Cancer
The objective of this survey was to determine
- which patients’ characteristics are associated with the use of so-called alternative medicine (SCAM) during cancer treatment,
- their pattern of use,
- and if it has any association with its safety profile.
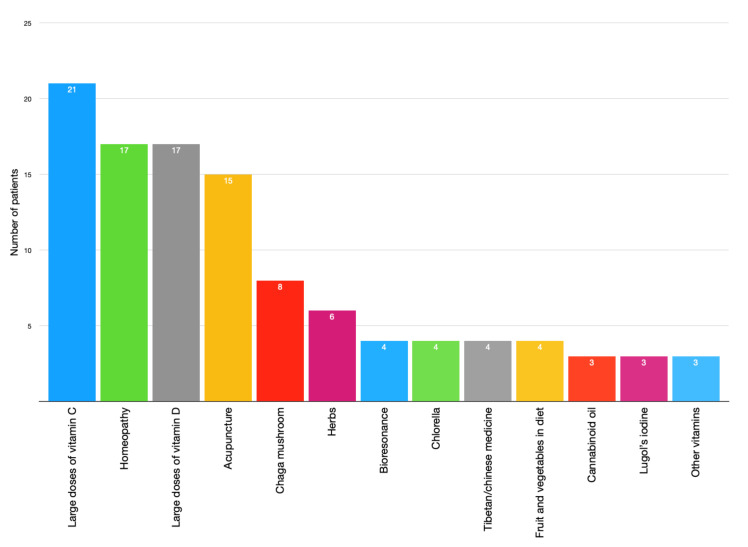
A total of 316 patients undergoing chemotherapy treatment in cancer centers in Poland between 2017 and 2019 were asked about their use of SCAM.
Patients’ opinion regarding the safety of unconventional methods is related to the use of SCAM. Moreover, patients’ thinking that SCAM can replace conventional therapy was correlated with his/her education. Moreover, the researchers performed analyses to determine factors associated with SCAM use including sociodemographic and clinical characteristics.
Crucially, they also conducted a survival analysis of patients undergoing chemotherapy with 42 months of follow-up. Using Kaplan-Meier curves and log-rank analysis, they found no statistical difference in overall survival between the groups that used and did not use any form of SCAM.

The authors concluded that SCAM use is common among patients undergoing chemotherapy treatment and should be considered by medical teams as some agents may interact with chemotherapy drugs and affect their efficacy or cause adverse effects.
As I have stated before, I find most surveys of SCAM use meaningless. This article is no exception – except for the survival analysis. It would have merited a separate, more detailed paper, yet the authors hardly comment on it. The analysis shows that SCAM users do not live longer than non-users. Previously, we have discussed several studies that suggested they live less long than non-users.
While this aspect of the new study is interesting, it proves very little. There are, of course, multiple factors involved in the survival of cancer patients, and even if SCAM use were a determinant, it is surely less important than many other factors. To get a better impression of the role SCAM plays, we need studies that carefully match patients according to the most obvious prognostic variables (RCTs would be problematic, difficult to do and unethical). Such studies do exist and they too fail to show that SCAM use prolongs survival, some even suggest it might shorten survival.
The aim of this investigation was to evaluate the marketing practices, beliefs and health claims regarding the use of colloidal silver in Finland. Contents of three company websites selling colloidal silver were reviewed, and the claims used in the marketing of colloidal silver were compared to the scientific information about silver. In Facebook posts and discussion about colloidal silver were analyzed.
In Finland, the marketing of colloidal silver products on websites selling the products did not follow the regulations of authorities; several scientifically unfounded claims about the efficacy and medical use of colloidal silver were found. After the Finnish Broadcasting Company (Yle) documentary and an intervention by authorities, contents of the websites were changed, but still questionable information and misleading claims could be found. In the analyzed Facebook groups attitudes towards medical use of colloidal silver were uncritically positive, internal use was highly promoted and the restrictions of use were considered unjustified.
The authors concluded that the use of quackery products such as colloidal silver can be dangerous, and their use and marketing should be controlled and restricted.
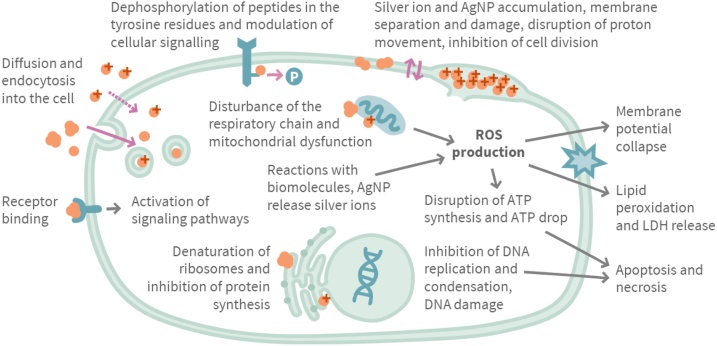
The authors stress that silver nanoparticles (AgNPs) are potentially toxic due to their small size and Ag+-release capabilities, and the use of colloidal silver products containing AgNPs can cause a wide variety of adverse effects such as argyria.
WebMD cautions that despite promoters’ claims, silver has no known function in the body and is not an essential mineral supplement. Colloidal silver products were once available as over-the-counter drug products. In 1999 the U.S. Food and Drug Administration (FDA) ruled that these colloidal silver products were not considered safe or effective. Colloidal silver products marketed for medical purposes or promoted for unproven uses are now considered “misbranded” under the law without appropriate FDA approval as a new drug. There are currently no FDA-approved over-the-counter or prescription drugs containing silver that are taken by mouth. However, there are still colloidal silver products being sold as homeopathic remedies and dietary supplements.
