depression
‘CLAMP DOWN ON THE BOGUS SCIENCE OF HOMEOPATHY’ is the title of a comment by Oliver Klamm in The Times today. Here is the background to his article.
In September 2020, the website of Homeopathy UK, www.homeopathy-uk.org, featured a page titled “Conditions Directory” with text that stated “Please find below a list of conditions where homeopathy can help …” followed by a list of medical conditions that included depression, diabetes, infertility, psoriasis and asthma. When consumers clicked-through the links to the conditions listed on that page, they were taken to separate pages for each that contained anecdotal descriptions from doctors detailing how they had applied homeopathic methods to the relevant conditions.
The UK Advertising Standards Authority received a complainant that challenged whether the ad discouraged essential treatment for conditions for which medical supervision should be sought, namely depression, diabetes, infertility, psoriasis and asthma.
The response of ‘Homeopathy UK’ said that, as a registered charity, they sought to share information about homeopathy for the benefit of others, rather than for commercial gain, and that they would always recommend that patients seeking homeopathic care did so under the supervision of a qualified medical practitioner…
The ASA upheld the complaint and argued as follows:
The CAP Code required that marketers must not discourage essential treatment for conditions for which medical supervision should be sought. For example, they must not offer specific advice on, diagnosis or treatment for such conditions unless that advice, diagnosis or treatment was conducted under the supervision of a suitably qualified medical professional. The ad referred to “depression”, “diabetes”, “infertility”, “psoriasis” and “asthma”, which we considered were conditions for which medical supervision should be sought. Any advice, diagnosis or treatment, therefore, must be conducted under the supervision of a suitably qualified medical professional. We acknowledged that the articles had been written by GMC-registered doctors, who we considered would be suitably qualified to offer advice, diagnosis or treatment. However, we noted that the ad and the articles to which it linked referred to homeopathy in general, rather than treatment by a specific individual. We understood that there were no minimum professional qualifications required to practice homeopathy, which could result in consumers being advised, diagnosed, or treated for the conditions listed in the ad by a practitioner with no medical qualification. We therefore considered Homeopathy UK would not be able to demonstrate that all such treatment would be conducted under the supervision of a suitably qualified health professional.
Furthermore, we understood that, although elsewhere on the website there were links to specific clinics, not all treatment would be conducted under the supervision of a suitably qualified health professional across those clinics. Because Homeopathy UK had not supplied evidence that treatment would always be carried out by a suitably qualified health professional. Also, because reference to the conditions listed in the ad, and discussed in the related articles, could discourage consumers from seeking essential treatment under the supervision of a suitably qualified health professional, we concluded that the ad had breached the Code.
On that point the ad breached CAP Code (Edition 12) rule 12.2 (Medicines, medical devices, health-related products and beauty products).
The ad must not appear again in the form complained about. We told Homeopathy UK to ensure their future marketing communications did not to refer to conditions for which advice should be sought from suitably qualified health professionals.
___________________________
Depression, diabetes, and asthma have few things in common. Just two characteristics stand out, in my view:
- they are potentially fatal;
- homeopathy is ineffective in changing their natural history.
- It was therefore high time that the ASA stopped this criminally dangerous nonsense of deluded homeopaths.
The article by Oliver Klamm concludes with the following wise words about homeopathy:
“For public officials and opinion formers, the time for appeasing this dangerous quackery should be long past.”
Reflexology (originally called ‘zone therapy’ by its inventor) is a manual technique where pressure is applied to the sole of the patient’s foot. Reflexology is said to have its roots in ancient cultures. Its current popularity goes back to the US doctor William Fitzgerald (1872-1942) who did some research in the early 1900s and thought to have discovered that the human body is divided into 10 zones each of which is represented on the sole of the foot. Reflexologists thus drew maps of the sole of the foot where all the body’s organs are depicted. Numerous such maps have been published and, embarrassingly, they do not all agree with each other as to the location of our organs on the sole of our feet. By massaging specific zones which are assumed to be connected to specific organs, reflexologists believe to positively influence the function of these organs.
So, does reflexology do more good than harm?
The aim of this review was to conduct a systematic review, meta-analysis, and metaregression to determine the current best available evidence of the efficacy and safety of foot reflexology for adult depression, anxiety, and sleep quality.
Twenty-six studies could be included. The meta-analyses showed that foot reflexology intervention significantly improved adult depression, anxiety, and sleep quality. Metaregression revealed that an increase in total foot reflexology time and duration can significantly improve sleep quality.
The authors concluded that foot reflexology may provide additional nonpharmacotherapy intervention for adults suffering from depression, anxiety, or sleep disturbance. However, high quality and rigorous design RCTs in specific population, along with an increase in participants, and a long-term follow-up are recommended in the future.
Sounds good!
Finally a so-called alternative medicine (SCAM) that is backed by soild evidence!
Or perhaps not?
Here are a few concerns that lead me to doubt these conclusions:
- Most of the primary studies were of poor methodological quality.
