vaccination
Germany seems to have a significant problem with anti-vaxxers. Today, only 68% of the population has had a COVID vaccination. In the UK and France, these figures are 72% and 75% respectively.
How come?
This study investigated the willingness to vaccinate of parents of minors and people without children who are minors. The investigation was based on a random sample of Germans (telephone survey, n = 2,014, collected between 12 November and 10 December 2020). The evaluation is primarily based on the sub-sample of people with minors in the household (n = 461).
Parents of minors consistently show a lower willingness to be vaccinated with a COVID-19 vaccine than respondents without minors (54.1% vs 71.1%). Fathers show a stronger willingness to be vaccinated than mothers. Furthermore, men are more willing to get their own child vaccinated with a COVID-19 vaccine than are women.
The authors concluded that among parents and especially mothers, a considerable misrepresentation of vaccination risks and frequent beliefs in vaccination conspiracy theories can be observed. Clear and easily understandable information on the effects and side effects of vaccination with a COVID-19 vaccine by relevant institutions and physicians is recommended.
And what has this to do with so-called alternative medicine (SCAM) and homeopathy?
In the results section of the paper, the authors report interesting additional findings (my translation):
In the total sample, a significantly higher willingness to vaccinate is associated with the rejection of “alternative healing methods”. There is also a significant correlation between the attitude towards homeopathy and one’s own willingness to vaccinate: if homeopathy is supported, the willingness to vaccinate is lower. This correlation between the attitude towards homeopathy and willingness to vaccinate is also evident in the sub-sample of parents. Among parents, it is again women who significantly more often have a positive attitude towards homeopathy than men, who more often do not think anything of it.
The authors also report that the parents were asked: “If a vaccine against the coronavirus is approved in Germany, would you get vaccinated?” CERTAINLY NOT was the answer of:
- 41% of homeopathy fans
- 10% of people who thought nothing at all about homeopathy
- 15% of participants who were not fully convinced by homeopathy
Yes, Germany seems to have a problem with the anti-vaccination brigade but it seems that at the heart of it is a problem with a homeopathy cult.
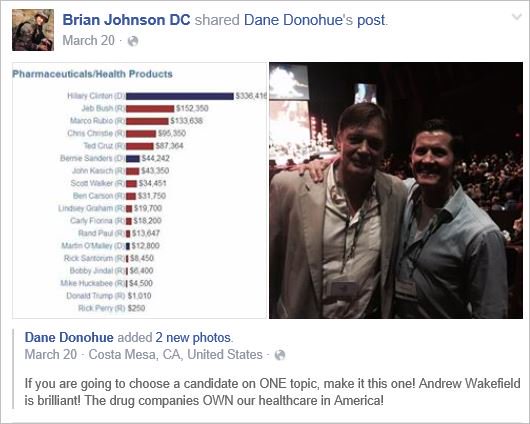
This article from AP News caught my attention. Here it is (I haven’t changed a word):
The flashy postcard, covered with images of syringes, beckoned people to attend Vax-Con ’21 to learn “the uncensored truth” about COVID-19 vaccines.
Participants traveled from around the country to a Wisconsin Dells resort for a sold-out convention that was, in fact, a sea of misinformation and conspiracy theories about vaccines and the pandemic. The featured speaker was the anti-vaccine activist who appeared in the 2020 movie “Plandemic,” which pushed false COVID-19 stories into the mainstream. One session after another discussed bogus claims about the health dangers of mask wearing and vaccines.
The convention was organized by members of a profession that has become a major purveyor of vaccine misinformation during the pandemic: chiropractors.
At a time when the surgeon general says misinformation has become an urgent threat to public health, an investigation by The Associated Press found a vocal and influential group of chiropractors has been capitalizing on the pandemic by sowing fear and mistrust of vaccines.
They have touted their supplements as alternatives to vaccines, written doctor’s notes to allow patients to get out of mask and immunization mandates, donated large sums of money to anti-vaccine organizations and sold anti-vaccine ads on Facebook and Instagram, the AP discovered. One chiropractor gave thousands of dollars to a Super PAC that hosted an anti-vaccine, pro-Donald Trump rally near the U.S. Capitol on Jan. 6.
They have also been the leading force behind anti-vaccine events like the one in Wisconsin, where hundreds of chiropractors from across the U.S. shelled out $299 or more to attend. The AP found chiropractors were allowed to earn continuing education credits to maintain their licenses in at least 10 states.