On this blog, we have discussed that colloidal silver is nevertheless marketed aggressively by crooks (see here and here). The message that emerges from all this seems clear: do not fall for the plethora of false claims made by irresponsible entrepreneurs who want your money and risk your health. Keep your money and health by staying away from colloidal silver and similar SCAMs.
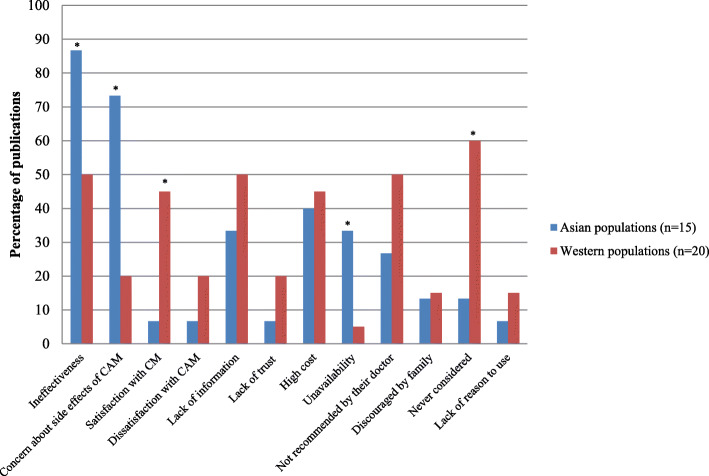
The authors of this review wanted to determine similarities and differences in the reasons for using or not using so-called alternative medicine (SCAM) amongst general and condition-specific populations, and amongst populations in each region of the globe.
Quantitative or qualitative original articles in English, published between 2003 and 2018 were reviewed. Conference proceedings, pilot studies, protocols, letters, and reviews were excluded. Papers were appraised using valid tools and a ‘risk of bias’ assessment was also performed. Thematic analysis was conducted. Reasons were coded in each paper, then codes were grouped into categories. If several categories reported similar reasons, these were combined into a theme. Themes were then analysed using χ2 tests to identify the main factors related to reasons for CAM usage.
A total of 231 publications were included. Reasons for SCAM use amongst general and condition-specific populations were similar. The top three reasons were:
- (1) having an expectation of benefits of SCAM (84% of publications),
- (2) dissatisfaction with conventional medicine (37%),
- (3) the perceived safety of SCAM (37%).
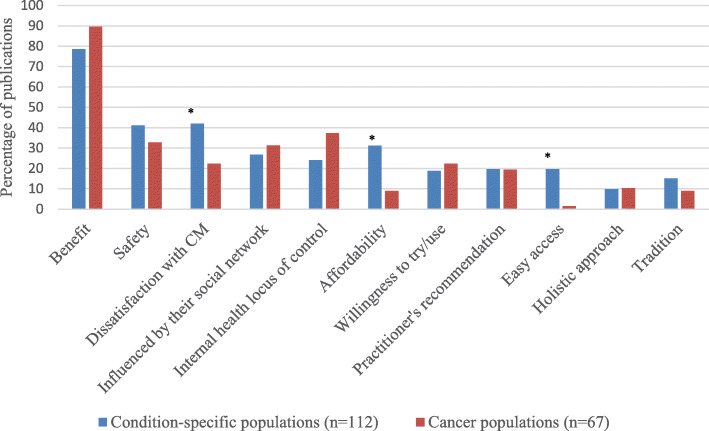
Internal health locus of control as an influencing factor was more likely to be reported in Western populations, whereas the social networks was a common factor amongst Asian populations (p < 0.05). Affordability, easy access to SCAM and tradition were significant factors amongst African populations (p < 0.05). Negative attitudes towards SCAM and satisfaction with conventional medicine were the main reasons for non-use (p < 0.05).
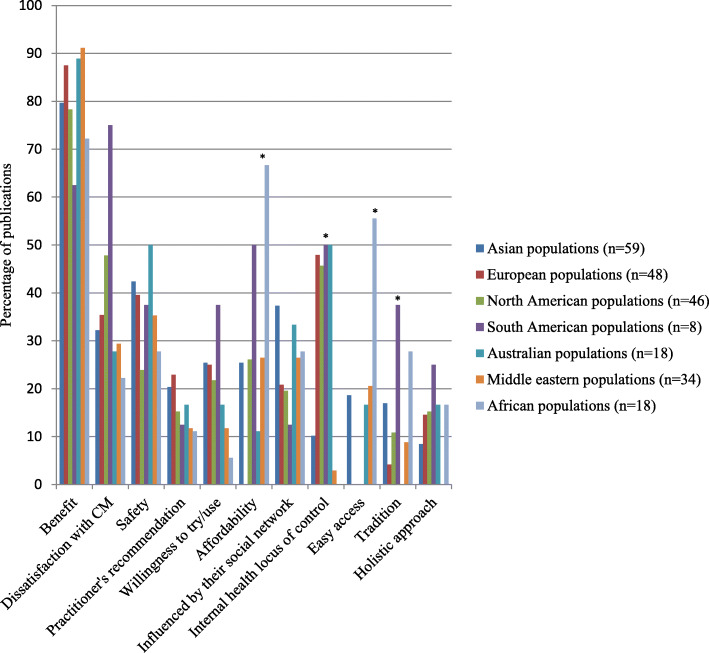
The authors concluded that dissatisfaction with conventional medicine and positive attitudes toward SCAM, motivate people to use SCAM. In contrast, satisfaction with conventional medicine and negative attitudes towards SCAM are the main reasons for non-use.
At this point, I thought: so what? This is all very obvious and does not necessitate an extensive review of the published literature. What it actually shows is that the realm of SCAM is obsessed with conducting largely useless surveys, a phenomenon, I once called ‘survey mania‘. But a closer look at the review does reveal some potentially interesting findings.