- Most studies failed to mention adverse effects.
- Very few studies controlled for placebo effects.
- There was evidence of publication bias (negative studies tended to remain unpublished).
- Studies published in languages other than English were not considered.
- The authors fail to point out that a foot massage is, of course, agreeable (and thus may relieve a range of symptoms), but reflexology with all its weird assumptions is less than plausible.
- Many of the studies located by the authors were excluded for reasons that are less than clear.
The last point seems particularly puzzling. Our own trial, for instance, was excluded because, according to the review authors, it did not include relevant outcomes. However, our method secion makes it clear that the primary focus for this study was the subscores for anxiety and depression, which comprise four and seven items, respectively. As it happens, our study was negative.
Also cuirous is the fact that the authors did not mention our own 2011 systematic review of reflexology:
Reflexology is a popular form of complementary and alternative medicine (CAM). The aim of this update is to critically evaluate the evidence for or against the effectiveness of reflexology in patients with any type of medical condition. Six electronic databases were searched to identify all relevant randomised clinical trials (RCTs). Their methodological quality was assessed independently by the two reviewers using the Jadad score. Overall, 23 studies met all inclusion criteria. They related to a wide range of medical conditions. The methodological quality of the RCTs was often poor. Nine high quality RCTs generated negative findings; and five generated positive findings. Eight RCTs suggested that reflexology is effective for the following conditions: diabetes, premenstrual syndrome, cancer patients, multiple sclerosis, symptomatic idiopathic detrusor over-activity and dementia yet important caveats remain. It is concluded that the best clinical evidence does not demonstrate convincingly reflexology to be an effective treatment for any medical condition.
I wonder why!
Mindfulness is one of the 150 so-called alternative medicines (SCAMs) that I have evaluated in my recent book ‘Alternative Medicine: A Critical Assessment of 150 Modalities‘. Here is an excerpt from my text:
Mindfulness is a form of meditation which involves bringing one’s attention to experiences occurring in the present moment while sitting silently and paying attention to thoughts, sounds, the sensations of breathing or parts of the body.
-
- Many experts do not consider mindfulness to be an alternative therapy but see it as a set of psychological methods that have long become well-accepted, conventional treatments.
- There are several forms of mindfulness meditation; one of the best-known and most thoroughly researched is Mindfulness-Based Stress Reduction developed by Jon Kabat-Zinn (1944- ). It uses a combination of mindfulness meditation, body awareness, and yoga to help people become more mindful.
- Mindfulness programs are currently popular and have been widely adopted in schools, hospitals, and other settings. They are also being applied to initiatives such as for healthy aging, weight management, athletic performance enhancement, for children with special needs, and as a help during the perinatal period.
- Novices are advised to start with short periods of about 10 minutes of meditation practice per day. With regular practice, it becomes easier to keep the attention focused and the length of time spent practising can be extended.
- There has been much research interest in mindfulness, and many studies are now available. However, the quality of these trials is often poor which is one reason why the evidence is less clear than one would hope.
- Several systematic reviews have assessed mindfulness for various medical conditions, e. g.:
-
- A systematic review of mindfulness for chronic headaches concluded that, due to the low number, small scale and often high or unclear risk of bias of included randomized controlled trials, the results are imprecise; this may be consistent with either an important or negligible effect. Therefore, more rigorous trials with larger sample sizes are needed.[1]
- A systematic review of mindfulness for addictions found support for the effectiveness of the mindfulness-based interventions.[2]
- An overview included 26 reviews and found a substantially consistent picture… Improvements in depressive disorders, particularly recurrent major depression, were strongly supported. Evidence for other psychological conditions was limited by lack of data. In populations with physical conditions, the evidence for significant improvements in psychological well-being was clear, regardless of population or specific mindfulness intervention. Changes in physical health measures were inconclusive; however, pain acceptance and coping were improved.[3]
-
- Some reports have linked mindfulness to increasing fear and anxiety panic or “meltdowns” after treatments. However, these seem to be rare events; in general, mindfulness is considered to be a safe therapy.
[1] https://www.ncbi.nlm.nih.gov/pubmed/29863407
[2] https://www.ncbi.nlm.nih.gov/pubmed/29651257
[3] https://www.ncbi.nlm.nih.gov/pubmed/29306938
Now there is new evidence regarding the safety of Mindfulness, including an estimate of the incidence of adverse effects. An article in the NEW SCIENTIST warned that about one in 12 people who try meditation experience an unwanted negative effect, usually a worsening in depression or anxiety, or even the onset of these conditions for the first time, according to the first systematic review of the evidence. “For most people it works fine but it has undoubtedly been overhyped and it’s not universally benevolent,” says Miguel Farias at Coventry University in the UK, one of the researchers behind a paper which as yet is not available on-line.
