TCM
One theory as to how acupuncture works is that it increases endorphin levels in the brain. These ‘feel-good’ chemicals could theoretically be helpful for weaning alcohol-dependent people off alcohol. So, for once, we might have a (semi-) plausible mechanism as to how acupuncture could be clinically effective. But a ‘beautiful hypothesis’ does not necessarily mean acupuncture works for alcohol dependence. To answer this question, we need clinical trials or systematic reviews of clinical trials.
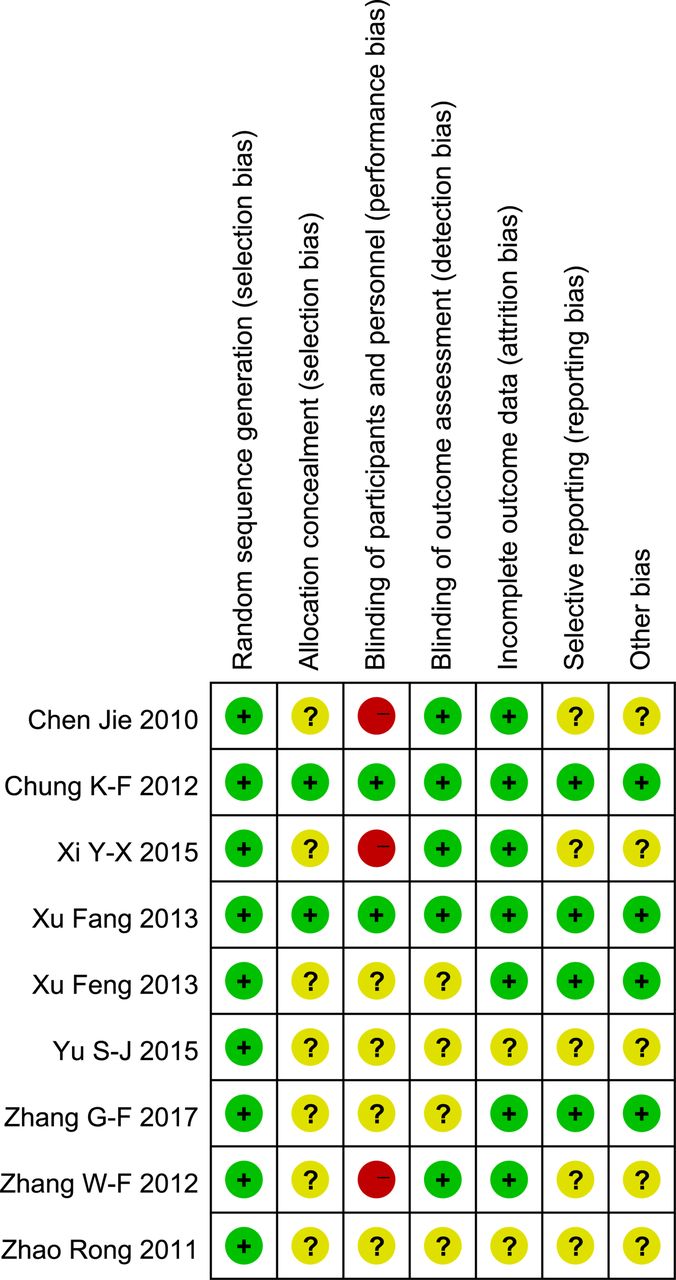
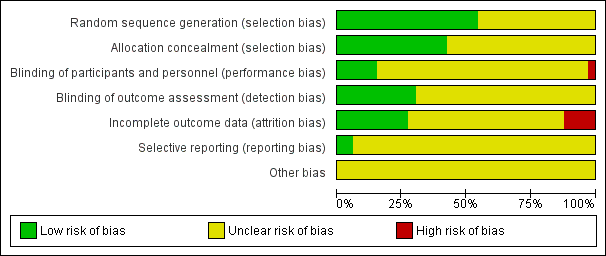
A new systematic review assessed the effects and safety of acupuncture for alcohol withdrawal syndrome (AWS). All RCTs of drug plus acupuncture or acupuncture alone for the treatment of AWS were included. Eleven RCTs with a total of 875 participants were included. In the acute phase, two trials reported no difference between drug plus acupuncture and drug plus sham acupuncture in the reduction of craving for alcohol; however, two positive trials reported that drug plus acupuncture was superior to drug alone in the alleviation of psychological symptoms. In the protracted phase, one trial reported acupuncture was superior to sham acupuncture in reducing the craving for alcohol, one trial reported no difference between acupuncture and drug (disulfiram), and one trial reported acupuncture was superior to sham acupuncture for the alleviation of psychological symptoms. Adverse effects were tolerable and not severe.
The authors concluded that there was no significant difference between acupuncture (plus drug) and sham acupuncture (plus drug) with respect to the primary outcome measure of craving for alcohol among participants with AWS, and no difference in completion rates (pooled results). There was limited evidence from individual trials that acupuncture may reduce alcohol craving in the protracted phase and help alleviate psychological symptoms; however, given concerns about the quantity and quality of included studies, further large-scale and well-conducted RCTs are needed.
