bogus claims
Chiropractic spinal manipulative therapy (CSMT) for migraine?
Why?
There is no good evidence that it works!
On the contrary, there is good evidence that it does NOT work!
A recent and rigorous study (conducted by chiropractors!) tested the efficacy of chiropractic CSMT for migraine. It was designed as a three-armed, single-blinded, placebo -controlled RCT of 17 months duration including 104 migraineurs with at least one migraine attack per month. Active treatment consisted of CSMT (group 1) and the placebo was a sham push manoeuvre of the lateral edge of the scapula and/or the gluteal region (group 2). The control group continued their usual pharmacological management (group 3). The results show that migraine days were significantly reduced within all three groups from baseline to post-treatment. The effect continued in the CSMT and placebo groups at all follow-up time points (groups 1 and 2), whereas the control group (group 3) returned to baseline. The reduction in migraine days was not significantly different between the groups. Migraine duration and headache index were reduced significantly more in the CSMT than in group 3 towards the end of follow-up. Adverse events were few, mild and transient. Blinding was sustained throughout the RCT. The authors concluded that the effect of CSMT observed in our study is probably due to a placebo response.
One can understand that, for chiropractors, this finding is upsetting. After all, they earn a good part of their living by treating migraineurs. They don’t want to lose patients and, at the same time, they need to claim to practise evidence-based medicine.
What is the way out of this dilemma?
Simple!
They only need to publish a review in which they dilute the irritatingly negative result of the above trial by including all previous low-quality trials with false-positive results and thus generate a new overall finding that alleges CSMT to be evidence-based.
This new systematic review of randomized clinical trials (RCTs) evaluated the evidence regarding spinal manipulation as an alternative or integrative therapy in reducing migraine pain and disability.
The searches identified 6 RCTs eligible for meta-analysis. Intervention duration ranged from 2 to 6 months; outcomes included measures of migraine days (primary outcome), migraine pain/intensity, and migraine disability. Methodological quality varied across the studies. The results showed that spinal manipulation reduced migraine days with an overall small effect size as well as migraine pain/intensity.
The authors concluded that spinal manipulation may be an effective therapeutic technique to reduce migraine days and pain/intensity. However, given the limitations to studies included in this meta-analysis, we consider these results to be preliminary. Methodologically rigorous, large-scale RCTs are warranted to better inform the evidence base for spinal manipulation as a treatment for migraine.
Bob’s your uncle!
Perhaps not perfect, but at least the chiropractic profession can now continue to claim they practice something akin to evidence-based medicine, while happily cashing in on selling their unproven treatments to migraineurs!
But that’s not very fair; research is not for promotion, research is for finding the truth; this white-wash is not in the best interest of patients! I hear you say.
Who cares about fairness, truth or conflicts of interest?
Christine Goertz, one of the review-authors, has received funding from the NCMIC Foundation and served as the Director of the Inter‐Institutional Network for Chiropractic Research (IINCR). Peter M. Wayne, another author, has received funding from the NCMIC Foundation and served as the co‐Director of the Inter‐Institutional Network for Chiropractic Research (IINCR)
And who the Dickens are the NCMIC and the IINCR?
At NCMIC, they believe that supporting the chiropractic profession, including chiropractic research programs and projects, is an important part of our heritage. They also offer business training and malpractice risk management seminars and resources to D.C.s as a complement to the education provided by the chiropractic colleges.
The IINCR is a collaborative effort between PCCR, Yale Center for Medical Informatics and the Osher Center for Integrative Medicine at Brigham and Women’s Hospital and Harvard Medical School. They aim at creating a chiropractic research portfolio that’s truly translational. Vice Chancellor for Research and Health Policy at Palmer College of Chiropractic Christine Goertz, DC, PhD (PCCR) is the network director. Peter Wayne, PhD (Osher Center for Integrative Medicine at Brigham and Women’s Hospital and Harvard Medical School) will join Anthony J. Lisi, DC (Yale Center for Medical Informatics and VA Connecticut Healthcare System) as a co-director. These investigators will form a robust foundation to advance chiropractic science, practice and policy. “Our collective efforts provide an unprecedented opportunity to conduct clinical and basic research that advances chiropractic research and evidence-based clinical practice, ultimately benefiting the patients we serve,” said Christine Goertz.
Really: benefiting the patients?
You could have fooled me!
 ‘Mom’s Choice Awards’ have just honoured the homeopathic product ‘COLD CALM KIDS’. This remedy has the following ingredients:
‘Mom’s Choice Awards’ have just honoured the homeopathic product ‘COLD CALM KIDS’. This remedy has the following ingredients:
- Allium cepa 3C HPUS
- Apis mellifica 15C HPUS
- Eupatorium perfoliatum 3C HPUS
- Gelsemium sempervirens 6C HPUS
- Kali bichromicum 6C HPUS
- Nux vomica 3C HPUS
- Phytolacca decandra 6C HPUS
- Pulsatilla 6C HPUS
3C = a dilution of 1:1000000
6C = a dilution of 1:1000000000000
15C = a dilution of 1:1000000000000000000000000000000
The ingredients are, according to this website, claimed to have the following effects:
- Allium cepa 3C HPUS – Relieves sneezing and runny nose
- Apis mellifica 15C HPUS – Relieves nasal congestion
- Eupatorium perfoliatum 3C HPUS – Relieves aches associated with colds
- Gelsemium sempervirens 6C HPUS – Relieves headaches associated with colds
- Kali bichromicum 6C HPUS – Relieves nasal discharge
- Nux vomica 3C HPUS – Relieves sneezing attacks
- Phytolacca decandra 6C HPUS – Relieves mild fever
- Pulsatilla 6C HPUS – Relieves colds with a loss of taste and smell
The formula could easily make Hahnemann turn in his grave! It goes against most of what he has been teaching. But I found these claims interesting nevertheless.
