risk
Nausea and vomiting are common symptoms of patients with advanced cancer. While there is some evidence for acupuncture point stimulation in the treatment of these symptoms for patients having anticancer treatment, there is little for when they are not related to such treatment.
This study aimed to determine whether acupressure at the pericardium 6 sites can help treat nausea and vomiting suffered by palliative care patients with advanced cancer. The researchers conducted a double-blind randomized controlled trial-active versus placebo acupressure wristbands. In-patients with advanced cancer in two specialist palliative care units who fitted either or both of the following criteria were approached: nausea that was at least of moderate severity; vomiting daily on average for the prior 3 days.
A total of 57 patients were randomized to have either active or placebo acupressure wristbands. There was no difference in any of the outcome measures between the two groups:
- change from the baseline number of vomits;
- Visual Analogue Scale for ‘did acupressure wristbands help you to feel better?’;
- the total number of doses of antiemetic medication;
- the need for escalation of antiemetics.
The authors concluded that, in contrast to a previously published feasibility study, active acupressure wristbands were no better than placebo for specialist palliative care in patients with advanced cancer and nausea and vomiting.
When the research into acupuncture for nausea and vomiting began some 20 years ago, the evidence turned out to be encouraging. Later, as the studies became more and more rigorous, many trials failed to confirm the initial findings. Today, the totality of the evidence is far less convincing than it seemed years ago.
This is a phenomenon that can be observed not just in acupuncture research but in many types of treatment:
- Initially, over-enthusiastic researchers become victims of their own optimism.
- These investigators are less into testing hypotheses than into confirming their own wishful thinking.
- Thus, several positive trials emerge.
- These, however, turn out to be methodologically flawed.
- Eventually, the subject might be picked up by real scientists who truly test hypotheses.
- More and more negative studies thus emerge.
- Depending on how many flawed studies were initially published and how critical the authors of systematic reviews are, it can take years until the totality of the evidence depicts the true picture which discloses the initial findings as false-positive.
The message is, I think, clear: poor quality studies have the potential to mislead us for many years. Eventually, however, the self-cleansing ability of science should generate the truth about the value of any treatment. In other words:
poor-quality science is not just useless, it causes long-term harm
and
critical thinking prevents harm
Alan Gaby, the assistant editor of the journal Integr Med has written an interesting commentary about widespread fraud in natural health products research. Here is an excerpt of his article:
During the past 49 years, I have reviewed and analyzed more than 50 000 papers from the biomedical literature, most of which were related to the field of nutritional medicine. Doing this work has given me some understanding of how to assess the reliability of a study. Over the past 10 to 15 years, an uncomfortably large and growing number of published papers related to my area of expertise have left me wondering whether the research was fabricated; that is, whether people were writing papers about research that had not actually been conducted. If the studies were not actually conducted, the publishing of this research is an affront to all who value integrity in science, and it has the potential to harm practitioners and patients who rely on its findings.
The studies that have raised concerns have come primarily from Iran and to a lesser extent from Egypt, China, India, Japan, and a few other countries. Characteristics of these concerning studies typically include one or more of the following:
- The study comes from an investigator or research group that has published an enormous number of randomized clinical trials in a relatively short period of time.
- The number of participants in the trial is unusually large, when considering the resources that appear to be available to the researchers.
- The recruitment period for the trial is unusually short.
- The paper is submitted to a journal unusually rapidly after the study is completed, or in some cases before it would have been possible to have completed the trial.
- A randomized double-blind trial is conducted before there is any preliminary evidence of efficacy in humans (such as case reports or uncontrolled trials). Because double-blind trials are expensive to conduct, such trials are generally reserved for treatments for which there is some evidence of efficacy.
- The magnitude of the reported improvement is much larger than is typically seen in trials using just one or two nutrients.
- No funding source is listed or the study is listed as self-funded. This is of particular concern when the sample size or study design suggests that the study was expensive.
- The design of the study raises ethical issues, such as participants not being permitted to use treatments that are known to be effective.
- One or more baseline characteristics of the study group appear to be implausible.
- The research was conducted by a student as part of a graduate school thesis, and the magnitude of the project seems to have been beyond the capabilities and resources of a student.