There is little to add here. Perhaps just two short points:
1. The quality of the trials was poor; only one study of the 11 trials was of acceptable rigor. Here is its abstract:
We report clinical data on the efficacy of acupuncture for alcohol dependence. 503 patients whose primary substance of abuse was alcohol participated in this randomized, single blind, placebo controlled trial. Patients were assigned to either specific acupuncture, nonspecific acupuncture, symptom based acupuncture or convention treatment alone. Alcohol use was assessed, along with depression, anxiety, functional status, and preference for therapy. This article will focus on results pertaining to alcohol use. Significant improvement was shown on nearly all measures. There were few differences associated with treatment assignment and there were no treatment differences on alcohol use measures, although 49% of subjects reported acupuncture reduced their desire for alcohol. The placebo and preference for treatment measures did not materially effect the results. Generally, acupuncture was not found to make a significant contribution over and above that achieved by conventional treatment alone in reduction of alcohol use.
To me, this does not sound all that encouraging.
2. Of the 11 RCTs, 8 failed to report on adverse effects of acupuncture. In my book, this means these trials were in violation with basic research ethics.
My conclusion of all this: another ugly fact kills a beautiful hypothesis.
Acupuncture research does not have a good name; if it originates from China, even less so.
And this note in ‘ACUPUNCTURE IN MEDICINE’ is not likely to change this image:
Fang J, Keller CL, Chen L, et al. Effect of acupuncture and Chinese herbal medicine on subacute stroke outcomes: a single-centre randomised controlled trial. Acupuncture in Medicine Published online first 10 November 2017. doi: 10.1136/acupmed-2016-011167.
This article is retracted by the Editor-in-Chief on grounds of redundant publication.
The above article reports that a trial originally planned to be carried out at three hospitals was reduced to a single centre for reasons of cost. This is incorrect. The full three-centre trial was run and reported elsewhere (Scientific Reports 6, Article number: 25850 (2016) DOI: 10.1038/srep25850).
The Scientific Reports paper was accepted for publication prior to submission of the above paper to Acupuncture in Medicine. The third author takes responsibility for the mistake. All authors have agreed to this retraction.
The abstract of the paper in SCIENTIFIC REPORTS is here:
To determine whether integrative medicine rehabilitation (IMR) that combines conventional rehabilitation (CR) with acupuncture and Chinese herbal medicine has better effects for subacute stroke than CR alone, we conducted a multicenter randomized controlled trial that involved three hospitals in China. Three hundred sixty patients with subacute stroke were randomized into IMR and CR groups. The primary outcome was the Modified Barthel Index (MBI). The secondary outcomes were the National Institutes of Health Stroke Scale (NIHSS), the Fugl-Meyer Assessment (FMA), the mini-mental state examination (MMSE), the Montreal Cognitive Assessment (MoCA), Hamilton’s Depression Scale (HAMD), and the Self-Rating Depression Scale (SDS). All variables were evaluated at week 0 (baseline), week 4 (half-way of intervention), week 8 (after treatment) and week 20 (follow-up). In comparison with the CR group, the IMR group had significantly better improvements (P < 0.01 or P < 0.05) in all the primary and secondary outcomes. There were also significantly better changes from baseline in theses outcomes in the IMR group than in the CR group (P < 0.01). A low incidence of adverse events with mild symptoms was observed in the IMR group. We conclude that conventional rehabilitation combined with integrative medicine is safe and more effective for subacute stroke rehabilitation.
I find all this odd in several ways:
- The publication of the ACUPUNCTURE IN MEDICINE article does not seem to have been a ‘mistake‘ but plain scientific fraud, in my view.
- The paper in SCIENTIFIC REPORTS (SR) was published in May 2016. Therefore the reviewers and editor of AIM could and should have spotted the fraud.
- In the SR paper, the authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. As the authors were affiliated to three different departments of acupuncture, I feel this to be debatable.
What do you think?
Traditional Chinese Medicine (TCM) is the umbrella term for modalities historically used in ancient China. TCM includes many therapeutic and some diagnostic modalities. Even though, these modalities differ in many respects, they are claimed to have in common that they are based on assumptions most of which originate from Taoist philosophy:
- The human body is a miniature version of the universe.
- Harmony between the two opposing forces, yin and yang, means health.
- Disease is caused by an imbalance between these forces.
- Five elements—fire, earth, wood, metal, and water—symbolically represent all phenomena, including the stages of human life, and explain the functioning of the body and how it changes during disease.
- The vital energy, qi or chi, flows through the body in meridians, is essential for maintaining health.
TCM is a construct of Mao Zedong who lumped all historical Chinese treatments together under this umbrella and created the ‘barefoot doctor’ to practice TCM nationwide – not because he believed in TCM, but because China was desperately short of real doctors and needed at least a semblance of healthcare.
Over the past few years, China has been aggressively promoting TCM for expanding its global influence and for a share of the estimated US$50-billion global market (of products of dubious quality). A recent article in ‘Nature’ explains that the WHO’s governing body, the World Health Assembly, is set to adopt the 11th version of the organization’s global compendium — known as the International Statistical Classification of Diseases and Related Health Problems (ICD). For the first time, the ICD will include information about TCM. Chapter 26 of the ICD will feature a classification system on TCM, largely based not on science or facts, but on obsolete nonsense.