Are they true? To find out, I did some research. Here is what I found (in case anyone can find more evidence, I’d be most grateful to let me know):
- Allium cepa 3C HPUS – Relieves sneezing and runny nose NO GOOD EVIDENCE FOR THIS CLAIM
- Apis mellifica 15C HPUS – Relieves nasal congestion NO GOOD EVIDENCE FOR THIS CLAIM
- Eupatorium perfoliatum 3C HPUS – Relieves aches associated with colds NO GOOD EVIDENCE FOR THIS CLAIM
- Gelsemium sempervirens 6C HPUS – Relieves headaches associated with colds NO GOOD EVIDENCE FOR THIS CLAIM
- Kali bichromicum 6C HPUS – Relieves nasal discharge NO GOOD EVIDENCE FOR THIS CLAIM
- Nux vomica 3C HPUS – Relieves sneezing attacks NO GOOD EVIDENCE FOR THIS CLAIM
- Phytolacca decandra 6C HPUS – Relieves mild fever NO GOOD EVIDENCE FOR THIS CLAIM
- Pulsatilla 6C HPUS – Relieves colds with a loss of taste and smell NO GOOD EVIDENCE FOR THIS CLAIM
I am confused! If there is no good evidence, how come Boiron, the manufacturer of the product, is allowed to make these claims? And how come the product just was given an award?
The Mom’s Choice Awards® (MCA) evaluates products and services created for children, families and educators. The program is globally recognized for establishing the benchmark of excellence in family-friendly media, products and services. The organization is based in the United States and has reviewed thousands of items from more than 55 countries…
An esteemed panel of evaluators includes education, media and other experts as well as parents, children, librarians, performing artists, producers, medical and business professionals, authors, scientists and others.
MCA evaluators volunteer their time and are bound by a strict code of ethics which ensures expert and objective analysis free from any manufacturer association.
The evaluation process uses a proprietary methodology in which items are scored on a number of elements including production quality, design, educational value, entertainment value, originality, appeal and cost. Each item is judged on its own merit.
MCA evaluators are especially interested in items that help families grow emotionally, physically and spiritually; are morally sound and promote good will; and are inspirational and uplifting…
Now I am even more confused!
A benchmark of excellence?
A strict code of ethics?
Morally sound?
I must have misunderstood something! Or perhaps the award was for achieving a maximum of 8 false claims for one single product!? Can someone please enlighten me?
Whenever there are discussions about homeopathy (currently, they have reached fever-pitch both in France and in Germany), one subject is bound to emerge sooner or later: its cost. Some seemingly well-informed person will exclaim that USING MORE HOMEOPATHY WILL SAVE US ALL A LOT OF MONEY.
 The statement is as predictable as it is wrong.
The statement is as predictable as it is wrong.
Of course, homeopathic remedies tend to cost, on average, less than conventional treatments. But that is beside the point. A car without an engine is also cheaper than one with an engine. Comparing the costs of items that are not comparable is nonsense.
What we need are proper analyses of cost-effectiveness. And these studies clearly fail to prove that homeopathy is a money-saver.
Even researchers who are well-known for their pro-homeopathy stance have published a systematic review of economic evaluations of homeopathy. They included 14 published assessments, and the more rigorous of these investigations did not show that homeopathy is cost-effective. The authors concluded that “although the identified evidence of the costs and potential benefits of homeopathy seemed promising, studies were highly heterogeneous and had several methodological weaknesses. It is therefore not possible to draw firm conclusions based on existing economic evaluations of homeopathy“.
Probably the most meaningful study in this area is an investigation by another pro-homeopathy research team. Here is its abstract:
OBJECTIVES:
This study aimed to provide a long-term cost comparison of patients using additional homeopathic treatment (homeopathy group) with patients using usual care (control group) over an observation period of 33 months.
METHODS:
Health claims data from a large statutory health insurance company were analysed from both the societal perspective (primary outcome) and from the statutory health insurance perspective (secondary outcome). To compare costs between patient groups, homeopathy and control patients were matched in a 1:1 ratio using propensity scores. Predictor variables for the propensity scores included health care costs and both medical and demographic variables. Health care costs were analysed using an analysis of covariance, adjusted for baseline costs, between groups both across diagnoses and for specific diagnoses over a period of 33 months. Specific diagnoses included depression, migraine, allergic rhinitis, asthma, atopic dermatitis, and headache.
