case report
Guest post by Ken McLeod
On 31 March 2020, the Chiropractic Board of Australia issued a statement1 to all Australian chiropractors that they:
“should not make advertising claims on preventing or protecting patients and health consumers from contracting COVID-19 or accelerating recovery from COVID-19. To do so involves risk to public safety and may be unlawful advertising. For example, we are seeing some advertising claims that spinal adjustment/manipulation, acupuncture and some products confer or boost immunity or enhance recovery from COVID-19 when there is no acceptable evidence in support.
“Advertisers must be able to provide acceptable evidence of any claims made about treatments that benefit patients/health consumers. We will consider taking action against anyone found to be making false or misleading claims about COVID-19 in advertising. If the advertiser is a registered health practitioner, breaching advertising obligations is also a professional conduct matter which may result in disciplinary action, especially where advertising is clearly false, misleading or exploitative.”
What could be clearer than that?
So what was published by a registered chiropractor on 16 March 2020, two weeks before the Board’s warning, and is still on his website 10 months later? You guessed it, a video on the website of chiropractor Morgan Weber, a video ‘Coronavirus – Balancing the hysteria…’, 2 in which he says:
– the COVID-19 19 pandemic is all ‘hysteria’ and ‘what have we got to worry about’, because ‘Our body, (has) 51 trillion cells’ vs ‘A one single-cell virus,’ (sic.) ‘51 trillion cells that orchestrate our immune system, every function. Yet we seem to have more faith and trust in ‘medicine’ than we do in this amazing body we call home. Crazy, right? Crazy.’
Weber further downplays the crisis by saying ‘Enough of this nonsense about the big bad bug and all the worry about washing your hands.’
Weber, after denigrating evidence-based medicine, recommends instead:
– ‘Keep up with your chiropractic adjustments….’
Weber is a registered chiropractor practicing at Wave Chiropractic, Maroochydore, Queensland, Australia. His AHPRA registration is CHI0001601286. Weber’s webpage home site is at https://www.wavechiropractic.com.au/index.php
WEBER’S VIDEO:
Since 16 March 2020 Weber has posted a video on his website a video ‘Coronavirus – Balancing the hysteria…’. 3
Weber says:
BEGINS TRANSCRIPT
00:00. Hi everyone. Hasn’t it been fascinating lately? The news, the hysteria. Everything has gone almost upside-down. Crazy. I found it so fascinating.
00:12. So today we thought we would have a bit of a chat and sort of balance the scales and the story getting told out there in the mass media. I hope you’ve got your toilet paper stockpiled and sorted ha ha ha ha. It’s hilarious to see people coming and going with huge amounts under their arms as they come out of the grocery store. Crazy isn’t it, crazy times.
00:42. So let’s think about if for a second, and if we bypass all that hysteria and noise and just think a little bit about this. Our body, 51 trillion cells. A one single-cell virus. My gosh. What have we got to worry about? We have this amazing system. 51 trillion cells that orchestrate our immune system, every function. Yet we seem to have more faith and trust in ‘medicine’ than we do in this amazing body we call home. Crazy, right? Crazy.
01:20 ‘The other story, the other sort of facts behind what we do, and I (unintelligible) told a fair few of you of this already, how the immune system works. So, across the road from Waves, we have a really kind of bare patch of grass, just before you go onto the beach. Now if I took a handful of seeds. Now this is an analogy for how our system works, and how amazing our body’s immune system is. If I took a bunch of seeds and dropped them onto the ground, some grass seeds, not all of those seeds would take. There needs to be a hospitable environment, a moist warm sunlit area for those seeds to take, then root and grow into a fully mature grass and perpetuate on and on and on. However that area across the road is barren rocky sandy and yuck. You drop those seeds, most of those are going to blow off and away because that area is a no-go, it’s got a strong resistance, a barrier, a non-hospitable environment.
02:18. Now that is how our immune system works. Now the story I feel that should be out there, is what are you doing to nurture your body to do the best it can be, to have the strongest barrier it can be.
02: 30. Enough of this nonsense about the big bad bug and all the worry about washing your hands. ‘Cause I tell you what, if you are neglecting to nurture your body and the 51 trillion cells to be the best they can be, watch out, that may not be enough, washing your hands.
02:47. So let’s talk about that. How do we orchestrate a healthy system that has a strong immune barrier to anything that’s out there? And really guys, this should be a day-to-day forte (?) for everyone who just wants to be their best.
03:00. So let’s go through it. Boosting your barriers. You need to trust your body. First and foremost, the 51 trillion cells are remarkable. Trust in that.
03: 12. You’ve gotta eat well. Eat well with nutrient-dense, mineral-dense foods. Stay well hydrated. Move. You’ve gotta move well. Exercise your body regularly, moving all parts in all directions. Enjoy healthy sunlight exposure. You’ve gotta think well. Follow your passions and purpose. Think positively. Perhaps switch off the TV.
03:41. Keep up with your chiropractic adjustments. An optimal brain and body communication via the nervous system is vital so ensuring your body is in a surviving state. Do all these things guys. Up the ante of them. Go in harder with your (unintelligible) exercises, your hydration etcetera, and trust in your body. It’s amazing. It’s built with this in-built protective mechanism. Foster it. Help to balance that story out there, and help people to take on a more useful interpretation of this current crisis out there.
04:19. I hope this was of value and you guys enjoy.
END TRANSCRIPT
The regulator has been informed. As the world’s death toll rockets past 2 million, we wait to see if they really meant what they said about disciplinary action.
I was criticised for not referencing this article in a recent post on adverse effects of spinal manipulation. In fact the commentator wrote: Shame on you Prof. Ernst. You get an “E” for effort and I hope you can do better next time. The paper was published in a third-class journal, but I will nevertheless quote the ‘key messages’ from this paper, because they are in many ways remarkable.
- Adverse events from manual therapy are few, mild, and transient. Common AEs include local tenderness, tiredness, and headache. Other moderate and severe adverse events (AEs) are rare, while serious AEs are very rare.
- Serious AEs can include spinal cord injuries with severe neurological consequences and cervical artery dissection (CAD), but the rarity of such events makes the provision of epidemiological evidence challenging.
- Sports-related practice is often time sensitive; thus, the manual therapist needs to be aware of common and rare AEs specifically associated with spinal manipulative therapy (SMT) to fully evaluate the risk-benefit ratio.
