quackery
The COVID-19 pandemic has posed an unprecedented challenge to global health. Classical homeopathy may, according to homeopaths, have a role to play in alleviating this burden. The objective of this study was to curate data on the treatment effect of classical homeopathy for COVID-19 in a real-world scenario to guide future scientific investigations.
Classical homeopaths from the International Academy of Classical Homeopathy (IACH) were asked to provide details on cases they treated by filling out a standardized questionnaire. COVID-19 cases were defined according to World Health Organization (WHO) criteria as suspected/probable/confirmed cases, with intervention provided being either stand-alone classical homeopathy or combined with conventional therapy for COVID-19. Cases were followed up with main outcomes being ‘improved’, ‘not improved’, or ‘progressed’ post-treatment. Details of the homeopathic remedies used and the main symptoms at the presentation were gathered. Factors associated with main outcomes were investigated with correlational and regression analyses.
367 patients (male 166, female 201) met eligibility criteria (mean age 42.75 years). The mean follow-up period was 6.5 (standard deviation, SD=5.3) days. 255 were confirmed COVID-19 cases, with 61 probable and 51 suspected cases, respectively. The most used remedy was Arsenicum album. Over 73% of COVID-19 patients (and about 79% of severe cases) improved under classical homeopathic treatment. The number of remedies required per individual was negatively correlated to improvement (P< 0.01). Fever, the most common symptom at presentation (74.4%), was associated with an increased likelihood of improvement (P<0.01). Improvement was negatively associated with advanced age, but not associated with sex (P<0.01).
The authors conclude that this study suggests that classical homeopathy was associated with improvement in COVID-19, including severe cases. Despite limitations from study design and data sources, our findings should prompt further studies on the role of classical homeopathy in the management of COVID-19.
I BEG TO DIFFER!
These cases suggest nothing of the sort. If anything, these highly selected cases suggest that about 27% of the exemplary patients did not improve, perhaps they even died. This implies to me that classical homeopathy worsens the prognosis of patients infected with COVID-19.
The ‘International Academy of Classical Homeopathy‘ is led by the ‘Ueber-Homeopath’, George Vithoulkas. His vision is that this Academy will become a center of real knowledge which will provide an education that will far exceed the technical and strictly “medical” aspect of one’s learning. One might ask what fanatics like he truly want to achieve – is it perhaps the promotion of ‘euthanasia homoeopathica’?
This trial investigated the effect of osteopathic visceral manipulation (OVM) on disability and pain intensity in individuals with functional constipation and chronic nonspecific low back pain. It was designed as a randomized controlled trial with a blinded assessor. Seventy-six volunteers with functional constipation and chronic nonspecific low back pain were randomized to two groups: OVM and sham OVM. The primary clinical outcome was pain intensity measured using a numeric rating scale (NRS) and disability measured using the Oswestry Disability Index (ODI). The secondary outcomes were electromyographic signals measured during the flexion-extension cycle, the finger-to-floor distance during complete flexion of the trunk, and the Fear-Avoidance Beliefs Questionnaire (FABQ). All outcomes were determined after six weeks of treatment as well as three months after randomization.
The OVM group reported a reduction in pain intensity after six weeks of treatment and at the three-month evaluation (p < .0002) and the sham group reported a reduction in pain intensity after three-month evaluation (p < .007). For the ODI was also found in the OVM group six weeks after the end of treatment (treatment effect = -6.59, 95% CI: -12.01 to -1.17, p = .01) and at the three-month evaluation (treatment effect = -6.02, 95% CI: -11.55 to -0.49, p = .03). Significant differences were also found for paravertebral muscle activity during the dynamic phases (flexion and extension) six-week evaluations.
The authors concluded that the OVM group demonstrated a reduction in pain intensity and improvement in disability after six-weeks and three-month follow-up while the sham group reduction in pain three-month follow-up.
I have no access to the full paper (if someone can send me the paper, I would update my post accordingly), but from reading the abstract, it seems the reported findings are based on within-group changes. The whole point of having a control group is to compare verum and control. The other point of importance is that it would have been crucial to verify whether patients were able to tell the verum from the sham intervention. If patients were able to tell, they would no longer be blinded and the placebo effect would have not been accounted for. A third point of relevance might be that the study seems tiny and far too small for drawing general conclusions about the value of OVM.