The WHO’s support applies to all traditional medicines, but its relationship with Chinese medicine, and with China, has grown especially close, in particular during the tenure of Margaret Chan, who ran the organization from 2006 to 2017 and made sure that several documents favourable to TCM were passed. The WHO’s declarations about traditional medicine are puzzling. Various of these WHO documents call for the integration of “traditional medicine, of proven quality, safety and efficacy”, while being silent as to which traditional medicines and diagnostics are proven. Wu Linlin, a WHO representative in the Beijing office, told Nature that the “WHO does not endorse particular traditional and complementary medicine procedures or remedies”.
But this is evidently not the case and in sharp contrast to the WHO’s actions in other areas. The agency provides, for instance, specific advice on what vaccines and drugs to use and what foods to avoid. With traditional medicines, however, such specifics are missing. The message therefore can only be that the WHO endorses TCM as safe and effective.
The evidence, however, tells us a different story. On this blog, we have repeatedly discussed that:
- the clinical trials of TCM are often of poor quality,
- there are several good reasons why one has to be very sceptical about research coming out of China,
- critics are silenced,
- in general, the evidence on TCM is neither positive nor trustworthy.
China’s drug regulator gets more than 230,000 reports of adverse effects from TCM each year, and Chinese herbal medicines carry multiple direct risks:
- one or more ingredients can be toxic,
- some have been shown to be contaminated with toxic materials such as heavy metals,
- others are adulterated with synthetic drugs such as steroids,
- others again can interact with prescription drugs taken concomitantly,
- and not to forget, the risk for endangered species.
To this, we have to add the indirect risk of employing useless treatments for otherwise treatable conditions.
In view of all this, the WHO’s endorsement of TCM and its obsolete concepts is not just not understandable, it is a dangerous step backwards and, in my view, even intolerable.
I remember reading this paper entitled ‘Comparison of acupuncture and other drugs for chronic constipation: A network meta-analysis’ when it first came out. I considered discussing it on my blog, but then decided against it for a range of reasons which I shall explain below. The abstract of the original meta-analysis is copied below:
The objective of this study was to compare the efficacy and side effects of acupuncture, sham acupuncture and drugs in the treatment of chronic constipation. Randomized controlled trials (RCTs) assessing the effects of acupuncture and drugs for chronic constipation were comprehensively retrieved from electronic databases (such as PubMed, Cochrane Library, Embase, CNKI, Wanfang Database, VIP Database and CBM) up to December 2017. Additional references were obtained from review articles. With quality evaluations and data extraction, a network meta-analysis (NMA) was performed using a random-effects model under a frequentist framework. A total of 40 studies (n = 11032) were included: 39 were high-quality studies and 1 was a low-quality study. NMA showed that (1) acupuncture improved the symptoms of chronic constipation more effectively than drugs; (2) the ranking of treatments in terms of efficacy in diarrhoea-predominant irritable bowel syndrome was acupuncture, polyethylene glycol, lactulose, linaclotide, lubiprostone, bisacodyl, prucalopride, sham acupuncture, tegaserod, and placebo; (3) the ranking of side effects were as follows: lactulose, lubiprostone, bisacodyl, polyethylene glycol, prucalopride, linaclotide, placebo and tegaserod; and (4) the most commonly used acupuncture point for chronic constipation was ST25. Acupuncture is more effective than drugs in improving chronic constipation and has the least side effects. In the future, large-scale randomized controlled trials are needed to prove this. Sham acupuncture may have curative effects that are greater than the placebo effect. In the future, it is necessary to perform high-quality studies to support this finding. Polyethylene glycol also has acceptable curative effects with fewer side effects than other drugs.
END OF 1st QUOTE
This meta-analysis has now been retracted. Here is what the journal editors have to say about the retraction:
After publication of this article [1], concerns were raised about the scientific validity of the meta-analysis and whether it provided a rigorous and accurate assessment of published clinical studies on the efficacy of acupuncture or drug-based interventions for improving chronic constipation. The PLOS ONE Editors re-assessed the article in collaboration with a member of our Editorial Board and noted several concerns including the following:
- Acupuncture and related terms are not mentioned in the literature search terms, there are no listed inclusion or exclusion criteria related to acupuncture, and the outcome measures were not clearly defined in terms of reproducible clinical measures.
- The study included acupuncture and electroacupuncture studies, though this was not clearly discussed or reported in the Title, Methods, or Results.
- In the “Routine paired meta-analysis” section, both acupuncture and sham acupuncture groups were reported as showing improvement in symptoms compared with placebo. This finding and its implications for the conclusions of the article were not discussed clearly.
- Several included studies did not meet the reported inclusion criteria requiring that studies use adult participants and assess treatments of >2 weeks in duration.
- Data extraction errors were identified by comparing the dataset used in the meta-analysis (S1 Table) with details reported in the original research articles. Errors included aspects of the study design such as the experimental groups included in the study, the number of study arms in the trial, number of participants, and treatment duration. There are also several errors in the Reference list.
- With regard to side effects, 22 out of 40 studies were noted as having reported side effects. It was not made clear whether side effects were assessed as outcome measures for the other 18 studies, i.e. did the authors collect data clarifying that there were no side effects or was this outcome measure not assessed or reported in the original article. Without this clarification the conclusion comparing side effect frequencies is not well supported.