The author of this paper is Aleksander Chaibi, PT, DC, PhD who holds several positions in the Norwegian Chiropractors’ Association, and currently holds a position as an expert advisor in the field of biomedical brain research for the Brain Foundation of the Netherlands. I feel that he might benefit from reading some more critical texts on the subject. In fact, I recommend my own 2020 book. Here are a few passages dealing with the safety of SMT:
Relatively minor AEs after SMT are extremely common. Our own systematic review of 2002 found that they occur in approximately half of all patients receiving SMT. A more recent study of 771 Finish patients having chiropractic SMT showed an even higher rate; AEs were reported in 81% of women and 66% of men, and a total of 178 AEs were rated as moderate to severe. Two further studies reported that such AEs occur in 61% and 30% of patients. Local or radiating pain, headache, and tiredness are the most frequent adverse effects…
A 2017 systematic review identified the characteristics of AEs occurring after cervical spinal manipulation or cervical mobilization. A total of 227 cases were found; 66% of them had been treated by chiropractors. Manipulation was reported in 95% of the cases, and neck pain was the most frequent indication for the treatment. Cervical arterial dissection (CAD) was reported in 57%, and 46% had immediate onset symptoms. The authors of this review concluded that there seems to be under-reporting of cases. Further research should focus on a more uniform and complete registration of AEs using standardized terminology…
In 2005, I published a systematic review of ophthalmic AEs after SMT. At the time, there were 14 published case reports. Clinical symptoms and signs included:
- central retinal artery occlusion,
- nystagmus,
- Wallenberg syndrome,
- ptosis,
- loss of vision,
- ophthalmoplegia,
- diplopia,
- Horner’s syndrome…
Vascular accidents are the most frequent serious AEs after chiropractic SMT, but they are certainly not the only complications that have been reported. Other AEs include:
- atlantoaxial dislocation,
- cauda equina syndrome,
- cervical radiculopathy,
- diaphragmatic paralysis,
- disrupted fracture healing,
- dural sleeve injury,
- haematoma,
- haematothorax,
- haemorrhagic cysts,
- muscle abscess,
- muscle abscess,
- myelopathy,
- neurologic compromise,
- oesophageal rupture
- pneumothorax,
- pseudoaneurysm,
- soft tissue trauma,
- spinal cord injury,
- vertebral disc herniation,
- vertebral fracture…
In 2010, I reviewed all the reports of deaths after chiropractic treatments published in the medical literature. My article covered 26 fatalities but it is important to stress that many more might have remained unpublished. The cause usually was a vascular accident involving the dissection of a vertebral artery (see above). The review also makes the following important points:
- … numerous deaths have been associated with chiropractic. Usually high-velocity, short-lever thrusts of the upper spine with rotation are implicated. They are believed to cause vertebral arterial dissection in predisposed individuals which, in turn, can lead to a chain of events including stroke and death. Many chiropractors claim that, because arterial dissection can also occur spontaneously, causality between the chiropractic intervention and arterial dissection is not proven. However, when carefully evaluating the known facts, one does arrive at the conclusion that causality is at least likely. Even if it were merely a remote possibility, the precautionary principle in healthcare would mean that neck manipulations should be considered unsafe until proven otherwise. Moreover, there is no good evidence for assuming that neck manipulation is an effective therapy for any medical condition. Thus, the risk-benefit balance for chiropractic neck manipulation fails to be positive.
- Reliable estimates of the frequency of vascular accidents are prevented by the fact that underreporting is known to be substantial. In a survey of UK neurologists, for instance, under-reporting of serious complications was 100%. Those cases which are published often turn out to be incomplete. Of 40 case reports of serious adverse effects associated with spinal manipulation, nine failed to provide any information about the clinical outcome. Incomplete reporting of outcomes might therefore further increase the true number of fatalities.
- This review is focussed on deaths after chiropractic, yet neck manipulations are, of course, used by other healthcare professionals as well. The reason for this focus is simple: chiropractors are more frequently associated with serious manipulation-related adverse effects than osteopaths, physiotherapists, doctors or other professionals. Of the 40 cases of serious adverse effects mentioned above, 28 can be traced back to a chiropractor and none to a osteopath. A review of complications after spinal manipulations by any type of healthcare professional included three deaths related to osteopaths, nine to medical practitioners, none to a physiotherapist, one to a naturopath and 17 to chiropractors. This article also summarised a total of 265 vascular accidents of which 142 were linked to chiropractors. Another review of complications after neck manipulations published by 1997 included 177 vascular accidents, 32 of which were fatal. The vast majority of these cases were associated with chiropractic and none with physiotherapy. The most obvious explanation for the dominance of chiropractic is that chiropractors routinely employ high-velocity, short-lever thrusts on the upper spine with a rotational element, while the other healthcare professionals use them much more sparingly.
Another review summarised published cases of injuries associated with cervical manipulation in China. A total of 156 cases were found. They included the following problems:
- syncope (45 cases),
- mild spinal cord injury or compression (34 cases),
- nerve root injury (24 cases),
- ineffective treatment/symptom increased (11 cases),
- cervical spine fracture (11 cases),
- dislocation or semi-luxation (6 cases),
- soft tissue injury (3 cases),
- serious accident (22 cases) including paralysis, deaths and cerebrovascular accidents.
Manipulation including rotation was involved in 42% of all cases. In total, 5 patients died…
To sum up … chiropractic SMT can cause a wide range of very serious complications which occasionally can even be fatal. As there is no AE reporting system of such events, we nobody can be sure how frequently they occur.
[references from my text can be found in the book]This is an analysis that I have long hesitated to conduct. The reason for my hesitation is simple: some people might think it is vindictive, revengeful or ad hominem. After reflecting about it for years, I have now decided to go ahead with it (sorry, it’s a bit lengthy). This case study is not meant to be vindictive, but offers an important insight into the power of conflicts of interest in SCAM that are not financial but ideological. I think it is crucial that people are aware of and consider such conflicts carefully, and I can’t see how else I might demonstrate my point so plainly.
Dr Adrian White was a co-worker of mine for about 10 years. He became a trusted colleague, my ‘right hand’ man and even my deputy at my Exeter department. When I discovered that my trust had been misplaced, I did not prolong his contract (I will not dwell on this episode, those who are interested find it in my memoir). Adrian then got a senior research fellowship with Prof John Campbell (not my favourite colleague at Exeter) at the department of general practice where he continued his research on acupuncture for about 10 more years largely unsupervised.
Adrian had been an acupuncturist body and soul (in fact, I had never before met anyone so utterly convinced of the value of this therapy). When he joined my team, he was scientifically naive, and we spent many month trying to teach him how to think like a scientist. Initially, he found it very difficult to think critically about acupuncture. Later, I thought the problem was under control. Yet, most of his research in my department was guided by me and tightly supervised (i.e. I made sure that out studies were testing rather than promoting SCAM, and that our reviews were critical assessments of the existing evidence).
Thus there exist two separate and well-documented periods of a pro-acupuncture researcher:
- 10 years guided by me and members of my team;
- 10 years largely unsupervised.
What could be more tempting than to compare Adrian’s output during these two periods?
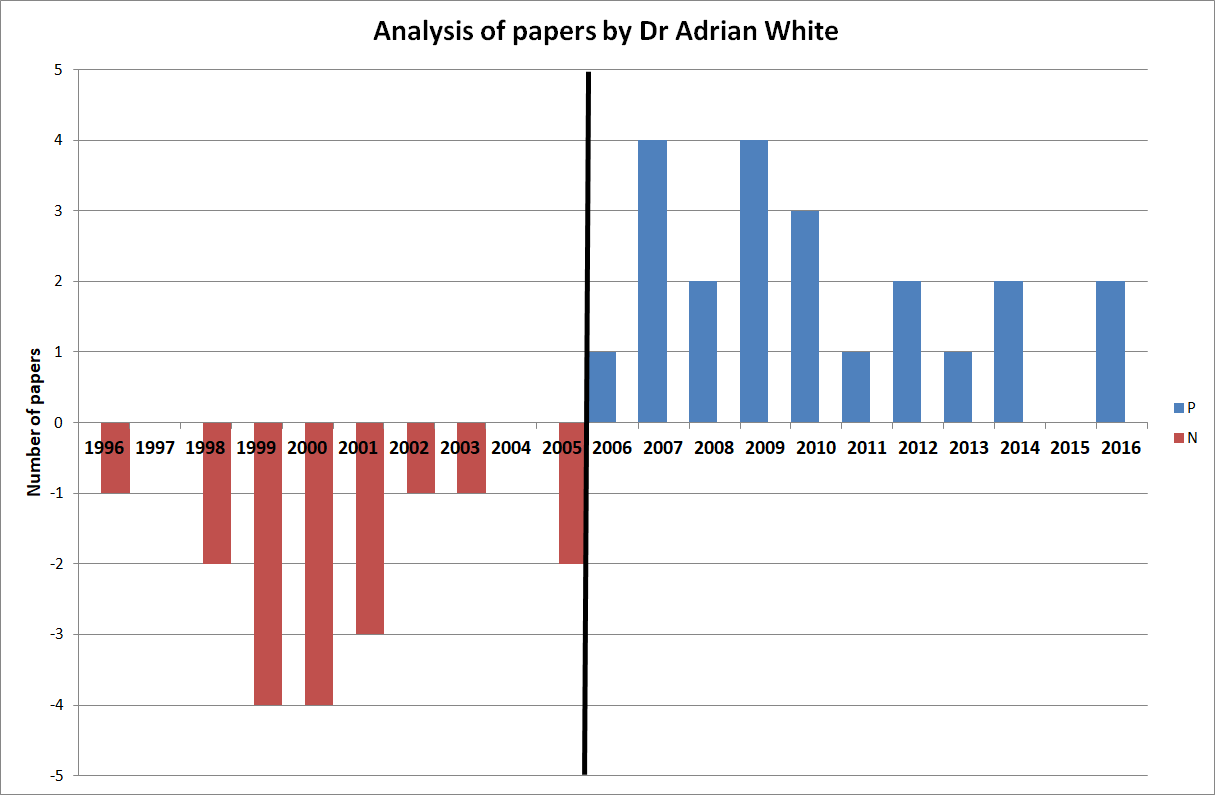
To do this, I looked up all of Adrian’s 120 publications on acupuncture and selected those 52 articles that generated factual new data (mostly clinical trials or systematic reviews). As it happens, they are numerically distributed almost equally within the two periods. The endpoints for my analysis were the directions of the conclusions of his papers. I therefore extracted, dated, and rated the 52 articles as follows:
- P = positive from the point of view of an acupuncture advocate,
- N = negative from the point of view of an acupuncture advocate.
- P/N = not clearly pointing in either direction.
To render this exercise transparent (occasionally, I was not entirely sure about my ratings), I copied all the 52 conclusions and provided links to the original papers so that anyone inferested is able to check easily.
Here are my findings. Articles 1 – 27 were published AFTER Adrian had left my department; articles 28 – 52 are his papers from the time while he worked with me.
- A definitive three-arm trial is feasible. Further follow-up reminders, minimum data collection and incentives should be considered to improve participant retention in the follow-up processes in the standardised advice and exercise booklet arm. (2016) P/N
- The available evidence suggests that adding acupuncture to symptomatic treatment of attacks reduces the frequency of headaches. Contrary to the previous findings, the updated evidence also suggests that there is an effect over sham, but this effect is small. The available trials also suggest that acupuncture may be at least similarly effective as treatment with prophylactic drugs. Acupuncture can be considered a treatment option for patients willing to undergo this treatment. As for other migraine treatments, long-term studies, more than one year in duration, are lacking. (2016) P
- The available results suggest that acupuncture is effective for treating frequent episodic or chronic tension-type headaches, but further trials – particularly comparing acupuncture with other treatment options – are needed. (2016) P
- Acupuncture during pregnancy appears to be associated with few AEs when correctly applied. (2014) P
- Although pooled estimates suggest possible short-term effects there is no consistent, bias-free evidence that acupuncture, acupressure, or laser therapy have a sustained benefit on smoking cessation for six months or more. However, lack of evidence and methodological problems mean that no firm conclusions can be drawn. Electrostimulation is not effective for smoking cessation. Well-designed research into acupuncture, acupressure and laser stimulation is justified since these are popular interventions and safe when correctly applied, though these interventions alone are likely to be less effective than evidence-based interventions. (2014) P
- The current evidence suggests that acupuncture may have some effects on drug dependence that have been missed because of choice of outcome in many previous studies, and future studies should use outcomes suggested by clinical experience. Body points and electroacupuncture, used in the original clinical observation, justify further research. (2013) P
- Acceptability is very high and may be maximised by taking a number of factors into account: full information should be provided before treatment begins; flexibility should be maintained in the appointment system and different levels of contact between fellow patients should be fostered; sufficient space and staffing should be provided and single-sex groups used wherever possible. (2012) P
- This is the first evaluation of nurse-led group (multibed) acupuncture clinics for patients with knee osteoarthritis to include a 2 year follow-up. It shows the practicability of offering a low-cost acupuncture service as an alternative to knee surgery and the service’s success in providing long-term symptom relief in about a third of patients. Using realistic assumptions, the cost consequences for the local commissioning group are an estimated saving of £100 000 a year. Sensitivity analyses are presented using different assumptions. (2012) P
- There is no consistent, bias-free evidence that acupuncture, acupressure, laser therapy or electrostimulation are effective for smoking cessation, but lack of evidence and methodological problems mean that no firm conclusions can be drawn. Further, well designed research into acupuncture, acupressure and laser stimulation is justified since these are popular interventions and safe when correctly applied, though these interventions alone are likely to be less effective than evidence-based interventions. (2011) P/N
- Eight (8) of 10 international acupuncture experts were able to reach consensus on the syndromes, symptoms, and treatment of postmenopausal women with hot flashes. The syndromes were similar to those used by practitioners in the ACUFLASH clinical trial, but there were considerable differences between the acupuncture points. This difference is likely to be the result of differences in approach of training schools, and whether it is relevant for clinical outcomes is not well understood. (2011) P
- 70% of those patients eligible to participate volunteered to do so; all participants had clinically identified MTrPs; a 100% completion rate was achieved for recorded self-assessment data; no serious adverse events were reported as a result of either intervention; and the end of treatment attrition rate was 17%. A phase III study is both feasible and clinically relevant. This study is currently being planned. (2010) P
- In conclusion, the results from all studies are in agreement with the hypothesis that acupuncture needling relieves hot flushes. There are few data however supporting the hypothesis that the effect of acupuncture is point specific. Future research should investigate whether there is a biological effect of needling on hot flushes or not, whether tailored treatment is superior to standardised treatment, and ways of delivering treatment that causes least discomfort and least cost. (2010) P
- Acupuncture can contribute to a more rapid reduction in vasomotor symptoms and increase in health-related quality of life in postmenopausal women but probably has no long-term effects. (2010) P
- within the context of this pilot study, the sham acupuncture intervention was found to be a credible control for acupuncture. This supports its use in a planned, definitive, randomised controlled trial on a similar whiplash injured population. (2009) N/P
- factors other than the TCM syndrome diagnoses and the point selection may be of importance regarding the outcome of the treatment. (2009) N/P
- Acupuncture plus self-care can contribute to a clinically relevant reduction in hot flashes and increased health-related quality of life in postmenopausal women. (2009) P
- the authors conclude that acupuncture could be a valuable non-pharmacological tool in patients with frequent episodic or chronic tension-type headaches. (2009) P
- there is consistent evidence that acupuncture provides additional benefit to treatment of acute migraine attacks only or to routine care. There is no evidence for an effect of ‘true’ acupuncture over sham interventions, though this is difficult to interpret, as exact point location could be of limited importance. Available studies suggest that acupuncture is at least as effective as, or possibly more effective than, prophylactic drug treatment, and has fewer adverse effects. Acupuncture should be considered a treatment option for patients willing to undergo this treatment. (2009) P