_________________________
I have now seen the protocol of the paper – thanks for making it available – and might add the following points to the discussion:
- The sham treatment consisted of “light touches over the different parts of the abdomen, without any deep mobilization or movement. The osteopath applied her hands over the same points with the
same duration as in OVM to give the patient the perception of being treated.” It is likely that patients in the control group could have guessed that they were sham-treated. - The stats issue cannot be resolved on the basis of just the protocol.
- “To assess patients’ blinding to treatment allocation, patients are asked post treatment (six weeks after
the start of treatment) to report which study treatment they think that they received (OVM/SOVM). The effect of their reports on outcome will be examined in explorative analysis.” As I have no
access to the results, I still do not know whether blinding was successful.
The General Chiropractic Council (GCC) “regulates chiropractors in the UK to ensure the safety of patients undergoing chiropractic treatment”. One might have assumed that they thus fulfill the important role of controlling the profession. Yet, one would have assumed wrongly. Instead of controlling, the GCC usually prefers promoting the profession. Their recent Chiropractic Patient Satisfaction and Experience is a good example. Let me show you several important sections of this document:
The outcomes reported here highlight two key findings:
• Overwhelmingly, chiropractic patients report high levels of satisfaction and positive experiences with their care. This was true both in the literature that examined international patient cohorts as well as the specific data collected from UK based chiropractic patients.
• A strong therapeutic relationship and good communication between patient and chiropractor underpins high satisfaction scores and a positive experience. This was confirmed both in the international literature and through both quantitative and qualitative analysis of specific data collected from UK based chiropractic patients.
Conclusion
This report shows that both existing literature and de novo data collection from patients receiving chiropractic care in the UK highlight excellent perceived experience and high satisfaction with such care.
Factors such as therapeutic alliance and communication are strongly associated with these positive perceptions by patients although other factors such as treatment beliefs were also significantly associated with satisfaction scores.
Recommendations
• To offer the highest quality of care, both in terms of clinical outcomes and patient experience, chiropractors should be explicitly skilled at curating excellent therapeutic alliances and communication with patients.
• Such skills and competences within chiropractic care delivery should receive higher visibility within the chiropractic profession generally and more specifically through advocacy within leading institutions and core emphasis within chiropractic curricula.
__________________________
By changing a few words, I have adapted the above excerpts to become a Customer Satisfaction and Experience Report of a fictitious hamburger joint published by the Hamburger General Council (HGC) of Great Britain which regulates hamburger joints in the UK to ensure the safety of consumers undergoing hamburger nutrition:
The outcomes reported here highlight two key findings:
• Overwhelmingly, customers report high levels of satisfaction and positive experiences with their restaurant. This was true both in the literature that examined international consumer cohorts as well as the specific data collected from UK based customers.
• A strong professional relationship and good communication between customer and service personell underpins high satisfaction scores and a positive experience. This was confirmed both in the international literature and through both quantitative and qualitative analysis of specific data collected from UK based hamburger consumers.
Conclusion
This report shows that both existing literature and de novo data collection from consumers eating hamburgers in the UK highlight excellent perceived experience and high satisfaction with such service.
Factors such as personal alliance and communication are strongly associated with these positive perceptions by consumers although other factors such as appetite were also significantly associated with satisfaction scores.
Recommendations
• To offer the highest quality of service, both in terms of profit and patient experience, hamburger vendors should be explicitly skilled at curating excellent professional alliances and communication with customers.
• Such skills and competences within hamburger delivery should receive higher visibility within the gastronomic trade generally and more specifically through advocacy within leading institutions and core emphasis within servers’ curricula.
___________________________
If you get the impression that I am taking the Mickey of the GCC, you are not mistaken. Yet, this post also has slightly more serious purposes. I wanted to 1) show how, in the chiropractic profession, pure BS is often disguised as research, and 2) question whether the GCC is fit for purpose.
On a more constructive note: there are many open questions that urgently need addressing in the realm of chiropractic (e.g. do chiropractors more good than harm?). I, therefore, suggest that the GCC stops publishing idiotic promotional documents disguised as research and gets on with its responsibilities.