In less developed parts of the world, like Africa, SCAM use seems to be determined by affordability, accessibility and tradition. This makes sense and ties in with my impression that consumers in such countries would give up SCAM as soon as they can afford proper medicine.

This notion seems to be further supported by the reasons for not using SCAM. Asian consumers claim overwhelmingly that this is because they consider SCAM ineffective and unsafe.
In our review of 2011 (not cited in the new review), we looked at some of the issues from a slightly different angle and evaluated the expectations of SCAM users. Seventy-three articles met our inclusion criteria of our review. A wide range of expectations emerged. In order of prevalence, they included:
- the hope to influence the natural history of the disease;
- the desire to prevent disease and promote health/general well-being;
- the hope of fewer side effects;
- the wish to be in control over one’s health;
- the hope for symptom relief;
- the ambition to boost the immune system;
- the hope to receive emotional support;
- the wish to receive holistic care;
- the hope to improve quality of life;
- the expectation to relief of side effects of conventional medicine;
- the desire for a good therapeutic relationship;
- the hope to obtain information;
- the hope of coping better with illness;
- the expectation of supporting the natural healing process;
- the availability of SCAM.
All of these aspects, issues and notions might be interesting, even fascinating to some, but we should not forget three important caveats:
- Firstly, SCAM is such a diverse area that any of the above generalisations are highly problematic; the reasons and expectations of someone trying acupuncture may be entirely different from those of someone using homeopathy, for instance.
- Secondly (and more importantly), the ‘survey mania’ of SCAM researchers has not generated the most reliable data; in fact, most of the papers are hardly worth the paper they were printed on.
- Thirdly (and even more importantly, in my view), why should any of this matter? We have known about some of these issues for at least 3 decades. Has this line of research changed anything? Has it prevented consumers getting exploited by scrupulous SCAM entrepreneurs? Has it made consumers, politicians or anyone else more aware of the risks associated with SCAM? Has it saved many lives? I doubt it!
Acupuncture-moxibustion therapy (AMT) is a so-called alternative medicine (SCAM) that has been used for centuries in treatment of numerous diseases. Some enthusiasts even seem to advocate it for chemotherapy-induced leukopenia (CIL) The purpose of this review was to evaluate the efficacy and safety of acupuncture-moxibustion therapy in treating CIL.
Relevant studies were searched in 9 databases up to September 19, 2020. Two reviewers independently screened the studies for eligibility, extracted data, and assessed the methodological quality of selected studies. Meta-analysis of the pooled mean difference (MD) and risk ratio (RR) with their respective 95% confidence intervals (CI) were calculated.
Seventeen studies (1206 patients) were included, and the overall quality of the included studies was moderate. In comparison with medical therapy, AMT has a better clinical efficacy for CIL (RR, 1.24; 95% CI, 1.17-1.32; P < 0.00001) and presents advantages in increasing leukocyte count (MD, 1.10; 95% CI, 0.67-1.53; P < 0.00001). Also, the statistical results show that AMT performs better in improving the CIL patients’ Karnofsky performance score (MD, 5.92; 95% CI, 3.03-8.81; P < 0.00001).
The authors concluded that this systematic review and meta-analysis provides updated evidence that AMT is a safe and effective alternative for the patients who suffered from CIL.
A CIL is a serious complication. If I ever were afflicted by it, I would swiftly send any acupuncturist approaching my sickbed packing.
But this is not an evidence-based attitude!!!, I hear some TCM-fans mutter. What more do you want that a systematic review showing it works?
I beg to differ. Why? Because the ‘evidence’ is hardly what critical thinkers can accept as evidence. Have a look at the list of the primary studies included in this review:
- Lin Z. T., Wang Q., Yu Y. N., Lu J. S. Clinical observation of post-chemotherapy-leukopenia treated with ShenMai injectionon ST36. World Journal of Integrated Traditional and Western Medicine. 2010;5(10):873–876. [Google Scholar]
- Wang H. Clinical Observation of Acupoint Moxibustion on Leukopenia Caused by Chemotherapy. Beijing, China: Beijing University of Chinese Medicine; 2011. [Google Scholar]
- Fan J. Y. Coupling of Yin and Yang between Ginger Moxibustion Improve the Clinical Effect of the Treatment of Chemotherapy Adverse Reaction. Henan, China: Henan University of Chinese Medicine; 2013. [Google Scholar]
- Lu D. R., Lu D. X., Wei M., et al. Acupoint injection with addie injection for patients of nausea and vomiting with cisplatin induced by chemotherapy. Journal of Clinical Acupuncture and Moxibustion. 2013;29(10):33–38. [Google Scholar]
- Yang J. E. The Clinical Observation on Treatment of Leukopenia after Chemotherapy with Needle Warming Moxibustion. Hubei, China: Hubei University of Chinese Medicine; 2013. [Google Scholar]
- Fu Y. H., Chi C. Y., Zhang C. Y. Clinical effect of acupuncture and moxibustion on leukopenia after chemotherapy of malignant tumor. Guide of China Medicine. 2014;12(12) [Google Scholar]
- Wang J. N., Zhang W. X., Gu Q. H., Jiao J. P., Liu L., Wei P. K. Protection of herb-partitioned moxibustion on bone marrow suppression of gastric cancer patients in chemotherapy period. Chinese Archives of Traditional Chinese Medicine. 2014;32(12):110–113. [Google Scholar]
- Zhang J. The Clinical Research on Myelosuppression and Quality of Life after Chemotherapy Treated by Grain-Sized Moxibustion. Nanjing, China: Nanjing University of Chinese Medicine; 2014. [Google Scholar]
- Tian H., Lin H., Zhang L., Fan Z. N., Zhang Z. L. Effective research on treating leukopenia following chemotherapy by moxibustion. Clinical Journal of Chinese Medicine. 2015;7(10):35–38. [Google Scholar]