__________________________________
What Gaby alludes to is a problem indeed. I have previously posted about the Chinese aspect of this story. What Gaby does not mention is the fact that even many studies of so-called alternative medicine (SCAM) which seem to be not overtly fraudulent are nevertheless highly suspect. I am referring to trials that are fatally flawed and/or studies that draw unwarranted conclusions. These are, of course, the types of studies that are the main target of this blog. Because they are so numerous, I feel that the damage they do is much bigger than that of the more overtly fraudulent papers.
I came across an interesting case report recently published in an Austrian magazine. Here is my translation for non-German speakers:
A 42-year-old woman from Vienna has suffered from endometriosis since the age of 13. But it was only 8 years later that she found out what made the first two days of her menstruation so unbearable. She was not allowed to take painkillers to help herself during all that time. Her parents listened to medical “gurus” who distrusted conventional medicine.
“I grew up in a household where almost all illnesses were treated with homeopathy,” she wrote on Twitter. That’s exactly what became the IT expert’s undoing. In a recent interview, she looked back bitterly: “All infections and illnesses were treated with Bach flower remedies or homeopathics. Only in case of accidents or broken bones did my parents drive me to the hospital.” Her father suffered from an auto-immune disease. Because conventional medicine could not help him, he tried alternative approaches. “My parents slowly drifted more and more into this scene. At some point, they stopped listening to ‘normal’ doctors. It went downhill from there.”
As a girl, the Viennese had little chance of standing up to her parents’ “whisperers,” as she calls their esoteric advice. “When I got my period, I was in the worst pain. I fainted every month, even falling off my chair when I did it, once even at school. I vomited until I was so exhausted that I fell asleep.”
She begged her family to finally be allowed to consult a gynecologist. But he didn’t take the teenager seriously at the time and simply wanted to prescribe her the pill without a thorough examination. “I then went to my parents’ homeopathic ‘pill pusher’, who gave me homeopathics against my complaints. I wasn’t allowed to take painkillers because they ‘damage the liver’.” The guru persuaded the young woman that her health problems were her fault. “He said I just didn’t accept myself as a woman and that’s why I was in pain. I thought for a long time that I was just not strong and good enough.”
It wasn’t until she was already in her early 20s that her then-boyfriend took her to a gynecologist who finally took her condition seriously. “The ultrasound showed that I had quite a few cysts in my abdomen.” The diagnosis was also finally certain: she was now officially suffering from endometriosis. She was given the right medicine, and most of the endometriotic growths regressed. But a cyst had wrapped itself tightly around her right ovary, damaging it irrevocably over the years. It had died. “Homeopathy cost me my ovary,” the Viennese woman laments.
The fact that she nevertheless was able to become the mother of two children is thanks to her other ovary, which fortunately remained intact. But the feeling of having been treated wrongly, or not treated at all, for such a long time makes her angry. “I don’t blame my parents today. They have apologized and found their own way out of the gurus’ world of thought and out of the scene,” she emphasizes. “But I blame the people who pretend to be able to cure the majority of all diseases with homeopathy. Yet most of the time they can’t even find the right diagnosis and just give patients some stuff that has no side effects.” She now calls for an end to homeopathy.
_________________________
How many times have I said it?
His remedy might be risk-free, but the homeopath certainly isn’t!
Prof. Fabricio Benedetti is one of the world’s leading experts in the study of placebo effects. I have mentioned his excellent work before, for instance, here where he cautioned that quackery has today one more weapon on its side, which is paradoxically represented by the hard science–supported placebo mechanisms. Now he has expressed his concerns even more clearly in an article entitled “Alternative and natural medicine quackery is on the rise. Here’s why the placebo effect is part of the problem”. Here are a few excerpts from this excellent paper:
For several decades now, many scientists, including me, have been working hard to reveal the full power and scope of the placebo effect — the amazing ability of a simple sugar pill or other non-pharmaceutical “fake intervention” to improve someone’s quality of life. This research has been crucial to giving scientific credibility to a powerful psychological effect. But the advances of science have also backfired, spawning an alternative industry that preys on the vulnerable…
All this means that some alternative medicines can indeed have positive outcomes for patients, though not necessarily through the mechanisms that the therapy’s inventors supposed, but rather through a placebo effect. This holds true for treatments ranging from strange talismans to acupuncture — studies have shown that pain relief is about the same for patients receiving true acupuncture with needles, for example, as for those receiving sham acupuncture with trick needles.