- We have conducted the first survey of the effects of provision of acupuncture in UK general practice, using data provided by the NHS, and uncovered a wide variation in the availability of the service in different areas. We have been unable to demonstrate any consistent differences in the prescribing or referral rates that could be due to the use of acupuncture in these practices. The wide variation in the data means that if such a trend exists, a very large survey would be needed to identify it. However, we discovered inaccuracies and variations in presentation of data by the PCTs which have made the numerical input, and hence our results, unreliable. Thus the practicalities of access to data and the problems with data accuracy would preclude a nationwide survey. (2008) P
- In conclusion, there is limited evidence deriving from one study that deep needling directly into myofascial trigger points has an overall treatment effect when compared with standardised care. Whilst the result of the meta-analysis of needling compared with placebo controls does not attain statistically significant, the overall direction could be compatible with a treatment effect of dry needling on myofascial trigger point pain. However, the limited sample size and poor quality of these studies highlights and supports the need for large scale, good quality placebo controlled trials in this area. (2009) P
- We conclude that limited evidence supports acupuncture use in treating pregnancy-related pelvic and back pain. Additional high-quality trials are needed to test the existing promising evidence for this relatively safe and popular complementary therapy. (2008) P
- Acupuncture appears to offer symptomatic improvement to some patients with fibromyalgia in a tertiary clinic who have failed to respond to other treatments. In view of its safety, further acupuncture research is justified in this population. (2007) P
- It is speculated that optimal results from acupuncture treatment for osteoarthritis of the knee may involve: climatic factors, particularly high temperature; high expectations of patients; minimum of four needles; electroacupuncture rather than manual acupuncture, and particularly, strong electrical stimulation to needles placed in muscle; and a course of at least 10 treatments. These factors offer some support to criteria for adequate acupuncture used in the recent review. In addition, ethnic and cultural factors may influence patients’ reporting of their symptoms, and different versions of an outcome measure are likely to differ in their sensitivity – both factors which may lead to apparent rather than real differences between studies. The many variables in a study are likely to be more tightly controlled in a single centre study than in multicentre studies. (2007) P
- Any effects of acupressure on smoking withdrawal, as an adjunct to the use of NRT and behavioural intervention, are unlikely to be detectable by the methods used here and further preliminary studies are required before the hypothesis can be tested. (2007) P
- Auricular acupuncture appears to be effective for smoking cessation, but the effect may not depend on point location. This calls into question the somatotopic model underlying auricular acupuncture and suggests a need to re-evaluate sham controlled studies which have used ‘incorrect’ points. Further experiments are necessary to confirm or refute these observational conclusions. (2006) P
- Acupuncture that meets criteria for adequate treatment is significantly superior to sham acupuncture and to no additional intervention in improving pain and function in patients with chronic knee pain. Due to the heterogeneity in the results, however, further research is required to confirm these findings and provide more information on long-term effects. (2007) P
- There is no consistent evidence that acupuncture, acupressure, laser therapy or electrostimulation are effective for smoking cessation, but methodological problems mean that no firm conclusions can be drawn. Further research using frequent or continuous stimulation is justified. (2006) N/P
- Acupuncture is not superior to sham treatment for recovery in activities of daily living and health-related quality of life after stroke, although there may be a limited effect on leg function in more severely affected patients. (2005) N
- The evidence from controlled trials is insufficient to conclude whether acupuncture is an effective treatment for depression, but justifies further trials of electroacupuncture. (2005) N
- Acupuncture effectively relieves chronic low back pain. No evidence suggests that acupuncture is more effective than other active therapies. (2005) N/P
- In view of the small number of studies and their variable quality, doubt remains about the effectiveness of acupuncture for gynaecological conditions. Acupuncture and acupressure appear promising for dysmenorrhoea, and acupuncture for infertility, and further studies are justified. (2003) N
- In conclusion, the results suggest that the procedure using the new device is indistinguishable from the same procedure using real needles in acupuncture naïve subjects, and is inactive, where the specific needle sensation (de qi) is taken as a surrogate measure of activity. It is therefore a valid control for acupuncture trials. The findings also lend support to the existence of de qi, a major concept underlying traditional Chinese acupuncture. (2002) N/P
- There is no clear evidence that acupuncture, acupressure, laser therapy or electrostimulation are effective for smoking cessation. (2002) N
- Collectively, these data imply that acupuncture is superior to various control interventions, although there is insufficient evidence to state whether it is superior to placebo. (2002) N/P
- In conclusion, the incidence of adverse events following acupuncture performed by doctors and physiotherapists can be classified as minimal; some avoidable events do occur. Acupuncture seems, in skilled hands, one of the safer forms of medical intervention. (2001) N/P
- Based on the evidence of rigorous randomised controlled trials, there is no compelling evidence to show that acupuncture is effective in stroke rehabilitation. Further, better-designed studies are warranted. (2001) N
- Although it has already been demonstrated that severe adverse events seem to be uncommon in standard practice, many serious cases of negligence have been found in the present review, suggesting that training system for acupuncturists (including medical doctors) should be improved and that unsupervised self-treatment should be discouraged. (2001) N
- Direct needling of myofascial trigger points appears to be an effective treatment, but the hypothesis that needling therapies have efficacy beyond placebo is neither supported nor refuted by the evidence from clinical trials. Any effect of these therapies is likely because of the needle or placebo rather than the injection of either saline or active drug. Controlled trials are needed to investigate whether needling has an effect beyond placebo on myofascial trigger point pain. (2001) N/P
- Although the incidence of minor adverse events associated with acupuncture may be considerable, serious adverse events are rare. Those responsible for establishing competence in acupuncture should consider how to reduce these risks. (2001) N
- In conclusion, this study does not provide evidence that this form of acupuncture is effective in the prevention of episodic tension-type headache. (2000) N
- The present study provides no strong evidence to support the hypothesis that the acupuncture point SP6 is more tender in women and in men. Recommendations for further investigations are discussed. (2000) N
- Acupuncture has not been demonstrated to be efficacious as a treatment for tinnitus on the evidence of rigorous randomized controlled trials. (2000) N
- We conclude that acupuncture continues to be associated with occasional, serious adverse events and fatalities. These events have no geographical limits. Most of these events are due to negligence. Everyone concerned with setting standards, delivering training, and maintaining competence in acupuncture should familiarise themselves with the lessons to be learnt from these untoward events. (2000) N