- The network geometry presented in Fig 5 is not correct and misrepresents some of the study designs, for example showing two-arm studies as three-arm studies.
- The overall results of the meta-analysis are strongly reliant on the evidence comparing acupuncture versus lactulose treatment. Several of the trials that assessed this comparison were poorly reported, and the meta-analysis dataset pertaining to these trials contained data extraction errors. Furthermore, potential bias in studies assessing lactulose efficacy in acupuncture trials versus lactulose efficacy in other trials was not sufficiently addressed.
While some of the above issues could be addressed with additional clarifications and corrections to the text, the concerns about study inclusion, the accuracy with which the primary studies’ research designs and data were represented in the meta-analysis, and the reporting quality of included studies directly impact the validity and accuracy of the dataset underlying the meta-analysis. As a consequence, we consider that the overall conclusions of the study are not reliable. In light of these issues, the PLOS ONE Editors retract the article. We apologize that these issues were not adequately addressed during pre-publication peer review.
LZ disagreed with the retraction. YM and XD did not respond.
END OF 2nd QUOTE
Let me start by explaining why I initially decided not to discuss this paper on my blog. Already the first sentence of the abstract put me off, and an entire chorus of alarm-bells started ringing once I read further.
- A meta-analysis is not a ‘study’ in my book, and I am somewhat weary of researchers who employ odd or unprecise language.
- We all know (and I have discussed it repeatedly) that studies of acupuncture frequently fail to report adverse effects (in doing this, their authors violate research ethics!). So, how can it be a credible aim of a meta-analysis to compare side-effects in the absence of adequate reporting?
- The methodology of a network meta-analysis is complex and I know not a lot about it.
- Several things seemed ‘too good to be true’, for instance, the funnel-plot and the overall finding that acupuncture is the best of all therapeutic options.
- Looking at the references, I quickly confirmed my suspicion that most of the primary studies were in Chinese.
In retrospect, I am glad I did not tackle the task of criticising this paper; I would probably have made not nearly such a good job of it as PLOS ONE eventually did. But it was only after someone raised concerns that the paper was re-reviewed and all the defects outlined above came to light.
While some of my concerns listed above may have been trivial, my last point is the one that troubles me a lot. As it also related to dozens of Cochrane reviews which currently come out of China, it is worth our attention, I think. The problem, as I see it, is as follows:
- Chinese (acupuncture, TCM and perhaps also other) trials are almost invariably reporting positive findings, as we have discussed ad nauseam on this blog.
- Data fabrication seems to be rife in China.
- This means that there is good reason to be suspicious of such trials.
- Many of the reviews that currently flood the literature are based predominantly on primary studies published in Chinese.
- Unless one is able to read Chinese, there is no way of evaluating these papers.
- Therefore reviewers of journal submissions tend to rely on what the Chinese review authors write about the primary studies.
- As data fabrication seems to be rife in China, this trust might often not be justified.
- At the same time, Chinese researchers are VERY keen to publish in top Western journals (this is considered a great boost to their career).
- The consequence of all this is that reviews of this nature might be misleading, even if they are published in top journals.
I have been struggling with this problem for many years and have tried my best to alert people to it. However, it does not seem that my efforts had even the slightest success. The stream of such reviews has only increased and is now a true worry (at least for me). My suspicion – and I stress that it is merely that – is that, if one would rigorously re-evaluate these reviews, their majority would need to be retracted just as the above paper. That would mean that hundreds of papers would disappear because they are misleading, a thought that should give everyone interested in reliable evidence sleepless nights!
So, what can be done?
Personally, I now distrust all of these papers, but I admit, that is not a good, constructive solution. It would be better if Journal editors (including, of course, those at the Cochrane Collaboration) would allocate such submissions to reviewers who:
- are demonstrably able to conduct a CRITICAL analysis of the paper in question,
- can read Chinese,
- have no conflicts of interest.
In the case of an acupuncture review, this would narrow it down to perhaps just a handful of experts worldwide. This probably means that my suggestion is simply not feasible.
But what other choice do we have?
One could oblige the authors of all submissions to include full and authorised English translations of non-English articles. I think this might work, but it is, of course, tedious and expensive. In view of the size of the problem (I estimate that there must be around 1 000 reviews out there to which the problem applies), I do not see a better solution.
(I would truly be thankful, if someone had a better one and would tell us)
I have often cautioned my readers about the ‘evidence’ supporting acupuncture (and other alternative therapies). Rightly so, I think. Here is yet another warning.
This systematic review assessed the clinical effectiveness of acupuncture in the treatment of postpartum depression (PPD). Nine trials involving 653 women were selected. A meta-analysis demonstrated that the acupuncture group had a significantly greater overall effective rate compared with the control group. Moreover, acupuncture significantly increased oestradiol levels compared with the control group. Regarding the HAMD and EPDS scores, no difference was found between the two groups. The Chinese authors concluded that acupuncture appears to be effective for postpartum depression with respect to certain outcomes. However, the evidence thus far is inconclusive. Further high-quality RCTs following standardised guidelines with a low risk of bias are needed to confirm the effectiveness of acupuncture for postpartum depression.
What a conclusion!
What a review!
What a journal!
What evidence!