Farias’s team combed through medical journals and found 55 relevant studies. Once the researchers had excluded those that had deliberately set out to find negative effects, they worked out the prevalence of people who experienced harms within each study and then calculated the average, adjusted for the study size, a common method in this kind of analysis. They found that about 8 per cent people who try meditation experience an unwanted effect. “People have experienced anything from an increase in anxiety up to panic attacks,” says Farias. They also found instances of psychosis or thoughts of suicide.
I will add a link to the original paper, once it has been published
The aim of this systematic review was to assess the efficacy of homeopathic remedies (HRs) in the treatment of mental disorders.
Italian psychiatrists performed a Medline/Embase search for studies written in English and published from any date to October 23, 2018. All randomized controlled trials enrolling patients with any psychiatric disorder and comparing HR with placebo, no treatment, or other psychotropic drugs were included.
A total of 212 studies were screened, 9 met all selection criteria and reported data on major depressive disorder (MDD) (n = 4), generalized anxiety disorder (n = 1), attention-deficit/hyperactivity disorder (n = 2), and premenstrual syndrome/dysphoric disorder (n = 2). Eight of 9 randomized controlled trials showed high risk of bias. Homeopathy showed greater efficacy in MDD compared with fluoxetine, and in premenstrual syndrome/dysphoric disorder compared with placebo, whereas no difference emerged between homeopathy and placebo in MDD and attention deficit/hyperactivity disorder.
The authors concluded that the available data on homeopathy in psychiatric disorders are insufficient to support their use in clinical practice.
In their discussion section, they also add an interesting note of caution: Ethical considerations should therefore prevent clinicians from recommending HRs, which have a cost either for patients or for health care systems, until when a sufficient amount of solid evidence becomes available. In addition, systematic reviews of randomized trials, if unavailable, are advisable for all medical conditions for which homeopathy is currently prescribed.
This is a rigorous, transparent and clear review which generates no surprises. Few critical thinkers would have expected a positive result. It also teaches us, I think, a valuable lesson about the difference between a rigorous and a flimsy review, between independent and biased research. In 2011, evidently pro-homeopathy authors published a paper of the latter kind. Here is its abstract:
Objective: To systematically review placebo-controlled randomized trials of homeopathy for psychiatric conditions.
Data sources: Eligible studies were identified using the following databases from database inception to April 2010: PubMed, CINAHL, PsycINFO, Hom-Inform, Cochrane CENTRAL, National Center for Complementary and Alternative Medicine grantee publications database, and ClinicalTrials.gov. Gray literature was also searched using Google, Google Scholar, the European Committee for Homeopathy, inquiries with homeopathic experts and manufacturers, and the bibliographic lists of included published studies and reviews. Search terms were as follows: (homeopath* or homoeopath*) and (placebo or sham) and (anxiety or panic or phobia or post-traumatic stress or PTSD or obsessive-compulsive disorder or fear or depress* or dysthym* or attention deficit hyperactivity or premenstrual syndrome or premenstrual disorder or premenstrual dysphoric disorder or traumatic brain injury or fibromyalgia or chronic fatigue syndrome or myalgic encephalitis or insomnia or sleep disturbance). Searches included only English-language literature that reported randomized controlled trials in humans.
Study selection: Trials were included if they met 7 criteria and were assessed for possible bias using the Scottish Intercollegiate Guidelines Network (SIGN) 50 guidelines. Overall assessments were made using the Grading of Recommendations Assessment, Development and Evaluation procedure. Identified studies were grouped into anxiety or stress, sleep or circadian rhythm complaints, premenstrual problems, attention-deficit/hyperactivity disorder, mild traumatic brain injury, and functional somatic syndromes.
Results: Twenty-five eligible studies were identified from an initial pool of 1,431. Study quality according to SIGN 50 criteria varied, with 6 assessed as good, 9 as fair, and 10 as poor. Outcome was unrelated to SIGN quality. Effect size could be calculated in 16 studies, and number needed to treat, in 10 studies. Efficacy was found for the functional somatic syndromes group (fibromyalgia and chronic fatigue syndrome), but not for anxiety or stress. For other disorders, homeopathy produced mixed effects. No placebo-controlled studies of depression were identified. Meaningful safety data were lacking in the reports, but the superficial findings suggested good tolerability of homeopathy. A funnel plot in 13 studies did not support publication bias (χ(2)(1) = 1.923, P = .166).
Conclusions: The database on studies of homeopathy and placebo in psychiatry is very limited, but results do not preclude the possibility of some benefit.
The two conclusions speak for themselves, I think. They should remind us that, although systematic reviews are in principle the most reliable source of evidence, it is still necessary to check the quality of the work and the independence of the worker.
Neurolinguistic programming (NLP) was developed in the mid-seventies. It is a so-called alternative therapy (SCAM) that is not easy to define. Those who started it and those involved in it use such vague language that NLP means different things to different people. One metaphor keeps recurring: NLP claims to help people change by teaching them to program their brains. We were given brains, we are told, without an instruction manual, and NLP offers a user-manual for the brain. Consciously or unconsciously, NLP is based on the assumptions that:
- the unconscious mind constantly influences our conscious thoughts and actions;
- Freud’s theories are correct;
- hypnotherapy is effective.