- Overall, the existing evidence suggests that acupuncture has a role in the treatment of recurrent headaches. However, the quality and amount of evidence is not fully convincing. There is urgent need for well-planned, large-scale studies to assess effectiveness and efficiency of acupuncture under real life conditions. (1999) N/P
- While the frequency of adverse effects of acupuncture is unknown and they may be rare, knowledge of normal anatomy and anatomical variations is essential for safe practice and should be reviewed by regulatory bodies and those responsible for training courses. (1999) N
- In conclusion, the hypothesis that acupuncture is efficacious in the treatment of neck pain is not based on the available evidence from sound clinical trials. Further studies are justified. (1999) N
- Even though all studies are in accordance with the notion that acupuncture is effective for temporomandibular joint dysfunction, this hypothesis requires confirmation through more rigorous investigations. (1999) N
- Acupuncture is not free of risks. All adverse events reported in 1997 would have been avoidable. The absolute number of cases is small, but the degree of underreporting remains unknown. (1999) N
- This form of electroacupuncture is no more effective than placebo in reducing nicotine withdrawal symptoms. (1998) N
- Acupuncture was shown to be superior to various control interventions, although there is insufficient evidence to state whether it is superior to placebo. (1998) N/P
- Considerable variation was observed in the scores awarded by the acupuncture experts. (1998) N
- It is therefore concluded that, according to the data published to date, the evidence that acupuncture is a useful adjunct for stroke rehabilitation is encouraging but not compelling. More and better trials are required to clarify this highly relevant issue. (1996) N
The results are remarkable (particularly considering that one would not expect unbiased studies or reviews of acupuncture to generate plenty of positive conclusions):
0 times N, 5 times N/P, 22 times P – after Adrian had left my department,
17 times N, 7 times N/P, 0 times P – while Adrian worked in my department.
From these figures, it is tempting to calculate the ratios for both periods of negative : positive conclusions:
zero versus infinite
If that is not impressive, I don’t know what is!
Looking just at the positive and the negative papers over the years:
 One could discuss these papers in more detail, but I think this is hardly necessary. Just a few highlights perhaps: look at articles No 5, 20 and 27 for examples of turning an essentially negative finding into a positive conclusion. Notice that Adrian conducted a clinical trial of acupuncture for smoking cessation (No 49) while working with me and later published uncritical positive reviews on the subject. Does this not indicate that he distrusted his own study because it had not generated the result he had hoped for?
One could discuss these papers in more detail, but I think this is hardly necessary. Just a few highlights perhaps: look at articles No 5, 20 and 27 for examples of turning an essentially negative finding into a positive conclusion. Notice that Adrian conducted a clinical trial of acupuncture for smoking cessation (No 49) while working with me and later published uncritical positive reviews on the subject. Does this not indicate that he distrusted his own study because it had not generated the result he had hoped for?
Of course, my analysis is merely a case study and therefore my findings are not generalisable. However, in my personal experience, the described phenomenon is by no means an exception in SCAM research. I have observed similar phenomena over and over again. Just look at the ALTERNATIVE MEDICINE HALL OF FAME that I created for this blog:
- John Weeks (editor of JCAM)
- Deepak Chopra (US entrepreneur)
- Cheryl Hawk (US chiropractor)
- David Peters (osteopathy, homeopathy, UK)
- Nicola Robinson (TCM, UK)
- Peter Fisher (homeopathy, UK)
- Simon Mills (herbal medicine, UK)
- Gustav Dobos (various, Germany)
- Claudia Witt (homeopathy, Germany and Switzerland)
- George Lewith (acupuncture, UK)
- John Licciardone (osteopathy, US)
But Adrian’s case might be unique because it allows us to make a longitudinal observation over two decades. And it suggests to me that an ideological bias can (and often is) so strong and indistructable that is re-emerges as soon as it is no longer kept under strict control.
I have long suspected that ideological conflicts of interest have a much more powerful influence in SCAM research than financial ones. Such an overpowering influence might even be characteristic to much of SCAM research. And because it can be so dominant, it seems important to know about. People reading research need to be aware that it originates from a biased source, and funders who finance research would be wise to think twice about supporting researchers who are likely to generate findings that are biased and therefore false-positive. In the final analysis, such research is worse than no research at all.
We are all prone to fall victim to the ‘post hoc ergo propter hoc’ fallacy. It describes the erroneous assumption that something that happened after an event was cased by that event. The fallacy is essentially due to confusing correlation with causation:
- the sun does not rise because the rooster has crowed;
- yellow colouring of the 2nd and 3rd finger of a smoker is not the cause of lung cancer;
- some children developing autism after vaccinations does not mean that autism is caused by vaccination.
As I said, we are all prone to this sort of thing, even though we know better. Scientists, journal editors and reviewers of medical papers, however, should not allow themselves to be fooled by overt cases of the ‘post hoc ergo propter hoc’ fallacy. And if they do, they have lost all credibility – just like the individuals involved in a recent paper on animal homeopathy.
Pododermatitis in penguins usually occurs after changes in normal activity that result from being held captive. It is also called ‘bumlefoot’ (which fails to reflect the seriousness of the condition) and amounts to one of most frequent and important clinical complications in penguins kept in captivity or in rehabilitation centres.
This veterinary case study reports the use of oral homeopathic treatment on acute and chronic pododermatitis in five Magellanic penguins in a zoological park setting. During treatment, the patients remained in the penguins’ living area, and the effect of the treatment on the progression of their lesions was assessed visually once weekly. The treatment consisted of a combination of Arnica montana and Calcarea carbonica.
After treatment, the appearance of the lesions had noticeably improved: in the majority of penguins there was no longer evidence of infection or edema in the feet. The rate of recovery depended on the initial severity of the lesion. Those penguins that still showed signs of infection nevertheless exhibited a clear diminution of the size and thickness of the lesions. Homeopathic treatment did not cause any side effects.
The authors concluded that homeopathy offers a useful treatment option for pododermatitis in captive penguins, with easy administration and without side effects.
So, the homeopathic treatment happened before the recovery and, according to the ‘post hoc ergo propter hoc’ fallacy, the recovery must have been caused by the therapy!
I know, this is a tempting conclusion for a lay person, but it is also an unjustified one, and the people responsible for this paper are not lay people. Pododermitis does often disappear by itself, particularly if the hygenic conditions under which the penguins had been kept are improved. In any case, it is a potentially life-threatening condition (a bit like an infected bed sore in an immobilised human patient) that can be treated, and one should certainly not let a homeopath deal with it.