I have to admit that I do not regularly read the DMZ, a German paper. In fact, until a minute ago, I did not know it existed. Nor do I know Anton Aeberhard. I saw his DMZ homeopathy article on the Internet and find it excellent; so much so that I translated parts of it for you:
… Because this pseudoscience is considered by some people to be an effective alternative to conventional medicine, it is important to understand the potential dangers and risks of homeopathy…
Homeopathy is based on the principle of the rule of similars and extreme dilution of substances. However, there is no scientific evidence that homeopathic remedies have any therapeutic effect beyond the placebo effect. Most studies that purport to show efficacy are methodologically flawed. Homeopathy contradicts fundamental principles of biology, chemistry, and physics. It is therefore irresponsible to consider this practice a legitimate medical treatment.
One of the greatest and real dangers of homeopathy is that it can cause people to refuse or delay effective medical treatments. By believing in homeopathic remedies, life-threatening conditions such as cancer, heart disease, or infections may not be treated appropriately. This can lead to worsening health conditions and increase the risk of complications or even death…
Conclusion I
Homeopathy is a pseudoscientific practice based on outdated principles and a lack of scientific evidence. The dangers of this practice should not be underestimated. It can cause people to reject or delay effective medical treatments, which can endanger their health and lives. It is important to make informed decisions about health care and to rely on evidence-based medicine to provide the best possible treatment and care.
Conclusion II.
Homeopathy is a joke.
________________________
Thank you Anton Aeberhard!
It is not often that we find a journalist who has the courage to defy the demand for ‘balance’. In the case of clear nonsensical issues, this demand becomes a demand for misleading people, a demand for FALSE balance!
When a journalist writes about the planet, he does not require a representative of the FLAT EARTH SOCIETY to add his views. Similarly, when someone writes about homeopathy, there is no need to interview the chair of a homeopaths’ association saying: “But we have 200 years of experience and we therefore know it works…”
Lumbosacral Radicular Syndrome (LSRS) is a condition characterized by pain radiating in one or more dermatomes (Radicular Pain) and/or the presence of neurological impairments (Radiculopathy). So far, different reviews have investigated the effect of HVLA (high-velocity low-amplitude) spinal manipulations in LSRS. However, these studies included ‘mixed’ population samples (LBP patients with or without LSRS) and treatments other than HVLA spinal manipulations (e.g., mobilisation, soft tissue treatment, etc.). Hence, the efficacy of HVLAT in LSRS is yet to be fully understood.
This review investigated the effect and safety of HVLATs on pain, levels of disability, and health-related quality of life in LSRS, as well as any possible adverse events.
Randomized clinical trials (RCTs) published in English in the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (PubMed), EMBASE, PEDro, and Web of Science were identified. RCTs on an adult population (18-65 years) with LSRS that compared HVLATs with other non-surgical treatments, sham spinal manipulation, or no intervention were considered. Two authors selected the studies, extracted the data, and assessed the methodological quality through the ‘Risk of Bias (RoB) Tool 2.0’ and the certainty of the evidence through the ‘GRADE tool’. A meta-analysis was performed to quantify the effect of HVLA on pain levels.
A total of 308 records were retrieved from the search strings. Only two studies met the inclusion criteria. Both studies were at high RoB. Two meta-analyses were performed for low back and leg pain levels. HVLA seemed to reduce the levels of low back (MD = -1.48; 95% CI = -2.45, -0.50) and lower limb (MD = -2.36; 95% CI = -3.28, -1.44) pain compared to other conservative treatments, at three months after treatment. However, high heterogeneity was found (I² = 0.0%, p = 0.735). Besides, their certainty of the evidence was ‘very low’. No adverse events were reported.
