risk
Due to polypharmacy combined with the rising popularity of so-called alternative medicines (SCAM), oncology patients are at particular risk of drug-drug interactions (DDI) or herb-drug interactions (HDI). Caution is therefore indicated.
The aims of this study were to assess DDI and HDI in outpatients taking oral anticancer drugs.
All prescribed and non-prescribed medications, including SCAM, were prospectively collected by hospital pharmacists during a structured interview with the patient. DDI and HDI were analyzed using four interaction software programs: Thériaque®, Drugs.com®, Hédrine, and Memorial Sloan Kettering Cancer Center (MSKCC) database. All detected interactions were characterized by severity, risk, and action mechanism. The need for pharmaceutical intervention to modify drug use was determined on a case-by-case basis.
294 patients were included, with a mean age of 67 years. The median number of chronic drugs per patient was 8 [1-29] and 55% of patients used at least one SCAM. At least 0ne interaction was found for 267 patients (90.8%): 263 (89.4%) with DDI, 68 (23.1%) with HDI, and 64 (21.7%) with both DDI and HDI. Only 13% of the DDI were found in Thériaque® and Drugs.com® databases, and 125 (2.5%) were reported with a similar level of risk on both databases. 104 HDI were identified with only 9.5% of the interactions found in both databases. 103 pharmaceutical interventions were performed, involving 61 patients (20.7%).
The authors concluded that potentially clinically relevant drug interactions were frequently identified in this study, showing that several databases and structured screening are required to detect more interactions and optimize medication safety.
This figure of potential HDIs is high – much higher than in most previous studies. A possible explanation could be that the study was carried out in France where the use of herbal remedies is considerable. As some HDIs can cause serious problems for patients, my advice is to think twice about using herbal remedies while taking prescription drugs. I think this advice is sound regardless of whether someone is suffering from cancer or any other condition.
It has been reported by several outlets that a young woman is fighting for her life after a chiropractic adjustment went horribly wrong. Caitlin Jensen had only recently graduated from University. When she went for what was meant to be a simple chiropractic adjustment on June 16, she suffered four dissected arteries in her neck, this damage led to cardiac arrest, stroke and her being without a pulse for over 10 minutes, requiring resuscitation.
She was rushed to the Memorial Hospital in Savannah, Georgia, where she was operated on. She was then taken to the neuro ICU in a critical condition with a traumatic brain injury. Every day since she’s been fighting. Currently, she is conscious and able to respond to verbal commands by blinking her eyes, as well as wiggling the toes of her left foot. However, most of her body remains paralyzed.
Her mother Darlene has been posting updates about her daughter’s condition on Facebook. On Saturday Darlene shared the latest news on the condition of her daughter. “She gave her best effort to smile today, and it was the most beautiful thing I’ve ever seen,” Darlene said. “She is progressing with her movements on the left side – wiggling and flexing. She can’t lift her arm yet, or turn her head. Her right side is unchanged – still no movement. Her face doesn’t move very much yet, but she can open her eyes widely to show surprise, and the left corner of her mouth tries to smile. Adorable. Still working on the pneumonia. The antiplatelet therapy seems to be going OK. We don’t see any signs of internal bleeding and are praying that it stays that way.”

And the day before, Darlene posted: “Two weeks ago tonight we didn’t know if Caitlin would make it through the night,” Darlene said. “Dire and catastrophic are two of the words that we heard from our ICU team. We knew they didn’t casually throw around words like that. But – she is alive, and every day is a little better. The accomplishments are both small and monumental at the same time. Today, she gave us a thumbs up. We have been working on this, and she got it! She also nodded again today. It helps to see these things because it reassures us that she is working hard to stay with us and recover. Caitlin is strong, disciplined, and well practised in exercising her brain, and I truly believe that her science background and all of her time studying is going to help her in this long journey. “
Studies have found that traumatic cervical artery dissection is one of the leading causes of stroke in patients under the age of 45, and recent chiropractic neck manipulation is among factors that can be associated with risk of vertebral artery dissection.
Following the tragedy, Caitlin’s mother, Darlene, launched a GoFundMe and has raised more than US$20,000 (AU $29,334 or £16,512) for her ongoing medical expenses.
It is clear that these news reports lack important medical details. What is equally clear is the fact that most such cases are never reported in the medical literature and are thus available only in this fragmented form. The reason for this lamentable situation is obvious: there is no post-marketing surveillance system for chiropractic (such a safeguard would be bad for business, of course).