The scientific advances in understanding placebo are fascinating. But one unfortunate outcome of all this work is that profit-seeking companies and individuals now have a new weapon: It is no longer necessary to demonstrate the effectiveness of their proposed therapies; it is enough to assert that these work because of the placebo effect. I receive myriad eccentric proposals for new therapies, ranging from talismans and concoctions to mascots and weird rituals. Their inventors claim that these are capable of inducing substantial health benefits and often seek my endorsement. These proposals have stepped up sharply in recent years. Sadly, the science of the placebo effect is fueling this new breed of pseudoscience…
So, if a salesperson says: “This concoction (or ritual or talisman) will reduce your pain,” it is not necessarily a lie, as the placebo effect may indeed stimulate pain-relieving circuits in the brain. But anyone could truthfully use these words, within limits.
These marketers often overstate the size of the possible response, claim to provide a “cure” rather than pain relief or incorrectly suggest that only their own expensive products will have this effect. Even worse, they may present the products as an alternative to more effective traditional medications for serious conditions such as cancer. In other words, they prey on the vulnerable by making undeliverable promises, purportedly backed by the science of placebo.
Even if taking a placebo can reduce symptoms such as pain, this isn’t always the best course of action. An apparently trivial pain may, for example, be the first sign of something far more serious. Treating the pain alone may prevent diagnosis by a physician or delay important medical treatments…
…Education, communication and honesty are the best friends of medical practice. Patients and health care professionals deserve to know what placebos can and cannot do.
The research and medical communities must be more transparent about the efficacy of many conventional pharmacological and nonpharmacological treatments, by acknowledging that some of them are useful whereas some others are not. Many over-the-counter products have doubtful efficacy, for example. Honesty will boost patients’ trust and confidence in medicine, which are the best antidotes to quackery.
BRAVO PROF BENEDETTI!
Almost 10 years ago, I posted this:
When I decided to become a doctor I, like most medical students, did so mainly to help suffering individuals. When I became a researcher, I felt more removed from this original ideal. Yet I told myself that, by conducting research, I might eventually contribute to a better health care of tomorrow. Helping suffering patients was still firmly on the agenda. But then I realised that my articles in peer-reviewed medical journals somehow missed an important target: in alternative medicine, one ought to speak not just to health care professionals but also to consumers and patients; after all, it is they who often make the therapeutic decisions in this area.
Once I had realised this, I started addressing the general public by writing for The Guardian and other newspapers, giving public lectures and publishing books for a lay audience, like TRICK OR TREATMENT…The more I did this sort of thing, the more I noticed how important this activity was. And when a friend offered to help me set up a blog, I did not hesitate for long.
So, the reason for my enthusiasm for this blog turns out to be the same as the one that enticed me to go into medicine in the first place. I do believe that it is helpful for consumers to know the truth about alternative medicine. Considering the thousands of sources of daily misinformation in this area, there is an urgent need for well-informed, critical information. By providing it, I am sure I can assist people to make better therapeutic decisions. In a way, I am back where I started all those years ago: hoping to help suffering patients in the most direct way my expertise allows.
Helping vulnerable patients often means warning them from dangerous charlatans, and this is precisely what I frequently try to do with this blog. But how successful are my endeavors?
More often than not, I have no idea and can only hope for the best. Sometimes I do get some feedback that is encouraging and motivates me to carry on. Rarely, however, do I witness immediate, tangible success. And this is why the recent story is so remarkable:
- On 6 June, an Australian acquaintance from the FRIENDS OF SCIENCE IN MEDICINE sent me some material about a planned lecture in the UK by someone promoting dangerous quackery.
- I looked into it and published a blog post about it a few hours later.
- A reader then suggested in the comments section of this post alerting the UK press to it.
- Another reader contacted THE TIMES, and I wrote to several other journalists.
- THE TIMES turned out to be interested in the story.
- They did some research and interviewed Michael Marshall from the GOOD THINKING SOCIETY (and myself).
- Today, THE TIMES published an article about the planned event.
- Finally, a kind person made the article available to those who don’t want to pay for it.
The whole thing amounts to superb teamwork, in my view. It shows how like-minded people who do not even all know each other can manage to achieve a respectable result with little more than goodwill and dedication.
A respectable result?
Of course, the optimal result would be to stop Barbara O’Neill’s UK lectures. Let’s hope this is what eventually will happen – and please let me know if you know more.