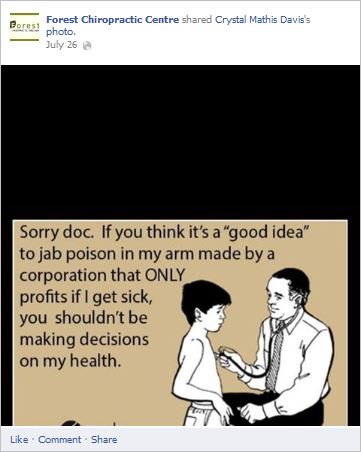
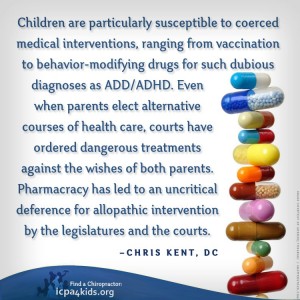
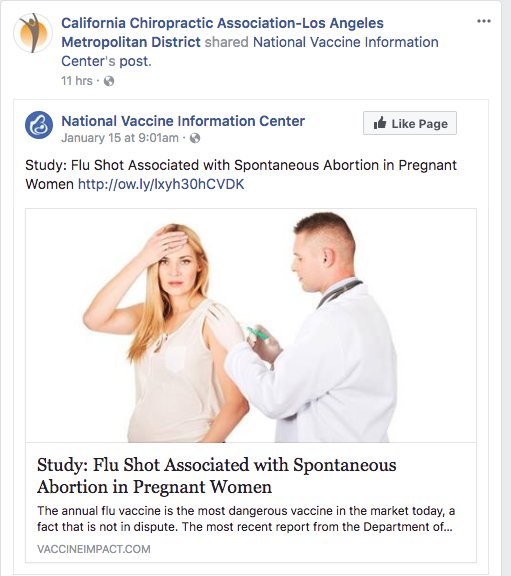
On this blog, I have often discussed that chiropractors tend to be anti-vax. It all goes back to their founding father, DD Palmer, who famously wrote:
- Vaccination and inoculation are pathological; chiropractic is physiological,
- and who in 1894, published his views on smallpox vaccination: ‘…the monstrous delusion … fastened on us by the medical profession, enforced by the state boards, and supported by the mass of unthinking people …’
- and who stated in 1896 that keeping tissue healthy is therefore the best prevention against infections; and this is best achieved by magnetic healing.
But that’s long ago! We are not like that anymore! … say the chiros of today.
Do you believe them?
If so, you might want to read this article by Jann Bellamy. Or alternatively, just look at some of my finds from the Internet:

The purpose of this survey was to quantify and describe the clinical practice beliefs and behaviors associated with US chiropractors. A 10% random sample of US chiropractors (n = 8975) was selected from all 50 state regulatory board lists and invited to participate in a survey. The survey consisted of a 7-item questionnaire; 6 items were associated with chiropractic ideological and practice characteristics and 1 item was related to the self-identified role of chiropractic in the healthcare system which was utilized as the dependent variable to identify chiropractic subgroups. Multinomial logistic regression with predictive margins was used to analyze which responses to the 6 ideology and practice characteristic items were predictive of chiropractic subgroups.
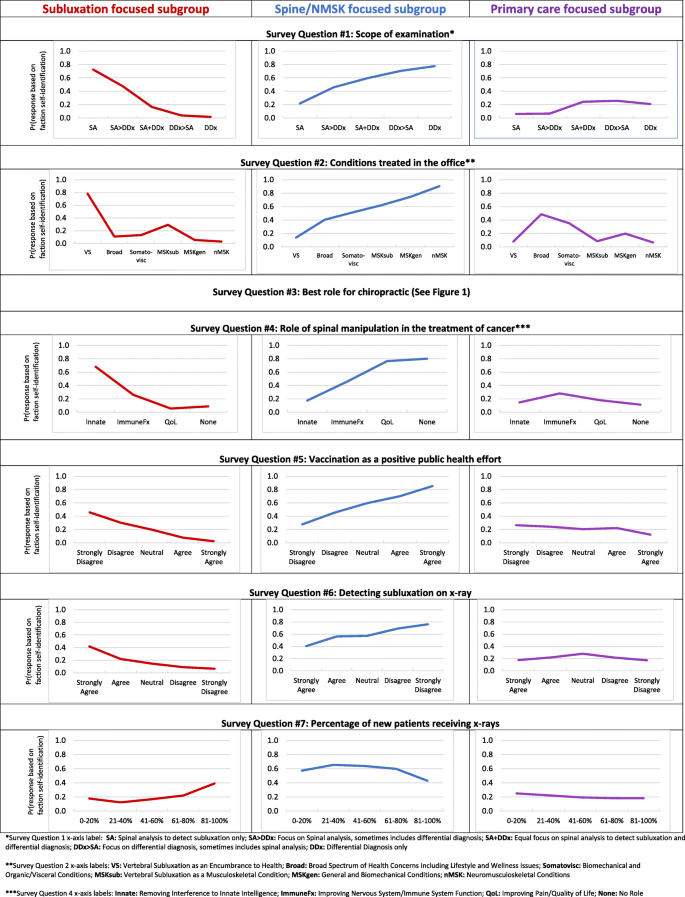
The survey instrument used in this study was developed by the authors and modeled after similar chiropractic identity analyses. The survey instrument included a total of 7 items intended to elicit divergent ideologies and practice behaviors. The figure below is a copy of the survey instrument.

