critical thinking
My ‘ALTERNATIVE MEDICINE HALL OF FAME’ is filling up nicely. But I noticed that so far we have nobody from Spain. That can be rectified ever so easily. I think I found the ideal candidate to join this group of illustrious experts who never bring themselves to publish a negative conclusion: JORGE VAS.
Jorge Vas works at the ‘Pain Treatment Unit, Doña Mercedes Primary Health Care Center, Dos Hermanas’ in Spain. I have long noticed his research which is focused on ACUPUNCTURE. From memory, I had the impression that his findings are always positive.
But is this true? To find out, I did a Medline search and found 11 clinical trials of acupuncture in his name, published between 2006 and 2019. Here are the conclusions:
- After 2 weeks of treatment, ear acupuncture applied by midwives and associated with standard obstetric care significantly reduces lumbar and pelvic pain in pregnant women, improves quality of life and reduces functional disability.
- Individualised acupuncture treatment in primary care in patients with fibromyalgia proved efficacious in terms of pain relief, compared with placebo treatment. The effect persisted at 1 year, and its side effects were mild and infrequent. Therefore, the use of individualised acupuncture in patients with fibromyalgia is recommended.
- The use of acupuncture to treat impingement syndrome seems to be a safe and reliable technique to achieve clinically significant results and could be implemented in the therapy options offered by the health services.
- …all 3 modalities of acupuncture were better than conventional treatment alone…
- Moxibustion treatment applied at acupuncture point BL67 can avoid the need for caesarean section and achieve cost savings for the healthcare system in comparison with conventional treatment.
- The application of auriculopressure in patients with non-specific spinal pain in primary healthcare is effective and safe, and therefore should be considered for inclusion in the portfolio of primary healthcare services.
- The degree of pain relief experienced by patients from acupuncture justifies a more rigorous study.
- Moxibustion at acupuncture point BL67 is effective and safe to correct non-vertex presentation when used between 33 and 35 weeks of gestation. We believe that moxibustion represents a treatment option that should be considered to achieve version of the non-vertex fetus.
- Single-point acupuncture in association with physiotherapy improves shoulder function and alleviates pain, compared with physiotherapy as the sole treatment. This improvement is accompanied by a reduction in the consumption of analgesic medicaments.
- Acupuncture plus diclofenac is more effective than placebo acupuncture plus diclofenac for the symptomatic treatment of osteoarthritis of the knee.
- In the treatment of the intensity of chronic neck pain, acupuncture is more effective than the placebo treatment and presents a safety profile making it suitable for routine use in clinical practice.
Eleven of 11 trials with a positive conclusion!
That surely is a rare feast.
Actually, I cheated a tiny bit. The unabridged sentence from the conclusion of paper N4 was: In the analysis adjusted for the total sample (true acupuncture relative risk 5.04, 95% confidence interval 2.24-11.32; sham acupuncture relative risk 5.02, 95% confidence interval 2.26-11.16; placebo acupuncture relative risk 2.57 95% confidence interval 1.21-5.46), as well as for the subsample of occupationally active patients, all 3 modalities of acupuncture were better than conventional treatment alone, but there was no difference among the 3 acupuncture modalities, which implies that true acupuncture is not better than sham or placebo acupuncture. Thus this (multicentre) study was negative with just a touch of positivity.
But still, look at the range of conditions that respond positively to acupuncture in Vas’ hands. Is there anyone who doubts that Jorge Vas does not deserve to join all these other geniuses in THE ALTERNATIVE MEDICINE HALL OF FAME?
- Andreas Michalsen ( various SCAMs, Germany)
- Jennifer Jacobs (homeopath, US)
- Jenise Pellow (homeopath, South Africa)
- Adrian White (acupuncturist, UK)
- Michael Frass (homeopath, Austria)
- Jens Behnke (research officer, Germany)
- John Weeks (editor of JCAM, US)
- Deepak Chopra (entrepreneur, US)
- Cheryl Hawk (US chiropractor)
- David Peters (osteopathy, homeopathy, UK)
- Nicola Robinson (TCM, UK)
- Peter Fisher (homeopathy, UK)
- Simon Mills (herbal medicine, UK)
- Gustav Dobos (various SCAMs, Germany)
- Claudia Witt (homeopathy, Germany/Switzerland)
- George Lewith (acupuncture, UK)
- John Licciardone (osteopathy, US)
I am sure that Vas has more than merited to join them.
WELCOME JORGE VAS!
There are skeptics who keep claiming that there is no research in so-called alternative medicine (SCAM). And there are plenty of SCAM enthusiasts who claim that there is an abundance of good research in SCAM.
Who is right and who is wrong?
I submit that both camps are incorrect.
To demonstrate the volume of SCAM research I looked into Medline to find the number of papers published in 2020 for the SCAMs listed below:
- acupuncture 2 752
- anthroposophic medicine 29
- aromatherapy 173
- Ayurvedic medicine 183
- chiropractic 426
- dietary supplement 5 739
- essential oil 2 439
- herbal medicine 5 081
- homeopathy 154
- iridology 0
- Kampo medicine 132
- massage 824
- meditation 780
- mind-body therapies 968
- music therapy 539
- naturopathy 68
- osteopathic manipulation 71
- Pilates 97
- qigong 97
- reiki 133
- tai chi 397
- Traditional Chinese Medicine 15 277
- yoga 698
I think the list proves anyone wrong who claims there is no (or very little) research into SCAM.