Wikipedia is more outspoken about it: Neuro-linguistic programming (NLP) is a pseudoscientific approach to communication, personal development, and psychotherapy…
Despite the fact that NLP is unproven (to say the least), the COLLEGE OF MEDICINE AND INTEGRATED HEALTH (COMAIH) is sufficiently impressed by NLP to offer a course for GPs and SCAM practitioners. Here is their announcement:
Neurolinguistic Healthcare in association with the College of Medicine brings you a 2-day Introduction to Hypnosis, Neurolinguistic Programming (NLP) and Neurolinguistic Healthcare (NLH). Dr Wong and Dr Akhtar who lead the course are Trainers in NLP and Hypnosis and GPs who apply their skills in daily practice within the 10-minute consultation. The course is suitable for both medical professionals and complementary therapists. This is a limited training event offered by them to share their years of knowledge and skills with you.
You will learn:
-
- A basic overview of NLP and the most useful aspects to use it to begin making effective changes in how you and the people you treat think and behave
- An understanding of the NLH model of the mind so that you understand the concepts of therapy using this mixed hypnosis/ NLP approach in relation to health.
- The ability to Hypnotise effectively in a very short period of time with practical experience – the ability to go through all the stages of hypnosis – the induction, deepening, therapy, and emergence, including rapid hypnosis techniques. (Hypnosis courses which are less practical often charge in excess of £2000 for this)
- Learn at least 3 therapeutic techniques, including the NLP therapeutic techniques which work much better in trance, so using and applying the skills you will learn in hypnosis
- Access to an online mentorship programme with Dr Akhtar or Dr Wong for 6 months and who will provide 3x30mins group webinar meetings after the course to ensure any remaining questions get answered and that you are actually going forth to apply these skills. (worth another £600 in value)
- Access to an online learning membership site with educational videos and other content like pain relief techniques, papers with therapeutic scripts, etc
This is an opportunity to learn a different way of helping people from doctors who target the 10-minute consultation with fast, effective formal hypnosis techniques and sleight-of-mouth. It is possible to make change happen in 10-minutes.
Note that attending this course will not make you a certified hypnotherapist, but confer you the skills you will learn to use personally and in the context of guided meditations and relaxations that are commonplace now.
And what evidence do I have for stating that NLP is unproven?
Is there an up-to-date and sound systematic review of NLP?
The answer is yes.
This systematic review of NLP included 10 experimental studies. Five studies were RCTs and five were uncontrolled pre-post studies. Targeted health conditions were anxiety disorders, weight maintenance, morning sickness, substance misuse, and claustrophobia during MRI scanning. NLP interventions were mainly delivered across 4-20 sessions although three were single session. Eighteen outcomes were reported and the RCT sample sizes ranged from 22 to 106. Four RCTs reported no significant between group differences with the fifth finding in favour of NLP. Three RCTs and five pre-post studies reported within group improvements. Risk of bias across all studies was high or uncertain.
The authors concluded that there is little evidence that NLP interventions improve health-related outcomes. This conclusion reflects the limited quantity and quality of NLP research, rather than robust evidence of no effect. There is currently insufficient evidence to support the allocation of NHS resources to NLP activities outside of research purposes.
Surprised?
I am not!
I did not expect the COMAIH to allow critical thinking to get in the way of quackery-promotion.
This post is dedicated to all who claim that I never discuss anything positive about so-called alternative medicine (SCAM).
Autogenic training is a therapy developed in the 1920s by the German psychiatrist Johannes Heinrich Schultz (1884 – 1970). It is an auto-hypnotic relaxation technique popular in Germany but less so other countries. (The lack of international appreciation of autogenic training might be related to Schultz’ well-documented Nazi past. In 1935, he published an essay which supported compulsory sterilization of men to eliminate hereditary illnesses. Later he was appointed deputy director of the Göring Institute in Berlin. Through this institute, he had an active role in the extermination of mentally handicapped individuals in the framework of the ‘Aktion T4’, the Nazi’s infamous euthanasia programme.)
Autogenic training consists of mental exercises using instructions directed at different parts of the body to control bodily perceptions, such as ‘my right foot feels warm’ or ‘my left arm feels heavy’. Patients tend to report an intense sense of relaxation during and after autogenic training. Autogenic training is taught in a series of lessons by a qualified instructor.
Autogenic training should be practised regularly and does not require further supervision. It is thus an inexpensive therapy. The technique is claimed to help for a range of (mostly stress-related) conditions. However, the evidence from clinical trials is scarce and, not least due to methodological problems, less than convincing.
