medicines (e.g., meditation, biofeedback),
- massage,
- acupuncture/acupressure.
The most targeted symptoms included:
- pain,
- anxiety,
- mood disturbances,
- distress.
Recommendation frequencies for specific modality-for-symptom combinations ranged from little use (e.g. aromatherapy for constipation) to occasional use (e.g. mind-body interventions for psychiatric symptoms). Finally, recommendation rates increased as a function of pediatric practice, noninpatient practice setting, provider age, and proportion of effort spent delivering palliative care.
The authors concluded that to the best of our knowledge, this is the first national survey to characterize PC providers’ SCAM recommendation behaviors and assess specific therapies and common target symptoms. Providers recommended a broad range of SCAM but do so less frequently than patients report using SCAM. These findings should be of interest to any provider caring for patients with serious illness.
Initially, one might feel encouraged by these data. Mind-body therapies are indeed supported by reasonably sound evidence for the symptoms listed. The evidence is, however, not convincing for many other forms of SCAM, in particular massage or acupuncture/acupressure. So encouragement is quickly followed by disappointment.
Some people might say that in PC one must not insist on good evidence: if the patient wants it, why not? But the point is that there are several forms of SCAMs that are backed by good evidence for use in PC. So, why not follow the evidence and use those? It seems to me that it is not in the patients’ best interest to disregard the evidence in medicine – and this, of course, includes PC.