A total of 3538 responses were collected (39.4% response rate). Respondents self-identified into three distinct subgroups based on the perceived role of the chiropractic profession in the greater healthcare system:
- 57% were spine/neuromusculoskeletal focused;
- 22% were primary care focused;
- 21% were vertebral subluxation focused.
Patterns of responses to the 6 ideologies and practice characteristic items were substantially different across the three professional subgroups.
The authors concluded that respondents self-identified into one of three distinct intra-professional subgroups. These subgroups can be differentiated along themes related to clinical practice beliefs and behaviors.
Here are the results in more detail as sated by the authors:
Regarding scope of examination (survey question 1), respondents reporting the scope of their clinical examination to only include spinal analysis for the assessment of vertebral subluxation had a 70% probability of belonging to the subluxation focused subgroup, a 20% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup. Conversely, respondents who reported the scope of their clinical examination only includes a differential diagnosis had a 0% probability of belonging to the vertebral subluxation focused subgroup, an 80% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup.
Concerning conditions treated (survey question 2), respondents who reported predominantly treating vertebral subluxation as an encumbrance to health had an 80% probability of belonging to the vertebral subluxation focused subgroup, a 10% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup. In contrast, respondents reporting predominantly treating neuromusculoskeletal conditions had a 0% probability of belonging to the vertebral subluxation focused subgroup, a 90% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup.
Regarding the role of spinal manipulation for those with cancer (survey question 4), respondents reporting the role of spinal manipulation for those with cancer is to remove interference to innate intelligence had a 70% probability of belonging to the vertebral subluxation focused subgroup, a 20% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup. Respondents reporting there is no role of spinal manipulation in those with cancer also had a 10% probability of belonging to the subluxation focused subgroup, an 80% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup.
Regarding vaccination (survey question 5), respondents who strongly disagreed that vaccinations have had a positive effect on global public health had a 50% probability of belonging to the vertebral subluxation focused subgroup, an approximately 25% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and an approximately 25% probability of belonging to the primary care focused subgroup. In contrast, respondents who strongly agreed that vaccinations have had a positive effect on global public health had a 0% probability of belonging to the vertebral subluxation focused subgroup, a 90% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup.
Concerning the detection of vertebral subluxation on x-ray (survey question 6), respondents who strongly agreed that x-ray is helpful in detecting vertebral subluxations had a 40% probability of belonging to the vertebral subluxation focused subgroup, a 40% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup. Respondents who strongly disagreed that x-ray is helpful in detecting vertebral subluxations had a near 0% probability of belonging to the vertebral subluxation focused subgroup, an 80% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and slightly below a 20% probability of belonging to the primary care focused subgroup.
Regarding use of x-rays for new patients (survey question 7), respondents who reported prescribing x-rays for 0–20% of new patients had a 20% probability of belonging to the vertebral subluxation focused subgroup, a 60% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup. Respondents reporting prescribing x-rays for 81–100% of new patients had a 40% probability of belonging to the vertebral subluxation focused subgroup, a 40% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup.
END OF QUOTE
While I am not sure that the division into the 3 subgroups is valid and suspect that there must be a substantial overlap between them, I must admit that the paper is rich in fascinating information. Generally speaking, I find all subgroups somewhat mysterious and would ask them the following questions:
Subgroup 1: why did you not study medicine or physiotherapy?
Subgroup 2: does it not bother you that your education and training are woefully insufficient for primary care?
Subgroup 3: is it not time to abandon the obsolete nonsense of your guru, the old charlatan DD Palmer?