As to the enthusiasts who claim that there is plenty of good evidence, I am afraid, I disagree with them too. The above-quoted numbers are perhaps impressive to some SCAM proponents, but they are not large. To make my point more clearly, let me show you the 2020 volumes for a few topics in conventional medicine:
- psychiatry 668,492
- biologicals 300,679
- chemotherapy 109,869
- radiotherapy 17,964
- rehabilitation 21,751
- rehabilitation medicine 21,751
- surgery 256,958
I think we can agree that these figures make the SCAM numbers look pitifully small.
But the more important point is, I think, not the quantity but the quality of the SCAM research. As this whole blog is about the often dismal rigor of SCAM research, I do surely not need to produce further evidence to convince you that it is poor, often even very poor.
So, both camps tend to be incorrect when they speak about SCAM research. The truth is that there is quite a lot, but sadly reliable studies are like gold dust.
But actually, when I started writing this post and doing all these Medline searches to produce the above-listed volumes of SCAM research, I was thinking of a different subject entirely. I wanted to see which areas of SCAM were research-active and which are not. This is why I chose terms for my list that do not overlap with others (yet we need to realize that the figures are not precise due to misclassification and other factors). And in this respect, the list is interesting too, I find.
It identifies the SCAMs that are remarkably research-inactive:
- anthroposophic medicine
- iridology
- naturopathy
- osteopathy
- Pilates
- qigong
Perhaps more interesting are the areas that show a relatively high research activity:
- acupuncture
- dietary supplements
- essential oils
- herbal medicine
- massage
- meditation
- mind-body therapies
- TCM
- yoga
This, in turn, suggests two things:
- It is not true that only commercial interests drive research activity.
- The Chinese (TCM and acupuncture) are pushing the ferociously hard to conquer SCAM research.
The last point is worrying, in my view, because we know from several independent studies that Chinese studies are often the flimsiest and least reliable of all the SCAM literature. As I have suggested recently, the unreliability of SCAM research might one day be its undoing: This self-destructive course of SCAM might be applauded by some skeptics. However, if you believe (as I do) that there are a few good things to be found in SCAM, this development can only be regrettable. I fear that the growing dominance of Chinese research will help to speed up this process.
Since Gwyneth Paltrow, as well as US Olympic swimmers, were publicly sporting their cupping marks, cupping has repeatedly occupied the pages of this blog. Now, cupping is in the news yet again. It has been reported that an image of a self-proclaimed ‘cupping’ expert performing treatment on a newborn baby has caused a major outcry. The photo shows a three-month-old baby’s skin on its back being sucked into a cup with the skin deformed and bright red.

The man, known as Mustafa, who refers to himself as an ‘expert’ at a ’cupping centre’ in the city of Istanbul, recently shared the images on social media where he was apparently treating the baby for ‘gas’. “We provide cupping for everyone from three-month-old babies to 70-year-olds. We do it since it is an Islamic tradition and we believe that everyone should take part in it,“ Mustafa said. “I am not a swindler. I do not demand money from people. They give as much as they choose.”
Child and adolescent psychiatrist associate, Dr Veysi Ceri, slammed the parents who allowed the procedure to be performed on their children. “Children cannot be left at the mercy of their parents,” Dr Ceri said. “Cupping is something that is not based on scientific evidence and children are physically harmed from it.”
On social media, people expressed their fury, labelling the practice as “questionable”. One commenter wrote: “Are these people crazy? They don’t read or learn anything.” But there were also those who shared their positive experiences. “I congratulate the family who had cupping performed on their baby,” one person wrote. “I also do cupping regularly and I haven’t had a headache in years. I do not take any medicine either. It is also beneficial for children to have cupping.“
___________________________
So, is there any reliable evidence about dry cupping for children?
Is it demonstrably effective for any paediatric condition?
Is it harmful?
Believe it or not, there has been at least one clinical trial of dry cupping as a treatment of constipation in children:
One hundred and twenty children (4-18 years old) diagnosed as functional constipation according to ROME III criteria were assigned to receive a traditional dry cupping protocol on the abdominal wall for 8 minutes every other day or standard laxative therapy (Polyethylene glycol (PEG) 40% solution without electrolyte), 0.4 g/kg once daily) for 4 weeks, in an open label randomized controlled clinical trial using a parallel design with a 1:1 allocation ratio. Patients were evaluated prior to and following 2, 4, 8 and 12 weeks of the intervention commencement in terms of the ROME III criteria for functional constipation.
Results: There were no significant differences between the two arms regarding demographic and clinical basic characteristics. After two weeks of the intervention, there was a significant better result in most of the items of ROME III criteria of patients in PEG group. In contrast, after four weeks of the intervention, the result was significantly better in the cupping group. There was no significant difference in the number of patients with constipation after 4 and 8 weeks of the follow-up period.
Conclusion: This study showed that dry cupping of the abdominal wall, as a traditional manipulative therapy, can be as effective as standard laxative therapy in children with functional constipation.