Let’s start with the conclusion: if the authors feel that the evidence is ‘inconclusive’, why do they state that ‘acupuncture appears to be effective for postpartum depression‘. To me this does simply not make sense!
Such oddities are abundant in the review. The abstract does not mention the fact that all trials were from China (published in Chinese which means that people who cannot read Chinese are unable to check any of the reported findings), and their majority was of very poor quality – two good reasons to discard the lot without further ado and conclude that there is no reliable evidence at all.
The authors also tell us very little about the treatments used in the control groups. In the paper, they state that “the control group needed to have received a placebo or any type of herb, drug and psychological intervention”. But was acupuncture better than all or any of these treatments? I could not find sufficient data in the paper to answer this question.
Moreover, only three trials seem to have bothered to mention adverse effects. Thus the majority of the studies were in breach of research ethics. No mention is made of this in the discussion.
In the paper, the authors re-state that “this meta-analysis showed that the acupuncture group had a significantly greater overall effective rate compared with the control group. Moreover, acupuncture significantly increased oestradiol levels compared with the control group.” This is, I think, highly misleading (see above).
Finally, let’s have a quick look at the journal ‘Acupuncture in Medicine’ (AiM). Even though it is published by the BMJ group (the reason for this phenomenon can be found here: “AiM is owned by the British Medical Acupuncture Society and published by BMJ”; this means that all BMAS-members automatically receive the journal which thus is a resounding commercial success), it is little more than a cult-newsletter. The editorial board is full of acupuncture enthusiasts, and the journal hardly ever publishes anything that is remotely critical of the wonderous myths of acupuncture.
My conclusion considering all this is as follows: we ought to be very careful before accepting any ‘evidence’ that is currently being published about the benefits of acupuncture, even if it superficially looks ok. More often than not, it turns out to be profoundly misleading, utterly useless and potentially harmful pseudo-evidence.
Reference
Acupunct Med. 2018 Jun 15. pii: acupmed-2017-011530. doi: 10.1136/acupmed-2017-011530. [Epub ahead of print]
Effectiveness of acupuncture in postpartum depression: a systematic review and meta-analysis.
Li S, Zhong W, Peng W, Jiang G.
Needle acupuncture in small children is controversial, not least because the evidence that it works is negative or weak, and because small children are unable to consent to the treatment. Yet it is recommended by some acupuncturists for infant colic. This, of course, begs the questions:
- Does the best evidence tell us that acupuncture is effective for infant colic?
- Are acupuncturists who recommend acupuncture for this condition responsible and ethical?
This systematic review and a blinding-test validation based on individual patient data from randomised controlled trials was aimed to assess its efficacy for treating infantile colic. Primary end-points were crying time at mid-treatment, at the end of treatment and at a 1-month follow-up. A 30-min mean difference (MD) in crying time between acupuncture and control was predefined as a clinically important difference. Pearson’s chi-squared test and the James and Bang indices were used to test the success of blinding of the outcome assessors [parents].
The investigators included three randomised controlled trials with data from 307 participants. Only one of the included trials obtained a successful blinding of the outcome assessors in both the acupuncture and control groups. The MD in crying time between acupuncture intervention and no acupuncture control was -24.9 min at mid-treatment, -11.4 min at the end of treatment and -11.8 min at the 4-week follow-up. The heterogeneity was negligible in all analyses. The statistically significant result at mid-treatment was lost when excluding the apparently unblinded study in a sensitivity analysis: MD -13.8 min. The registration of crying during treatment suggested more crying during acupuncture.
The authors concluded that percutaneous needle acupuncture treatments should not be recommended for infantile colic on a general basis.
The authors also provide this further comment: “Our blinding test validated IPD meta-analysis of minimal acupuncture treatments of infantile colic did not show clinically relevant effects in pain reduction as estimated by differences in crying time between needle acupuncture intervention and no acupuncture control. Analyses indicated that acupuncture treatment induced crying in many of the children. Caution should therefore be exercised in recommending potentially painful treatments with uncertain efficacy in infants. The studies are few, the analysis is made on small samples of individuals, and conclusions should be considered in this context. With this limitation in mind, our findings do not support the idea that percutaneous needle acupuncture should be recommended for treatment of infantile colic on a general basis.”
So, returning to the two questions that I listed above – what are the answers?
I think they must be:
- No.
- No.
Most people probably think of acupuncture as being used mainly as a therapy for pain control. But acupuncture is currently being promoted (and has traditionally been used) for all sorts of conditions. One of them is stroke. It is said to speed up recovery and even improve survival rates after such an event. There are plenty of studies on this subject, but their results are far from uniform. What is needed in this situation, is a rigorous summary of the evidence.
The authors of this Cochrane review wanted to assess whether acupuncture could reduce the proportion of people suffering death or dependency after acute ischaemic or haemorrhagic stroke. They included all randomized clinical trials (RCTs) of acupuncture started within 30 days after stroke onset. Acupuncture had to be compared with placebo or sham acupuncture or open control (no placebo) in people with acute ischaemic or haemorrhagic stroke, or both. Comparisons were made versus (1) all controls (open control or sham acupuncture), and (2) sham acupuncture controls.
The investigators included 33 RCTs with 3946 participants. Outcome data were available for up to 22 trials (2865 participants) that compared acupuncture with any control (open control or sham acupuncture) but for only 6 trials (668 participants) comparing acupuncture with sham acupuncture.