Consequently, chiropractors across the globe continue to be able to say that such reports are unreliable. The medical literature, they are keen to point out, holds only very few case studies of serious risks of chiropractic spinal manipulation. Hence they falsely claim on every possible occasion that their adjustments are safe. The end effect is that many consumers continue to wrongly assume that chiropractic manipulations might be worth a try.
Guest post by Ken McLeod
Believe it or not, there are practitioners of a health system with little or no evidence of efficacy and safety who are registered with the Australian Health Practitioner Registration Agency. That is, so-called Traditional Chinese Medicine, whose practitioners are registered alongside evidence-based practitioners such as doctors, nurses, pharmacists, and dentists.
Governments who framed the relevant legislation evidently hoped that registration would enable the public to have confidence that they would be treated with evidence-based medicine. Such confidence is misplaced, as has been shown in The Skeptic and elsewhere many times.
Here’s another example of the failure of the health practitioner registration system.
Jamie Lloyd Allan is registered with AHPRA with the Chinese Medical Registration Number CMR0002096457, with no endorsements. He practices at his clinic in eastern Sydney. He advertises at his website meridianremedies.com.au.
And some of his claims are deeply worrying. Allan claims that he uses “Chinese Herbal medicine & Acupuncture in conjunction with testing and removal of accumulated toxins and heavy metals, developing comprehensive individualised herbal antimicrobial and detoxification protocols.”
He claims that “toxins and heavy metals … enter our bodies, disrupt normal healthy cell behaviour, impair our immune system, often contribute and sometimes cause many different types of illnesses and health conditions.”
His claims are designed to generate unfounded worries in people, offering a smorgasbord of claims how he can help people learn [the words and spelling are his]:
• how mercury from common amalgam fillings can be passed from mother to child to grandchild and why preconception detoxification is important;
• how to assess a dentist to know your [sic] getting the best and safest care during amalgam removal;
• about mercury/autism connection, heavy metal accumulation and neurological diseases such as Alzheimer’s, Parkinson’s and Dementia;
• more about mercury, aluminium, cadmium and lead toxicity;
• how heavy metal accumulation acts as an antenna for electromagnetic radiation from devices such as wifi, cell phone, cordless phones, thus focusing the frequencies on the areas where the metals are stored, causing changes in the proteins and even DNA;
• the science behind electromagnetic radiation and how it affects human cells;
• Glyphosate toxicity, and how many of us have it and how it affects our health, and lots more.
Allan goes into the alleged toxicity of mercury amalgam fillings further at his blog. I should not have to say it, but his claims are baseless and have been debunked many times. The US Food and Drug Administration has said that existing evidence shows that dental amalgam is not harmful to the general population (tinyurl.com/589mbrr6). And as Scientific American said “Mercury and Autism: Enough Already! The science shows that they have nothing to do with each other and never have.” (tinyurl.com/mwwdxxak)
Allan also writes extensively on “EMF Sensitivity Wi-Fi and Cell Phone radiation – Heavy Metals and EMF Sensitivity and Autism” – he claims “Autism rates double every 5 years and the only thing that parallels that in our environment is the increase of man made Electro magnetic Radiation and fields largely in the high frequencies from cell phone Wi-Fi, smart meters and other Electro magnetic devices.’ This is unconscionable; scaring potential clients with this, while conveniently forgetting that correlation does not mean causation.
Allan also offers the following techniques as a “Detox for autism”:
• Sauna or heat therapy (far infrared is best) Cold shower straight after to close pores and wash of toxins
• Clay plasters, Clay on scars, then shower
• Ionic Foot Cleanses, Detox baths, Takara foot Pads, or raw white potato strapped on soles of feet
• Fibre + Enemas or colonics, slippery elm, keep bowls [sic] moving
• Liver gall bladder flush with lemon oil
• Exercise, dry skin brush
• Chi Machine for lymph drainage and movement to parasympathetic dominance
• Olive or other healthy oils for swish and spit
• Genetic, vitamin, mineral testing to guide your diet and supplements
• Western and Chinese Herbs to detox bowls [sic], liver, kidney, lymph
• Homeopathic drops & plenty of water orally
• Laser Energetic detox
• Ozonized bath, Epson salt bath
• Enema for detox reactions in kids
• Stronger detox agents DMPS, DMSA, EDTA can be used in case of high-level toxicity. For children, the use of the above mention techniques over DMPS, DMSA and EDTA is preferred first.
“Raw white potato strapped on soles of feet”!! Come on! This is lunacy. And enemas for children? And what qualifications does Allan hold to diagnose and administer these dangerous pharmaceuticals?