They say, one has to try everything at least once – except line-dancing and incest. So, when I was invited to co-organize a petition, I considered it and thought: WHY NOT?
Here is the text (as translated by myself) of our petition to the German Medical Association:
Dear President Dr Reinhardt,
Dear Ms Lundershausen,
Mrs Held,
Dear Ms Johna,
We, the undersigned doctors, would like to draw your attention to the insistence of individual state medical associations on preserving “homeopathy” as a component of continuing medical education. We hope that you, by virtue of your office, will ensure a nationwide regulation so that this form of sham treatment [1], as has already happened in other European countries, can no longer call itself part of medicine.
We justify our request by the following facts:
- After the landmark vote in Bremen in September 2019 to remove “homeopathy” from the medical training regulations, 10 other state medical associations have so far followed Bremen’s example. For reasons of credibility and transparency, it would be desirable if the main features of the training content taught were not coordinated locally in the future, but centrally and uniformly across the country so that there is no “training tourism”. Because changes to a state’s own regulations of postgraduate training are only binding for the examination committee of the respective state, this does not affect national regulations but is reduced to only a symbolic character without sufficient effects on the portfolio of medical education nationwide.
- Medicine always works through the combination of a specifically effective part and non-specific placebo effects. By insisting on a pseudo-medical methodology – as is “homeopathy” represents in our opinion – patients are deprived of the specific effective part and often unnecessarily deprived of therapy appropriate to the indication. Tragically, it happens again and again that the “therapeutic window of opportunity” for an appropriate therapy is missed, tumors can grow to inoperable size, etc.
- Due to the insistence of individual state medical associations on the “homeopathic doctrine of healing” as part of the medical profession, we are increasingly exposed to the blanket accusation that, by tolerating this doctrine, we are supporting and promoting ways of thinking and world views that are detached from science. This is a dangerous situation, which in times of a pandemic manifests itself in misguided aggression reflected not just in vaccination skepticism and vaccination refusal, but also in unacceptable personal attacks and assaults on vaccinating colleagues in private practice.
Responsible:
Dr. med. Dent. Hans-Werner Bertelsen
Prof. Dr. med. Edzard Ernst
George A. Rausche
You can sign the petition here:
Prior research has generated inconsistent results regarding vaccination rates among patients using so-called alternative medicine (SCAM). Given that SCAM includes a wide range of therapies – about 400 different treatments have been counted – variable vaccination patterns may occur within consultations with different types of SCAM practitioners.
A recent analysis aimed to evaluate differences between categories of SCAM regarding vaccination behavior among US adults.
Data from the 2017 National Health Interview Survey (NHIS; n = 26,742; response rate 80.7%) were used. Prevalences of flu vaccination, consultations with SCAM practitioners in the past 12 months, and their potential interactions were examined. 42.7% of participants had received the flu vaccination in the past 12 months, 32.4% had seen one or more SCAM practitioners. Users of any type of SCAM were as likely as non-users to have received a flu vaccination (44.8% users versus 41.7% non-users; p = 0,862; adjusted odds ratio [AOR] = 1.01, 95% confidence interval [CI] = 0.95–1.07).
Regarding specific SCAM types,
- individuals consulting with naturopaths (p < 0.001; AOR = 0.67, 95 %CI = 0.54–0.82),
- homeopaths (p < 0.001; AOR = 0.55; 95 %CI = 0.44–0.69)
- chiropractors (p = 0.016; AOR = 0.9, 95 %CI = 0.83–0.98)
were less likely to be vaccinated. Other SCAMs showed no significant association with flu vaccination behavior. Independent predictors for a flu shot were prior diabetes, cancer, current asthma, kidney disease, overweight and current pregnancy. As well, higher educational level, age, ethnicity, health insurance coverage, and having seen a general physician or medical specialist in the past 12 months were also associated with a higher vaccination rate.
The authors concluded that SCAM users were equally likely to receive an influenza vaccination compared with non-users. Different SCAM therapies showed varied associations with vaccination behavior. Further analyses may be needed to distinguish influencing factors among patients’ vaccination behavior.
This survey confirms what we have discussed repeatedly on this blog (see, for instance here, here, here, here, and here). The reason why consumers who consult naturopaths, homeopaths, or chiropractors get vaccinated less regularly is presumably that these practitioners tend to advise against vaccinations. And why do they do that?
- Naturopaths claim that vaccines are toxic and their therapeutic options protect against infections.