I think that the researchers who wrote the article, the journal editor who accepted it for publication, and the referees who reviewed the paper should all bow their heads in shame and go on a basic science course (perhaps a course in medical ethics as well) before they are let anywhere near research again.
Coffee enemas consist of the administration of warm coffee via the rectum into a patient’s intestines. They are popular, not least because they cause profuse bowel movements and thus lead to immediate relief of constipation and therefore to short-lasting weight loss.
Coffee enemas are promoted for detox under the erroneous assumption that that the content of our colon is toxic, an obsolete theory known as ‘autointoxication’. Other notions assume that coffee enemas have beneficial antioxidant effects or stimulate the liver. Supporters of coffee enemas also claim they are effective treatments for:
- boosting immunity
- increasing energy
- preventing yeast overgrowth
- treating autoimmune diseases
- excreting parasites from the digestive tract
- removing heavy metals from the body
- alleviating depression
- treating cancer
Coffee enemas can cause adverse reactions some of which can be severe and have even caused fatalities:
- electrolyte imbalances
- rectal burns
- nausea
- vomiting
- cramping
- bloating
- dehydration
- bowel perforation
This new systematic review was conducted to investigate the safety and effectiveness of self-administered coffee enema and to provide evidence about its benefits and risks.
Relevant studies were retrieved from multiple electronic literature searches. Considering self-administered coffee enema being used in a various indication, study population was not restricted. Any types of published studies that included outcomes of effectiveness or safety of self-administered coffee enema with or without comparators were eligible for inclusion in this systematic review. Data on biomedical indications, patient-reported outcomes, and adverse events were collected. Descriptive analyses were planned because diverse health conditions and outcome variables did not allow for quantitative synthesis.
Nine case reports that describe adverse events were identified and included in the analysis. The reported problems included:
- colitis,
- proctocolitis,
- rectal perforation, peritonitis,
- rectal burn,
- cardiorespitatory arrest, followed by death,
- hepatic failure, followed by death,
- vomiting, dyspnoea, followed by death.
No study reporting on the effectiveness of coffee enema was found.
The authors concluded that, based on the evidences reviewed, this systematic review does not recommend coffee enema self-administration as a SCAM modality that can be adopted as a mean of self-care, given the unsolved issues on its safety and insufficient evidence with regard to the effectiveness.
So-called alternative medicine (SCAM) is full of truly barmy ideas, but coffee enems are amongst the worst. They are disgusting, uncomfortable, useless and risky. I am posting this article with the sincere hope that nobody reading it will ever consider using such nonsense.
On his website, Phillip Hughes – D. Hom (Med), M.A.R.H, describes himself as follows:
In the early 1990’s my life was turned upside-down by a prolapsed disk in my back, putting me in traction in a hospital for 6 weeks! The doctor’s prognosis was poor, leaving me with little hope of full mobility, and no choice but to seek treatment elsewhere.
I decided on Homeopathy, and after treatment I experienced real change in my condition within a month, and was completely well within 3 months. I was so inspired by this I decided to study Homeopathy myself – and in 1994 I enrolled at the Hahnemann College of Homeopathy in London, qualifying in 1998.
After qualifying I set up my first clinic in Waterloo, Liverpool. I also became a senior lecturer at the Hahnemann College of Homeopathy, and founder of the Liverpool branch of the Hahnemann College.
I then moved my clinic to College Road Crosby, when I took up the role of secretary of Homeopathic Medical Association (since resigned). It was during this time that my wife Rosa found a lump in her breast, motivating us again to seek safer and alternative treatments, this time using Thermography. We now run Thermography and Homeopathic clinics side by side.
I had never heard of Mr Hughes until yesterday, when it was reported that he had treated a Sean Walsh, a young musician, for Hodgkin lymphoma that had initially been controlled with chemotherapy, but had later returned. Here is an excerpt from the sad story:
Sean was having scans at a clinic – Medical Thermal Imaging – run by a couple called Philip and Rosa Hughes. Philip Hughes, a homeopath, had previously told Sean’s parents he’d successfully treated Rosa for breast cancer. Dawn [Sean’s girlfriend] went along to Sean’s first appointment. “Phil was just talking all about how damaging chemotherapy is, you know, on the human body… saying, ‘I’ve had lots of people come to my clinic, but by the time I get them, they’re shot with all this chemotherapy, so I can’t help them … And then he was talking all about how you can change your diet, which can reverse cancer. He’d said that Rosa had developed breast cancer. She’d had a lump in her breast, and she decided not to do hospital treatment, and she was going to, you know, reverse the cancer herself. So obviously Sean’s listening to this thinking, ‘Well, if one person’s done it, and then I’m hearing other little stories off them, I can do this’. Sean’s scans did carry a disclaimer, stating that thermography does not see or diagnose cancer and recommending further clinical investigation. But the scan results seemed reassuring – and Sean was convinced his cancer had gone. ‘Medical Thermal Imaging’ describe their scans as “100% safe and radiation-free”.
To find out more about the service the Hughes were offering, a BBC reporter went to the clinic where Sean had his scans, posing as a patient who’d found a lump. They were seen by Rosa Hughes, who had provided scans for Sean. Rosa told our reporter that when she went to the breast clinic to have her lump investigated, she should have an ultrasound rather than a mammogram. This is a transcript of what she said: “Not a mammogram, because you’re going to get radiated, and it’s going to squash… and the amount of women that have had their tumours, the tumour burst, that spreads cancer.”
[The BBC] asked cancer specialist Prof Andrew Wardley, of Manchester’s Christie Hospital, to review the medical claims Rosa Hughes made to our reporter. “That’s preposterous. You don’t burst tumours, they are solid. You do squash the breast down to do a mammogram, it is unpleasant but it’s a short-term thing. You do not spread cancer by doing a mammogram, that’s a complete fallacy.” Rosa and Philip Hughes say they “utterly reject” the allegation that they gave Mr Walsh inappropriate advice. They added they had “consistently made clear” that thermography can only be used alongside other tests, such as MRIs or mammograms.
At first Sean believed he had cured his own cancer. But tragically Sean was wrong. Gradually his health declined, until he was rushed to hospital in Liverpool where medical staff found he had multiple tumours in his stomach and chest. He did eventually receive chemotherapy but it was too late.
Sean died in January 2019.
On Philip Hughes’ website, he advertises his services with the help of several testimonials from happy customers. Here is one of them:
In November 2000, I had an aggressive Sarcoma Tumour removed along with my left lung. Shortly after surgery I was referred to Weston Park Hospital, Sheffield for ‘follow up’ treatments where I was offered both chemotherapy and radiotherapy. At around the same time, I first visited Waterloo Homeopathic Clinic on a friends recommendation. After this initial introduction to Homeopathy I began ti educate myself about my condition and possible treatments. Consequently I considered chemotherapy to be a crude option and decided to refuse it. However, the frightening thought of this aggressive tumour returning encourages me to go ahead with a six week course of radiotherapy as a precaution alongside Homeopathic treatment. Accordingly this holistic approach resulted in my immune system being boosted by Homeopathy and my body prepared for this medical treatment. Leading up to the radiotherapy and during the six weeks of treatments, I took a rang of Homeopathic remedies. Radium Brom, in my opinion, was undoubtedly the input that enabled me to go through an intense course of treatment daily and continue my healthy recovery. I didn’t miss a days work and finished a half marathon only three weeks after completing the radiotherapy. I have since remained in good health and all checks been clear.