- Hu G. W., Wang J. D., Zhao C. Y. Effect of acupuncture on the first WBC reduction after chemotherapy for breast cancer. Beijing Journal of Traditional Chinese Medicine. 2016;35(8):777–779. [Google Scholar]
- Zhu D. L., Lu H. Y., Lu Y. Y., Wu L. J. Clinical observation of Qi-blood-supplementing needling for leukopenia after chemotherapy for breast cancer. Shanghai Journal of Acupuncture and Moxibustion. 2016;35(8):964–966. [Google Scholar]
- Chen L, Xu G. Y. Observation on the prevention and treatment of chemotherapy-induced leukopenia by moxibustion therapy. Zhejiang Journal of Traditional Chinese Medicine. 2016;51(8):p. 600. [Google Scholar]
- Mo T., Tian H., Yue S. B., Fan Z. N., Zhang Z. L. Clinical observation of acupoint moxibustion on leukocytopenia caused by tumor chemotherapy. World Chinese Medicine. 2016;11(10):2120–2122. [Google Scholar]
- Nie C. M. Nursing observation of acupoint moxibustion in the treatment of leucopenia after chemotherapy. Today Nurse. 2017;4:93–95. [Google Scholar]
- Wang D. Y. Clinical Research on Post-chemotherapy-leukopenia with Spleen-Kidney Yang Deficiency in Colorectal Cancer Treated with Point-Injection. Yunnan, China: Yunnan University of Chinese Medicine; 2017. [Google Scholar]
- Gong Y. Q, Zhang M. Q, Zhang B. C. Prevention and treatment of leucocytopenia after chemotherapy in patients with malignant tumor with ginger partitioned moxibustion. Chinese Medicine Modern Distance Education of China. 2018;16(21):135–137. [Google Scholar]
- Li Z. C., Lian M. J., Miao F. G. Clinical observation of fuzheng moxibustion combined with wenyang shengbai decoction in the treatment of 80 cases of leukopenia after chemotherapy. Hunan Journal of Traditional Chinese Medicine. 2019;35(3):64–66. [Google Scholar]
Notice anything peculiar?
- The studies are all from China where data fabrication was reported to be rife.
- They are mostly unavailable for checking (why the published adds links that go nowhere is beyond me).
- Many do not look at all like randomised clinical trials (which, according to the authors, was an inclusion criterion).
- Many do not look as though their primary endpoint was the leukocyte count (which, according to the authors, was another inclusion criterion).
Intriguingly, the authors conclude that AMT is not just effective but also ‘safe’. How do they know? According to their own data extraction table, most studies failed to mention adverse effects. And how exactly is acupuncture supposed to increase my leukocyte count? Here is what the authors offer as a mode of action:
I think it is high time that we stop tolerating that the medical literature gets polluted with such nonsense (helped, of course, by journals that are beyond the pale) – someone might actually believe it, in which case it would surely hasten the death of vulnerable patients.
Recent comments on this blog prompted me to look into a very strange therapeutic and diagnostic device used by some practitioners of so-called alternative medicine (SCAM):
The OBERON provides the most unique tool for scanning the various organs and systems of the physical body without having to make a medical or surgical intrusion. Developed by Russian scientists since the early 1990’s, the OBERON is the most revolutionary computer programmed invention available in the world today for analyzing and treating all the body’s organs and functions.
This device scans each organ or tissue on a cellular level. It compares the measurements to a database of thousands of referenced conditions and their diagnosis. OBERON uses a special emitter to modulate the carrier frequency for the cell communication and it uses special sensor trigger readers built into headphones to read the cells own signals.
OBERON finds out how stressed an organ is, and if there are any diseases developing, how much the cells are influenced by a specific disease, and which micro organisms and bacteria are in the area at the time of the scan.
BENEFITS OF THE OBERON:
Rebalances the body so that it can start to heal itself!
Makes intrusive and embarrassing examinations a THING OF THE PAST!!!!
Quick examination (in seconds) with immediate results
Replaces dozens of traditional diagnostic methods.
Finds weaknesses in the skeleton, organs, blood, tissue, etc.
There are no side effects, unpleasantness or injury after treatment
Bio-resonance META-therapy
A print out of the report on findings can be taken at the end of the session…
The method is based on an analysis of the brain stems electromagnetic waves which contain the complete information of the entire organism. This information is read by a sensor. A frequency transmitter aimed at the projection area of the brain stem stimulates this electromagnetic radiation.
Meta- Therapy repairs the organism using a diversity of modulated electromagnetic waves. This treatment stimulates the body’s own functions so that they solve the problem and it stimulates the immune defense and is a very good supplement or alternative to traditional treatment. The patient can follow on the screen how the organ progressively gets better, and afterwards one can take a new measurement showing the improvement…
________________________________________
Sounds fantastic?
Yes, indeed – fantastic as in fantasy!
Almost as much relation to reality as OBERON, king of the fairies in medieval literature.
The modern OBERON device is being used by infamous proponents of integrated medicine like Dr Julian Kenyon who already made an appearance on this blog. On his website, Kenyon published a paper in which he provides details about the OBERON. To a lay person, the sciency text might look like science; however, this impression would be false. The ‘study’ Kenyon mentioned is not on Medline. In fact, Dr Kenyon (former associate of the late George Lewith) has merely 4 Medline-listed papers:
- Physiological and psychological explanations for the mechanism of acupuncture as a treatment for chronic pain. Soc Sci Med. 1984;19(12):1367-78. doi: 10.1016/0277-9536(84)90026-1.PMID: 6085191 Review.