Luckily, Allan offers the perfect scanner to diagnose what’s wrong with you, the Oligoscan.
As described, “This a [sic] spectrographic-based test. Every element on the periodic table has its own unique absorption spectra, meaning that different elements absorb certain wavelengths of light, and reflect others. The spectra of lead will be different from that of mercury, or calcium, or any other element. The Oligoscan shines a laser on different points on the hand, and based off of [sic] which wavelengths of light are absorbed or reflected back, the levels of different metals and minerals in the cells of your hand can be determined. This is similar to how astronomers can analyze the wavelengths of light emitted by distant stars to determine their chemical make-up.
“The Oligoscan has the advantage of testing the levels of metals that are actually in your cells, not what you are able to excrete. It tests the heavy metal load of the tissues. This is important because heavy metals have a affinity [sic] for tissues and are often store [sic] there and not in the blood. It can also measure aluminium, which most other tests will miss. Oligoscan results tend to correlate with other accurate tests.”
A search of the TGA’s register of therapeutic goods did not find the Oligoscan listed.
Clearly, Allan is engaged in a process of scaring potential clients with misinformation, then offering diagnostic and treatment processes that are deceptive, ineffective and dangerous, and not listed with the TGA; for all of which he is not qualified.
COMPLAINT PROCESS
A complaint was sent to the NSW Health Care Complaints Commission describing the above issues. (In NSW and Queensland, complaints concerning health care practitioners, registered and unregistered, are lodged with the relevant State authorities, the HCCC and OHO respectively.) We added that “This should not be treated as merely a case of misleading advertising; Allan is clearly endangering the public, so I recommend a thorough audit of his practice, and when my allegations are found to be proven, suitable disciplinary action taken and entered on the AHPRA register.”
The HCCC responded saying “Following consultation with the Chinese Medicine Council of New South Wales, it was decided to refer this matter to the Australian Health Practitioner
Regulation Agency (AHPRA) as AHPRA is the designated agency to manage concerns about advertising. We did not identify any other issues that would require further action by the Commission.” (We approached the Chinese Medicine Council of NSW – their response is quoted in the sidebar.)
The HCCC continued: “The Commission obtained a written response from Mr Allan. In his response to the Commission, Mr Allan stated that he had no record of providing any care and treatment to you.
“Mr Allan acknowledged that his website may have created a misunderstanding about what actual treatments are offered at his clinic, and what was on his website for educational purposes only.
“Mr Allan noted that he has never owned an Oligoscan or used it at his clinic, he has therefore removed that information from his website.
“Mr Allan confirmed that he does not offer the techniques under the heading ‘detox for autism’ at his clinic, the information was for educational purposes only, and he has now removed this information from his website.
“Further, Mr Allan has confirmed that he has removed the information on his website about Glyphosate Toxicity, Toxicity of Mercury Amalgam fillings, Nutrition for Autism, and all avenues of receiving mercury toxicity.
“Mr Allan also stated that he has since edited the information on EMF Sensitivity Wi-Fi and Cell Phone radiation – Heavy Metals and EMF Sensitivity Autism, as well as editing the information contained on the home and about pages of his website.
“Mr Allan stated that he has left the resources section with all the raw studies, and some information contained in other sections, as he feels that they are of use for anybody wanting to learn more about this specialised area.”
So, in spite of the detailed evidence and a call for a thorough audit of his practice, this was treated as merely a case of misleading advertising. This is standard operating procedure; the regulatory authorities cannot get over the divide between advertising and clinical practice. This has been shown in the hundreds of complaints sent to regulators; misleading advertising of dangerous practices and misinformation is simply treated as an advertising issue. The regulators cannot accept that if a practitioner advertises a therapy then they are more than likely using those therapies and, when those therapies have been found to be ineffective, they are engaging in practice in their clinics that deserves more than the dismissive response we received.
The public deserve much better than that.
Note: All of the quotes above were from Allan’s website until he removed them. The relevant pages have, nonetheless, can be accessed via the WayBack Machine, and can be supplied if required.
The Chinese Medicine Council’s position
The Chinese Medical Council were referred to the issues in the main article and were asked the following questions:
• Is the advice and those therapies [offered by Allan] of any concern to the Council?
• Should the complaint to the NSW Health Care Complaints Commission have led to an audit of his practice and when the allegations are proven, should there have been disciplinary action?
A spokesperson for the Chinese Medicine Council of NSW replied: “The Chinese Medicine Council of NSW (the Council) works in collaboration with the NSW Health Care Complaints Commission (HCCC) to receive and manage complaints about registered practitioners in
NSW. Our paramount legal obligation is to protect the public. We deal with practitioners whose conduct, performance or health may represent a risk to the public or is not in the public interest.
“We do this by assessing complaints, promoting compliance with professional standards and delivering programs to ensure practitioners provide safe care to the public and their patients. We do not have the legal power to discipline a NSW practitioner or to deregister them.
“By law, the Council cannot provide information about an individual practitioner. Only information that is publicly available can be disclosed, such as information recorded on the national register of practitioners which is maintained by the Australian Health Practitioner Regulation Agency (AHPRA), or publication of the outcomes of NCAT [New South Wales Civil and Administrative Tribunal] proceedings.
“Changes to a registered health practitioner’s registration status, such as the imposition of conditions or suspension, are published on the AHPRA online public register.
“The Council will not be making any further public comments at this time.
So, the Chinese Medicine Council have taken no action to protect the public and made no real comment. At least they have promised “Only information that is publicly available can be disclosed”, a statement of breathless inanity.
*‘first published in the Australian Skeptic magazine of June 2022.
This multi-center, open-label, randomized controlled trial assessed the effects of anthroposophic treatments on toxicity related to intensive-phase chemotherapy treatment in children aged 1-18 with the primary outcome of the toxicity sum score. Secondary outcomes were chemotherapy-related toxicity, overall and event-free survival after 5 years in study patients.
The main sponsorship for the study was provided by: Helixor Heilmittel GmbH & Co. KG, Rosenfeld. Additional finacial support was provided by: WALA Heilmittel GmbH, Bad Boll/Eckwälden; Weleda AG, Schwäbisch Gmünd: Mahle Stiftung, Stuttgart; Software AG Stiftung, Darmstadt; Stiftung Helixor, Rosenfeld; and Injex Pharma AG, Berlin.
The intervention and control groups were both given standard chemotherapy according to malignancy & tumor type. The intervention arm was provided with anthroposophic supportive treatment (AST); given as anthroposophic base medication (AMP), as a base medication for all patients, and additional on-demand treatment tailored to the patient in the intervention groups. The control was given no AMP. The toxicity sum score (TSS) was assessed using NCI-CTC scales.
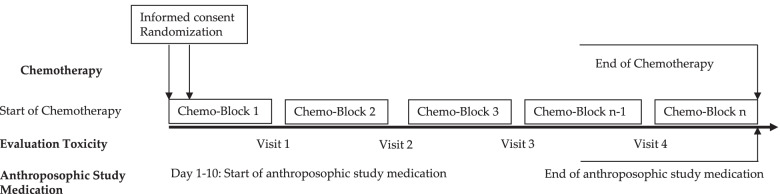
The AST consisted of base AMP including Helixor®, and on-demand supplementary AMP given as needed for symptoms. Administration of the AST intervention and chemotherapy protocol were tailored for each type of pediatric malignancy included in the trial. This included both the base and the on-demand AMP, which were administered based on acute symptoms during intensive chemotherapy. The intervention group started the AST between the day of randomization and day 10 of the first chemotherapy cycle.
Data of 288 patients could be analyzed. The analysis did not reveal any statistically significant differences between the AST and the control group for the primary endpoint or the toxicity measures (secondary endpoints). Furthermore, groups did not differ significantly in the five-year overall and event-free survival follow-up.
The authors concluded that their findings showed that AST was able to be safely administered in a clinical setting, although no beneficial effects of AST between group toxicity scores, overall or event-free survival were shown.
In their discussion section, the authors explain the findings more clearly: “In the long term follow up, the explorative analysis of the data available for the 5-year follow up found no indications that efficacy of chemotherapy was influenced by AST. For long-term toxicities there were also no indications of an influence of AST.”
Question: what do we call a treatment that has neither adverse nor beneficial effects?
Could it be
PLACEBO?
An epidemiological study from the US just published in the BMJ concluded that “the mortality gap in Republican voting counties compared with Democratic voting counties has grown over time, especially for white populations, and that gap began to widen after 2008.”
In a BMJ editorial, Steven Woolf comments on the study and provides further evidence on how politics influence health in the US. Here are his concluding two paragraphs:
Political influence on US mortality rates became overt during the covid-19 pandemic, when public health policies, controlled by states, were heavily influenced by party affiliation. Republican politicians, often seeking to appeal to President Trump and his supporters, challenged scientific evidence and opposed enforcement of vaccinations and safety measures such as masking. A macabre natural experiment occurred in 2021, a year marked by the convergence of vaccine availability and contagious variants that threatened unvaccinated populations: states led by governors who promoted vaccination and mandated pandemic control measures experienced much lower death rates than the “control” group, consisting of conservative states with lax policies and large unvaccinated populations. This behavior could explain why US mortality rates associated with covid-19 were so catastrophic, vastly exceeding losses in other high income countries.
Observers of health trends in the US should keep their eye on state governments, where tectonic shifts in policy are occurring. While gridlock in Washington, DC incapacitates the federal government, Republican leaders in dozens of state capitols are passing laws to undermine health and safety regulations, ban abortion, limit LGBT+ rights, and implement more conservative policies on voting, school curriculums, and climate policy. To understand the implications for population health, researchers must break with custom; although scientific literature has traditionally avoided discussing politics, the growing influence of partisan affiliation on policies affecting health makes this covariate an increasingly important subject of study.
_____________________
What has this to do with so-called alternative medicine (SCAM)?
Not a lot.
Except, of course, that Trump has been quite sympathetic to both quackery and quacks (see, for instance, here and here). Moreover, the embarrassing Dr. Oz, America’s charlatan-in-chief, is now a Republican candidate for the US senate. And the creation of the NHI office for alternative medicine, currently called NCCIH, was the idea of the Republican senator, Tom Harkin.
I think we get the drift: on the US political level, SCAM seems to be a right-wing thing.
Am I claiming that SCAM is the cause of the higher mortality in Republican counties?
No.
Do I feel that both are related to irresponsible attitudes towards healthcare issues?
Yes.
It seems that no ancient treatment is daft enough for some researchers of so-called alternative medicine (SCAM) to not pick it up. Even bloodletting is back, it seems!
The aim of this study was to investigate the effects of therapeutic phlebotomy on ambulatory blood pressure in patients with grade 1 hypertension. In this randomized-controlled intervention study, patients with unmedicated hypertension grade 1 were randomized into an intervention group (phlebotomy group; 500 mL bloodletting at baseline and after 6 weeks) and a control group (waiting list) and followed up for 8 weeks. The primary endpoint was the 24-h ambulatory mean arterial pressure between the intervention and control groups after 8 weeks. Secondary outcome parameters included ambulatory/resting systolic/diastolic blood pressure, heart rate, and selected laboratory parameters (e.g., hemoglobin, hematocrit, erythrocytes, and ferritin). Resting systolic/diastolic blood pressure/heart rate and blood count were also assessed at 6 weeks before the second phlebotomy to ensure safety. A per-protocol analysis was performed.
Fifty-three hypertension participants (56.7 ± 10.5 years) were included in the analysis (n = 25 intervention group, n = 28 control group). The ambulatory measured mean arterial pressure decreased by -1.12 ± 5.16 mmHg in the intervention group and increased by 0.43 ± 3.82 mmHg in the control group (between-group difference: -1.55 ± 4.46, p = 0.22). Hemoglobin, hematocrit, erythrocytes, and ferritin showed more pronounced reductions in the intervention group in comparison with the control group, with significant between-group differences. Subgroup analysis showed trends regarding the effects on different groups classified by serum ferritin concentration, body mass index, age, and sex. Two adverse events (AEs) (anemia and dizziness) occurred in association with the phlebotomy, but no serious AEs.
The authors concluded that therapeutic phlebotomy resulted in only minimal reductions of 24-h ambulatory blood pressure measurement values in patients with unmedicated grade 1 hypertension. Further high-quality clinical studies are warranted, as this finding contradicts the results of other studies.
This paper requires a few short comments:
- The effect on blood pressure was not ‘minimal’, as the authors pretend, it was non-existent (i.e. not significant and due to chance only).
- This lack of effect had to be expected considering human physiology.
- The fact that hemoglobin, hematocrit, erythrocytes, and ferritin all change after bloodletting is equally expected.
- Mild adverse effects are also no surprise.
- What is a surprise, however, that such a trial was ever conducted and passed by an ethics committee. Any medic who has not slept through his/her cardiovascular physiology lectures could have predicted the results quite accurately. And running a trial where the result is well-known before the study has started can hardly be called ethical.
In India, the homeopathic remedy, Arsenicum Album 30C (prepared from arsenic trioxide) is widely prescribed and publicly supplied to adults and children for preventing COVID infections. Inorganic arsenic, known as the “king of poisons” is a highly toxic substance with the potential to cause acute as well as chronic injury to multiple organ systems, mainly skin, lung, liver, and kidneys.
Indian researchers present three cases of acute liver injury, leading to the death of one patient with underlying non-alcoholic steatohepatitis (NASH) cirrhosis, after consumption of the homeopathic remedy AA30 for COVID-19 prevention.
Case one
A 70-year-old man with compensated non-alcoholic steatohepatitis (NASH)-related cirrhosis and diabetes mellitus consumed the homeopathic IB AA30 as prescribed for 12 weeks prior to the onset of symptoms. He presented with jaundice and abdominal distension within four weeks after the onset of loss of appetite and well-being. The patient was not on any other hepatotoxic agents, over-the-counter medications, or herbal and dietary supplements. Investigations revealed the presence of conjugated hyperbilirubinemia, ascites, and abnormal coagulation, suggestive of acute-on-chronic liver failure (ACLF). Further investigations to identify known causes of acute deterioration of underlying cirrhosis were performed, including a transjugular liver biopsy. All competing causes for acute liver injury were meticulously ruled out. These included infections-tests for immunoglobulin M (IgM) for viral hepatitis A and E; hepatitis B surface antigen and IgM antibody to hepatitis B core antigen; nucleic acid tests via polymerase chain reaction for hepatitis C; IgM for herpes zoster and herpes simplex, cytomegalovirus, parvovirus, Epstein-Barr virus. Complete auto-antibody testing for autoimmune hepatitis (AIH) was negative. The Roussel Uclaf Causality Assessment (RUCAM) demonstrated “probable” (score 7) drug-induced liver injury (DILI) and simplified AIH score was less than 5, revealing the cause of acute liver injury leading to ACLF as the homeopathic remedy, AA30. The liver biopsy revealed multiacinar hepatocyte necrosis, lymphocytic, neutrophilic, and eosinophilic inflammation in the absence of interface hepatitis, which were predominantly portal-based in the background of cirrhosis, suggestive of DILI. Analysis of drugs consumed could not be performed in view of inadequate sample availability. The patient and family consented to arsenic analysis in nail and hair samples which revealed extremely high levels of the heavy metal, supportive of arsenic toxicity and associated liver injury in the patient. Evaluation of hair and hair samples of two family members (below detection limits, method detection limit being 0.1 mg/kg), staying in the same household did not reveal levels signifying cluster arsenic poisoning from water or soil sources. The patient succumbed to complications related to ACLF, nine months after the initial diagnosis.
Case two
A 68-year-old male with systemic hypertension controlled on telmisartan who ingested AA30 as prescribed for four weeks prior to the onset of symptoms. There was no associated jaundice or cholestatic symptoms, but liver tests revealed acute hepatitis with an elevation of liver enzymes. The patient was not on any other hepatotoxic agents, over-the-counter medications, or herbal and dietary supplements. Further investigations did not reveal the presence of underlying chronic liver disease or portal hypertension. All competing causes for acute liver injury were meticulously ruled out similar to the extensive workup that was done in case one. The RUCAM demonstrated “probable” (score 8) DILI and simplified AIH score was less than 5, revealing the cause of acute non-icteric hepatitis as the homeopathic remedy, AA30. The liver biopsy revealed perivenular hepatocyte necrosis, with predominantly portal-based mixed cellular inflammation consisting of plasma cells, eosinophils, lymphocytes, and scattered neutrophils. Additionally, ballooning of hepatocytes was marked with scattered rosettes and moderate interphase hepatitis in the presence of mild portal and sinusoidal fibrosis suggestive of DILI. Acute hepatitis resolved after drug withdrawal and finite course of steroids within three months, without any recurrence on follow-up.
Case three
A 48-year-old overweight woman consumed homeopathic AA30 pills as COVID-19 preventive for one week prior to the onset of her symptoms of cholestatic jaundice. Prior to the development of jaundice, she had nonspecific gastrointestinal symptoms such as nausea and progressive loss of appetite. Liver tests revealed conjugated hyperbilirubinemia with highly raised liver enzymes. The patient was not on any other hepatotoxic prescription drugs, over-the-counter medications, or herbal and dietary supplements. Further investigations did not reveal the presence of underlying chronic liver disease or portal hypertension. All competing causes for acute liver injury were meticulously ruled out similar to the extensive workup that was done in case one. The RUCAM demonstrated “probable” (score 7) DILI and simplified AIH score was less than 5, revealing the cause of acute cholestatic hepatitis as the homeopathic remedy, AA30. The liver biopsy revealed spotty, focal hepatocyte necrosis, with predominantly portal-based neutrophilic and eosinophil-rich inflammation, moderate steatosis, and mild interface hepatitis with underlying mild perisinusoidal fibrosis, suggestive of DILI. The acute cholestatic hepatitis resolved after drug withdrawal and a finite course of steroids within six months, without any recurrence on follow-up.
The chemical analysis and toxicology (inductively coupled optical emission spectroscopy and triple-quadrupole gas chromatography with tandem mass spectroscopy method) on two sets of AA30 samples retrieved from case three revealed D-mannose, melezitose, and arsenic respectively, demonstrating batch-to-batch variation due to poor manufacturing practices.
The authors draw the following conclusions: Health regulatory authorities, physicians, general and patient population must be aware of the potential harms associated with the large-scale promotion of untested, alternative medical systems during a medical emergency so as to prevent an “epidemic” of avoidable DILI within the ongoing pandemic. Even though ultra-diluted homeopathic remedies, found ineffective as shown in large-scale meta-analysis, are considered safe for use due to the absence of any active compound beyond 12C dilution. Nonetheless, poor manufacturing practices, use of concentrated tincture formulations, and adulteration and contamination of homeopathic remedies can still pose considerable toxicity in predisposed persons. From a scientific and evidence-based standpoint, it is imperative that the general population and at-risk persons understand that vaccination, and not untested, misleading IBs, remains the best available armamentarium against COVID-19 which helps in fighting back the pandemic.
If you have been following my blog for a while, you probably know the answer to this question. A recent article published in JAMA re-emphasizes it in an exemplary fashion:
According to National Health and Nutrition Examination Survey data, 52% of surveyed US adults reported using at least 1 dietary supplement in the prior 30 days and 31% reported using a multivitamin-mineral supplement. The most commonly cited reason for using supplements is for overall health and wellness and to fill nutrient gaps in the diet. Cardiovascular disease and cancer are the 2 leading causes of death and combined account for approximately half of all deaths in the US annually. Inflammation and oxidative stress have been shown to have a role in both cardiovascular disease and cancer, and dietary supplements may have anti-inflammatory and antioxidative effects.
Objective To update its 2014 recommendation, the US Preventive Services Task Force (USPSTF) commissioned a review of the evidence on the efficacy of supplementation with single nutrients, functionally related nutrient pairs, or multivitamins for reducing the risk of cardiovascular disease, cancer, and mortality in the general adult population, as well as the harms of supplementation.
Population Community-dwelling, nonpregnant adults.
Evidence Assessment The USPSTF concludes with moderate certainty that the harms of beta carotene supplementation outweigh the benefits for the prevention of cardiovascular disease or cancer. The USPSTF also concludes with moderate certainty that there is no net benefit of supplementation with vitamin E for the prevention of cardiovascular disease or cancer. The USPSTF concludes that the evidence is insufficient to determine the balance of benefits and harms of supplementation with multivitamins for the prevention of cardiovascular disease or cancer. Evidence is lacking and the balance of benefits and harms cannot be determined. The USPSTF concludes that the evidence is insufficient to determine the balance of benefits and harms of supplementation with single or paired nutrients (other than beta carotene and vitamin E) for the prevention of cardiovascular disease or cancer. Evidence is lacking and the balance of benefits and harms cannot be determined.
Recommendation The USPSTF recommends against the use of beta carotene or vitamin E supplements for the prevention of cardiovascular disease or cancer. (D recommendation) The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the use of multivitamin supplements for the prevention of cardiovascular disease or cancer. (I statement) The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the use of single- or paired-nutrient supplements (other than beta carotene and vitamin E) for the prevention of cardiovascular disease or cancer. (I statement)
The report also elaborates on potential harms:
For many of the vitamins and nutrients reviewed, there was little evidence of serious harms. However, an important harm of increased lung cancer incidence was reported with the use of beta carotene by persons who smoke tobacco or have occupational exposure to asbestos.
Excessive doses of vitamin supplements can cause several known adverse effects; for example, moderate doses of vitamin A supplements may reduce bone mineral density, and high doses may be hepatotoxic or teratogenic. Vitamin D has potential harms, such as a risk of hypercalcemia and kidney stones, when given at high doses. The potential for harm from other supplements at high doses should be carefully considered.
There is nothing new here, of course. I (and others) have been trying to get these points across for many years. But it is nevertheless most gratifying to see the message repeated by a top journal such as JAMA. I hope JAMA is more successful than I was in changing the behavior of the often all too gullible public!
Nausea and vomiting are common symptoms of patients with advanced cancer. While there is some evidence for acupuncture point stimulation in the treatment of these symptoms for patients having anticancer treatment, there is little for when they are not related to such treatment.