I have said it often, but it seems I have to say it again: the homeopathic remedy might be harmless, but the homeopath isn’t!
PS
The BBC documentary provides many more details about Sean and another of Mr Hughes’ patients. It also shows some rare footage from the inside of the Gerson clinic in Mexico where Sean went for a while. Very sad but well worth watching!!!
Yesterday, I received a tweet from a guy called Bart Huisman (“teacher beekeeping, nature, biology, classical homeopathy, agriculture, health science, social science”). I don’t know him and cannot remember whether I had previous contact with him. His tweet read as follows:
“Why should anyone believe what Professor Edzard Ernst says, after he put his name to a BBC programme, he now describes as “deception”.”
This refers to a story that I had almost forgotten. It’s a nice one with a ‘happy ending’, so let me recount it here briefly.
In 2005, the BBC had hired me as an advisor for their 4-part TV series on alternative medicine.
The first part of the series was on acupuncture, and Prof Kathy Sykes presented the opening scene taking place in a Chinese operation theatre. In it a Chinese women was having open heart surgery with the aid of acupuncture. Kathy’s was visibly impressed and said on camera that the patient was having the surgery “with only needles to control the pain.” However, the images clearly revealed that the patient was receiving all sorts of other treatments given through intra-venous lines. So, Prof Sykes was telling the UK public a bunch of porkies. This was bound to confuse many viewers.
One of them was Simon Singh. At the time, I did not know Simon (to be honest, I did not even know of him) and was surprised to receive a phone call from him. He politely asked me to confirm that I had been the adviser of the BBC on this production. I was happy to confirm this fact. Then he asked why I had missed such a grave error. I replied that I could not possibly have spotted it, because all I had been asked to do was to review and correct the text of the programme which the BBC had sent to me by email. Before it was broadcast, I had not seen a single passage of the film.
Correcting the text had already led to several problems (not so much regarding the acupuncture part but mostly the other sections), because the BBC was reluctant to change several of the mistakes I had identified. When I told them that, in this case, I would quit, they finally found a way to alter them. But the cooperation had been far from easy. I explained all this to Simon and eventually he asked me whether I would be willing to support the official complaint he was about to file with the BBC. I agreed. This is probably where I used the term ‘deception’ that Mr Huisman mentioned in his tweet.
So, Simon submitted his complaint and eventually won the case.
But this is not the happy ending I was referring to.
During the course of the complaint, Simon and I realised that we were thinking alike and were getting on well. A few months later, he suggested that the two of us write a book together about alternative medicine. At first, I was hesitant. Simon said, “let’s try just one chapter, and see how it works out.” So we did. It turned out to be fun and instructive for both of us. So we did the other chapters as well. The book was published in 2008 and is called TRICK OR TREATMENT. It was published in about 20 different languages and the German version became ‘science book of the year in 2011 (I think).
And that’s not the happy ending either (in fact, it caused a lot of hardship for Simon who was sued by the BCA; luckily, he won that case too).
The real happy ending is the fact that Simon and I became friends for life.
Thank you Bart Huisman for reminding me of this rather lovely story.
I have known for a long time that homeopathy can be dangerous, not least through the neglect of effective treatments for seriously ill patients. But I did not know that it can cause a bone fracture – until yesterday, that is.
Yes, you have understood me correctly! Here is the first case-report of a homeopathy-induced bone fracture:
My sister in law has two charming elderly ladies as neighbours. They are now in their 90ies and have, over the years, become very frail. She therefore has taken to looking after them where she can. Since the two sisters rarely leave their home these days, they have developed a new hobby: ordering things they find attractive through the post; it seems to be their greatest pleasure and has frequently led to complications that could easily fill a book of short stories.
Recently, an advertisement caught they eyes. It proclaimed in no uncertain terms that, even at their advanced age, they could re-gain some strength and energy through a specific homeopathic remedy (Boiron, I suspect, but I cannot be sure). This, of course, sounded far too good to not give it a try, and the two sisters promptly ordered what seemed to the the answer to their prayers.
The little package arrived yesterday, and the excitement must have been palpable. The more impatient of the two sisters insisted to try the wonder drug straight away. With her hands shaking in anticipation, she opened the tiny vial of globuli. Overwhelmed by trepidation, she spilled the entire content of globuli on the floor.
‘That’s bad but not disastrous’, she thought. Trying to pick them up, she stepped on some of them. As our frail hero weighs not even 50kg, the globuli acted like the ball-bearings or a pair of roller-skates. Her feet flew off, she lost her balance and landed abruptly and painfully on her side under the kitchen table covered by a table lamp and a chair.
The second sister rushed to help but proved to be too frail to get the patient back on her feet. This is when my sister in law was phoned and, ignoring the current lock-down, arrived with her husband to the rescue. What they saw was a scene of utter devastation: Globuli everywhere, their elderly neighbour moaning on the floor covered with various items she has tried to hold on to when attempting to prevent the fall. Together they managed to get the patient back up, but soon realised that she was badly injured. An ambulance was called and in the local hospital an X-ray confirmed the diagnosis: rib fracture.
I am glad to say, the old lady – my best wishes to her and her sister! – is now back home and recovering well. Little does she know that she is about to enter the history books of medicine as the first ever documented case of ‘homeopathy-induced rib fracture’.
During my almost 30 years of research into so-called alternative medicine (SCAM), I have published many papers which must have been severe disappointments to those who advocate SCAM or earn their living through it. Many SCAM proponents thus reacted with open hostility. Others tried to find flaws in those articles which they found most upsetting with a view of discrediting my work. The 2012 article entitled ‘A Replication of the Study ‘Adverse Effects of Spinal Manipulation: A Systematic Review‘ by the Australian chiropractor, Peter Tuchin, seems to be an example of the latter phenomenon (used recently by Jens Behnke in an attempt to defame me).
Here is the abstract of the Tuchin paper:
Objective: To assess the significance of adverse events after spinal manipulation therapy (SMT) by replicating and critically reviewing a paper commonly cited when reviewing adverse events of SMT as reported by Ernst (J Roy Soc Med 100:330-338, 2007).
Method: Replication of a 2007 Ernst paper to compare the details recorded in this paper to the original source material. Specific items that were assessed included the time lapse between treatment and the adverse event, and the recording of other significant risk factors such as diabetes, hyperhomocysteinemia, use of oral contraceptive pill, any history of hypertension, atherosclerosis and migraine.