This systematic review was conducted to evaluate the effectiveness of autogenic training on stress responses. A total 11 studies were included in a meta-analysis. They showed that autogenic training decreased anxiety and depression, and increased the high frequency of heart rate variability as well as a reduction of anxiety score by 1.37 points (n=85, SMD=-1.37: 95% CI -2.07 to -0.67), in the studies on short-term intervention targeting healthy adults.For depression, a reduction was noted of the symptom score by 0.29 point (n=327, SMD=-0.29: 95% CI -0.50 to -0.07) in the studies on long term intervention targeting the patient group.
The authors concluded that autogenic training is effective for adults’ stress management, and nurses will be able to effectively perform autogenic training programs for workers’ stress relief at the workplace.
I cannot access the full article because it was published in Korean. Nevertheless, I feel that the conclusions are probably correct.
Why?
Because I know (most of) the primary studies and three of the RCTs are my own.
(Yet, some of my critics continue to claim that I never conducted any positive studies of SCAM)
The ‘College of Medicine and Integrated Health’ (CMIH) has been the subject of several previous blog posts (see for instance here, here and here). Recently, they have come up with something new that, in my view, deserves a further comment.
The new ‘SELF CARE TOOL KIT’ began, according to the CMIH, in 2009 with a national multi-centre project commissioned by the UK Department of Health, to consider the best way to integrate self care into family practice. The project involved two large family health centres and two university departments. One output was the Self Care Library (SCL).
The Self Care Library (SCL) is an online patient resource providing free evidence-based information about self-care. The funding for the SCL did, however, not survive, and the facility was assigned to the CMIH. Thanks to funding from ‘Pukka Herbs Vitamins, Herbal Remedies & Health Supplements‘, the CMIH was able to transfer the content and to begin updating entries. Simon Mills, the coordinator of the original project who is now employed by Pukka, has led this transformation and helped the College set up the new parent portal, Our Health Directory.
The Self Care Toolkit is thus the new SCL. All concerned with this project are experienced in clinical practice and can separate the theory from real life needs. We all have academic lives as well so can be hard-nosed with the evidence base as well.
_______________________________________________________________
The above text is essentially based on the information provided by the CMIH. A few critical remarks and clarifications might therefore be in order:
- What does ‘separate the theory from real life needs’ mean? Does it mean that the scientific evidence can be interpreted liberally (see below)?
- Is it a good idea to have a commercial sponsor for such a project?
- Is it wise that the main person in charge is on the payroll of a manufacturer of dietary supplements?
- Is there any oversight to minimise undue bias and prevent the public from being misled?
- Is it really true that all people involved have academic lives? Simon Mills (who once was a member of my team) has no longer an academic appointment, as far as I know.
But, you are right, these are perhaps mere trivialities. Let’s see what the ‘Self Care Tool Kit’ actually delivers. I have chosen the entry on DEPRESSION to check its validity. Here it is:
_______________________________________________________________
It isn’t likely that taking extra vitamins will make much difference to low mood or depression. It is true that many people don’t get quite enough B, C and D vitamins in their food. And it’s also true that the brain and nervous system need these vitamins. Because they don’t get stored in the body, our daily diet has to supply them. Research has shown that people with low blood levels of the B vitamin folic acid are more likely to be depressed and less likely to do well on anti-depressant medicines. So, if you are eating a very poor diet, taking extra vitamins just might help. It’s also worth remembering that alcohol, refined sugars, nicotine and caffeine all take these vitamins out of the body. Yet most people who feel depressed probably won’t benefit from taking vitamins alone. To ensure that you get a good balance of these vitamins, try to eat more whole-foods, fruits, vegetables, nuts and seeds.
Some people say that taking high doses of vitamin C (1-2 g and more a day) helps lift their mood. There is a little research to support this and none showing that high doses of vitamin C actually help clinical depression. Vitamin C levels fall after surgery or inflammatory disease. The body needs more vitamin C when coping with stress, pregnancy and breast feeding. Aspirin, tetracycline and contraceptive pills take vitamin C out of the body. Smokers also need extra vitamin C because nicotine removes it. Fresh fruit and vegetables are the best sources of vitamin C.
Doctors are increasingly concerned about low vitamin D, especially in the Asian community. A lack of vitamin D can lead to depression. Oily fish and dairy products are good sources of vitamin D, and sunlight helps the body make vitamin D. Do you get enough sunshine and eat a good diet? It is estimated that worldwide over 1 billion people get too little vitamin D.
Evidence
Taking supplements of vitamins B and D might help some people, whose diet is poor, but more research is needed.
Safety
Very high doses of vitamins and minerals can upset the body and cause side-effects. Get medical advice if you intend to take large doses. To ensure that you get a good balance of these vitamins, try to eat more whole-foods, fruits, vegetables, nuts and seeds.
Cost
If your diet is poor and you don’t get into the sun, ask your doctor about a vitamin D blood test. If it’s normal, there’s no point in taking vitamin D. If it’s low, your GP will prescribe it for you or you can buy a vitamin D supplement.