RESULTS:
Data from 21,939 patients in the homeopathy group (67.4% females) and 21,861 patients in the control group (67.2% females) were analysed. Health care costs over the 33 months were 12,414 EUR [95% CI 12,022-12,805] in the homeopathy group and 10,428 EUR [95% CI 10,036-10,820] in the control group (p<0.0001). The largest cost differences were attributed to productivity losses (homeopathy: EUR 6,289 [6,118-6,460]; control: EUR 5,498 [5,326-5,670], p<0.0001) and outpatient costs (homeopathy: EUR 1,794 [1,770-1,818]; control: EUR 1,438 [1,414-1,462], p<0.0001). Although the costs of the two groups converged over time, cost differences remained over the full 33 months. For all diagnoses, homeopathy patients generated higher costs than control patients.
CONCLUSION:
The analysis showed that even when following-up over 33 months, there were still cost differences between groups, with higher costs in the homeopathy group.
A recent analysis confirms this situation. It concluded that patients who use homeopathy are more expensive to their health insurances than patients who do not use it. The German ‘Medical Tribune’ thus summarised the evidence correctly when stating that ‘Globuli are m0re expensive than conventional therapies’. This quote mirrors perfectly the situation in Switzerland which as been summarised as follows: ‘Globuli only cause unnecessary healthcare costs‘.
But homeopaths (perhaps understandably) seem reluctant to agree. They tend to come out with ever new arguments to defend the indefensible. They claim, for instance, that prescribing a homeopathic remedy to a patient would avoid giving her a conventional treatment that is not only more expensive but also has side-effects which would cause further expense to the system.
To some, this sounds perhaps reasonable (particularly, I fear, to some politicians), but it should not be reasonable argument for responsible healthcare professionals.
Why?
Because it could apply only to the practice of bad and unethical medicine: if a patient is ill and needs a medical treatment, she does certainly not need something that is ineffective, like homeopathy. If she is not ill and merely wants a placebo, she needs assurance, compassion, empathy, understanding and most certainly not an expensive and potentially harmful conventional therapy.
To employ the above analogy, if someone needs transport, she does not need a car without an engine!
So, whichever way we twist or turn it, the issue turns out to be quite simple:
WHITHOUT EFFECTIVENESS, THERE CAN BE NO COST-EFFECTIVENESS!
The ‘International Federation of Anthroposophic Medical Associations’ have just published a ‘Statement on Vaccination‘. Here it is in its full beauty:
Vaccines, together with health education, hygiene and adequate nutrition, are essential tools for preventing infectious diseases. Vaccines have saved countless lives over the last century; for example, they allowed the eradication of small pox and are currently allowing the world to approach the elimination of polio.
Anthroposophic Medicine fully appreciates the contribution of vaccines to global health and firmly supports vaccination as an important measure to prevent life threatening diseases. Anthroposophic Medicine is not anti-vaccine and does not support anti-vaccine movements.
Physicians with training in Anthroposophic Medicine are expected to act in accordance with national legislation and to carefully advise patients (or their caregivers) to help them understand the relevant scientific information and national vaccination recommendations. In countries where vaccination is not mandatory and informed consent is needed, this may include coming to agreement with the patient (or the caregivers) about an individualized vaccination schedule, for example by adapting the timing of vaccination during infancy.
Taking into account ongoing research, local infectious disease patterns and socioeconomic risk factors, individual anthroposophic physicians are at times involved in the scientific discussion about specific vaccines and appropriate vaccine schedules. Anthroposophic Medicine is pro-science and continued scientific debate is more important than ever in today’s polarized vaccine environment.
Already in 2010, The European Council for Steiner Waldorf Education published a press release, implying a similar stance:
We wish to state unequivocally that opposition to immunization per se, or resistance to national strategies for childhood immunization in general, forms no part of our specific educational objectives. We believe that a matter such as whether or not to innoculate a child against communicable disease should be a matter of parental choice. Consequently, we believe that families provide the proper context for such decisions to be made on the basis of medical, social and ethical considerations, and upon the perceived balance of risks. Insofar as schools have any role to play in these matters, we believe it is in making available a range of balanced information both from the appropriate national agencies and qualified health professionals with expertise in the filed. Schools themselves are not, nor should they attempt to become, determiners of decisions regarding these matters.
Such statements sound about right. Why then am I not convinced?
Perhaps because there are hundreds of anthroposophic texts that seem to contradict this pro-vaccination stance (not least those from Rudolf Steiner himself). Today, anthroposophy enthusiasts are frequently rampant anti-vax; look at this quote, for instance:
… anthroposophic and conventional medicine have dramatically different viewpoints as to what causes common childhood illnesses. Conventional medicine views childhood illnesses for which vaccines have been developed as a physical disease, inherently bad, to be prevented. Their main goal, therefore, is protection against contracting the disease making one free of illness. In contrast, these childhood illnesses are viewed by anthroposophic medicine as a necessary instrument in dealing with karma and, as discussed by Husemann, and Wolff, 6 the incarnation of the child. During childhood illnesses, anthroposophic medical practitioners administer medical remedies to assist the child in dealing with the illness not only as a disease affecting their physical body in the physical plane, but also for soul spiritual development, thereby promoting healing. In contrast, allopathic medicaments are aimed at suppression of symptoms and not necessarily the promotion of healing.