This study is squarely negative, yet the conclusions are clearly positive. I have stopped being amazed by such contradictions. After all, we are dealing with so-called alternative medicine (SCAM)!
For what it’s worth, here is our 2011 overview of all systematic reviews of cupping:
Several systematic reviews (SRs) have assessed the effectiveness of cupping for a range of conditions. Our aim was to provide a critical evaluation and summary of these data. Electronic searches were conducted to locate all SRs concerning cupping for any condition. Data were extracted by two authors according to predefined criteria. Five SRs met our inclusion criteria, which related to the following conditions: pain conditions, stroke rehabilitation, hypertension, and herpes zoster. The numbers of studies included in each SR were small. Relatively clear evidence emerged only for one indication, that cupping may be effective for reducing pain. Based on evidence from the currently available SRs, the effectiveness of cupping has been demonstrated only as a treatment for pain, and even for this indication doubts remain.
And here is our 2011 SR of cupping as a treatment of pain:
The objective of this study was to assess the evidence for or against the effectiveness of cupping as a treatment option for pain. Fourteen databases were searched. Randomized clinical trials (RCTs) testing cupping in patients with pain of any origin were considered. Trials using cupping with or without drawing blood were included, while trials comparing cupping with other treatments of unproven efficacy were excluded. Trials with cupping as concomitant treatment together with other treatments of unproven efficacy were excluded. Trials were also excluded if pain was not a central symptom of the condition. The selection of studies, data extraction and validation were performed independently by three reviewers. Seven RCTs met all the inclusion criteria. Two RCTs suggested significant pain reduction for cupping in low back pain compared with usual care (P < .01) and analgesia (P < .001). Another two RCTs also showed positive effects of cupping in cancer pain (P < .05) and trigeminal neuralgia (P < .01) compared with anticancer drugs and analgesics, respectively. Two RCTs reported favorable effects of cupping on pain in brachialgia compared with usual care (P = .03) or heat pad (P < .001). The other RCT failed to show superior effects of cupping on pain in herpes zoster compared with anti-viral medication (P = .065). Currently there are few RCTs testing the effectiveness of cupping in the management of pain. Most of the existing trials are of poor quality. Therefore, more rigorous studies are required before the effectiveness of cupping for the treatment of pain can be determined.
The included trials frequently were silent about adverse effects. Others reported no adverse effects and one mentioned three cases of vaso-vagal shock. None of the studies was on children.
So, here are my answers to the questions above:
- Is there any reliable evidence about dry cupping for children? No
- Is it demonstrably effective for any paediatric condition? No
- Is it harmful? Probably not that much (other than undermining common sense and rationality).
Yes, I have just published a new book! Its title is ‘Alternativmedizin – was hilft, was schadet: Die 20 besten, die 20 bedenklichsten Methoden’ (Alternative medicine – treatments that help and treatments that harm: The 20 best and the 20 most worrying methods). Yes, it is in German, and somehow I doubt that there will be an English version of it. Therefore I take the liberty of translating a short section for those who do not read German. 
But first, let me tell you about the book’s concept.
Some people who read this blog seem to have the impression that I am dead against so-called alternative medicine (SCAM) – my friend Dana Ullman, for instance, is convinced of it. This, however, is not quite correct (Dana rarely is). The truth is that I am
- FOR evidence-based medicine,
- FOR a level playing field in all areas of healthcare,
- FOR critically evaluating all options.
This also means, of course, that I am against misleading consumers about the value of SCAM. And therefore I am FOR any SCAM that demonstrably does more good than harm.
This attitude should have been clear from all my books. However, it seems to be difficult to understand for those who are on the more fanatical end of the SCAM spectrum. And because it is not that obvious, I decided to write a book that analyses (understandably yet analytically [including ~300 references of the original science]) the evidence for 20 SCAMs that are supported by reasonably sound evidence together with 20 for which this is not the case. My hope is that, with this approach, I might reach more consumers who are in favour of SCAM.
There is a risk, of course. Chances are that, instead of reaching more people from the pro-camp, I will merely offend both the sceptics as well as the enthusiasts.
We shall see.
Anyway, here is the promised bit that I translated for you. It is the postscript of the book, and I hope it gives you a flavour of what it is all about. Here we go:
In the first chapter of the book, I promised that I would neither uncritically hype alternative medicine nor unfairly condemn it. I have taken great pains to keep this promise.
Have I succeeded?
I fear there will be many who answer this question in the negative. And I can’t even blame my critics! Who likes to be criticized for something in which he deeply believes? Who likes to hear that his prejudices against everything called alternative medicine are wrong and counter-productive? Who doesn’t mind an ugly fact that destroys his beautiful theory? Both the dogmatic naysayers and the naive believers will be dissatisfied with my book (or at least parts of).
That’s a shame, but ultimately it is irrelevant. My point was not to take the word of one camp or another in the endless trench warfare that is alternative medicine. My main concern was to present the evidence as up-to-date, understandable, and objective as possible, and to serve those who are seriously interested in facts.
The book is thus not for dogged trench warriors; rather, it is aimed at ordinary consumers with an interest in their health. After all, the vast majority of the population is not among the unteachables of one camp or the other. Most people don’t want ideology, they want effective medicine. And most of them are baffled by the unmanageable variety of alternative medicine on offer, the grandiose promises of healing, and the vehement emotions that it all triggers.
In the area of alternative medicine, there is undoubtedly a lot of nonsense, charlatanry, and danger. But there are also some things that demonstrably do more good than harm. In order to separate the wheat from the chaff, consumers don’t need creeds. What they need above all is reliable evidence!
You can read about this evidence in my book. How you then deal with it is solely your decision. I do not want to tell anyone what to do with my presentation of the facts. But I know that the abundance of misinformation in the field of alternative medicine causes great damage and that the consumer and reader of my book, deserve better than to be led up the garden path.
If this book helps readers to make wise treatment decisions, my efforts will have been worthwhile. And if they get half as much pleasure from reading it as I did from writing it, my goal has been achieved.
THE END
(If by any chance you do read German and are in the position to publish a book review, please let me know and I will see that you get a free review copy of my book)
The objective of this review (entitled ‘Systematic Review on the Use of Homeopathy in Dentistry:
Critical Analysis of Clinical Trials‘) was to map the literature on homeopathy in dentistry and to evaluate the effectiveness of using homeopathy in dental practice through the critical analysis of clinical studies.
The search for scientific articles in any language, year, and place of publication was made in the databases of Public Medline (PUBMED), Web of Science, Cochrane, and Virtual Health Library; the articles selected were later classified according to the type of study. Gray literature was accessed through Google Scholar. Clinical trials were analyzed for methodological quality. Two trained reviewers accomplished the entire process independently.
Of the 281 studies retrieved by means of the search, 44 met the eligibility criteria. The included papers were:
- literature reviews (56.8%),
- clinical trials (34.1%),
- cross-sectional studies (6.8%),
- laboratory research (6.8%),
- longitudinal observational studies (4.5%).
The clinical trials were published from 1965 to 2019, using homeopathy in several dental specialties:
- Endodontics,
- Periodontics,
- Orofacial Pain,
- Surgery,
- Pediatric Dentistry,
- Stomatology,
- dental anxiety.
Qualitative failures, in all criteria investigated, and positive influences of the individual prescriptions on the results of treatments reported were observed.
The authors concluded that there is still a scarcity of studies about homeopathy and dentistry. The clinical trials selected showed positive effects on oral health; however, when they were critically evaluated, it was possible to recognize qualitative failures, mainly relative to double-blinding. It is necessary to encourage research on the subject, using standardized methodological procedures, to obtain better evaluation of the clinical applicability.
According to the authors, their review adhered to the PRISMA guideline of systematic reviews. This is, however, not the case. The authors correctly point out that the primary studies had many flaws: methodological failures were observed in the clinical trials, mainly related to double-blinding (66.7%). Significant failures were also observed in similarity (61.1%), randomization (27.8%), description of losses and exclusions (27.8%), and exclusion criteria (27.8%). They do not seem to realize that flaws of this nature and frequency should prevent positive conclusions.
So, what does this paper actually demonstrate? In my view, it shows that:
- the peer-review process at the JACM continues to be a joke;
- poor quality trials run by enthusiasts tend to produce false-positive results;
- in so-called alternative medicine (SCAM), people get away with publishing even the most obvious falsehoods.
Tuina is a massage therapy that originates from Traditional Chinese Medicine. Many of the techniques used in tuina resemble those of a western massage like gliding, kneading, vibration, tapping, friction, pulling, rolling, pressing, and shaking. Tuina involves a range of manipulations usually performed by the therapist’s finger, hand, elbow, knee, or foot. They are applied to muscle or soft tissue at specific locations of the body.
The aim of Tuina is to enhance the flow of the ‘vital energy’ or ‘chi’, that is alleged to control our health. Proponents of the therapy recommend Tuina for a range of conditions, including paediatric ones. Paediatric Tuina has been widely used in children with acute diarrhea in China. However, due to a lack of high-quality clinical evidence, the benefit of Tuina is not clear.
This study aimed to assess the effect of paediatric Tuina compared with sham Tuina as add-on therapy in addition to usual care for 0-6-year-old children with acute diarrhea.
Eighty-six participants aged 0-6 years with acute diarrhea were randomized to receive Tuina plus usual care (n = 43) or sham Tuina plus usual care (n = 43). The primary outcomes were days of diarrhea from baseline and times of diarrhea on day 3. Secondary outcomes included a global change rating (GCR) and the number of days when the stool characteristics returned to normal. Adverse events were assessed.
Tuina treatment in the intervention group was performed on the surface of the children’s body using moderate pressure (Fig. 1a). Tuina treatment in the control group was different: the therapist used one hand to hold the child’s hand or put one hand on the child’s body, while the other hand performed manipulations on the therapist’s own hand instead of the child’s hand or body (Fig. (Fig.11b).

Tuina was associated with a reduction in times of diarrhea on day 3 compared with sham Tuina in both ITT and per-protocol analyses. However, the results were not significant when adjusted for social-demographic and clinical characteristics. No significant difference was found between groups in days of diarrhea, global change rating, or number of days when the stool characteristics returned to normal.
The authors concluded that in children aged 0-6 years with acute diarrhea, pediatric Tuina showed significant effects in terms of reducing times of diarrhea compared with sham Tuina. Studies with larger sample sizes and adjusted trial designs are warranted to further evaluate the effect of pediatric Tuina therapy.
This study was well-reported and has interesting features, such as the attempt to use a placebo control and blinding (whether blinding was successful is a different matter and was not tested in the trial). It is, therefore, all the more surprising that the essentially negative result is turned into a positive one. After adjustment, the differences disappear (a fact which the authors hardly mention in the paper), which means they are not due to the treatment but to group differences and confounding. This, in turn, means that the study shows not the effectiveness but the ineffectiveness of Tuina.
The purpose of this survey (the authors call it a ‘study’) was to evaluate the patient-perceived benefit of yoga for symptoms commonly experienced by breast cancer survivors.
A total of 1,049 breast cancer survivors who had self-reported use of yoga on a follow-up survey, in an ongoing prospective Mayo Clinic Breast Disease Registry (MCBDR), received an additional mailed yoga-focused survey asking about the impact of yoga on a variety of symptoms. Differences between pre-and post- scores were assessed using Wilcoxon Signed Rank Test.
802/1,049 (76%) of women who were approached to participate, consented and returned the survey. 507/802 (63%) reported use of yoga during and/or after their cancer diagnosis. The vast majority of respondents (89.4%) reported some symptomatic benefit from yoga. The most common symptoms that prompted the use of yoga were breast/chest wall pain, lymphedema, and anxiety. Only 9% of patients reported that they had been referred to yoga by a medical professional. While the greatest symptom improvement was reported with breast/chest wall pain and anxiety, significant improvement was also perceived in joint pain, muscle pain, fatigue, headache, quality of life, hot flashes, nausea/vomiting, depression, insomnia, lymphedema, and peripheral neuropathy, (all p-values <0.004).
The authors concluded that data supporting the use of yoga for symptom management after cancer are limited and typically focus on mental health. In this study, users of yoga often reported physical benefits as well as mental health benefits. Further prospective studies investigating the efficacy of yoga in survivorship are warranted.
I have little doubt that yoga is helpful during palliative and supportive cancer care (but all the more doubts that this new paper will further the reputation of research in this area). In fact, contrary to what the conclusions state, there is quite good evidence for this assumption:
- A 2009 systematic review included 10 clinical trials. Its authors concluded that although some positive results were noted, variability across studies and methodological drawbacks limit the extent to which yoga can be deemed effective for managing cancer-related symptoms.
- A 2017 systematic review with 25 clinical trials concluded that among adults undergoing cancer treatment, evidence supports recommending yoga for improving psychological outcomes, with potential for also improving physical symptoms. Evidence is insufficient to evaluate the efficacy of yoga in pediatric oncology.
- A 2017 Cochrane review included 24 studies and found that moderate-quality evidence supports the recommendation of yoga as a supportive intervention for improving health-related quality of life and reducing fatigue and sleep disturbances when compared with no therapy, as well as for reducing depression, anxiety and fatigue, when compared with psychosocial/educational interventions. Very low-quality evidence suggests that yoga might be as effective as other exercise interventions and might be used as an alternative to other exercise programmes.[3]
So, why publish a paper like the one above?
Search me!
To be able to add one more publication to the authors’ lists?
And why would the journal editor go along with this nonsense?
Search me again!
No, hold on: Global Advances in Health and Medicine, the journal that carried the survey, is published in association with Academic Consortium for Integrative Medicine & Health.
Yes, that explains a lot.
As I have pointed out several times before, surveys of this nature are like going into a Mac Donald’s and asking the customers whether they like Hamburgers. You might then also find that “the vast majority of respondents (89.4%) reported”… blah, blah, blah.
The title of the paper is ‘Real-World Experiences With Yoga on Cancer-Related Symptoms in Women With Breast Cancer‘.
PS
NOTE TO MYSELF: never touch a paper with ‘real-world experience’ in the title.
Yesterday, someone posted a disparaging comment about Indian research into homeopathy; he claimed that it was unreliable. I agreed, but later I thought ‘HOW ARROGANT OF ME!’. So, I decided to do a little research – actually, it turned out to be a little more than just ‘a little’.
I searched Medline for ‘homeopathy, study, India’. This resulted in 101 hits. Of these 101 articles, 31 contained data published by Indian authors providing evidence at least vaguely related to the effectiveness of homeopathy. I decided to include these in my analysis. Below I quote first the title of each paper followed by (in brackets) the sentence from the 31 abstracts that best describes the direction of the results.
- Multimorbidity After Surgical Menopause Treated with Individualized Classical Homeopathy: A Case Report (She was treated with individualized classical homeopathy and followed up for 31 months. She was relieved of the vasomotor symptoms and psychological disturbances of climacteric syndrome, her weight reduced, the ultrasound scan showed absence of lipomatosis/gall bladder disease/hepatic steatosis. Blood tests showed reduction of thyroid stimulating hormone and a balance in the lipid status. Individualized classical homeopathy may have a role in the climacteric syndrome and comorbidities after surgical menopause.)