When compared with any control (11 trials with 1582 participants), findings of lower odds of death or dependency at the end of follow-up and over the long term (≥ three months) in the acupuncture group were uncertain and were not confirmed by trials comparing acupuncture with sham acupuncture. In trials comparing acupuncture with any control, findings that acupuncture was associated with increases in the global neurological deficit score and in the motor function score were uncertain. These findings were not confirmed in trials comparing acupuncture with sham acupuncture.Trials comparing acupuncture with any control showed little or no difference in death or institutional care or death at the end of follow-up.The incidence of adverse events (eg, pain, dizziness, faint) in the acupuncture arms of open and sham control trials was 6.2% (64/1037 participants), and 1.4% of these patients (14/1037 participants) discontinued acupuncture. When acupuncture was compared with sham acupuncture, findings for adverse events were uncertain.
The authors concluded that this updated review indicates that apparently improved outcomes with acupuncture in acute stroke are confounded by the risk of bias related to use of open controls. Adverse events related to acupuncture were reported to be minor and usually did not result in stopping treatment. Future studies are needed to confirm or refute any effects of acupuncture in acute stroke. Trials should clearly report the method of randomization, concealment of allocation, and whether blinding of participants, personnel, and outcome assessors was achieved, while paying close attention to the effects of acupuncture on long-term functional outcomes.
This Cochrane review seems to be thorough, but it is badly written (Cochrane reviewers: please don’t let this become the norm!). It contains some interesting facts. The majority of the studies came from China. This review confirmed the often very poor methodological quality of acupuncture trials which I have frequently mentioned before.
In particular, the RCTs originating from China were amongst those that most overtly lacked rigor, also a fact that has been discussed regularly on this blog.
For me, by far the most important finding of this review is that studies which at least partly control for placebo effects fail to show positive results. Depending on where you stand in the never-ending debate about acupuncture, this could lead to two dramatically different conclusions:
- If you are a believer in or earn your living from acupuncture, you might say that these results suggest that the trials were in some way insufficient and therefore they produced false-negative results.
- If you are a more reasonable observer, you might feel that these results show that acupuncture (for acute stroke) is a placebo therapy.
Regardless to which camp you belong, one thing seems to be certain: acupuncture for stroke (and other indications) is not supported by sound evidence. And that means, I think, that it is not responsible to use it in routine care.
Alternative practitioners practise highly diverse therapies. They seem to have nothing in common – except perhaps that ALL of them are allegedly stimulating our self-healing powers (and except that most proponents are latently or openly against vaccinations). And it is through these self-healing powers that the treatments in question cure anything and become a true panacea. When questioned what these incredible powers really are, most practitioners would (somewhat vaguely) name the immune system as the responsible mechanism. With this post, I intend to provide a short summary of the evidence on this issue:
Acupuncture: no good evidence to show stimulation of self-healing powers.
Aromatherapy: no good evidence to show stimulation of self-healing powers.
Bioresonance: no good evidence to show stimulation of self-healing powers.
Chiropractic: no good evidence to show stimulation of self-healing powers.
Detox: no good evidence to show stimulation of self-healing powers.
Energy healing: no good evidence to show stimulation of self-healing powers.
Feldenkrais: no good evidence to show stimulation of self-healing powers.
Gua sha: no good evidence to show stimulation of self-healing powers.
Herbal medicine: no good evidence to show stimulation of self-healing powers.
Homeopathy: no good evidence to show stimulation of self-healing powers.
Macrobiotics: no good evidence to show stimulation of self-healing powers.
Naturopathy: no good evidence to show stimulation of self-healing powers.
Osteopathy: no good evidence to show stimulation of self-healing powers.
Power bands: no good evidence to show stimulation of self-healing powers.
Reiki: no good evidence to show stimulation of self-healing powers.
Reflexology: no good evidence to show stimulation of self-healing powers.
Shiatsu: no good evidence to show stimulation of self-healing powers.
Tai chi: no good evidence to show stimulation of self-healing powers.
TCM: no good evidence to show stimulation of self-healing powers.
Vibrational therapy: no good evidence to show stimulation of self-healing powers.
Vaccinations: very good evidence to show stimulation of self-healing powers.
THE END
My previous post praised the validity and trustworthiness of Cochrane reviews. This post continues in the same line.
Like osteoarthritis, acute stroke has been a condition for which acupuncture-fans prided themselves of being able to produce fairly good evidence. A Cochrane review of 2005, however, was inconclusive and concluded that the number of patients is too small to be certain whether acupuncture is effective for treatment of acute ischaemic or haemorrhagic stroke. Larger, methodologically-sound trials are required.
So, 13 years later, we do have more evidence, and it would be interesting to know what the best evidence tells us today. This new review will tell us because it is the update of the previous Cochrane Review originally published in 2005.
The authors sought randomized clinical trials (RCTs) of acupuncture started within 30 days from stroke onset compared with placebo or sham acupuncture or open control (no placebo) in people with acute ischemic or haemorrhagic stroke, or both. Needling into the skin was required for acupuncture. Comparisons were made versus (1) all controls (open control or sham acupuncture), and (2) sham acupuncture controls.