___________________________________________________________________
In my view, this text begs several questions:
1) Am I right in thinking that phraseology such as the one below will encourage patients suffering from depression to try the supplements mentioned?
- people with low blood levels of the B vitamin folic acid are more likely to be depressed and less likely to do well on anti-depressant medicines..
- Some people say that taking high doses of vitamin C (1-2 g and more a day) helps lift their mood…
- There is a little research to support this and none showing that high doses of vitamin C actually help clinical depression…
- A lack of vitamin D can lead to depression.
- Taking supplements of vitamins B and D might help some people…
- … your GP will prescribe it for you or you can buy a vitamin D supplement.
2) How does that tally with the latest evidence? For instance:
- No significant reduction in depression was seen after vitamin D supplementation compared to placebo
- No additional effects from nutritional supplementation were detected
- Adding vitamin C to citalopram did not increase the efficacy of citalopram in MDD patients.
3) The CMIH state: ‘This site gives you information NOT medical advice.’ But, in view of the actual text above, is this true?
4) Depression is a life-threatening condition. Is there a risk that patients trust the CMHI’s (non-) advice and commit suicide because of its ineffectiveness?
5) Do Pukka, the sponsor of all this, happen to supply most of the self care remedies promoted in the ‘Self Care Tool Kit’?
The answer to the last question, I am afraid, is YES!
Homeopathy for depression? A previous review concluded that the evidence for the effectiveness of homeopathy in depression is limited due to lack of clinical trials of high quality. But that was 13 years ago. Perhaps the evidence has changed?
A new review aimed to assess the efficacy, effectiveness and safety of homeopathy in depression. Eighteen studies assessing homeopathy in depression were included. Two double-blind placebo-controlled trials of homeopathic medicinal products (HMPs) for depression were assessed.
- The first trial (N = 91) with high risk of bias found HMPs were non-inferior to fluoxetine at 4 and 8 weeks.
- The second trial (N = 133), with low risk of bias, found HMPs was comparable to fluoxetine and superior to placebo at 6 weeks.
The remaining research had unclear/high risk of bias. A non-placebo-controlled RCT found standardised treatment by homeopaths comparable to fluvoxamine; a cohort study of patients receiving treatment provided by GPs practising homeopathy reported significantly lower consumption of psychotropic drugs and improved depression; and patient-reported outcomes showed at least moderate improvement in 10 of 12 uncontrolled studies. Fourteen trials provided safety data. All adverse events were mild or moderate, and transient. No evidence suggested treatment was unsafe.
The authors concluded that limited evidence from two placebo-controlled double-blinded trials suggests HMPs might be comparable to antidepressants and superior to placebo in depression, and patients treated by homeopaths report improvement in depression. Overall, the evidence gives a potentially promising risk benefit ratio. There is a need for additional high quality studies.
I beg to differ!
What these data really show amounts to far less than the authors imply:
- The two ‘double-blind’ trials are next to meaningless. As equivalence studies they were far too small to produce meaningful results. Any decent review should discuss this fact in full detail. Moreover, these studies cannot have been double-blind, because the typical adverse-effects of anti-depressants would have ‘de-blinded’ the trial participants. Therefore, these results are almost certainly false-positive.
- The other studies are even less rigorous and therefore do also not allow positive conclusions.
This review was authored by known proponents of homeopathy. It is, in my view, an exercise in promotion rather than a piece of research. I very much doubt that a decent journal with a responsible peer-review system would have ever published such a biased paper – it had to appear in the infamous EUROPEAN JOURNAL OF INTEGRATIVE MEDICINE.
So what?
Who cares? No harm done!
Again, I beg to differ.
Why?
The conclusion that homeopathy has a ‘promising risk/benefit profile’ is frightfully dangerous and irresponsible. If seriously depressed patients follow it, many lives might be lost.
Yet again, we see that poor research has the potential to kill vulnerable individuals.
Aromatherapy usually involves the application of diluted essential (volatile) oils via a gentle massage of the body surface. The chemist Rene-Maurice Gattefosse (1881-1950) coined the term ‘aromatherapy’ after experiencing that lavender oil helped to cure a severe burn of his hand. In 1937, he published a book on the subject: Aromathérapie: Les Huiles Essentielles, Hormones Végétales. Later, the French surgeon Jean Valnet used essential oils to help heal soldiers’ wounds in World War II.
Aromatherapy is currently one of the most popular of all alternative therapies. The reason for its popularity seems simple: it is an agreeable, luxurious form of pampering. Whether it truly merits to be called a therapy is debatable.
The authors of this systematic review stated that they wanted to critically assess the effect of aromatherapy on the psychological symptoms as noted in the postmenopausal and elderly women. They conducted electronic literature searches and fount 4 trials that met their inclusion criteria. The findings demonstrated that aromatherapy massage significantly improves psychological symptoms in menopausal, elderly women as compared to controls. In one trial, aromatherapy massage was no more effective than the untreated group regarding their experience of symptoms such as nervousness.