In Manifestations of Karma, Rudolf Steiner states that humans may be able to influence their karma and remove the manifestation of certain conditions, i.e., disease, but they may not be liberated from the karmic effect which attempted to produce them. Says Steiner, “…if the karmic reparation is escaped in one direction, it will have to be sought in another … the souls in question would then be forced to seek another way for karmic compensation either in this or in another incarnation.” 7
In his lecture, Karma of Higher Beings 8, Steiner poses the question, “If someone seeks an opportunity of being infected in an epidemic, this is the result of the necessary reaction against an earlier karmic cause. Have we the right now to take hygienic or other measures?” The answer to this question must be decided by each person and may vary. For example, some may accept the risk of disease but not of vaccine side effects, while others may accept the risk associated with vaccination but not with the disease.
Anthroposophic medicine teaches that to prevent a disease in the physical body only postpones what will then be produced in another incarnation. Thus, when health measures are undertaken to eliminate the susceptibility to a disease, only the external nature of the illness is eliminated. To deal with the karmic activity from within, Anthroposphy states that spiritual education is required. This does not mean that one should automatically be opposed to vaccination. Steiner indicates that “Vaccination will not be harmful if, subsequent to vaccination, a person receives a spiritual education.”
Or consider this little statistic from the US:
Waldorf schools are the leading Nonmedical Exemption [of vaccinations] schools in various states, such as:
- Waldorf School of Mendocino County (California) – 79.1%
- Tucson Waldorf Schools (Arizona) – 69.6%
- Cedar Springs Waldorf School (California) – 64.7%
- Waldorf School of San Diego (California) – 63.6%
- Orchard Valley Waldorf School (Vermont) – 59.4%
- Whidbey Island Waldorf School (Washington) – 54.9%
- Lake Champlain Waldorf School (Vermont) – 49.6%
- Austin Waldorf School (Texas) – 48%
Or what about this quote?
Q: I am a mother who does not immunize my children. I feel as though I have to keep this a secret. I recently had to take my son to the ER for a tetanus shot when he got a fish hook in his foot, and I was so worried about the doctor asking if his shots were current. His grandmother also does not understand. What do you suggest?
A: You didn’t give your reasons for not vaccinating your children. Perhaps you feel intuitively that vaccinations just aren’t good for children in the long run, but you can’t explain why. If that’s the case, I think your intuition is correct, but in today’s contentious world it is best to understand the reasons for our decisions and actions.
There are many good reasons today for not vaccinating children in the United States I recommend you consult the book, The Vaccination Dilemma edited by Christine Murphy, published by SteinerBooks.
So, where is the evidence that anthroposophy-enthusiasts discourage vaccinations?
It turns out, there is plenty of it! In 2011, I summarised some of it in a review concluding that numerous reports from different countries about measles outbreaks centered around Steiner schools seem nevertheless to imply that a problem does exist. In the interest of public health, we should address it.
All this begs a few questions:
- Are anthroposophy-enthusiasts and their professional organisations generally for or against vaccinations?
- Are the statements above honest or mere distractions from the truth?
- Why are these professional organisations not going after their members who fail to conform with their published stance on vaccination?
I suspect I know the answers.
What do you think?
There is much propaganda for homeopathic vaccinations or homeoprophylaxis (as homeopaths like to call it, in order to give it a veneer of respectability), and on this blog we have discussed it repeatedly. The concept is unproven and dangerous. Yet it is being promoted relentlessly. Currently, I get > 12 million websites when I google ‘homeopathic vaccination’, and there are hundreds of dangerously misleading books and newspaper articles on the subject.

One study that I therefore always wanted to conduct was a trial comparing homeopathic ‘vaccines’ to placebo in terms of immunological response in human volunteers. Somehow, I never managed to get it going. Thus, I was delighted when, a few weeks ago, I received an article for peer-review (I hope I am allowed to disclose this fact here); it was almost exactly the trial I had dreamt of doing one day: the first ever study to test whether there is an antibody response to homeopathic vaccines. Now I am even more delighted to see that it has been published.
Its aim was to compare the antibody response of homeopathic and conventional vaccines and placebo in young adults. The authors hypothesized that there would be no significant difference between homeopathic vaccines and placebo, while there would be a significant increase in antibodies in those received conventional vaccines.
A placebo-controlled, double-blind RCT was conducted where 150 university students who had received childhood vaccinations were assigned to diphtheria, pertussis, tetanus, mumps, measles homeopathic vaccine, placebo, or conventional diphtheria, pertussis, tetanus (Tdap) and mumps, measles, rubella (MMR) vaccines. The primary outcome was a ≥ two-fold increase in antibodies from baseline following vaccination as measured by ELISA. Participants, investigators, study coordinator, data blood drawers, laboratory technician, and data analyst were blinded.
None of the participants in either the homeopathic vaccine or the placebo group showed a ≥ two-fold response to any of the antigens. In contrast, of those vaccinated with Tdap, 68% (33/48) had a ≥ two-fold response to diphtheria, 83% (40/48) to pertussis toxoid, 88% (42/48) to tetanus, and 35% (17/48) of those vaccinated with MMR had a response to measles or mumps antigens (p < 0.001 for each comparison of conventional vaccine to homeopathic vaccine or to placebo). There was a significant increase in geometric mean titres of antibody from baseline for conventional vaccine antigens (p < 0.001 for each), but none for the response to homeopathic antigens or placebo.
The authors concluded that homeopathic vaccines do not evoke antibody responses and produce a response that is similar to placebo. In contrast, conventional vaccines provide a robust antibody response in the majority of those vaccinated.
I think this is in every respect an excellent trial. It should once and for all get rid of what is arguably the homeopathy-cult’s most dangerous idea, namely that highly diluted homeopathic remedies can protect humans against infectious diseases. On this blog, I once called it ‘a danger for both the public and the individual who might believe in it … promoting HP is unethical, irresponsible and possibly even criminal.’
I said it ‘should’ get rid of this nonsense, but will it?
As homeopaths have, for now 200 years, showed themselves utterly impervious to evidence, I for one am not holding my breath. Yet, thanks to this excellent study, we can, when confronted with the notion of homeopathic vaccinations, henceforth point out that it is not just totally implausible but that, in addition, it has also been experimentally shown to be false.
My thanks to the Canadian investigators!
Mr William Harvey Lillard was the janitor contracted to clean the Ryan Building where D. D. Palmer’s magnetic healing office was located. In 1895, he became Palmer’s very first chiropractic patient and thus entered the history books. The very foundations of chiropractic are based on this story.

To call the ‘Chiropractor’ a reliable source would probably be stretching it a bit, and there are various versions of the event, even one where BJ Palmer, DD’s son, changed significant details of the story. Nevertheless, it’s a nice story, if there ever was one. But, like many nice stories, it’s just that: a tall tale, a story that might be not based on reality. In this case, the reality getting in the way of a good story is human anatomy.
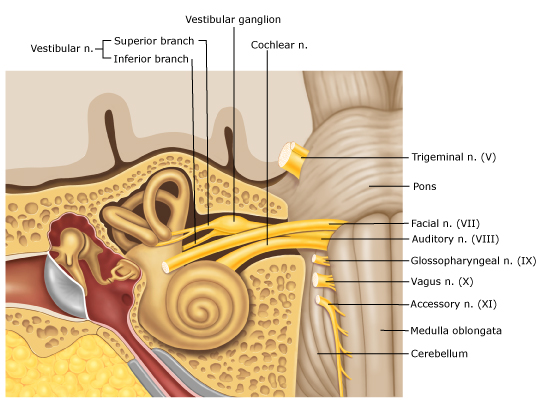
The nerve supply of the inner ear, the bit that enables us to hear, does not, like most other nerves of our body, run through the spine; it comes directly from the brain: the acoustic nerve is one of the 12 cranial nerves.

But chiropractors never let the facts get in the way of a good story! Thus they still tell it and presumably even believe it. Take this website, for instance, as an example of hundreds of similar sources:
… the very first chiropractic patient in history was named William Harvey Lillard, who experienced difficulty hearing due to compression of the nerves leading to his ears. He was treated by “the founder of chiropractic care,” David. D. Palmer, who gave Lillard spinal adjustments in order to reduce destructive nerve compressions and restore his hearing. After doing extensive research about physiology, Palmer believed that Lillard’s hearing loss was due to a misalignment that blocked the spinal nerves that controlled the inner ear (an example of vertebral subluxation). Palmer went on to successfully treat other patients and eventually trained other practitioners how to do the same.
How often have we been told that chiropractors receive a medical training that is at least as thorough as that of proper doctors? But that’s just another tall story, I guess.
I am being told to educate myself and rethink the subject of NAPRAPATHY by the US naprapath Dr Charles Greer. Even though he is not very polite, he just might have a point:
Edzard, enough foolish so-called scientific, educated assesments from a trained Allopathic Physician. When asked, everything that involves Alternative Medicine in your eyesight is quackery. Fortunately, every Medically trained Allopathic Physician does not have your points of view. I have partnered with Orthopaedic Surgeons, Medical Pain Specialists, General practitioners, Thoracic Surgeons, Forensic Pathologists and Others during the course, whom appreciate the Services that Naprapaths provide. Many of my current patients are Medical Physicians. Educate yourself. Visit a Naprapath to learn first hand. I expect your outlook will certainly change.
I have to say, I am not normally bowled over by anyone who calls me an ‘allopath’ (does Greer not know that Hahnemann coined this term to denigrate his opponents? Is he perhaps also in favour of homeopathy?). But, never mind, perhaps I was indeed too harsh on naprapathy in my previous post on this subject.
So, let’s try again.
Just to remind you, naprapathy was developed by the chiropractor Oakley Smith who had graduated under D D Palmer in 1899. Smith was a former Iowa medical student who also had investigated Andrew Still’s osteopathy in Kirksville, before going to Palmer in Davenport. Eventually, Smith came to reject Palmer’s concept of vertebral subluxation and developed his own concept of “the connective tissue doctrine” or naprapathy.
Dr Geer published a short article explaining the nature of naprapathy:
Naprapathy- A scientific, Evidence based, integrative, Alternative form of Pain management and nutritional assessment that involves evaluation and treatment of Connective tissue abnormalities manifested in the entire human structure. This form of Therapeutic Regimen is unique specifically to the Naprapathic Profession. Doctors of Naprapathy, pronounced ( nuh-prop-a-thee) also referred to as Naprapaths or Neuromyologists, focus on the study of connective tissue and the negative factors affecting normal tissue. These factors may begin from external sources and latently produce cellular changes that in turn manifest themselves into structural impairments, such as irregular nerve function and muscular contractures, pulling its’ bony attachments out of proper alignment producing nerve irritability and impaired lymphatic drainage. These abnormalities will certainly produce a pain response as well as swelling and tissue congestion. Naprapaths, using their hands, are trained to evaluate tissue tension findings and formulate a very specific treatment regimen which produces positive results as may be evidenced in the patients we serve. Naprapaths also rely on information obtained from observation, hands on physical examination, soft tissue Palpatory assessment, orthopedic evaluation, neurological assessment linked with specific bony directional findings, blood and urinalysis laboratory findings, diet/ Nutritional assessment, Radiology test findings, and other pertinent clinical data whose information is scrutinized and developed into a individualized and specific treatment plan. The diagnostic findings and results produced reveal consistent facts and are totally irrefutable. The deductions that formulated these concepts of theory of Naprapathic Medicine are rationally believable, and have never suffered scientific contradiction. Discover Naprapathic Medicine, it works.
What interests me most here is that naprapathy is evidence-based. Did I perhaps miss something? As I cannot totally exclude this possibility, I did another Medline search. I found several trials:
1st study (2007)
Four hundred and nine patients with pain and disability in the back or neck lasting for at least 2 weeks, recruited at 2 large public companies in Sweden in 2005, were included in this randomized controlled trial. The 2 interventions were naprapathy, including spinal manipulation/mobilization, massage, and stretching (Index Group) and support and advice to stay active and how to cope with pain, according to the best scientific evidence available, provided by a physician (Control Group). Pain, disability, and perceived recovery were measured by questionnaires at baseline and after 3, 7, and 12 weeks.
RESULTS:
At 7-week and 12-week follow-ups, statistically significant differences between the groups were found in all outcomes favoring the Index Group. At 12-week follow-up, a higher proportion in the naprapathy group had improved regarding pain [risk difference (RD)=27%, 95% confidence interval (CI): 17-37], disability (RD=18%, 95% CI: 7-28), and perceived recovery (RD=44%, 95% CI: 35-53). Separate analysis of neck pain and back pain patients showed similar results.
DISCUSSION:
This trial suggests that combined manual therapy, like naprapathy, might be an alternative to consider for back and neck pain patients.
2nd study (2010)
Subjects with non-specific pain/disability in the back and/or neck lasting for at least two weeks (n = 409), recruited at public companies in Sweden, were included in this pragmatic randomized controlled trial. The two interventions compared were naprapathic manual therapy such as spinal manipulation/mobilization, massage and stretching, (Index Group), and advice to stay active and on how to cope with pain, provided by a physician (Control Group). Pain intensity, disability and health status were measured by questionnaires.
RESULTS:
89% completed the 26-week follow-up and 85% the 52-week follow-up. A higher proportion in the Index Group had a clinically important decrease in pain (risk difference (RD) = 21%, 95% CI: 10-30) and disability (RD = 11%, 95% CI: 4-22) at 26-week, as well as at 52-week follow-ups (pain: RD = 17%, 95% CI: 7-27 and disability: RD = 17%, 95% CI: 5-28). The differences between the groups in pain and disability considered over one year were statistically significant favoring naprapathy (p < or = 0.005). There were also significant differences in improvement in bodily pain and social function (subscales of SF-36 health status) favoring the Index Group.
CONCLUSIONS:
Combined manual therapy, like naprapathy, is effective in the short and in the long term, and might be considered for patients with non-specific back and/or neck pain.
3rd study (2016)
Participants were recruited among patients, ages 18-65, seeking care at the educational clinic of Naprapathögskolan – the Scandinavian College of Naprapathic Manual Medicine in Stockholm. The patients (n = 1057) were randomized to one of three treatment arms a) manual therapy (i.e. spinal manipulation, spinal mobilization, stretching and massage), b) manual therapy excluding spinal manipulation and c) manual therapy excluding stretching. The primary outcomes were minimal clinically important improvement in pain intensity and pain related disability. Treatments were provided by naprapath students in the seventh semester of eight total semesters. Generalized estimating equations and logistic regression were used to examine the association between the treatments and the outcomes.
RESULTS:
At 12 weeks follow-up, 64% had a minimal clinically important improvement in pain intensity and 42% in pain related disability. The corresponding chances to be improved at the 52 weeks follow-up were 58% and 40% respectively. No systematic differences in effect when excluding spinal manipulation and stretching respectively from the treatment were found over 1 year follow-up, concerning minimal clinically important improvement in pain intensity (p = 0.41) and pain related disability (p = 0.85) and perceived recovery (p = 0.98). Neither were there disparities in effect when male and female patients were analyzed separately.
CONCLUSION:
The effect of manual therapy for male and female patients seeking care for neck and/or back pain at an educational clinic is similar regardless if spinal manipulation or if stretching is excluded from the treatment option.
_________________________________________________________________
I don’t know about you, but I don’t call this ‘evidence-based’ – especially as all the three trials come from the same research group (no, not Greer; he seems to have not published at all on naprapathy). Dr Greer does clearly not agree with my assessment; on his website, he advertises treating the following conditions:
Anxiety
Back Disorders
Back Pain
Cervical Radiculopathy
Cervical Spondylolisthesis
Cervical Sprain
Cervicogenic Headache
Chronic Headache
Chronic Neck Pain
Cluster Headache
Cough Headache
Depressive Disorders
Fibromyalgia
Headache
Hip Arthritis
Hip Injury
Hip Muscle Strain
Hip Pain
Hip Sprain
Joint Clicking
Joint Pain
Joint Stiffness
Joint Swelling
Knee Injuries
Knee Ligament Injuries
Knee Sprain
Knee Tendinitis
Lower Back Injuries
Lumbar Herniated Disc
Lumbar Radiculopathy
Lumbar Spinal Stenosis
Lumbar Sprain
Muscle Diseases
Musculoskeletal Pain
Neck Pain
Sciatica (Not Due to Disc Displacement)
Sciatica (Not Due to Disc Displacement)
Shoulder Disorders
Shoulder Injuries
Shoulder Pain
Sports Injuries
Sports Injuries of the Knee
Stress
Tendonitis
Tennis Elbow (Lateral Epicondylitis)
Thoracic Disc Disorders
Thoracic Outlet Syndrome
Toe Injuries
Odd, I’d say! Did all this change my mind about naprapathy? Not really.
But nobody – except perhaps Dr Greer – can say I did not try.
And what light does this throw on Dr Greer and his professionalism? Since he seems to be already quite mad at me, I better let you answer this question.
 Chiropractic may be nonsense, but it nevertheless earns chiros very good money. Chiropractors tend to treat their patients for unnecessarily long periods of time. This, of course, costs money, and even if the treatment in question ever was indicated (which, according to the best evidence, is more than doubtful), this phenomenon would significantly inflate healthcare expenditure. It was reported that over 80% of the money that the US Medicare paid to chiropractors in 2013 went for medically unnecessary procedures. The federal insurance program for senior citizens thus spent roughly $359 million on unnecessary chiropractic care that year.
Chiropractic may be nonsense, but it nevertheless earns chiros very good money. Chiropractors tend to treat their patients for unnecessarily long periods of time. This, of course, costs money, and even if the treatment in question ever was indicated (which, according to the best evidence, is more than doubtful), this phenomenon would significantly inflate healthcare expenditure. It was reported that over 80% of the money that the US Medicare paid to chiropractors in 2013 went for medically unnecessary procedures. The federal insurance program for senior citizens thus spent roughly $359 million on unnecessary chiropractic care that year.
Such expenditure may not benefit patients, but it surely benefits the chiropractors. A recent article in Forbes informed us that, according to the US Bureau of Labor Statistics’ Occupational Outlook Handbook, the employment of chiropractors is expected to grow 12% from 2016 to 2026, faster than the average for all occupations.
According to the latest data from the Bureau Occupational Employment Statistics, as of 2017, the average income of an US chiropractor amounts to US $ 85,870. However, chiropractors’ salaries aren’t this high in every US state. The lowest average income (US$ 45 000) per year is in the state of Wyoming.
Below you’ll find a breakdown of where chiropractors’ incomes are the highest.
| 1 | Rhode Island | $147,900 |
| 2 | Tennessee | $122,620 |
| 3 | Connecticut | $113,130 |
| 4 | Alaska | $106,600 |
| 5 | Colorado | $99,350 |
| 6 | New Hampshire | $99,330 |
| 7 | Nevada | $99,140 |
| 8 | Delaware | $97,650 |
| 9 | Massachusetts | $96,110 |
| 10 | Maryland | $95,190 |
These are tidy sums indeed – remember, they merely depict the averages. Individual chiropractors will earn substantially more than the average, of course. And there are hundreds of websites, books, etc. to teach chiros how to maximise their cash-flow. Some of the most popular ‘tricks of the chiro trade’ include:
- maintenance therapy,
- treatment of children,
- making unsupported therapeutic claims,
- disregarding the risks of spinal manipulation,
- selling useless dietary supplements.
Considering the sums of money that are at stake, I am beginning to understand why chiropractors tend to get so nervous, often even furious and aggressive, when I point out that they might be causing more harm than good to their patients.
Its the money, stupid!
My friend Roger, the homeopath, alerted me to the ‘Self-Controlled Energo Neuro Adaptive Regulation‘ (SCENAR). He uses it in his practice and explains:
The scenar uses biofeedback; by stimulating the nervous system, it is able to teach the body to heal itself. The device sends out a series of signals through the skin and measures the response. Each signal is only sent out when a change, in response to the previous signal, is recorded in the electrical properties of the skin. Visible responses include reddening of the skin, numbness, stickiness (the device will have the feeling of being magnetically dragged), a change in the numerical readout and an increase in the electronic clattering of the device.
The C-fibres, which comprise 85% of all nerves in the body, react most readily to the electro-stimulation and are responsible for the production of neuropeptides and other regulatory peptides. A TENS unit will only stimulate the A & B-fibres for temporary relief.
The body can get accustomed to a stable pathological state, which may have been caused by injury, disease or toxicity. The Scenar catalyses the process to produce regulatory peptides for the body to use where necessary, by stimulation of C-fibres . It is these neuropeptides that in turn reestablish the body’s natural physiological state and are responsible for the healing process. As these peptides last up to several hours, the healing process will continue long after the treatment is over. The large quantity of neuropeptides and C-fibres in the Central Nervous System can also result in the treatment on one area aiding with other general regulatory processes, like chemical imbalances, correcting sleeplessness, appetite and behavioral problems.
Sounds like science fiction?
Or perhaps more like BS?
But, as always, the proof of the pudding is in the eating. Roger explains:
What conditions can Scenar treat?
In the UK, the devices are licensed by the British Standards Institute for pain relief only. Likewise the FDA has approved the Scenar for pain relief. However, because of the nature of the device, viz., stimulating the nervous system, the Russian experience is that Scenar affects all the body systems in a curative manner.
The Russian experience suggests that it can be effective for a very broad range of diseases, including diseases of the digestive, cardio-vascular, respiratory, musculo-skeletal, urinary, reproductive and nervous systems. It is also useful for managing ENT diseases, eye diseases, skin conditions and dental problems. It has also been found beneficial in burns, fractures, insect bites, allergic reactions, diseases of the blood and disorders involving immune mechanisms; endocrine, nutritional and metabolic disorders; stress and mental depression, etc.
It is known to give real relief from many types of pain. It does so because it stimulates the body to heal the underlying disease causing the pain!
Another SCENAR therapist is much more specific. He tells us that SCENAR is effective for:
- Sports and other injuries
- Musculoskeletal problems
- Issues with circulation
- Respiratory diseases
- Digestive disorders
- Certain infections
- Immune dysfunctions
Perhaps I was a bit hasty; perhaps the SCENAR does work after all. It is certainly offered by many therapists like Roger. They cannot all be charlatans, or can they?
Time to do a proper Medline search and find out about the clinical trials that have been done with the SCENAR. Disappointingly, I only found three relevant papers; here they are:
A new technique of low-frequency modulated electric current therapy, SCENAR therapy, was used in treatment of 103 patients with duodenal ulcer (DU). The influence of SCENAR therapy on the main clinical and functional indices of a DU relapse was studied. It was shown that SCENAR therapy, which influences disturbed mechanisms of adaptive regulation and self-regulation, led to positive changes in most of the parameters under study. Addition of SCENAR therapy to the complex conventional pharmacotherapy fastened ulcer healing, increased the effectiveness of Helicobacter pylori eradication, and improved the condition of the gastroduodenal mucosa.
Administration of artrofoon in combination with SCENAR therapy to patients with localized suppurative peritonitis in the postoperative period considerably reduced plasma MDA level, stabilized ceruloplasmin activity, and increased catalase activity in erythrocytes compared to the corresponding parameters in patients receiving standard treatment in combination with SCENAR therapy.
The author recommends a self-control energoneuroadaptive regulator (SCENAR) as effective in the treatment of neurogenic dysfunction of the bladder in children with nocturnal enuresis. This regulator operates according to the principles of Chinese medicine and may be used in sanatoria and at home by the children’s parents specially trained by physiotherapist.
_____________________________________________________________________
While the quantity of the ‘studies’ is lamentable, their quality seems quite simply unacceptable.
We are thus left with two possibilities: either the SCENAR is more or less what its proponents promise and the science has for some strange reason not caught up with this reality; or the reality is that SCENAR is a bogus treatment used by charlatans who exploit the gullible public.
I know which possibility I favour – how about you?
As you can imagine, I get quite a lot of ‘fan-post’. Most of the correspondence amounts to personal attacks and insults which I usually discard. But some of these ‘love-letters’ are so remarkable in one way or another that I answer them. This short email was received on 20/3/19; it belongs to the latter category:
Dr Ernst,
You have been trashing homeopathy ad nauseum for so many years based on your limited understanding of it. You seem to know little more than that the remedies are so extremely dilute as to be impossibly effective in your opinion. Everybody knows this and has to confront their initial disbelief.
Why dont you get some direct understanding of homeopathy by doing a homeopathic proving of an unknown (to you) remedy? Only once was I able to convince a skeptic to take the challenge to do a homeopathic proving. He was amazed at all the new symptoms he experienced after taking the remedy repeatedly over several days.
Please have a similar bravery in your approach to homeopathy instead of basing your thoughts purely on your speculation on the subject, grounded in little understanding and no experience of it.
THIS IS HOW I RESPONDED
Dear Mr …
thank you for this email which I would like to answer as follows.
Your lines give the impression that you might not be familiar with the concept of critical analysis. In fact, you seem to confuse my criticism of homeopathy with ‘trashing it’. I strongly recommend you read up about critical analysis. No doubt you will then realise that it is a necessary and valuable process towards generating progress in healthcare and beyond.
You assume that I have limited understanding of homeopathy. In fact, I grew up with homeopathy, practised homeopathy as a young doctor, researched the subject for more than 25 years and published several books as well as over 100 peer-reviewed scientific papers about it. All of this, I have disclosed publicly, for instance, in my memoir which might interest you.
The challenge you mention has been taken by me and others many times. It cannot convince critical thinkers and, frankly, I am surprised that you found a sceptic who was convinced by what essentially amounts to little more than a party trick. But, as you seem to like challenges, I invite you to consider taking the challenge of the INH which even offers a sizable amount of money, in case you are successful.
Your final claim that my thoughts are based purely on speculation is almost farcically wrong. The truth is that sceptics try their very best to counter-balance the mostly weird speculations of homeopaths with scientific facts. I am sure that, once you have acquired the skills of critical thinking, you will do the same.
Best of luck.
Edzard Ernst