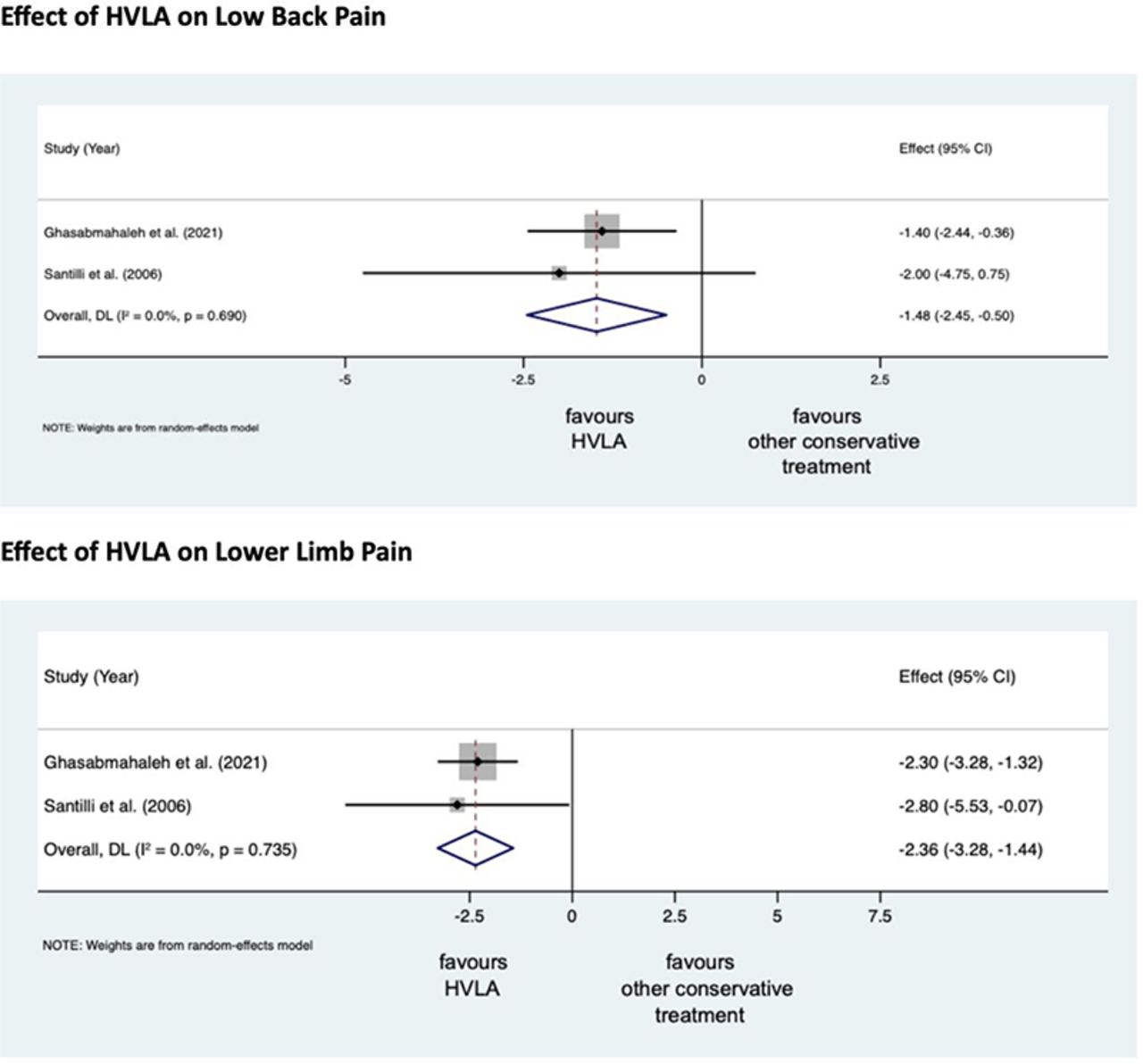
The authors stated that they cannot conclude whether HVLA spinal manipulations can be helpful for the treatment of LSRS or not. Future high-quality RCTs are needed to establish the actual effect of HVLA manipulation in this disease with adequate sample size and LSRS definition.
Chiropractors earn their living by applying HVLA thrusts to patients suffering from LSRS. One would therefore have assumed that the question of efficacy has been extensively researched and conclusively answered. It seems that one would have assumed wrongly!
Now that this is (yet again) in the open, I wonder whether chiropractors will, in the future, tell their patients while obtaining informed consent: “I plan to give you a treatment for which sound evidence is not available; it can also cause harm; and, of course, it will cost you – I hope you don’t mind.”