- Is electrodermal testing as effective as skin prick tests for diagnosing allergies? A double blind, randomised block design study. BMJ. 2001 Jan 20;322(7279):131-4. doi: 10.1136/bmj.322.7279.131.PMID: 11159567 Free PMC article. Clinical Trial.
- Randomised double-blind trial on the immediate effects of naloxone on classical Chinese acupuncture therapy for chronic pain. Acupunct Electrother Res. 1983;8(1):17-24. doi: 10.3727/036012983816715064.PMID: 6135300 Clinical Trial.
- Food sensitivity, a search for underlying causes. Case study of 12 patients. Kenyon JN.Acupunct Electrother Res. 1986;11(1):1-13. doi: 10.3727/036012986816359238.PMID: 2872775
And what about other researchers? Aren’t there ANY decent studies of the OBERON?
Not as far as I can see (if anyone does know of peer-reviewed research, please let me know).
So, what is the conclusion?
My conclusion is this:
There is no evidence that the OBERON does anything useful other than putting money in the bank accounts of those charlatans who use or manufacture it.
And what does that make Kenyon and all the other SCAM practitioners using the OBERON or similar devices?
I leave it to you to decide.
Despite reported widespread use of dietary supplements by cancer patients, few empirical data with regard to their safety or efficacy exist. Because of concerns that antioxidants could reduce the cytotoxicity of chemotherapy, a prospective study was carried out to evaluate associations between supplement use and breast cancer outcomes.
Patients with breast cancer randomly assigned to an intergroup metronomic trial of cyclophosphamide, doxorubicin, and paclitaxel were queried on their use of supplements at registration and during treatment (n =1,134). Cancer recurrence and survival were indexed at 6 months after enrollment.
There were indications that use of any antioxidant supplement (vitamins A, C, and E; carotenoids; coenzyme Q10) both before and during treatment was associated with an increased hazard of recurrence and, to a lesser extent, death. Relationships with individual antioxidants were weaker perhaps because of small numbers. For non-antioxidants, vitamin B12 use both before and during chemotherapy was significantly associated with poorer disease-free survival and overall survival. Use of iron during chemotherapy was significantly associated with recurrence as was use both before and during treatment. Results were similar for overall survival. Multivitamin use was not associated with survival outcomes.
The authors concluded that associations between survival outcomes and use of antioxidant and other dietary supplements both before and during chemotherapy are consistent with recommendations for caution among patients when considering the use of supplements, other than a multivitamin, during chemotherapy.
These data are interesting but, for a range of reasons, not compelling. There might have been several important confounding factors distorting the findings. Even though clinical and life-style variables were statistically adjusted for in this study, it might still be possible that supplement users and non-users were not comparable in impotant prognostic variables. Simply put, sicker patients might be more likely to use supplements and would then have worse outcomes not because of the supplements but their disease severity.
Moreover, it seems important to note that other research showed the opposite effects. For instance, a study prospectively examined the associations between antioxidant use after breast cancer (BC) diagnosis and BC outcomes in 2264 women. The cohort included women who were diagnosed with early stage, primary BC from 1997 to 2000 who enrolled, on average, 2 years postdiagnosis. Baseline data were collected on antioxidant supplement use since diagnosis and other factors. BC recurrence and mortality were ascertained, and hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated.
Antioxidant supplement use after diagnosis was reported by 81% of women. Among antioxidant users, frequent use of vitamin C and vitamin E was associated with a decreased risk of BC recurrence. Vitamin E use was associated with a decreased risk of all-cause mortality. Conversely, frequent use of combination carotenoids was associated with increased risk of death from BC and all-cause mortality.
The authors concluded that frequent use of vitamin C and vitamin E in the period after BC diagnosis was associated with a decreased likelihood of recurrence, whereas frequent use of combination carotenoids was associated with increased mortality. The effects of antioxidant supplement use after diagnosis likely differ by type of antioxidant.
Yet another study provided limited support for the hypothesis that antioxidant supplements may reduce the risk of breast cancer recurrence or breast cancer-related mortality.
Confused?
Me too!
What is needed, it seems, is a systematic review of all these contradicting studies. A 2009 review is available of the associations between antioxidant supplement use during breast cancer treatment and patient outcomes.
Inclusion criteria were: two or more subjects; clinical trial or observational study design; use of antioxidant supplements (vitamin C, vitamin E, antioxidant combinations, multivitamins, glutamine, glutathione, melatonin, or soy isoflavones) during chemotherapy, radiation therapy, and/or hormonal therapy for breast cancer as exposures; treatment toxicities, tumor response, recurrence, or survival as outcomes.
A total of 22 articles met the criteria. Their findings did not support any conclusions regarding the effects of individual antioxidant supplements during conventional breast cancer treatment on toxicities, tumor response, recurrence, or survival. A few studies suggested that antioxidant supplements might decrease side effects associated with treatment, including vitamin E for hot flashes due to hormonal therapy and glutamine for oral mucositis during chemotherapy. Underpowered trials suggest that melatonin may enhance tumor response during treatment.
The authors concluded that the evidence is currently insufficient to inform clinician and patient guidelines on the use of antioxidant supplements during breast cancer treatment. Thus, well designed clinical trials and observational studies are needed to determine the short- and long-term effects of such agents.
Still confused?
Me too!
Antioxidants seem to have evolved as parts of elaborate networks in which each substance plays slightly different roles. This means that each antioxidant has a different spectrum of actions. And this means that it is probably not very constructive to lump them all together and excect to see uniform effects. What we would need to create more clarity is a series of RCTs on single antioxidants. But who is going to fund them? We might be waiting a long time for more clarity. Meanwhile, consuming a healthy and well-balanced diet might be the best advice for cancer patients and everyone else.