Two review authors applied the inclusion criteria, assessed trial quality and risk of bias, and extracted data independently. They contacted study authors to ask for missing data and assessed the quality of the evidence by using the GRADE approach. The primary outcome was defined as death or dependency at the end of follow-up.
In total, 33 RCTs with 3946 participants were included. Twenty new trials with 2780 participants had been completed since the previous review. Outcome data were available for up to 22 trials (2865 participants) that compared acupuncture with any control (open control or sham acupuncture) but for only six trials (668 participants) that compared acupuncture with sham acupuncture control. The authors downgraded the evidence to low or very low quality because of risk of bias in included studies, inconsistency in the acupuncture intervention and outcome measures, and imprecision in effect estimates.
When compared with any control (11 trials with 1582 participants), findings of lower odds of death or dependency at the end of follow-up and over the long term (≥ three months) in the acupuncture group were uncertain (odds ratio [OR] 0.61, 95% confidence interval [CI] 0.46 to 0.79; very low-quality evidence; and OR 0.67, 95% CI 0.53 to 0.85; eight trials with 1436 participants; very low-quality evidence, respectively) and were not confirmed by trials comparing acupuncture with sham acupuncture (OR 0.71, 95% CI 0.43 to 1.18; low-quality evidence; and OR 0.67, 95% CI 0.40 to 1.12; low-quality evidence, respectively).In trials comparing acupuncture with any control, findings that acupuncture was associated with increases in the global neurological deficit score and in the motor function score were uncertain (standardized mean difference [SMD] 0.84, 95% CI 0.36 to 1.32; 12 trials with 1086 participants; very low-quality evidence; and SMD 1.08, 95% CI 0.45 to 1.71; 11 trials with 895 participants; very low-quality evidence).
These findings were not confirmed in trials comparing acupuncture with sham acupuncture (SMD 0.01, 95% CI -0.55 to 0.57; low-quality evidence; and SMD 0.10, 95% CI -0.38 to 0.17; low-quality evidence, respectively).Trials comparing acupuncture with any control reported little or no difference in death or institutional care at the end of follow-up (OR 0.78, 95% CI 0.54 to 1.12; five trials with 1120 participants; low-quality evidence), death within the first two weeks (OR 0.91, 95% CI 0.33 to 2.55; 18 trials with 1612 participants; low-quality evidence), or death at the end of follow-up (OR 1.08, 95% CI 0.74 to 1.58; 22 trials with 2865 participants; low-quality evidence).
The incidence of adverse events (eg, pain, dizziness, fainting) in the acupuncture arms of open and sham control trials was 6.2% (64/1037 participants), and 1.4% of these (14/1037 participants) discontinued acupuncture. When acupuncture was compared with sham acupuncture, findings for adverse events were uncertain (OR 0.58, 95% CI 0.29 to 1.16; five trials with 576 participants; low-quality evidence).
The authors concluded that this updated review indicates that apparently improved outcomes with acupuncture in acute stroke are confounded by the risk of bias related to use of open controls. Adverse events related to acupuncture were reported to be minor and usually did not result in stopping treatment. Future studies are needed to confirm or refute any effects of acupuncture in acute stroke. Trials should clearly report the method of randomization, concealment of allocation, and whether blinding of participants, personnel, and outcome assessors was achieved, while paying close attention to the effects of acupuncture on long-term functional outcomes.
These cautious conclusions might be explained by the fact that Chinese researchers are reluctant to state anything overtly negative about any TCM therapy. Recently, one expert who spoke out was even imprisoned for criticising a TCM product! But in truth, this review really shows that acupuncture has no convincing effect in acute stroke.
And for me, this conclusion is fascinating. I have been involved in acupuncture/stroke research since the early 1990s.
Our RCT produced a resounding negative result concluding that acupuncture is not superior to sham treatment for recovery in activities of daily living and health-related quality of life after stroke, although there may be a limited effect on leg function in more severely affected patients.
Our 1996 systematic review concluded that the evidence that acupuncture is a useful adjunct for stroke rehabilitation is encouraging but not compelling.
By 2001, more data had become available but the conclusion became even less encouraging: there is no compelling evidence to show that acupuncture is effective in stroke rehabilitation.
Finally, by 2010, there were 10 RCT and we were able to do a meta-analysis of the data. We concluded that our meta-analyses of data from rigorous randomized sham-controlled trials did not show a positive effect of acupuncture as a treatment for functional recovery after stroke.
Yes, my reviews were on slightly different research questions. Yet, they do reveal how a critical assessment of the slowly emerging evidence had to arrive at more and more negative conclusions about the role of acupuncture in the management of stroke patients. For a long time, this message was in stark contrast to what acupuncture-fans were claiming. I wonder whether they will now finally change their mind.
I have said it often, and I say it again: I do like well-conducted systematic reviews; and Cochrane reviews are usually the best, i. e. most transparent, most thorough and least biased. Thus, I was pleased to see a new Cochrane review of acupuncture aimed at assessing the benefits and harms of acupuncture in patients with hip OA.
The authors included randomized controlled trials (RCTs) that compared acupuncture with sham acupuncture, another active treatment, or no specific treatment; and RCTs that evaluated acupuncture as an addition to another treatment. Major outcomes were pain and function at the short term (i.e. < 3 months after randomization) and adverse events.