- Homeopaths claim that vaccines are toxic and their therapeutic options protect against infections.
- Chiropractors claim that vaccines are toxic and their therapeutic options protect against infections.
Do these ‘therapeutic options’ – detox, nosodes, spinal manipulation – have anything in common?
Yes, they are bogus!
Conclusion:
Many naturopaths, homeopaths, and chiropractors seem to be a risk to public health.
By guest blogger Ken McLeod
RICHARD MICHAEL NILSSON is the owner of Colloidal Minerals Australia Pty Ltd, ACN 003 484 955, of Wyongah New South Wales (NSW), Australia. On August 13 he was convicted in the Wyong Court, after pleading guilty to offences including intimidation with intent to cause fear of physical or mental harm.
Nilsson is a prolific antivaxxer, deluging unlucky politicians, journalists, health officials, etc with emails containing misinformation about vaccines and warning of the dire consequences to come to anyone involved in vaccination programs. He has been known to harass and threaten. Usually recipients have better things to do than engage with a crank, but he has been known to go too far.
As the Sydney Daily Telegraph reported on 14 August 2021: “Anti-vaccine activist Richard Nilsson pleads guilty to sending death threats.”
“A Central Coast anti-vaccine campaigner who sent death threats to The Sunday Telegraph journalist Jane Hansen has pleaded guilty to the charge of using intimidation to unlawfully influence a person.
“Richard Nilsson, 66, from Wyongah, sent an email to Ms Hansen’s work email address on the evening of February 27.
“The subject of the email was “WHEN IS A MURDER WARRANTED? YOURS, YES?”
The contents of the email read: ‘I am proposing that your murder might well be a celebration of not life but death! And what a celebrated and glorious one at that!
‘I know ten thousand that would do it, but of course it only needs one and you will never know until it is too late!
‘I expect you might meet your maker, maybe in the near future … the sooner the better, yes?’
“Ms Hansen has reported widely on vaccination since 2013 when The Sunday Telegraph launched the No Jab No Play campaign, and more recently has reported on the vaccine rollout for Covid-19.
“On February 27, the evening the email was sent, Sky News re-ran a documentary made by Ms Hansen called Big Shots, which looked at anti-vaccine activity in relation to the pandemic and the vaccine rollout.
“Mr Nilsson followed up his email with another with the subject line: “WHEN IS SLUT NOT A SLUT AND IS A SELECTIVE SLUT STILL A SLUT?” before launching into a barrage of abuse.
“Mr Nilsson, who runs a business selling colloidal silver, faced Wyong Court on August 11 and pleaded guilty to a charge of use intimidation/violence to unlawfully influence a person.
“He received an 18-month Community Corrections Order to be of good behaviour.
“Ms Hansen said threats to journalists who write on the subject of vaccination were not unusual but Mr Nilsson’s emails were unsettling in their violence.
‘All journalists get abused on occasion, especially on the currently highly emotive topic of vaccination, and mostly it is best ignored but this email was next level and no one should have to put up with such vile abuse,’ she said.
“Mr Nilsson is well known by politicians, who have also received numerous emails from him suggesting all manner of conspiracies, including that Covid vaccination is a mass depopulation exercise.”
Nilsson appeared before His Honour Ian Guy in case number 2021/00159728, R V Richard Michael Nilsson. He was convicted of stalking or intimidation with intent to cause fear of physical or mental harm, an offence under section 13 of the Crimes (Domestic and Personal Violence) Act 2007 (NSW). This attracts a maximum penalty of 5 years imprisonment and/or $5,500. He could also have been convicted of using a carriage service to menace, harass or cause offence, an offence under section 474.17 of the Criminal Code Act 1995 (Commonwealth of Australia). That carries a maximum penalty of 3 years imprisonment.
He was sentenced to a Community Corrections Order requiring him to be of good behaviour.
A rational person would have thought themselves lucky that they had avoided years of a high-fibre low-calorie diet of porridge and baked beans, but we are not dealing with a rational person here.
Hardly was the ink dry on the Court file, than on the 15th, two days after he was found guilty, Nilsson pounded his foam-flecked keyboard and sent another rant in an email to 130 people and organisations, including politicians, Skeptics groups, a Radiation Oncologist, government departments, doctors, political parties, people in the horse-racing industry, scientists, journalists, lobby groups including climate and conservation organisations, mental health groups, the National Security Hotline, and a coal mining company.