Melatonin is an indolamine hormone which is secreted from the human pineal gland during night-time acting as physiological regulator. In many countries, dietary supplements containing synthetically produced melatonin are available. Melatonin is being promoted as a treatment of a range of conditions, including virtually all types of cancer.
One website, for instance, states that the anti-cancer benefits of melatonin aren’t just indirect; this miracle molecule is also classified as a directly cytotoxic hormone and anti-cancer agent. Studies have referred to melatonin as a “full-service anti-cancer agent” due to its ability to inhibit the initiation of cell mutation and cancer growth, and to halt the progression and metastasis of cancer cell colonies.
Such statements sound far too good to be true. So, let’s have a look and find out what the evidence tells us. Test-tube experiments suggest that melatonin has anti-cancer effects.[1] Its actions include the advancement of apoptosis, the arrest of the cell cycle, inhibition of metastasis, and antioxidant activity.[2]
A review of 21 clinical trials of melatonin for cancer found positive effects for complete response, partial response, and stable disease. In trials combining melatonin with chemotherapy, adjuvant melatonin therapy decreased 1-year mortality and improved outcomes of complete response, partial response, and stable disease. In these studies, melatonin also significantly reduced asthenia, leukopenia, nausea and vomiting, hypotension, and thrombocytopenia. The authors concluded that melatonin may benefit cancer patients who are also receiving chemotherapy, radiotherapy, supportive therapy, or palliative therapy by improving survival and ameliorating the side effects of chemotherapy.[3]
A further systematic review of RCTs of melatonin in solid tumour cancer patients evaluated its effect on one-year survival. Ten trials were included of melatonin as either sole treatment or as adjunct treatment. Melatonin reduced the risk of death at 1 year. Effects were consistent across melatonin dose, and type of cancer. No severe adverse events were reported.[4]
A 2012 systematic review confirmed these findings by concluding that Melatonin as an adjuvant therapy for cancer led to substantial improvements in tumor remission, 1-year survival, and alleviation of radiochemotherapy-related side effects.[5]
Finally, a 2020 review concluded that melatonin in combination with anticancer agents may improve the efficacy of routine medicine and survival rate of patients with cancer. [6] Apart from its direct anticancer potential, melatonin also seems to reduce chemotherapy toxicity, while improving its therapeutic efficacy.[7]
So, is this evidence compelling? While all this does indeed sound encouraging, it is necessary to mention several important caveats:
- The primary studies of melatonin suffer from several methodological shortcomings.
- Their vast majority originate from one single research group.
- In recent years, there have been no further clinical studies trying to replicate the initial findings.
This means that definitive trials are still missing, and it would seem wise to interpret the existing evidence with great caution.
References
[1] Kong X, Gao R, Wang Z, Wang X, Fang Y, Gao J, Reiter RJ, Wang J. Melatonin: A Potential Therapeutic Option for Breast Cancer. Trends Endocrinol Metab. 2020 Sep 3:S1043-2760(20)30155-7. doi: 10.1016/j.tem.2020.08.001. Epub ahead of print. PMID: 32893084.
[2] Samanta S. Melatonin: an endogenous miraculous indolamine, fights against cancer progression. J Cancer Res Clin Oncol. 2020 Aug;146(8):1893-1922. doi: 10.1007/s00432-020-03292-w. Epub 2020 Jun 24. PMID: 32583237.
[3] Seely D, Wu P, Fritz H, Kennedy DA, Tsui T, Seely AJ, Mills E. Melatonin as adjuvant cancer care with and without chemotherapy: a systematic review and meta-analysis of randomized trials. Integr Cancer Ther. 2012 Dec;11(4):293-303. doi: 10.1177/1534735411425484. Epub 2011 Oct 21. PMID: 22019490.
[4] Mills E, Wu P, Seely D, Guyatt G. Melatonin in the treatment of cancer: a systematic review of randomized controlled trials and meta-analysis. J Pineal Res. 2005 Nov;39(4):360-6. doi: 10.1111/j.1600-079X.2005.00258.x. PMID: 16207291.
[5] Wang YM, Jin BZ, Ai F, Duan CH, Lu YZ, Dong TF, Fu QL. The efficacy and safety of melatonin in concurrent chemotherapy or radiotherapy for solid tumors: a meta-analysis of randomized controlled trials. Cancer Chemother Pharmacol. 2012 May;69(5):1213-20. doi: 10.1007/s00280-012-1828-8. Epub 2012 Jan 24. PMID: 22271210.
[6] Pourhanifeh MH, Mehrzadi S, Kamali M, Hosseinzadeh A. Melatonin and gastrointestinal cancers: Current evidence based on underlying signaling pathways. Eur J Pharmacol. 2020 Nov 5;886:173471. doi: 10.1016/j.ejphar.2020.173471. Epub 2020 Aug 30. PMID: 32877658.
[7] Iravani S, Eslami P, Dooghaie Moghadam A, Moazzami B, Mehrvar A, Hashemi MR, Mansour-Ghanaei F, Mansour-Ghanaei A, Majidzadeh-A K. The Role of Melatonin in Colorectal Cancer. J Gastrointest Cancer. 2020 Sep;51(3):748-753. doi: 10.1007/s12029-019-00336-4. PMID: 31792737.
I know of one patient who turned to the Gerson Therapy having been told that she was suffering from terminal cancer and would not survive another course of chemotherapy. Happily, seven years later she is alive and well. So therefore it is vital that, rather than dismissing such experiences, we should further investigate the beneficial nature of these treatments.
HRH The Prince of Wales (2004)
I was reminded of this embarrassing (because displaying profound ignorance) quote when I looked at the website of the ‘GERSON SUPPORT GROUP UK‘ where it is prominently cited. Under the heading ‘SCIENCE & CLINICAL RATIONAL’ the site offers a long article about the Gerson therapy (GT). Allow me to show you a few quotes from it:
Dr Max Gerson’s therapy is based on the belief that insufficient nutrients within the cells and an accumulation of toxins in the tissues lead to a breakdown in healthy cellular function which, if left unchecked, can trigger cancer.
That is interesting, I find, because the statement clearly admits that the GT is not an evidence-based therapy but a belief-based treatment.
The therapy that he developed uses a restrictive, plant-based diet and specific supplements to boost healthy cellular function; and various detoxification procedures, including coffee enemas, to eliminate waste products.
The claims hidden in this sentence remain unproven. There is no evidence that cellular fuction is boosted, nor that the procedures eliminate toxins.
… we only need to look at communities across the globe which exist in a pre-industrialised state to see that, whilst they might be more likely to die from pneumonia or tuberculosis, rates of degenerative illness are a fraction of those in the ‘developed‘ world. The age-adjusted death rate from breast cancer is less than 2 per 100,000 of the population in Thailand, Sri Lanka and El Salvador and around 33 per 100,000 in the UK, US, The Netherlands and numerous other affluent, Western countries.
Correlation is not causation! Pre-industrial societies also watch less TV, eat less ice-cream, read less fashion magazines, etc., etc. Are these habits also the cause of cancer?
… migrant studies show that within two generations the cancer rates of migrants increase rapidly towards Western rates, again underlining the assertion that cancer is caused primarily by diet and lifestyle rather than ‘faulty’ genes.
In no way is this an argument for eating raw vegetable and taking your coffee via the rectum.
In the German scientific golden age of the 1920s and 30s…
Golden age for what, for fascists?
Gerson had used a restricted diet to cure himself of migraines. He then helped another patient to reverse tuberculosis, and many others to reverse a variety of degenerative illnesses, all by similar means. He later developed his therapy to the point where he was able to help individuals reverse cancer.
In this case, Max Gerson was ignorant of the fact that experience and evidence are two fundamentally different things.
Max Gerson developed his therapy in an iterative way, starting with a restrictive plant-based diet, adding vitamins, minerals and enzymes to encourage the oxygenation of the cells and then introducing the coffee enemas to aid detoxification of waste products. What is fascinating is that science has subsequently explained the mechanism of action behind some of his theories. (See Biochemical Basis to the Therapy).
Science has not explained the mechanism of action, not least because the action has never been verified. There are no robust clinical trials of Gerson’s therapy. Evidently, 100 years were not enough to conduct any – or perhaps the proponents know only too well that they would not generate the results they hoped?
Equally interesting is that in 2012 Dr Thomas Seyfried published the results of many years research in Cancer as a Metabolic Disease.
Really? On Medline, I find only two cancer-related papers for Seyfried T. 2012:
Dietary restriction promotes vessel maturation in a mouse astrocytoma.
Thus, nearly a century after their original proposition that the fundamental cause of cancer was faulty cellular metabolism, it seems that doctors Otto Warburg and Max Gerson might be vindicated.
No, to ‘vindicate’ a therapeutic suggestion one needs several rigorous clinical trials. And for the GT, they remain absent.
_______________________________
So, what does the GT amount to?
- proponents had ~100 years to produce evidence;
- they failed to do so;
- thus the therapy is at best unproven;
- it is also biologically implausible;
- moreover, it is expensive;
- crucially it is not free of serious adverse effects;
- it is promoted only by those who seem to make money from it.
The only controlled clinical trial of a Gerson-like therapy that I know of is this one (rarely cited by Gerson fans):
Conventional medicine has had little to offer patients with inoperable pancreatic adenocarcinoma; thus, many patients seek alternative treatments. The National Cancer Institute, in 1998, sponsored a randomized, phase III, controlled trial of proteolytic enzyme therapy versus chemotherapy. Because most eligible patients refused random assignment, the trial was changed in 2001 to a controlled, observational study.
METHODS
All patients were seen by one of the investigators at Columbia University, and patients who received enzyme therapy were seen by the participating alternative practitioner. Of 55 patients who had inoperable pancreatic cancer, 23 elected gemcitabine-based chemotherapy, and 32 elected enzyme treatment, which included pancreatic enzymes, nutritional supplements, detoxification, and an organic diet. Primary and secondary outcomes were overall survival and quality of life, respectively.
RESULTS
At enrollment, the treatment groups had no statistically significant differences in patient characteristics, pathology, quality of life, or clinically meaningful laboratory values. Kaplan-Meier analysis found a 9.7-month difference in median survival between the chemotherapy group (median survival, 14 months) and enzyme treatment groups (median survival, 4.3 months) and found an adjusted-mortality hazard ratio of the enzyme group compared with the chemotherapy group of 6.96 (P < .001). At 1 year, 56% of chemotherapy-group patients were alive, and 16% of enzyme-therapy patients were alive. The quality of life ratings were better in the chemotherapy group than in the enzyme-treated group (P < .01).
CONCLUSION
Among patients who have pancreatic cancer, those who chose gemcitabine-based chemotherapy survived more than three times as long (14.0 v 4.3 months) and had better quality of life than those who chose proteolytic enzyme treatment.
Considering all this, I believe, it would be hard to name a cancer quackery that is less credible than the GT.
Coffee enemas consist of the administration of warm coffee via the rectum into a patient’s intestines. They are popular, not least because they cause profuse bowel movements and thus lead to immediate relief of constipation and therefore to short-lasting weight loss.