Six RCTs with 413 participants were included. Four RCTs included only people with OA of the hip, and two included a mix of people with OA of the hip and knee. All RCTs included primarily older participants, with a mean age range from 61 to 67 years, and a mean duration of hip OA pain from two to eight years. Approximately two-thirds of participants were women. Two RCTs compared acupuncture versus sham acupuncture; the other four RCTs were not blinded. All results were evaluated at short-term (i.e. four to nine weeks after randomization).In the two RCTs that compared acupuncture to sham acupuncture, the sham acupuncture control interventions were judged believable, but each sham acupuncture intervention was also judged to have a risk of weak acupuncture-specific effects, due to placement of non-penetrating needles at the correct acupuncture points in one RCT, and the use of penetrating needles not inserted at the correct points in the other RCT. For these two sham-controlled RCTs, the risk of bias was low for all outcomes.
The combined analysis of two sham-controlled RCTs gave moderate quality evidence of little or no effect in reduction in pain for acupuncture relative to sham acupuncture. Due to the small sample sizes in the studies, the confidence interval includes both the possibility of moderate benefit and the possibility of no effect of acupuncture (120 participants; Standardized Mean Difference (SMD) -0.13, (95% Confidence Interval (CI) -0.49 to 0.22); 2.1 points greater improvement with acupuncture compared to sham acupuncture on 100 point scale (i.e., absolute percent change -2.1% (95% CI -7.9% to 3.6%)); relative percent change -4.1% (95% CI -15.6% to 7.0%)). Estimates of effect were similar for function (120 participants; SMD -0.15, (95% CI -0.51 to 0.21)). No pooled estimate, representative of the two sham-controlled RCTs, could be calculated or reported for the quality of life outcome.
The four other RCTs were unblinded comparative effectiveness RCTs, which compared (additional) acupuncture to four different active control treatments. There was low quality evidence that addition of acupuncture to the routine primary care that RCT participants were receiving from their physicians was associated with statistically significant and clinically relevant benefits, compared to the routine primary physician care alone, in pain (1 RCT; 137 participants; mean percent difference -22.9% (95% CI -29.2% to -16.6%); relative percent difference -46.5% (95% CI -59.3% to -33.7%)) and function (mean percent difference -19.0% (95% CI -24.41 to -13.59); relative percent difference -38.6% (95% CI -49.6% to -27.6%)). There was no statistically significant difference for mental quality of life and acupuncture showed a small, significant benefit for physical quality of life.
The effects of acupuncture compared with either advice plus exercise or NSAIDs are uncertain. The authors are also uncertain whether acupuncture plus patient education improves pain, function, and quality of life, when compared to patient education alone.
In general, the overall quality of the evidence for the four comparative effectiveness RCTs was low to very low, mainly due to the potential for biased reporting of patient-assessed outcomes due to lack of blinding and sparse data.
Information on safety was reported in 4 RCTs. Two RCTs reported minor side effects of acupuncture, which were primarily minor bruising, bleeding, or pain at needle insertion sites.
The authors concluded that acupuncture probably has little or no effect in reducing pain or improving function relative to sham acupuncture in people with hip osteoarthritis. Due to the small sample size in the studies, the confidence intervals include both the possibility of moderate benefits and the possibility of no effect of acupuncture. One unblinded trial found that acupuncture as an addition to routine primary physician care was associated with benefits on pain and function. However, these reported benefits are likely due at least partially to RCT participants’ greater expectations of benefit from acupuncture. Possible side effects associated with acupuncture treatment were minor.
This is an excellent review of data that (because of contradictions, methodological limitations, heterogeneity etc.) are not easy to evaluate fairly. The review shows that previous verdicts about acupuncture for osteoarthritis might have been too optimistic. Acupuncture has no or only very small specific therapeutic effects. As we have much better therapeutic options for this condition, it means that acupuncture can no longer be recommended as an effective therapy.
That surely must be big news in the little world of acupuncture!
I have been personally involved in several similar reviews:
In 1997, I concluded that the most rigorous studies suggest that acupuncture is not superior to sham-needling in reducing pain of osteoarthritis: both alleviate symptoms to roughly the same degree.
In 2006, the balance of evidence seemed to have shifted and more positive data had emerged; consequently our review concluded that sham-controlled RCTs suggest specific effects of acupuncture for pain control in patients with peripheral joint OA. Considering its favourable safety profile acupuncture seems an option worthy of consideration particularly for knee OA. Further studies are required particularly for manual or electro-acupuncture in hip OA.
Now, it seems that my initial conclusion of 1996 was more realistic. To me this is a fascinating highlight on the fact that in EBM, we change our minds based on the current best evidence. By contrast, in alternative medicine, as we have often lamented on this blog, minds do not easily change and all too often dogma seems to reign.
The new Cochrane review is important in several ways. Firstly, it affirms an appropriately high standard for such reviews. Secondly, it originates from a research team that has, in the past, been outspokenly pro-acupuncture; it is therefore unlikely that the largely negative findings were due to an anti-acupuncture bias. Thirdly – and most importantly – osteoarthritis has been THE condition for which even critical reviewers had to admit that there was at least some good, positive evidence.
It seems therefore, that yet again a beautiful theory has been slain by an ugly fact.