The authors concluded that aromatherapy may be beneficial in attenuating the psychological symptoms that these women may experience, such as anxiety and depression, but it is not considered as an effective treatment to manage nervousness symptom among menopausal women. This finding should be observed in light of study limitations.
In the discussion section, the authors state that to the best of our knowledge, this is the first meta-analysis evaluating the effect of aromatherapy on the psychological symptoms. I believe that they might be mistaken. Here are two of my own papers (other researchers have published further reviews) on the subject:
- Aromatherapy is the therapeutic use of essential oil from herbs, flowers, and other plants. The aim of this overview was to provide an overview of systematic reviews evaluating the effectiveness of aromatherapy. We searched 12 electronic databases and our departmental files without restrictions of time or language. The methodological quality of all systematic reviews was evaluated independently by two authors. Of 201 potentially relevant publications, 10 met our inclusion criteria. Most of the systematic reviews were of poor methodological quality. The clinical subject areas were hypertension, depression, anxiety, pain relief, and dementia. For none of the conditions was the evidence convincing. Several SRs of aromatherapy have recently been published. Due to a number of caveats, the evidence is not sufficiently convincing that aromatherapy is an effective therapy for any condition.
- Aromatherapy is becoming increasingly popular; however there are few clear indications for its use. To systematically review the literature on aromatherapy in order to discover whether any clinical indication may be recommended for its use, computerised literature searches were performed to retrieve all randomised controlled trials of aromatherapy from the following databases: MEDLINE, EMBASE, British Nursing Index, CISCOM, and AMED. The methodological quality of the trials was assessed using the Jadad score. All trials were evaluated independently by both authors and data were extracted in a pre-defined, standardised fashion. Twelve trials were located: six of them had no independent replication; six related to the relaxing effects of aromatherapy combined with massage. These studies suggest that aromatherapy massage has a mild, transient anxiolytic effect. Based on a critical assessment of the six studies relating to relaxation, the effects of aromatherapy are probably not strong enough for it to be considered for the treatment of anxiety. The hypothesis that it is effective for any other indication is not supported by the findings of rigorous clinical trials.
Omitting previous research may be odd, but it is not a fatal flaw. What makes this review truly dismal is the fact that the authors fail to discuss the poor quality of the primary studies. They are of such deplorable rigor that one can really not draw any conclusion at all from them. I therefore find the conclusions of this new paper unacceptable and think that our statement (even though a few years old) is much more accurate: the evidence is not sufficiently convincing that aromatherapy is an effective therapy for any condition.
This systematic review included 18 studies assessing homeopathy in depression. Two double-blind placebo-controlled trials of homeopathic medicinal products (HMPs) for depression were assessed. The first trial (N = 91) with high risk of bias found HMPs were non-inferior to fluoxetine at 4 (p = 0.654) and 8 weeks (p = 0.965); whereas the second trial (N = 133), with low risk of bias, found HMPs was comparable to fluoxetine (p = 0.082) and superior to placebo (p < 0.005) at 6 weeks.
The remaining research had unclear/high risk of bias. A non-placebo-controlled RCT found standardised treatment by homeopaths comparable to fluvoxamine; a cohort study of patients receiving treatment provided by GPs practising homeopathy reported significantly lower consumption of psychotropic drugs and improved depression; and patient-reported outcomes showed at least moderate improvement in 10 of 12 uncontrolled studies. Fourteen trials provided safety data. All adverse events were mild or moderate, and transient. No evidence suggested treatment was unsafe.
The authors concluded that limited evidence from two placebo-controlled double-blinded trials suggests HMPs might be comparable to antidepressants and superior to placebo in depression, and patients treated by homeopaths report improvement in depression. Overall, the evidence gives a potentially promising risk benefit ratio. There is a need for additional high quality studies.
It is worth having a look at these two studies, I think.
The 1st (2011) study is from Brazil
Here is its abstract:
Homeopathy is a complementary and integrative medicine used in depression, The aim of this study is to investigate the non-inferiority and tolerability of individualized homeopathic medicines [Quinquagintamillesmial (Q-potencies)] in acute depression, using fluoxetine as active control. Ninety-one outpatients with moderate to severe depression were assigned to receive an individualized homeopathic medicine or fluoxetine 20 mg day−1 (up to 40 mg day−1) in a prospective, randomized, double-blind double-dummy 8-week, single-center trial. Primary efficacy measure was the analysis of the mean change in the Montgomery & Åsberg Depression Rating Scale (MADRS) depression scores, using a non-inferiority test with margin of 1.45. Secondary efficacy outcomes were response and remission rates. Tolerability was assessed with the side effect rating scale of the Scandinavian Society of Psychopharmacology. Mean MADRS scores differences were not significant at the 4th (P = .654) and 8th weeks (P = .965) of treatment. Non-inferiority of homeopathy was indicated because the upper limit of the confidence interval (CI) for mean difference in MADRS change was less than the non-inferiority margin: mean differences (homeopathy-fluoxetine) were −3.04 (95% CI −6.95, 0.86) and −2.4 (95% CI −6.05, 0.77) at 4th and 8th week, respectively. There were no significant differences between the percentages of response or remission rates in both groups. Tolerability: there were no significant differences between the side effects rates, although a higher percentage of patients treated with fluoxetine reported troublesome side effects and there was a trend toward greater treatment interruption for adverse effects in the fluoxetine group. This study illustrates the feasibility of randomized controlled double-blind trials of homeopathy in depression and indicates the non-inferiority of individualized homeopathic Q-potencies as compared to fluoxetine in acute treatment of outpatients with moderate to severe depression.