This systematic review was aimed at determining if there has been a change in the reporting of adverse events associated with spinal manipulation in randomized clinical trials (RCTs) since 2016.
Databases were searched from March 2016 to May 2022: MEDLINE (Ovid), Embase, CINAHL, ICL, PEDro, and Cochrane Library. The following search terms and their derivatives were adapted for each platform: spinal manipulation; chiropractic; osteopathy; physiotherapy; naprapathy; medical manipulation and clinical trial.
Domains of interest (pertaining to adverse events) included: completeness and location of reporting; nomenclature and description; spinal location and practitioner delivering manipulation; methodological quality of the studies and details of the publishing journal. Frequencies and proportions of studies reporting on each of these domains were calculated. Univariable and multivariable logistic regression models were fitted to examine the effect of potential predictors on the likelihood of studies reporting on adverse events.
There were 5399 records identified by the electronic searches, of which 154 (2.9%) were included in the analysis. Of these, 94 (61.0%) reported adverse events with only 23.4% providing an explicit description of what constituted an adverse event. Reporting of adverse events in the abstract had increased (n=29, 30.9%) while reporting in the results section had decreased (n=83, 88.3%) over the past 6 years. Spinal manipulation was delivered to 7518 participants in the included studies. No serious adverse events were reported in any of these studies.
The authors concluded that, while the current level of reporting of adverse events associated with spinal manipulation in RCTs has increased since our 2016 publication on the same topic, the level remains low and inconsistent with established standards. As such, it is imperative for authors, journal editors and administrators of clinical trial registries to ensure there is more balanced reporting of both benefits and harms in RCTs involving spinal manipulation.
In fact, it is an ethical imperative to accurately report adverse effects. Not reporting adverse effects amounts to a violation of medical research ethics. Adverse effects of spinal manipulation occur in about 50% of all patients. This means that investigators reporting significantly lower figures are likely guilty of under-reporting. And under-reporting of adverse events is also a breach of ethical standards.
My conclusion thus is that the vast majority of trials of spinal manipulation are unethical and should be discarded.
This study investigated the potential benefits of auricular point acupressure on cerebrovascular function and stroke prevention among adults with a high risk of stroke.
A randomized controlled study was performed with 105 adults at high risk for stroke between March and July 2021. Participants were randomly allocated to receive either
- auricular point acupressure with basic lifestyle interventions (n = 53) or
- basic lifestyle interventions alone (n = 52) for 2 weeks.
The primary outcome was the kinematic and dynamic indices of cerebrovascular function, as well as the CVHP score at week 2, measured by the Doppler ultrasonography and pressure transducer on carotids.
Of the 105 patients, 86 finished the study. At week 2, the auricular point acupressure therapy with lifestyle intervention group had higher kinematic indices, cerebrovascular hemodynamic parameters score, and lower dynamic indices than the lifestyle intervention group.
The authors concluded that ccerebrovascular function and cerebrovascular hemodynamic parameters score were greater improved among the participants undergoing auricular point acupressure combined with lifestyle interventions than lifestyle interventions alone. Hence, the auricular point acupressure can assist the stroke prevention.
Acupuncture is a doubtful therapy.
Acupressure is even more questionable.
Ear acupressure is outright implausible.
The authors discuss that the physiological mechanism underlying the effect of APA therapy on cerebrovascular hemodynamic function is not fully understood at present. There may be two possible explanations.
- First, a previous study has demonstrated that auricular acupuncture can directly increase mean blood flow velocity in the middle cerebral artery.
- Second, cerebrovascular hemodynamic function is indirectly influenced by the effect of APA therapy on blood pressure.
I think there is a much simpler explanation: the observed effects are directly or indirectly due to placebo. As regular listeners of this blog know only too well by now, the A+B versus B study design cannot account for placebo effects. Sadly, the authors of this study hardly discuss this explanation – that’s why they had to publish their findings in just about the worst SCAM journal of them all: EBCAM.