Coffee enemas are promoted for detox under the erroneous assumption that that the content of our colon is toxic, an obsolete theory known as ‘autointoxication’. Other notions assume that coffee enemas have beneficial antioxidant effects or stimulate the liver. Supporters of coffee enemas also claim they are effective treatments for:
- boosting immunity
- increasing energy
- preventing yeast overgrowth
- treating autoimmune diseases
- excreting parasites from the digestive tract
- removing heavy metals from the body
- alleviating depression
- treating cancer
Coffee enemas can cause adverse reactions some of which can be severe and have even caused fatalities:
- electrolyte imbalances
- rectal burns
- nausea
- vomiting
- cramping
- bloating
- dehydration
- bowel perforation
This new systematic review was conducted to investigate the safety and effectiveness of self-administered coffee enema and to provide evidence about its benefits and risks.
Relevant studies were retrieved from multiple electronic literature searches. Considering self-administered coffee enema being used in a various indication, study population was not restricted. Any types of published studies that included outcomes of effectiveness or safety of self-administered coffee enema with or without comparators were eligible for inclusion in this systematic review. Data on biomedical indications, patient-reported outcomes, and adverse events were collected. Descriptive analyses were planned because diverse health conditions and outcome variables did not allow for quantitative synthesis.
Nine case reports that describe adverse events were identified and included in the analysis. The reported problems included:
- colitis,
- proctocolitis,
- rectal perforation, peritonitis,
- rectal burn,
- cardiorespitatory arrest, followed by death,
- hepatic failure, followed by death,
- vomiting, dyspnoea, followed by death.
No study reporting on the effectiveness of coffee enema was found.
The authors concluded that, based on the evidences reviewed, this systematic review does not recommend coffee enema self-administration as a SCAM modality that can be adopted as a mean of self-care, given the unsolved issues on its safety and insufficient evidence with regard to the effectiveness.
So-called alternative medicine (SCAM) is full of truly barmy ideas, but coffee enems are amongst the worst. They are disgusting, uncomfortable, useless and risky. I am posting this article with the sincere hope that nobody reading it will ever consider using such nonsense.
The aim of this RCT was to examine symptom responses resulting from a home-based reflexology intervention delivered by a friend/family caregiver to women with advanced breast cancer undergoing chemotherapy, targeted, and/or hormonal therapy.
Patient-caregiver dyads (N = 256) were randomized to 4 weekly reflexology sessions or attention control. Caregivers in the intervention group were trained by a reflexology practitioner in a 30-min protocol. During the 4 weeks, both groups completed telephone symptom assessments using the M. D. Anderson Symptom Inventory. Those who completed at least one weekly call were included in this secondary analysis (N = 209). Each symptom was categorized as mild, moderate, or severe using established interference-based cut-points. Symptom response meant an improvement by at least one category or remaining mild. Symptom responses were treated as multiple events within patients and analysed using generalized estimating equations technique.
Reflexology was more successful than attention control in producing responses for pain with no significant differences for other symptoms. In the reflexology group, greater probability of response across all symptoms was associated with lower number of comorbid condition and lower depressive symptomatology at baseline. Compared to odds of responses on pain (chosen as a referent symptom), greater odds of symptom response were found for disturbed sleep and difficulty remembering with older aged participants.
Adjusted odds ratios (ORs) of symptom responses for reflexology arm versus control (adjusted for age, number of comorbid conditions, depressive symptoms at baseline, and treatment type: chemotherapy with or without hormonal therapy versus hormonal therapy alone)
Symptom OR (95% CI) p value
Fatigue 1.76 (0.99, 3.12) 0.06
Pain 1.84 (1.05, 3.23) 0.03
Disturbed sleep 1.45 (0.76, 2.77) 0.26
Shortness of breath 0.58 (0.26, 1.30) 0.19
Remembering 0.96 (0.51, 1.78) 0.89
Lack of appetite 1.05 (0.45, 2.49) 0.91
Dry mouth 1.84 (0.86, 3.94) 0.12
Numbness and tingling 1.40 (0.75, 2.64) 0.29
Depression 1.38 (0.78, 2.43) 0.27
The authors concluded that home-based caregiver-delivered reflexology was helpful in decreasing patient-reported pain. Age, comorbid conditions, and depression are potentially important tailoring factors for future research and can be used to identify patients who may benefit from reflexology.
This is certainly one of the more rigorous studies of reflexology. It is well designed and reported. How valid are its findings? To a large degree, this seems to depend on the somewhat unusual statistical approach the investigators employed:
Baseline characteristics were summarized by study group for outcome values and potential covariates. The unit of analysis was patient symptom; multiple symptoms were treated as nested within the patient being analyzed, using methodology described by Given et al. [24] and Sikorskii et al. [17]. Patient symptom responses were treated as multiple events, and associations among responses to multiple symptoms within patients were accounted for by specifying the exchangeable correlation structure in the generalized estimating equations (GEE) model. The GEE model was fitted using the GENMOD procedure in SAS 9.4 [25]. A dummy symptom variable with 9 levels was included in the interaction with the trial arm to differentiate potentially different effects of reflexology on different symptoms. Patient-level covariates included age, number of comorbid conditions, type of treatment (chemotherapy or targeted therapy with or without
hormonal therapy versus hormonal therapy only), and the CES-D score at baseline. Odds ratios (ORs) and their 95% confidence intervals (CIs) were obtained for the essential parameter of study group for each symptom.
Another concern is the fact that the study crucially depended on the reliability of the 256 carers. It is conceivable, even likely, I think, that many carers from both groups were less than strict in adhering to the prescribed protocol. This might have distorted the results in either direction.
Finally, the study was unable to control for the possibly substantial placebo response that a reflexology massage unquestionably provokes. Therefore, we are not able to tell whether the observed effect is due to the agreeable, non-specific effects of touch and foot massages, or to the postulated specific effects of reflexology.