There are many important points to make about this trial:
- Contrary to what the reviewers claim, the trial had no placebo group.
- It was a double-dummy equivalence study comparing individualised homeopathy with the antidepressant fluoxetine.
- Fluoxetine might have been under-dosed (see below).
- Equivalence studies require large sample sizes, and with just 91 patients (only 55 of whom finished the study), this trial was underpowered which means the finding of equivalence is false positive.
- The authors noted that a higher percentage of troublesome adverse effects reported by patients receiving fluoxetine. This means that the trial was not double-blind; patients were able to tell by their side-effects which group they were in.
- The authors also state that more patients randomized to homeopathy than to fluoxetine were excluded due to worsening of their depressive symptoms. I think this confirms that homeopathy was ineffective.
The 2nd (2015) study is from Mexico
Here is its abstract:
Background: Perimenopausal period refers to the interval when women’s menstrual cycles become irregular and is characterized by an increased risk of depression. Use of homeopathy to treat depression is widespread but there is a lack of clinical trials about its efficacy in depression in peri- and postmenopausal women. The aim of this study was to assess efficacy and safety of individualized homeopathic treatment versus placebo and fluoxetine versus placebo in peri- and postmenopausal women with moderate to severe depression.
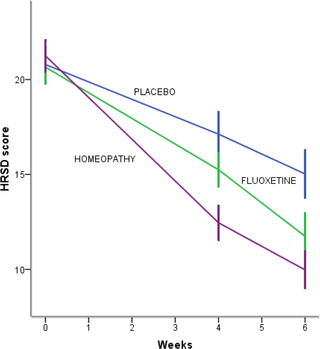
Methods/Design: A randomized, placebo-controlled, double-blind, double-dummy, superiority, three-arm trial with a 6 week follow-up study was conducted. The study was performed in a public research hospital in Mexico City in the outpatient service of homeopathy. One hundred thirty-three peri- and postmenopausal women diagnosed with major depression according to DSM-IV (moderate to severe intensity) were included. The outcomes were: change in the mean total score among groups on the 17-item Hamilton Rating Scale for Depression, Beck Depression Inventory and Greene Scale, after 6 weeks of treatment, response and remission rates, and safety. Efficacy data were analyzed in the intention-to-treat population (ANOVA with Bonferroni post-hoc test).
Results: After a 6-week treatment, homeopathic group was more effective than placebo by 5 points in Hamilton Scale. Response rate was 54.5% and remission rate, 15.9%. There was a significant difference among groups in response rate definition only, but not in remission rate. Fluoxetine-placebo difference was 3.2 points. No differences were observed among groups in the Beck Depression Inventory. Homeopathic group was superior to placebo in Greene Climacteric Scale (8.6 points). Fluoxetine was not different from placebo in Greene Climacteric Scale.
Conclusion: Homeopathy and fluoxetine are effective and safe antidepressants for climacteric women. Homeopathy and fluoxetine were significantly different from placebo in response definition only. Homeopathy, but not fluoxetine, improves menopausal symptoms scored by Greene Climacteric Scale.
And here are my critical remarks about this trial:
- The aim of a small study like this cannot be to assess or draw conclusions about the safety of the interventions used; for this purpose, we need sample sizes that are at least one dimension bigger.
- Fluoxetine might have been under-dosed (see below).
- The blinding of patients might have been jeopardized by patients experiencing the specific side-effects of fluoxetine. The authors reported adverse effects in all three groups. However, the characteristic and most common side-effects of fluoxetine (such as hives, itching, skin rash, restlessness, inability to sit still) were not included.
________________________________________________
Usual Adult Dose for Depression
Immediate-release oral formulations:
Initial dose: 20 mg orally once a day in the morning, increased after several weeks if sufficient clinical improvement is not observed
Maintenance dose: 20 to 60 mg orally per day
Maximum dose: 80 mg orally per day
Delayed release oral capsules:
Initial dose: 90 mg orally once a week, commenced 7 days after the last daily dose of immediate-release fluoxetine 20 mg formulations.
_________________________________________________
Considering all this, I feel that the conclusions of the above review are far too optimistic and not justified. In fact, I find them misleading, dangerous, unethical and depressing.