It reads: “Subject: FW: The Hidden Victims of the Covid Vaccine and why I included you all in this email…
“When will it be that enough lives have been ruined and enough have been murdered? And when will the maiming and the killing end?
“My hope is that some of you here own up and confess (I know who among you are in this group and I suspect in time you will all pay a heavy price for your crimes and transgressions), while others it is incumbent upon you to inform all those you purport to represent that the maiming and killing that has transpired and of course is inevitably and scheduled to transpire will continue until such time we say: f_ ck you!
“I know, and some of you know too, who the traitors are. Scott Morrison is just one and Greg Hunt is another and of course Jane Halton, Brendan Murphy and Paul Kelly are other worthless humans and are included and we know they are just tools – plasticised and fake as they are.
“I have an incomplete list of those who need to answer for their crimes and it does not include all I have included in this email.
“Add a Mr Skerrit. His evilness is seen in his face and in his utterings and communications and his connection with Jane Halton and the WHO and the so-called, Australian Health (sickness proliferation) Dep’t and Event 201 should not be lost on anyone with brain cells that still operate and are able to coordinate.
“Wake the f_ _k up!”
All emphases and redactions above are as in Nilsson’s email. Scott Morrison is the Prime Minister, Greg Hunt the Commonwealth Minister for Health, Brendan Murphy is a former Chief Medical Officer (CMO) of Australia and now Secretary of the Department of Health. Paul Kelly is the current Chief Medical Officer, the “Mr Skerrit” he refers to is Adjunct Professor John Skerritt, Deputy Secretary, Health Products Regulation Group, Therapeutics Goods Administration. “Jane Halton” is a former Secretary of the Commonwealth Dept of Health, now Council Member of the Australian Strategic Policy Institute.
The “Event 201” that Nilsson refers to was a tabletop exercise conducted in October 2019 by the Johns Hopkins Center for Health Security (CHS), the World Economic Forum and the Bill and Melinda Gates Foundation in New York City. According to the CHS, “®he exercise illustrated areas where public/private partnerships will be necessary during the response to a severe pandemic in order to diminish large-scale economic and societal consequences”.
Event 201 simulated the effects of a fictional coronavirus originating in bats but passing to humans via pigs. Claims that Event 201 was a rehearsal for the COVID-19 pandemic have been debunked by fact-checking outlets such as USA Today and FullFact, but facts have never matter to antivax conspiracy theorists and other assorted cranks. All emergency response authorities and health bureaucracies conduct exercises to identify threats and to develop and improve response plans. There was nothing unusual in “Event 201” except in the fevered imaginations of nutters and fruitloops.
Does Nilsson, with no qualifications whatsoever, really think that he knows more about emergency response and immunology than those distinguished experts, and all the scientists researching Covid19 and vaccines? How does 20 minutes reading email conspiracy theories trump PhDs, professorships and Nobel Prizes? How conceited does someone have to be to imagine that? Where is the boundary between conceit and dementia? So does accusing honourable people of ‘crimes and transgressions,’ ‘maiming and killing,’ being ‘traitors,’ are evil tools, ‘who need to answer for their crimes’ constitute the good behaviour that the Court imposed? And coming within hours of the Court hearing?
Watch this space.
It has been reported that an Australian naturopath would refuse entry to her business to anyone who has received a COVID-19 vaccine in the past two weeks. In her original Facebook post, Ms. Holland said that vaccinated people would have to wait a minimum of two weeks after vaccination before attending her clinic due to “the shedding of spike proteins” caused by “these experimental treatments”.
Christine Pope, who is on the Australian Traditional Medicine Society (ATMS) board of directors, said she believed the views shared by the Warrnambool naturopath were part of the alternative medicine sector’s “fringe” and didn’t represent the industry. “We’re always very careful to tell our practitioners about posting appropriately and within their scope of practice,” Ms. Pope said. “These sort of comments to me look like they’re outside their scope of practice. We do a lot of training about making sure that you’re posting appropriately within your scope of practice and about things about which you are qualified in. As an association supporting natural medicine practitioners, it’s not really our job to promote or comment on the vaccination program – we’re not public health experts … and this is really outside my scope of practice. But from a public health perspective (vaccination) is the best option we’ve got.”
Sharon Holland, who runs a clinic in Warrnambool, cited on Facebook a number of discredited medical professionals who have become figureheads of the anti-vax and COVID conspiracy movements, including Judy Mikovits, Robert Malone, Peter McCullogh, and J Bart Classen. “Often de-bunked and fact-checked (by whom) can mean silenced,” Ms. Holland wrote. “We still have free speech available to some extent. This is a very emotive and divisive subject so my post was bound to ‘ruffle feathers’.”