Results: The review of the 32 papers discussed by Ernst found numerous errors or inconsistencies from the original case reports and case series. These errors included alteration of the age or sex of the patient, and omission or misrepresentation of the long term response of the patient to the adverse event. Other errors included incorrectly assigning spinal manipulation therapy (SMT) as chiropractic treatment when it had been reported in the original paper as delivered by a non-chiropractic provider (e.g. Physician).The original case reports often omitted to record the time lapse between treatment and the adverse event, and other significant clinical or risk factors. The country of origin of the original paper was also overlooked, which is significant as chiropractic is not legislated in many countries. In 21 of the cases reported by Ernst to be chiropractic treatment, 11 were from countries where chiropractic is not legislated.
Conclusion: The number of errors or omissions in the 2007 Ernst paper, reduce the validity of the study and the reported conclusions. The omissions of potential risk factors and the timeline between the adverse event and SMT could be significant confounding factors. Greater care is also needed to distinguish between chiropractors and other health practitioners when reviewing the application of SMT and related adverse effects.
The author of this ‘replication study’ claims to have identified several errors in my 2007 review of adverse effects of spinal manipulation. Here is the abstract of my article:
Objective: To identify adverse effects of spinal manipulation.
Design: Systematic review of papers published since 2001.
Setting: Six electronic databases.
Main outcome measures: Reports of adverse effects published between January 2001 and June 2006. There were no restrictions according to language of publication or research design of the reports.
Results: The searches identified 32 case reports, four case series, two prospective series, three case-control studies and three surveys. In case reports or case series, more than 200 patients were suspected to have been seriously harmed. The most common serious adverse effects were due to vertebral artery dissections. The two prospective reports suggested that relatively mild adverse effects occur in 30% to 61% of all patients. The case-control studies suggested a causal relationship between spinal manipulation and the adverse effect. The survey data indicated that even serious adverse effects are rarely reported in the medical literature.
Conclusions: Spinal manipulation, particularly when performed on the upper spine, is frequently associated with mild to moderate adverse effects. It can also result in serious complications such as vertebral artery dissection followed by stroke. Currently, the incidence of such events is not known. In the interest of patient safety we should reconsider our policy towards the routine use of spinal manipulation.
In my view, there are several things that are strange here:
- Tuchin published his paper 5 years after mine.
- He did not publish it in the same journal as my original, but in an obscure chiro journal that hardly any non-chiropractor would ever read.
- Tuchin never contacted me and never alerted me to his publication.
- The journal that Tuchin chose was not Medline-listed in 2012; consequently, I never got to know about the Tuchin article in a timely fashion. (Therefore, I did never respond to it.)
- A ‘replication study’ is a study that repeats the methodology of a previous study.
- Tuchin’s paper is therefore NOT a replication study. Firstly, mine was a review and not a study. Secondly, and crucially, Tuchin never repeated my methodology but used an entirely different one.
But arguably, these points are trivial. They should not distract from the fact that I might have made mistakes. So, let’s look at the substance of Tuchin’s claim, namely that I made errors or omissions in my review.
As to ‘omissions’, one could argue that a review such as mine will always have to omit some details in order to generate a concise summary. The only way to not omit any details is to re-publish all the primary papers in one large volume. Yet, this can hardly be the purpose of a systematic review.
As to the ‘errors’, it seems that the ages and sex of three patients were wrong (I have not checked this against the primary publications but, for the moment, I believe Tuchin). This is, of course, lamentable and – even though I have no idea whether the errors happened at the data extraction phase, during the typing, the revising, or the publishing of the paper – it is entirely my responsibility. I also seem to have mistaken a non-chiropractor for a chiropractor. This too is regrettable but, as the review was about spinal manipulation and not about chiropractic, the error is perhaps not so grave.
Be that as it may, these errors are unquestionably not good, and I can only apologise for them. If Tuchin had dealt with them in the usual way – by publishing in a timely fashion a ‘letter to the editor’ of the JRSM – I could have easily corrected them for everyone to see.
But I think there is a more important point to be made here:
Tuchin concludes his paper stating that it is unwise to make conclusions regarding causality from any case study or multiple case studies. The number of errors or omissions in the 2007 Ernst paper significantly limit any reported conclusions. I believe that both sentences are unjustified. The safety of any intervention in routine use has to be examined on the basis of published case studies. This is particularly true for chiropractic where no post-marketing surveillance similar to that for drugs exists.
The conclusions based on such evidence can, of course, never be firm, but they provide valuable signals that can prompt more rigorous investigations in the interest of patient safety. In view of such considerations, my own conclusions in my 2007 paper were, I think, correct and are NOT invalidated by my relatively trivial mistakes: spinal manipulation, particularly when performed on the upper spine, has repeatedly been associated with serious adverse events. Currently the incidence of such events is unknown. Adherence to informed consent, which currently seems less than rigorous, should therefore be mandatory to all therapists using this treatment. Considering that spinal manipulation is used mostly for self-limiting conditions and that its effectiveness is not well established, we should adopt a cautious attitude towards using it in routine health care.
And my conclusions in the abstract have now, I believe, become established wisdom. They are thus even less in jeopardy through my calamitous lapsus or Tuchin’s ‘replication study’: Spinal manipulation, particularly when performed on the upper spine, is frequently associated with mild to moderate adverse effects. It can also result in serious complications such as vertebral artery dissection followed by stroke. Currently, the incidence of such events is not known. In the interest of patient safety we should reconsider our policy towards the routine use of spinal manipulation.
Deep venous thrombosis (DVT) is usually a blood clot in a deep vein of a leg. It is a potentially life-threatening condition, because the clot can detach itself and end up in the lungs thus causing a pulmonary embolism which can be fatal. A DVT therefore is a medical emergency which is typically managed by immobilising the patient and putting him/her on anticoagulants.
Yet, homeopaths seem to have discovered another approach. Indian homeopaths just published a case report of a DVT in an old patient totally cured exclusively by the non-invasive method of treatment with micro doses of potentized homeopathic drugs selected on the basis of the totality of symptoms and individualization of the case. The authors concluded that, since this report is based on a single case of recovery, results of more such cases are warranted to strengthen the outcome of the present study. 
The patient was advised by his doctor to have surgery which he refused. Instead, he consulted a homeopath who treated him homoeopathically. No conventional treatments were given. The patient recovered, yet his recovery is almost certainly unrelated to the homeopathics he received. Spontaneous recovery after DVT is not uncommon, and it is almost certain that it is this what the case report describes.
It is simply not plausible, nor is there evidence that homeopathy can alter the natural history of a DVT. This means that what the Indian homeopaths have described in their paper is nothing less than a case of gross negligence. Had the patient died of a pulmonary embolism due to an untreated DVT, it could have put them behind bars.
While it is, of course, most laudable that homeopaths have taken to publishing even their most serious errors, it would be more reassuring, if they developed some sort of insight into their mistakes. Instead, they seem naively confident and stupidly ignorant of the danger they pose to the public: homeopathy can play significant therapeutic roles in very serious diseases like DVT, provided the drugs are needs to be carefully selected on the basis of i) individualization of cases, ii) the totality of symptoms and personalized data, and iii) taking into consideration the pathogenicity level and proper diagnosis of the disease. Further, homeopathy may also be safely used in patients with conventional drug allergy (antibiotics) or other physical conditions preventing intake of conventional medicines.
My conclusion and recommendation: stay away from homeopaths, folks!