In the comments section, someone recently alerted us to a most remarkable article. I had a look at it and thought it would be a pity to let it pass without further comment. Here is the abstract:
There are many types of energy around us, including natural and artificial ones, the first of the ground energies due to the imbalance happened from the treatment of man with the ground (mines-the bases of huge buildings); the result of the Earth rotation, the result of geological faults, the flow of groundwater or energies resulting from other factors that result in radiations that harm organisms in general. Also we are continuously increasing the amount of carrier waves needed for the wireless technology of modern communication in the earth’s atmosphere every day. These electromagnetic waves are thousands of times stronger than the level used in the communication in our body cells. The problem is not the saturation of the earth’s atmosphere through quantity, but also a detrimental quality. Even people who avoid using high technology are not immune. No one is immune because these are carrier waves with penetrating properties. our immune systems are continuously trying to correct the distortion in the transfer of inner information in our body; very soon the threshold will be reached when a total collapse of our body defenses will take place. Balancing the activities of daily life, achieving harmony with our inner and outer environments, humanizing modern technology, integrating science and spirits, and discovering the unified scientific reality behind all religions is the work of some science such as Bio Geometry, Bio Design, Radiesthesia, …ext.
When one runs a blog on so-called alternative medicine (SCAM), it is almost inevitable to run into plenty of bullshit. Thus, over the years, I have gotten used to even the most compact versions of it. Yet, this paper – I do recommend you have a glance also at the full text – is truly outstanding.
In case there is someone amongst my readers who understands what the author wants to express, I would be most obliged to learn.
Numerous qualitative studies and a few quantitative studies have linked vaccine hesitancy or refusal with the belief in the efficacy of so-called alternative medicine (SCAM). Yet, large-scale data on this topic are scarce. In this study, the French researchers investigated the factors associated with the coverage rates of seven childhood vaccines or vaccine groups in the ninety-six metropolitan French departments. One of the factors investigated was the local interest in SCAM. In order to assess this interest, they built an Alternative Medicine Index based on departmental internet searches regarding SCAM—internet searches being a reliable indicator of the public’s actual interest in a given topic. They then conducted multiple regression analyses, which showed that this Index is a significant explanatory factor for the departmental variance in vaccination coverage rates, exceeding in importance the effect of other relevant local sociodemographic factors.
A further recent study from France adds to the picture. It presents the results of a survey conducted in July 2021 among a representative sample of the French mainland adult population (n = 3087). Using cluster analysis, the researchers identified five profiles of SCAM attitudes and found that even among the most pro-SCAM group, very few respondents disagreed with the idea that SCAM should only be used as a complement to conventional medicine. They then compared these SCAM attitudes to vaccine attitudes. Attitudes to SCAM had a distinct impact as well as a combined effect on attitudes to different vaccines and vaccines in general. They found that:
- attitudes to SCAM provide a very limited explanation of vaccine hesitancy;
- among the hesitant, pro-SCAM attitudes are often combined with other traits associated with vaccine hesitancy such as distrust of health agencies, radical political preferences, and low income.
Both SCAM endorsement and vaccine hesitancy are more prevalent among the socially disadvantaged. Drawing on these results, the researchers argue that, to better understand the relationship between SCAM and vaccine hesitancy, it is necessary to look at how both can reflect a lack of access and recourse to mainstream medicine and distrust of public institutions.
 The fact that the enthusiasm for SCAM is associated with vaccine hesitancy has been discussed on this blog many times before, e.g.:
The fact that the enthusiasm for SCAM is associated with vaccine hesitancy has been discussed on this blog many times before, e.g.:
- Preference of so-called alternative medicine predicts negative attitudes to vaccination
- What are the reasons for opposing COVID vaccinations?
- Intelligence, Religiosity, SCAM, Vaccination Hesitancy – are there links?
- More information on homeopaths’ and anthroposophic doctors’ attitude towards vaccinations
- The anti-vaccination movement is financed by the dietary supplement industry
- Sorry, I was wrong about homeopathy and vaccination
- The UK Society of Homeopaths, a hub of anti-vaccination activists?
- HOMEOPATHY = “the complete alternative to vaccination” ?!?!
- Are anthroposophy-enthusiasts for or against vaccinations?
- Far too many chiropractors believe that vaccinations do not have a positive effect on public health
- Naturopaths’ counselling against vaccinations could be criminally negligent
- HOMEOPATHS AGAINST VACCINATION: “The decision to vaccinate and how you implement that decision is yours and yours alone”
- Use of alternative medicine is associated with low vaccination rates
- Integrative medicine physicians tend to harbour anti-vaccination views
- Vaccination: chiropractors “espouse views which aren’t evidence based”
What seems fairly clear to me is that a cross-correlation exists: an attitude against modern medicine and the ‘scientific establishment’ determines both the enthusiasm for SCAM and the aversion to vaccination. What is, however, far from clear to me is what we could do about it.
Yes, better education seems important – and that’s precisely what I aim at achieving with this blog. Sadly, judging from some of the comments we receive, it does not seem crowned with much success.
Any other ideas?
“The decline of homeopathy, the ‘medicine’ that doesn’t cure anything” is the title of a remarkable article in EL PAIS of which I take the liberty of showing you a few key passages:
In the more than 200 years that have passed since its invention, no one has been able to prove that homeopathy is actually capable of curing anything with its alleged medicines that have no active ingredients…
…EL PAÍS reached out to some of its main promoters, such as the pharmaceutical company Boiron, leader in the sector; the Spanish Association of Homeopathy Pharmacists and the Spanish Society of Homeopathic Doctors. In the absence of a response from all three, the explanations are given by experts who are more critical of the discipline.
Many people who used to consume homeopathy were not even aware that this was the case. Fernando Frías, one of the activists who worked to undermine the discipline’s remaining prestige, recalls that people did not believe them when they were told that compounds with diluted Berlin Wall were sold to overcome the feelings of oppression and anxiety. This was actually commercialized under the premise that “like cures like”: if the Berlin Wall oppressed, a piece of it diluted in water should remedy it. “Many were under the impression that it was just a natural therapy and that we were making things up to attack it,” says Frías…
… There has been a lot of debate about how to regulate an alleged drug whose only effect is, in truth, the placebo effect. In 2001, the European Parliament issued a directive that covered its use in countries with a homeopathic tradition; sources explain that this happened due to the pressure exerted by both the industries and the governments of countries where pseudoscience is deep-rooted, such as France (where Boiron is headquartered) or Germany, where its consumption is much higher than in others, such as Spain.
“Having regard to the particular characteristics of these homeopathic medicinal products, such as the very low level of active principles they contain and the difficulty of applying to them the conventional statistical methods relating to clinical trials, it is desirable to provide a special, simplified registration procedure for those homeopathic medicinal products which are placed on the market without therapeutic indications in a pharmaceutical form and dosage which do not present a risk for the patient,” states the directive.
In its more than two centuries of history, this is not the first time that homeopathy loses ground. Still, Frías warns, it cannot be ruled out that at some point something will come up that will make it fashionable again. “Look at the example of chemtrails [the condensation trails left by airplanes that some conspiracy theorists believe are a way of poisoning the population from the air]. It seemed that no one remembered them anymore, but now they’re back,” he says. Frías cites the astrophysicist and disseminator Javier Armentia, who states that beliefs are like a rubber duck: no matter how much they sink, they always resurface. “Especially if there is money behind,” he adds.
______________________
As reported previously, homeopathy and other forms of so-called alternative medicine (SCAM) have come under fire in Spain. In 2017, ‘HOMEOPATHY PLUS‘ reported that “in a reversal of the 2015 Royal Legislative Decree, the Minister of Health has withdrawn homeopathic remedies and outlawed the practice in Spain’s national health services.” In 2018, more than 400 people signed an open letter triggered by the case of a cancer patient who died after preferring homeopathy to regular treatment. “Let’s be clear: pseudoscience kills,” begins the letter. Since then, the struggle of Spanish rational thinkers to stop misleading information about SCAM in general and homeopathy, in particular, has only intensified.
Spain is thus joining other European countries in opposing misinformation about homeopathy. Contrary to what some have claimed (for instance, in the comments section of this blog), most of the opponents do not want to restrict the public’s choice. People who wish to use homeopathy should be able to do so (but should pay for it themselves). However, the choice must be based on evidence-based information.