This article almost left me speechless:
The back-to-back waves of the COVID-19 pandemic have made a devastating impact globally. The conventional healthcare system is going through serious pressure as cases of the disease continue to spread and the numbers of hospitalizations are increasing every moment. It is becoming hard and challenging because the hospital resources are limited in number as compared with the rate of daily hospitalizations. There are significant shortages of patient care facilities and medical care providers, and on top of that, conventional healthcare systems do not have any proven treatments for COVID-19 patients. Experimental drugs like hydroxychloroquine, followed by remdesivir, ritonavir/lopinavir, and favipiravir are being administered under emergency use authorization (EUA). There is evidence that these experimental medications are causing adverse drug reactions, thus claiming the lives of the hospitalized COVID-19 patients. And those patients who survive the EUA medications and hospitalizations are left with iatrogenic immunosuppressive states leading to increased susceptibility towards secondary life-threatening infections like fungal diseases. In this scenario, complementary and alternative medical systems (CAMS) are providing commendable results with negligible adverse effects or iatrogenic issues in patients with COVID-19. There are several clinical cases recorded and published by various independent homoeopathic doctors and researchers worldwide. But unfortunately, because of a biased medical model and greed for monopolies, these effective treatment methods are not given equal opportunity as their conventional counterparts.
I think the best way to react to this nonsense might be to remind us what the only RCT of homeopathy for COVID showed.
This randomized, double-blind, two-armed, parallel, single-center, placebo-controlled study investigated the effectiveness and safety of the homeopathic medicine, Natrum muriaticum LM2, for mild cases of COVID-19.
Participants aged > 18 years, with influenza-like symptoms and a positive COVID test were recruited and randomized (1:1) into two groups that received different treatments during a period of at-home isolation. One group received the homeopathic medicine Natrum muriaticum, prepared with the second degree of the fifty-millesimal dynamization (LM2; Natrum muriaticum LM2), while the other group received a placebo.
The primary endpoint was time until recovery from COVID-19 influenza-like symptoms. Secondary measures included a survival analysis of the number and severity of COVID-19 symptoms (influenza-like symptoms plus anosmia and ageusia) from a symptom grading scale that was informed by the participant, hospital admissions, and adverse events. Kaplan-Meier curves were used to estimate time-to-event (survival) measures.
Data from 86 participants were analyzed (homeopathy, n = 42; placebo, n = 44). There was no difference in time to recovery between the two groups (homeopathy, n = 41; placebo, n = 41; P = 0.56), nor in a sub-group that had at least 5 moderate to severe influenza-like symptoms at the beginning of monitoring (homeopathy, n = 15; placebo, n = 17; P = 0.06). Secondary outcomes indicated that a 50% reduction in symptom score was achieved significantly earlier in the homeopathy group (homeopathy, n = 24; placebo, n = 25; P = 0.04), among the participants with a basal symptom score ≥ 5. Moreover, values of restricted mean survival time indicated that patients receiving homeopathy might have improved 0.9 days faster during the first five days of follow-up (P = 0.022). Hospitalization rates were 2.4% in the homeopathy group and 6.8% in the placebo group (P = 0.62). Participants reported 3 adverse events in the homeopathy group and 6 in the placebo group.
The authors concluded that the results showed that Natrum muriaticum LM2 was safe to use for COVID-19, but there was no statistically significant difference in the primary endpoints of Natrum muriaticum LM2 and placebo for mild COVID-19 cases.
Another relevant study compared the antibody response of homeopathic and conventional vaccines and placebo in young adults. A placebo-controlled, double-blind RCT was conducted where 150 university students who had received childhood vaccinations were assigned to diphtheria, pertussis, tetanus, mumps, measles homeopathic vaccine, placebo, or conventional diphtheria, pertussis, tetanus (Tdap) and mumps, measles, rubella (MMR) vaccines. The primary outcome was a ≥ two-fold increase in antibodies from baseline following vaccination as measured by ELISA. Participants, investigators, study coordinators, data blood drawers, laboratory technicians, and data analysts were all blinded.
None of the participants in either the homeopathic vaccine or the placebo group showed a ≥ two-fold response to any of the antigens. In contrast, of those vaccinated with Tdap, 68% (33/48) had a ≥ two-fold response to diphtheria, 83% (40/48) to pertussis toxoid, 88% (42/48) to tetanus, and 35% (17/48) of those vaccinated with MMR had a response to measles or mumps antigens (p < 0.001 for each comparison of conventional vaccine to homeopathic vaccine or to placebo). There was a significant increase in geometric mean titres of antibody from baseline for conventional vaccine antigens (p < 0.001 for each), but none for the response to homeopathic antigens or placebo.
The authors concluded that homeopathic vaccines do not evoke antibody responses and produce a response that is similar to placebo. In contrast, conventional vaccines provide a robust antibody response in the majority of those vaccinated.
To give ‘equal opportunity’ to implausible therapies would, in my view, not merely be wrong, it would be scandalously unethical. The role of homeopathy in the prophylaxis and symptomatic management of COVID-19 or other infections is very easily described; it is:
zero,
nil,
nothing,
null,
naught,
zilch.
Bee venom acupuncture (BVA) is a bizarre form of acupuncture where bee venom is applied via a bee sting or an injection into acupuncture points. The paper below starts with the sentence: “BVA is an effective treatment method for various diseases.” This clearly is not true. In fact, there is no convincing evidence that it is effective for any condition. In addition, it can cause serious harm, even life-threatening anaphylaxis.
With this review, Korean authors tried to estimate the incidence rate of anaphylaxis in response to BVA. 
The investigators searched eight databases (MEDLINE (Pubmed), EMBASE, Cochrane Central Register of Controlled, KISS, KMBASE, Koreamed, OASIS, and NDSL) and systematically reviewed the articles that met the inclusion/exclusion criteria.
Among 225 potentially relevant articles, 49 were selected for this study. The overall incidence rate of anaphylaxis in response to BVA was 0.045% (95% CI 0.028-0.062). Women (0.083%, 95% CI 0.010-0.157) showed a higher incidence rate than men (0.019%, 95% CI -0.018 to 0.055), while the incidence for patients who had a skin test conducted (0.041%, 95% CI 0.011-0.072) was not significantly different compared to that obtained for patients for which there was no information about a skin test (0.047%, 95% CI 0.026-0.067). The publication year affected the incidence rate: it was highest before 1999 (1.099%, 95% CI -1.043 to 3.241), lower between 2000 and 2009 (0.049%, 95% CI 0.025-0.073), and lowest between 2010 and 2021 (0.037% 95% CI 0.014-0.060).
The authors concluded that, in this study, we provide reference data about risk size and factors of BVA-related anaphylaxis, which is essentially required for BVA application in clinics.
I fail to understand why this review included only observational studies and RCTs. Why not case reports? We would need a proper post-marketing surveillance system to obtain reliable incidence figures. Yet, such a system does not exist. Therefore, the data generated by this paper are next to worthless.
All this article does, is confirm that anaphylactic reactions after BVA are a reality. As the treatment has not been proven to be effective for any condition, its risk/benefit balance turns out to be negative. In other words, we should therefore not use BVA.
I was made aware of an advertisement announcing that the ‘international health lecturer’, Barbara O’Neill, is soon (19-26 June) coming to the UK.
Who is Barbara O’Neill? I hear you ask.
Here is more interesting information about her:
The NSW Health Care Complaints Commission conducted an investigation into the professional conduct of Mrs Barbara O’Neill, an unregistered practitioner who provides services as a naturopath, nutritionist and health educator.
Complaints received by the Commission alleged that Mrs O’Neill makes dubious and dangerous health claims that are not evidence based or supported by mainstream medicine, regarding: infant nutrition; causes and treatment of cancer; antibiotics; and vaccinations. Some of the non-evidence based comments made in Mrs O’Neill’s publications include:
- raw goat’s milk is an appropriate substitute for breast milk in infant nutrition;
- cancer is a fungus that can be treated with bicarbonate soda and can be cured by following a program that includes the cancer conquering diet and sodium bicarbonate wraps for the body;
- pregnant women diagnosed with Strep B do not have to take antibiotics;
- there are no safe vaccines; vaccinations have caused an epidemic of ADHD, autism, epilepsy and cot death.
The investigation found that Mrs O’Neill has limited qualifications in the area of nutrition and dietetics, which she attained more than 10 years ago. Of particular concern to the Commission is that Mrs O’Neill is providing health advice beyond the limits of her training and experience. Mrs O’Neill considers herself qualified to provide health advice in highly complex and specialised areas such as cancer treatment, use of antibiotics for Strep B and immunisation, in circumstances where it is clear her knowledge is limited.
The investigation also found that Mrs O’Neill does not recognise that she is misleading vulnerable people (including mothers and cancer sufferers) by providing very selective information. The misinformation has real potential to have a detrimental effect on the health of individuals because Mrs O’Neill also discourages mainstream treatment for cancer, antibiotics and vaccinations.
The investigation determined that Mrs O’Neill breached the Code of Conduct for Unregistered Health Practitioners under Schedule 3 of the Public Health Regulation 2012 in respect of:
- Clause 3(1): a health practitioner must provide health services in a safe and ethical manner;
- Clause 5(1): a health practitioner must not hold himself or herself out as qualified, able or willing to cure cancer or other terminal illnesses;
- Clause 7(1): a health practitioner must not attempt to dissuade clients from seeking or continuing with treatment by a registered medical practitioner;
- Clause 12(1): a health practitioner must not engage in any form of misrepresentation in relation to the products or services he or she provides or as to his or her qualifications, training or professional affiliations;
- Clause 15: a health practitioner must maintain accurate, legible and contemporaneous clinical records for each client consultation.
The Commission is satisfied that Mrs O’Neill poses a risk to the health and safety of members of the public and therefore makes the following prohibition order:
- Mrs O’Neill is permanently prohibited from providing any health services, as defined in s4 Of the Health Care Complaints Act 1993, whether in a paid or voluntary capacity.
The Commission has determined to make its Statement of Decision publicly available under section 41B(3)(c) of the Health Care Complaints Act 1993 but has removed material which it considers to be confidential information.
The full Public Statement of Decision can be read here
____________________________
Barbara has clear and concise messages:
- Vaccinations have caused an epidemic of ADHD, autism, epilepsy and cot death.
- Cancer is a fungus that can be treated with bicarbonate soda.
Just what we needed in the UK!?
Or maybe not.
Yes, we did get used to being lied to by our PM. We are also slowly getting used to our NHS being vandalized by our Tory government. But that does not mean that we now should opt to cure cancer with baking soda.
Perhaps it would be better to use existing legislation (e.g. the cancer act) and stop this ‘international health lecturer’ in her tracks?
PS
In case you wonder who might organize such an event, it is this one:
Manna House Health Education & Wellness is a community interest company that works with people to improve their health. Manna House has been using natural health principles to help the body heal itself. It was established for the purpose of educating people in the principles and laws of healthful living.
Many systematic reviews have summarized the evidence on spinal manipulative therapy (SMT) for low back pain (LBP) in adults. Much less is known about the older population regarding the effects of SMT. This paper assessed the effects of SMT on pain and function in older adults with chronic LBP in an individual participant data (IPD) meta-analysis.
Electronic databases were searched from 2000 until June 2020; reference lists of eligible trials and related reviews were also searched. Randomized controlled trials (RCTs) were considered if they examined the effects of SMT in adults with chronic LBP compared to interventions recommended in international LBP guidelines. The authors of trials eligible for the IPD meta-analysis were contacted and invited to share data. Two review authors conducted a risk of bias assessment. Primary results were examined in a one-stage mixed model, and a two-stage analysis was conducted in order to confirm the findings. The main outcomes and measures were pain and functional status examined at 4, 13, 26, and 52 weeks.
A total of 10 studies were retrieved, including 786 individuals; 261 were between 65 and 91 years of age. There was moderate-quality evidence that SMT results in similar outcomes at 4 weeks (pain: mean difference [MD] – 2.56, 95% confidence interval [CI] – 5.78 to 0.66; functional status: standardized mean difference [SMD] – 0.18, 95% CI – 0.41 to 0.05). Second-stage and sensitivity analysis confirmed these findings.
The authors concluded that SMT provides similar outcomes to recommended interventions for pain and functional status in the older adult with chronic LBP. SMT should be considered a treatment for this patient population.
This is a fine analysis. Unfortunately, its results are less than fine. Its results confirm what I have been saying ad nauseam: we do not currently have a truly effective therapy for back pain, and most options are as good or as bad as the rest. This is most frustrating for everyone concerned, but it is certainly no reason to promote SMT as usually done by chiropractors or osteopaths.
The only logical solution, in my view, is to use those options that:
- are associated with the least risks,
- are the least expensive,
- are widely available.
However you twist and turn the existing evidence, the application of these criteria does not come up with chiropractic or osteopathy as an optimal solution. The best treatment is therapeutic exercise initially taught by a physiotherapist and subsequently performed as a long-term self-treatment by the patient at home.
Necrotizing infection (NI) of the breast associated with underlying malignancy is a rare phenomenon characterized by necrosis of breast parenchyma. It can cause a delay in diagnosis and even lead to sepsis. Researchers from the Aga Khan University Hospital in Karachi, PAK, present a case of a 42-year-old woman with NI of the right breast, while on homeopathic treatment for a right breast lump for six months. Tissue culture showed a polymicrobial infection and histopathology established the diagnosis of breast carcinoma. After treating the NI, her breast cancer was managed as per standard guidelines.
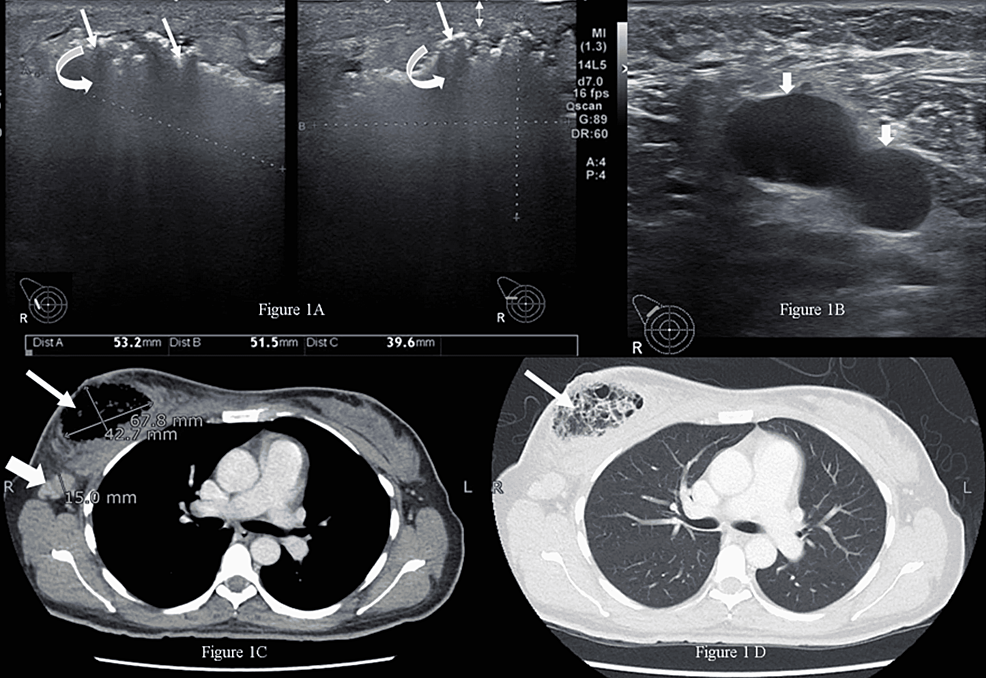
The married, nulliparous, diabetic, hypertensive patient was a non-smoker and presented to the emergency room with complaints of fever, severe pain, and foul-smelling bloody discharge from her right breast for two weeks. She had a history of a right breast lump for six months, for which she had been taking oral homeopathic remedies, the names of which were not recorded. On examination, she had a blood pressure of 132/76 mmHg, a pulse of 84 bpm, a temperature of 99 °F, and a respiratory rate of 14 breaths per minute. The right breast was tender and hard, with a 4 x 3-cm necrotic skin patch on the upper half with bleeding and a palpable right axillary lymph node. The rest of the examination was unremarkable.
The patient was advised to undergo a metastatic workup in the emergency room, which included a contrast-enhanced CT (CECT) of the chest, abdomen, and pelvis and a bone scan. The CT confirmed the presence of an air-filled cavity in the right breast with thin septations and enlarged right axillary lymph nodes; however, there was no enhancing mass to suggest neoplasm in either breast. The CT and bone scans were negative for metastasis. The presence of severely tender breast on clinical examination and air within the breast on ultrasound suggested the possibility of NI, which warranted an early surgical intervention to prevent impending sepsis.
Microscopic examination of the debrided tissue revealed an invasive breast carcinoma of no special type [invasive ductal carcinoma (IDC), NST grade III] along with extensive necrosis and dense acute and chronic inflammation. The right axillary node biopsy was positive for nodal metastasis, and the patient was staged as cT4N1MO. A tissue culture showed a few colonies of Staphylococcus aureus and Enterococcus species suggestive of NI. After a discussion at a multidisciplinary tumor board meeting, the patient underwent a right modified radical mastectomy. Her postoperative course was unremarkable.
____________________
I have said it often but I am afraid I need to say it again: the homeopathic remedy might be harmless, but that does not mean that homeopathy is not dangerous.