- Therapeutic evaluation of homeopathic treatment for canine oral papillomatosis (The current study proves that the combination of homeopathy drugs aids in fastening the regression of canine oral papilloma and proved to be safe and cost-effective.)
- Deep vein thrombosis cured by homeopathy: A case report (The present case report intends to record yet another case of DVT in an old patient totally cured exclusively by the non-invasive method of treatment with micro doses of potentized homeopathic drugs selected on the basis of the totality of symptoms and individualization of the case.)
- Diabetic retinopathy screening uptake after health education with or without retinal imaging within the facility in two AYUSH hospitals in Hyderabad, India: A nonrandomized pilot study (AYUSH hospitals could provide a feasible and acceptable location for providing DR screening services.)
- Individualised Homeopathic Therapy in ANCA Negative Rapidly Progressive Necrotising Crescentic Glomerulonephritis with Severe Renal Insufficiency – A Case Report (A 60-year-old Indian woman was treated with classical homeopathy for ANCA-negative RPGN, and after one year of treatment, serum creatinine and other parameters indicating renal injury dropped steadily despite the withdrawal of immunosuppressive drugs; renal dialysis, which was conducted twice a week initially, was made rarer and stopped after one year. Classical homeopathy may be considered a potential therapeutic modality in severe pathologies.)
- Improvements in long standing cardiac pathologies by individualized homeopathic remedies: A case series (… individualized homeopathic therapy was instituted along with the conventional medicines and the results were encouraging. The changes in the laboratory diagnostic parameters (single-photon emission computed tomography, electrocardiograph, echocardiography and ejection fraction as the case may be) are demonstrated over time. The key result seen in all three cases was the preservation of general well-being while the haemodynamic states also improved.)
- Could Homeopathy Become An Alternative Therapy In Dengue Fever? An example Of 10 Case Studies (We present a retrospective case series of 10 Indian patients who were diagnosed with dengue fever and treated exclusively with homeopathic remedies at Bangalore, India. This case series demonstrates with evidence of laboratory reports that even when the platelets dropped considerably there was good result without resorting to any other means.)
- Homeopathic Treatment of Vitiligo: A Report of Fourteen Cases (In 14 patients with vitiligo treated with individualized homeopathy, the best results were achieved in the patients who were treated in the early stages of the disease. We believe that homeopathy may be effective in the early stages of vitiligo, but large controlled clinical studies are needed in this area.)
- An Exploratory Study of Autonomic Function Investigations in Hemophiliacs on Homoeopathy Medications Using Impedance Plethysmography (Homoeopathic medicines used as an adjunct was associated with decrease in parasympathetic modulations.)
- Embryonic Zebrafish Model – A Well-Established Method for Rapidly Assessing the Toxicity of Homeopathic Drugs: – Toxicity Evaluation of Homeopathic Drugs Using Zebrafish Embryo Model (Our findings clearly demonstrate that no toxic effects were observed for these three homeopathic drugs at the potencies and exposure times used in this study. The embryonic zebrafish model is recommended as a well-established method for rapidly assessing the toxicity of homeopathic drugs.)
- Treatment of hemorrhoids with individualized homeopathy: An open observational pilot study (Under classical homeopathic treatment, hemorrhoids patients improved considerably in symptoms severity and anoscopic scores. However, being observational trial, our study cannot provide efficacy data. Controlled studies are required.)
- Patients’ preference for integrating homeopathy (PPIH) within the standard therapy settings in West Bengal, India: The part 1 (PPIH-1) study (A favorable attitude toward integrating homeopathy into conventional healthcare settings was obtained among the patients attending the homeopathic hospitals in West Bengal, India.)
- Patients’ Preference for Integrating Homoeopathy Services within the Secondary Health Care Settings in India: The Part 3 (PPIH-3) Study (A total of 82.40% (95% confidence interval = 79.23, 85.19) of the participants were in favor of integrating homoeopathy services.)
- Obstetrics and gynecology outpatient scenario of an Indian homeopathic hospital: A prospective, research-targeted study (The most frequently treated conditions were leucorrhea (20.5%), irregular menses (13.3%), dysmenorrhea (10%), menorrhagia (7.5%), and hypomenorrhea (6.3%). Strongly positive outcomes (+3/+2) were mostly recorded in oligomenorrhea (41.7%), leucorrhea (34.1%), polycystic ovary (33.3%), dysmenorrhea (28%), and irregular menses (22.2%). Individualized prescriptions predominated (95.6%).)
- Relative Apoptosis-inducing Potential of Homeopa-thic Condurango 6C and 30C in H460 Lung Cancer Cells In vitro: -Apoptosis-induction by homeopathic Condurango in H460 cells (Condurango 30C had greater apoptotic effect than Condurango 6C as claimed in the homeopathic doctrine.)
- Beliefs, attitudes and self-use of Ayurveda, Yoga and Naturopathy, Unani, Siddha, and Homeopathy medicines among senior pharmacy students: An exploratory insight from Andhra Pradesh, India (Pharmacy students held favorable attitude and beliefs about AYUSH use.)
- Integrative nanomedicine: treating cancer with nanoscale natural products (Taken together, the nanoparticulate research data and the Banerji Protocols for homeopathic remedies in cancer suggest a way forward for generating advances in cancer treatment with natural product-derived nanomedicines.)
- Evidence of an Epigenetic Modification in Cell-cycle Arrest Caused by the Use of Ultra-highly-diluted Gonolobus Condurango Extract (Condurango 30C appeared to trigger key epigenetic events of gene modulation in effectively combating cancer cells, which the placebo was unable to do.)
- Calcarea carbonica induces apoptosis in cancer cells in p53-dependent manner via an immuno-modulatory circuit (Our results indicated a “two-step” mechanism of the induction of apoptosis in tumor cells by calcarea carbonica)
- Post-cancer Treatment with Condurango 30C Shows Amelioration of Benzo[a]pyrene-induced Lung Cancer in Rats Through the Molecular Pathway of Caspa- se-3-mediated Apoptosis Induction: -Anti-lung cancer potential of Condurango 30C in rats (The overall result validated a positive effect of Condurango 30C in ameliorating lung cancer through caspase-3-mediated apoptosis induction and EGFR down-regulation.)
- The potentized homeopathic drug, Lycopodium clavatum (5C and 15C) has anti-cancer effect on hela cells in vitro (Thus, the highly-diluted, dynamized homeopathic remedies LC-5C and LC-15C demonstrated their capabilities to induce apoptosis in cancer cells, signifying their possible use as supportive medicines in cancer therapy.)
- Ameliorating effect of mother tincture of Syzygium jambolanum on carbohydrate and lipid metabolic disorders in streptozotocin-induced diabetic rat: Homeopathic remedy (The result of the present study indicated that the homeopathic drug S jambolanum (mother tincture) has a protective effect on diabetic induced carbohydrate and lipid metabolic disorders in STZ-induced diabetic animal.)
- SEM studies on blood cells of Plasmodium berghei infected Balb/c mice treated with artesunate and homeopathic medicine China (The combination of artesunate and China was found to be very effective and did not cause any alteration on the surface of blood cells as observed in SEM.)
- Induction of apoptosis of tumor cells by some potentiated homeopathic drugs: implications on mechanism of action (These data indicate that apoptosis is one of the mechanisms of tumor reduction of homeopathic drugs.)
- TDZ-induced high frequency shoot regeneration in Cassia sophera Linn. via cotyledonary node explants (Regenerated plantlets were successfully acclimatized and hardened off inside the culture room and then transferred to green house with 100 % survival rate.)
- Modulation of Signal Proteins: A Plausible Mechanism to Explain How a Potentized Drug Secale Cor 30C Diluted beyond Avogadro’s Limit Combats Skin Papilloma in Mice (We tested the hypothesis if suitable modulations of signal proteins could be one of the possible pathways of action of a highly diluted homeopathic drug, Secale cornutum 30C (diluted 10(60) times; Sec cor 30). It could successfully combat DMBA + croton oil-induced skin papilloma in mice as evidenced by histological, cytogenetical, immunofluorescence, ELISA and immunoblot findings.)
- Can homeopathy bring additional benefits to thalassemic patients on hydroxyurea therapy? Encouraging results of a preliminary study (The homeopathic remedies being inexpensive and without any known side-effects seem to have great potentials in bringing additional benefits to thalassemic patients; particularly in the developing world where blood transfusions suffer from inadequate screening and fall short of the stringent safety standards followed in the developed countries.)
- Effect of homeopathic medicines on transplanted tumors in mice (These findings support that homeopathic preparations of Ruta and Hydrastis have significant antitumour activity. The mechanism of action of these medicines is not known at present.)
- Inhibition of chemically induced carcinogenesis by drugs used in homeopathic medicine (These studies demonstrate that homeopathic drugs, at ultra low doses, may be able to decrease tumor induction by carcinogen administration.)
- Can homeopathic treatment slow prostate cancer growth? (The findings indicate that selected homeopathic remedies for the present study have no direct cellular anticancer effects but appear to significantly slow the progression of cancer and reduce cancer incidence and mortality in Copenhagen rats injected with MAT-LyLu prostate cancer cells.)
- Ameliorating effect of microdoses of a potentized homeopathic drug, Arsenicum Album, on arsenic-induced toxicity in mice (The results lend further support to our earlier views that microdoses of potentized Arsenicum Album are capable of combating arsenic intoxication in mice, and thus are strong candidates for possible use in human subjects in arsenic contaminated areas under medical supervision.)
So, 31 of 31 yield positive results and conclusions – 100%!
When I suggested that Indian research into homeopathy is suspect, I was merely speculating on the basis of reading such papers for many years. I had not seen a systematic analysis to justify my harsh judgment; in fact, I don’t think that such a review is currently available (which would make this post the first of its kind). I had no idea how true my seemingly disrespectful remark would turn out to be. There is not one paper from India that does not suggest positive findings for homeopathy. I find this truly remarkable!
You can, of course, interpret my findings in two very different ways:
- Either you assume that homeopathy is hugely effective and works always and for everything under every experimental condition.
- Or you conclude that Indian research into homeopathy is suspect and far from trustworthy.
If you believe the first option to be true, I fear that you must be as deluded as homeopathic remedies are diluted.
The aim of the paper (published in ‘HOMEOPATHY’) was to perform a systematic review of basic research of homeopathic high dilutions in cancer.
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline, we conducted a literature search in the database PubMed for original publications, from 2000 to 2018 and in English, on in vitro and in vivo experimental cancer models testing homeopathic high dilutions.
Twenty-three articles met the inclusion criteria-14 in vitro, eight in vivo, and one in vitro plus in vivo experimental models. Most studies were from India. Research prominently focused on cytotoxic effects involving apoptotic mechanisms. Intrinsic aspects of homeopathy should be considered in experimental designs to emphasize the specificity of such effects.
The authors concluded that fundamental research of homeopathy in cancer is still at an early stage and has mainly been performed by a few groups of investigators. The results point to an interference of well-selected homeopathic medicines with cell cycle and apoptotic mechanisms in cancer cells. However, these findings still need independent reproduction.
I happen to be a co-author of the PRISMA guideline and can assure you that this systematic review is very far from adhering to it. It borders on fraud to state otherwise; at the very minimum, the authors, the editor of ‘HOMEOPATHY‘, as well as the reviewers of this article are guilty of seriously misleading the public. Any reputable journal would have insisted that the abstract of this paper makes the following points very clear so that misunderstandings are avoided:
- There is no valid hypothesis to suggest that homeopathic high dilutions affect cancer.
- The included studies are mostly of poor or very poor quality.
- The results of such pre-clinical in vitro and in vivo experiments have little bearing on the treatment of human cancers.
- The fact that independent replications are missing suggests that these studies are irreproducible.
- The fact that most studies originate from the same research groups implies that homeopathy is not considered to be a viable avenue by rational thinkers.
- In the interest of cancer patients, the idea that homeopathy might be of any use in cancer needs to be discouraged.
In one of my last posts, I stated that research into so-called alternative medicine (SCAM) is fast becoming the laughing stock of serious scientists. This paper is an excellent example of this phenomenon.
The objective of this survey was to determine
- which patients’ characteristics are associated with the use of so-called alternative medicine (SCAM) during cancer treatment,
- their pattern of use,
- and if it has any association with its safety profile.
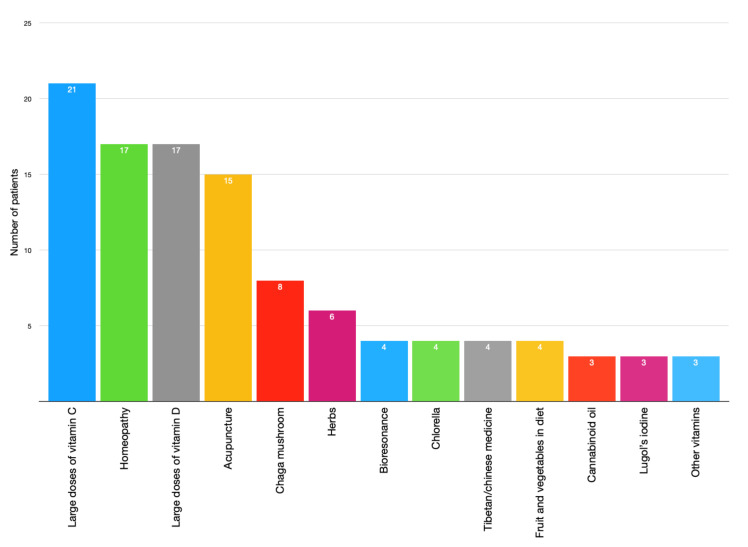
A total of 316 patients undergoing chemotherapy treatment in cancer centers in Poland between 2017 and 2019 were asked about their use of SCAM.
Patients’ opinion regarding the safety of unconventional methods is related to the use of SCAM. Moreover, patients’ thinking that SCAM can replace conventional therapy was correlated with his/her education. Moreover, the researchers performed analyses to determine factors associated with SCAM use including sociodemographic and clinical characteristics.
Crucially, they also conducted a survival analysis of patients undergoing chemotherapy with 42 months of follow-up. Using Kaplan-Meier curves and log-rank analysis, they found no statistical difference in overall survival between the groups that used and did not use any form of SCAM.

The authors concluded that SCAM use is common among patients undergoing chemotherapy treatment and should be considered by medical teams as some agents may interact with chemotherapy drugs and affect their efficacy or cause adverse effects.
As I have stated before, I find most surveys of SCAM use meaningless. This article is no exception – except for the survival analysis. It would have merited a separate, more detailed paper, yet the authors hardly comment on it. The analysis shows that SCAM users do not live longer than non-users. Previously, we have discussed several studies that suggested they live less long than non-users.
While this aspect of the new study is interesting, it proves very little. There are, of course, multiple factors involved in the survival of cancer patients, and even if SCAM use were a determinant, it is surely less important than many other factors. To get a better impression of the role SCAM plays, we need studies that carefully match patients according to the most obvious prognostic variables (RCTs would be problematic, difficult to do and unethical). Such studies do exist and they too fail to show that SCAM use prolongs survival, some even suggest it might shorten survival.