This study aimed to determine whether acupressure at the pericardium 6 sites can help treat nausea and vomiting suffered by palliative care patients with advanced cancer. The researchers conducted a double-blind randomized controlled trial-active versus placebo acupressure wristbands. In-patients with advanced cancer in two specialist palliative care units who fitted either or both of the following criteria were approached: nausea that was at least of moderate severity; vomiting daily on average for the prior 3 days.
A total of 57 patients were randomized to have either active or placebo acupressure wristbands. There was no difference in any of the outcome measures between the two groups:
- change from the baseline number of vomits;
- Visual Analogue Scale for ‘did acupressure wristbands help you to feel better?’;
- the total number of doses of antiemetic medication;
- the need for escalation of antiemetics.
The authors concluded that, in contrast to a previously published feasibility study, active acupressure wristbands were no better than placebo for specialist palliative care in patients with advanced cancer and nausea and vomiting.
When the research into acupuncture for nausea and vomiting began some 20 years ago, the evidence turned out to be encouraging. Later, as the studies became more and more rigorous, many trials failed to confirm the initial findings. Today, the totality of the evidence is far less convincing than it seemed years ago.
This is a phenomenon that can be observed not just in acupuncture research but in many types of treatment:
- Initially, over-enthusiastic researchers become victims of their own optimism.
- These investigators are less into testing hypotheses than into confirming their own wishful thinking.
- Thus, several positive trials emerge.
- These, however, turn out to be methodologically flawed.
- Eventually, the subject might be picked up by real scientists who truly test hypotheses.
- More and more negative studies thus emerge.
- Depending on how many flawed studies were initially published and how critical the authors of systematic reviews are, it can take years until the totality of the evidence depicts the true picture which discloses the initial findings as false-positive.
The message is, I think, clear: poor quality studies have the potential to mislead us for many years. Eventually, however, the self-cleansing ability of science should generate the truth about the value of any treatment. In other words:
poor-quality science is not just useless, it causes long-term harm
and
critical thinking prevents harm
Alan Gaby, the assistant editor of the journal Integr Med has written an interesting commentary about widespread fraud in natural health products research. Here is an excerpt of his article:
During the past 49 years, I have reviewed and analyzed more than 50 000 papers from the biomedical literature, most of which were related to the field of nutritional medicine. Doing this work has given me some understanding of how to assess the reliability of a study. Over the past 10 to 15 years, an uncomfortably large and growing number of published papers related to my area of expertise have left me wondering whether the research was fabricated; that is, whether people were writing papers about research that had not actually been conducted. If the studies were not actually conducted, the publishing of this research is an affront to all who value integrity in science, and it has the potential to harm practitioners and patients who rely on its findings.
The studies that have raised concerns have come primarily from Iran and to a lesser extent from Egypt, China, India, Japan, and a few other countries. Characteristics of these concerning studies typically include one or more of the following:
- The study comes from an investigator or research group that has published an enormous number of randomized clinical trials in a relatively short period of time.
- The number of participants in the trial is unusually large, when considering the resources that appear to be available to the researchers.
- The recruitment period for the trial is unusually short.
- The paper is submitted to a journal unusually rapidly after the study is completed, or in some cases before it would have been possible to have completed the trial.
- A randomized double-blind trial is conducted before there is any preliminary evidence of efficacy in humans (such as case reports or uncontrolled trials). Because double-blind trials are expensive to conduct, such trials are generally reserved for treatments for which there is some evidence of efficacy.
- The magnitude of the reported improvement is much larger than is typically seen in trials using just one or two nutrients.
- No funding source is listed or the study is listed as self-funded. This is of particular concern when the sample size or study design suggests that the study was expensive.
- The design of the study raises ethical issues, such as participants not being permitted to use treatments that are known to be effective.
- One or more baseline characteristics of the study group appear to be implausible.
- The research was conducted by a student as part of a graduate school thesis, and the magnitude of the project seems to have been beyond the capabilities and resources of a student.
__________________________________
What Gaby alludes to is a problem indeed. I have previously posted about the Chinese aspect of this story. What Gaby does not mention is the fact that even many studies of so-called alternative medicine (SCAM) which seem to be not overtly fraudulent are nevertheless highly suspect. I am referring to trials that are fatally flawed and/or studies that draw unwarranted conclusions. These are, of course, the types of studies that are the main target of this blog. Because they are so numerous, I feel that the damage they do is much bigger than that of the more overtly fraudulent papers.