The ATMS says its accredited practitioners need to “stay within their scope of practice” and avoid posting about vaccines they haven’t studied. Ms. Pope urged people to lodge a complaint about bogus health claims through the ATMS website or the healthcare complaint commissioner in the appropriate state.
___________________________
This course of events begs several questions. In my view, the most important are:
- Is Sharon Holland an exception, or are many/most naturopaths of her opinion?
- Instructing practitioners about “posting appropriately and within their scope of practice” sounds fine but might miss the point entirely. What really matters are the messages ATMS members orally convey to their patients. Is there any evidence on this issue?
- Surely, the anti-vax sentiments of naturopaths must originate from their education. Is there any evidence as to what they are taught about the subject?
- Is the ATMS going to take action against Ms. Holland and other members who endanger the public with their anti-vax stance?
Prof Harald Walach has had a few rough weeks. First, he published his paper suggesting that Covid vaccinations do more harm than good which was subsequently retracted as flawed, if not fraudulent. Next, he published a paper showing that children are put in danger when wearing face masks suggesting that “decision-makers weigh the hard evidence produced by these experimental measurements accordingly, which suggest that children should not be forced to wear face masks.” Now, the journal put out the following announcement about it:
The Research Letter, “Experimental Assessment of Carbon Dioxide Content in Inhaled Air With or Without Face Masks in Healthy Children: A Randomized Clinical Trial,” by Harald Walach, PhD, and colleagues published online in JAMA Pediatrics on June 30, 2021,1 is hereby retracted.
Following publication, numerous scientific issues were raised regarding the study methodology, including concerns about the applicability of the device used for assessment of carbon dioxide levels in this study setting, and whether the measurements obtained accurately represented carbon dioxide content in inhaled air, as well as issues related to the validity of the study conclusions. In their invited responses to these and other concerns, the authors did not provide sufficiently convincing evidence to resolve these issues, as determined by editorial evaluation and additional scientific review. Given fundamental concerns about the study methodology, uncertainty regarding the validity of the findings and conclusions, and the potential public health implications, the editors have retracted this Research Letter.
To make things even worse, Walach’s University fired him because of his fraudulent anti-vax research. Poznan University of Medical Sciences tweeted on 6 July:
We wish to emphasize that the claims included in dr Harald Walach’s recent article in @Vaccines_MDPI do not represent the position of @PUMS_tweets . We find that the article lacked scientific diligence and proper methodology. Dr. Walach’s affiliation with PUMS was now terminated. Throughout the pandemic PUMS has actively promoted vaccination programs, offering scientific expertise in the media, broadcasting seminars, and reported on progress of the vaccination program. We consider vaccinations as the paramount tool in the global fight against the pandemic. We consider vaccinations as the paramount tool in the global fight against the #pandemic. Over 85% of our own academic community has already been vaccinated with support and encouragement from the University.
As I said, this is truly unlucky …
.. or perhaps not?
Come to think of it, it is lucky when pseudo-science and fraud are called out. It means that the self-cleaning mechanisms of science are working and we are protected from the harm done by charlatans.
I recently discussed the incredible paper by Walach et al. To remind you, here is its abstract again:
COVID-19 vaccines have had expedited reviews without sufficient safety data. We wanted to compare risks and benefits.
Method: We calculated the number needed to vaccinate (NNTV) from a large Israeli field study to prevent one death. We accessed the Adverse Drug Reactions (ADR) database of the European Medicines Agency and of the Dutch National Register (lareb.nl) to extract the number of cases reporting severe side effects and the number of cases
with fatal side effects.
Result: The NNTV is between 200–700 to prevent one case of COVID-19 for the mRNA vaccine marketed by Pfizer, while the NNTV to prevent one death is between 9000 and 50,000 (95% confidence interval), with 16,000 as a point estimate. The number of cases experiencing adverse reactions has been reported to be 700 per 100,000 vaccinations. Currently, we see 16 serious side effects per 100,000 vaccinations, and the number of fatal side effects is at 4.11/100,000 vaccinations. For three deaths prevented by vaccination we have to accept two inflicted by vaccination.
Conclusions: This lack of clear benefit should cause governments to rethink their vaccination policy.
In my post, I pointed out that the analysis was deeply flawed and its conclusion ridiculous. Many other observers agreed, and several editorial board members of the journal, Vaccines, that unbelievably had published this junk resigned. Yesterday, the journal reacted by retracting the paper. Here is their statement:
The journal retracts the article, The Safety of COVID-19 Vaccinations—We Should Rethink the Policy.
Serious concerns were brought to the attention of the publisher regarding misinterpretation of data, leading to incorrect and distorted conclusions.
The article was evaluated by the Editor-in-Chief with the support of several Editorial Board Members. They found that the article contained several errors that fundamentally affect the interpretation of the findings.
These include, but are not limited to:
The data from the Lareb report (https://www.lareb.nl/coronameldingen) in The Netherlands were used to calculate the number of severe and fatal side effects per 100,000 vaccinations. Unfortunately, in the manuscript by Harald Walach et al. these data were incorrectly interpreted which led to erroneous conclusions. The data was presented as being causally related to adverse events by the authors. This is inaccurate. In The Netherlands, healthcare professionals and patients are invited to report suspicions of adverse events that may be associated with vaccination. For this type of reporting a causal relation between the event and the vaccine is not needed, therefore a reported event that occurred after vaccination is not necessarily attributable to vaccination. Thus, reporting of a death following vaccination does not imply that this is a vaccine-related event. There are several other inaccuracies in the paper by Harald Walach et al. one of which is that fatal cases were certified by medical specialists. It should be known that even this false claim does not imply causation, which the authors imply. Further, the authors have called the events ‘effects’ and ‘reactions’ when this is not established, and until causality is established they are ‘events’ that may or may not be caused by exposure to a vaccine. It does not matter what statistics one may apply, this is incorrect and misleading.
The authors were asked to respond to the claims, but were not able to do so satisfactorily. The authors were notified of the retraction and did not agree.
Two questions still remain to be answered:
- Were Walach et al just incompetent or did they wilfully try to mislead us?
- How much nonsense is Walach allowed to publish before he is finally stopped?
Prof Harald Walach is well-known to regular readers of this blog (see, for instance, here, here, and here). Those who are aware of his work will know that he is not an expert in infectious diseases, epidemiology, virology, or vaccinations. This did not stop him to publish an analysis that questions the safety and rationale of the current COVID-19 vaccination programs. Here is the abstract:
COVID-19 vaccines have had expedited reviews without sufficient safety data. We wanted to compare risks and benefits.
Method: We calculated the number needed to vaccinate (NNTV) from a large Israeli field study to prevent one death. We accessed the Adverse Drug Reactions (ADR) database of the European Medicines Agency and of the Dutch National Register (lareb.nl) to extract the number of cases reporting severe side effects and the number of cases
with fatal side effects.
Result: The NNTV is between 200–700 to prevent one case of COVID-19 for the mRNA vaccine marketed by Pfizer, while the NNTV to prevent one death is between 9000 and 50,000 (95% confidence interval), with 16,000 as a point estimate. The number of cases experiencing adverse reactions has been reported to be 700 per 100,000 vaccinations. Currently, we see 16 serious side effects per 100,000 vaccinations, and the number of fatal side effects is at 4.11/100,000 vaccinations. For three deaths prevented by vaccination we have to accept two inflicted by vaccination.
Conclusions: This lack of clear benefit should cause governments to rethink their vaccination policy.
I hesitate to comment because some could think that I have a personal grudge, as Walach propagated lies about me. And crucially, like he, I am not a vaccination expert. Yet, I feel I ought to point out that the data that form the basis of Walach’s calculations should not be used in this way for at least two reasons.
- Death after vaccination does not mean that this event was caused by the vaccine. For example, if someone had a fatal accident after vaccination, it would count as a vaccine incident according to Walach’s calculation.
- Vaccine effectiveness cannot be measured by calculating how many people must receive a vaccine to prevent one case of COVID-19 vaccination. Since vaccines have a protective effect on the community, this would be an outright miscalculation. The more people who receive a vaccine, the fewer people need to receive it to prevent a single case. This situation is the exact opposite of what Walach assumes in his paper.
Conclusion: amongst all his previous nonsense, Walach’s new publication stands out, I feel, as the most stupid and the most dangerous. The mistakes seem too obvious to not be deliberate. Let’s hope the journal editor in chief (who failed miserably when publishing this idiocy) has the wisdom to retract it swiftly. One of its editors already tweeted:
I have resigned from the Editorial Board of
following the publication of this article. It is grossly negligent and I can’t believe it passed peer-review. I hope it will be retracted.
And another ed-board member had this to say:
