Monthly Archives: August 2022
Le Figaro reported that France’s medical appointment booking service ‘Doctolib’ is being accused of promoting so-called alternative medicine (SCAM) on its platform. “Measures will be taken soon. Several options are on the table, we do not exclude anything,” announced Doctolib after declaring during the day on its Twitter account the immediate suspension of some profiles.
Health professionals and patients have been criticizing the platform for allowing its users to make appointments with practitioners claiming to be naturopaths and some offering dangerous quackery. Naturopathy is not recognized in France and is sometimes considered to be linked to charlatanism.
A member of the office for the control of conspiracies, Tristan Mendès France, had found a practitioner promoting urine therapy via Doctolib. “The presence of these individuals on a service that puts patients and health professionals in touch with each other gives them totally unjustified credit and endorsement,” stated a Twitter account aimed at informing “about the dangers of certain pseudo-alternatives in terms of health and nutrition”.
Amongst the questioned profiles were the naturopaths Thierry Casasnovas and Irène Grosjean, two influential personalities in the naturopathic world who are discredited in the health world. “We would like to point out that it is impossible for a patient to make an [appointment] on Doctolib in a practitioner not referenced by the Ministry of Health, without having expressly sought to do so,” Doctolib defended its position stating that it would proceed to checks on practitioners “whose actions would be dangerous or condemnable by law” and who would have been the subject of complaints on social media.
97%” of practitioners signed up with Doctolib are registered with the Ministry of Health,” the company claimed. According to Doctolib, only 3% of its practitioners are therefore from the realm of SCAM: sophrologists, hypnotherapists, naturopaths. In France, these practitioners are not regulated and do not have the status of health professional, but they are nevertheless legal. The appointments made on Doctolib with such practitioners represent “0.3% of the totality” of the volume recorded on the platform.
The CEO of Doctolib, Stanislas Niox-Chateau, said that he was responding to a request from patients and refused to position his site as a simple directory of the Ministry of Health: “The demand is there. It is not up to us to say whether these activities are effective or useful. They are legal, so we have no reason to prevent practitioners from being listed on our site.”
As so often in the realm of SCAM, the dispute seems to be one between ethical/moral responsibilities and commercial interests of the parties involved.
Developing interventions against age-related memory decline and for older adults experiencing neurodegenerative disease is perhaps one of the greatest challenges of our generation. Spermidine supplementation has shown beneficial effects on brain and cognitive health in animal models, and there has been preliminary evidence of memory improvement in individuals with subjective cognitive decline.
This randomized, double-masked, placebo-controlled phase 2b trial was aimed at determining the effect of longer-term spermidine supplementation on memory performance and biomarkers in this at-risk group. The study was a monocenter trial carried out at an academic clinical research center in Germany. Eligible individuals were aged 60 to 90 years with subjective cognitive decline who were recruited from health care facilities as well as through advertisements in the general population.
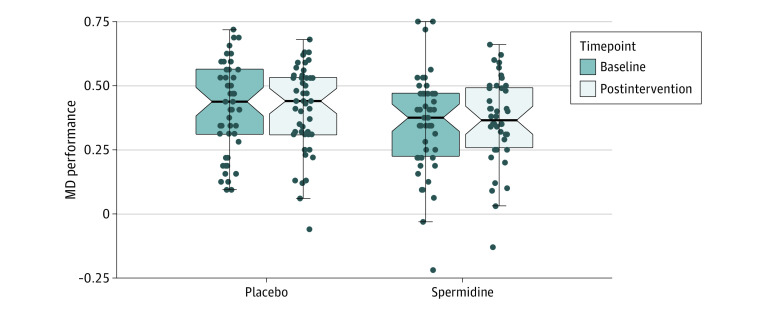
One hundred participants were randomly assigned (1:1 ratio) to 12 months of dietary supplementation with either a spermidine-rich dietary supplement extracted from wheat germ (0.9 mg spermidine/d) or placebo (microcrystalline cellulose). Eighty-nine participants (89%) successfully completed the trial. The primary outcome was change in memory performance from baseline to 12-month postintervention assessment (intention-to-treat analysis), operationalized by mnemonic discrimination performance assessed by the Mnemonic Similarity Task. Secondary outcomes included additional neuropsychological, behavioral, and physiological parameters. Safety was assessed in all participants and exploratory per-protocol, as well as subgroup, analyses were performed.
A total of 100 participants (51 in the spermidine group and 49 in the placebo group) were included in the analysis (mean [SD] age, 69 [5] years; 49 female participants [49%]). Over 12 months, no significant changes were observed in mnemonic discrimination performance (between-group difference, -0.03; 95% CI, -0.11 to 0.05; P = .47) and secondary outcomes. Exploratory analyses indicated possible beneficial effects of the intervention on inflammation and verbal memory. Adverse events were balanced between groups.
The authors concluded that in this randomized clinical trial, longer-term spermidine supplementation in participants with subjective cognitive decline did not modify memory and biomarkers compared with placebo. Exploratory analyses indicated possible beneficial effects on verbal memory and inflammation that need to be validated in future studies at higher dosage.
The absence of an effect might have, according to the authors, two reasons.
- The daily dose of 0.9 mg spermidine might not have been sufficient to achieve strong effects on memory function and biomarkers in cognitively healthy older individuals.
- The supplementation with dietary spermidine might not act as a memory booster, but rather prevent age-related memory impairment and development of AD, a possibility supported by evidence from animal studies.
I am tempted to add a third one: spermidine might not be effective at all for this indication (or any other condition)!
Israel’s Health Ministry announced the revocation of Dr. Aryeh Avni’s medical license, after he called to violate the ministry’s COVID guidelines during the pandemic and published defamatory articles against the medical community. The Jerusalem District Court rejected Avni’s appeal following the decision to revoke his medical license. Avni, who was a specialist in general surgery, engaged for years in so-called alternative medicine (SCAM) and had previously been caught forging vaccination certificates. He claimed in court that he operates in the context of freedom of expression and that his objective is to help the public and to rescue patients from the harm caused by medications and vaccines.
About a year and a half ago, the Health Ministry’s disciplinary committee recommended that Avni’s license be suspended for two years, but former Judge Amnon Shtrashnov, who was granted authority by the health minister, rejected the recommendation and ordered the permanent revocation of Avni’s license. In his decision, Shtrashnov called Avni “a charlatan, a clear coronavirus denier and a dangerous trickster, who behaves that way under the aegis of a licensed doctor.” “There must be a distinction between expressing an opinion and incitement, while conducting a smear campaign against medical authorities in order to dissuade the public from acting in accordance with their directive,” District Court Judge Nimrod Flax said in his decision. “A doctor who chooses to conduct a delegitimization campaign of this kind excludes himself, and is behaving in a manner unbefitting a licensed doctor. “And we will say once again – expressing an opinion, absolutely; conducting a campaign of incitement and defamation against his fellow doctors, while attempting to bias public opinion and to prevent the public from acting in accordance with the recommendations of the medical authorities, absolutely not,” added Judge Flax. “In general, criticism of the directives and decisions of the health care system and those who head it is legitimate, but that’s when these things are said in polite language and are based on true facts,” added the judge. “Granting approval to the appellant to continue to possess a medical license, while he continues with his previous practices, and in particular preaches to violate medical directives given by the authorized bodies, cannot accord with the public interest,” added the judge.
__________________________
Dr. Avni has a website where he writes about himself: “During his work in the hospital but also in his private life, Dr. Avni was exposed to the dismal results of conventional cancer treatments, he lost his wife and sister. The difficult events made him think that allopathic medicine is not the only option and he started looking for other solutions. Better, and less dangerous in terms of “do no harm”.
This is how Dr. Avni came in his decades of journey to many methods and treatments that have in common that they treat problems from the root and not only the symptom, they are not harmful, in repairing one disease they do not increase the risk of new disease, they treat the person and do not see only the “disease” And their natural origin.
The more he delved into his research, the more Dr. Avni discovered to his amazement that there were powerful forces trying to silence and obscure vital information about these treatments. In the United States, for example, several dozen doctors died prematurely and for “strange” reasons, these were doctors who opposed vaccines or conventional cancer treatments. In recent years, Dr. Avni has also faced constant persecution by the media and the Ministry of Health, and once his license was suspended. But Dr. Avni did not flinch or fold, this is his life mission and for that we appreciate him and thank him! And we are not the only ones.
____________________________
Personally, I feel that the world is a safer place without anti-vax doctors in clinical practice. Other countries should perhaps follow the example of Israel and be more ready to revoke the licenses of anti-vax charlatans.
England’s record goalscorer Ellen White has revealed she suffered a punctured lung while receiving acupuncture treatment. The injury accelerated her decision to retire. White, 33, said she was still coming to terms with the “traumatic” injury.
Manchester City had sourced a “specialist” – evidently not such an excellent acupuncturist because the complication is avoidable with proper knowledge of anatomy – outside the club to provide her with acupuncture to treat her back problem because of a high number of injuries in the squad at the time. “If you’d said to me two or three years ago that you’re going to retire, I would have said ‘absolutely not’, but I’ve got to a time in my career,” she said. “I had a challenging time last year – coming back from the Olympics, I basically punctured my lung, and it was a lot for me to have to go through and a big reason that accelerated my want to retire.”
The injury happened when she returned to her club with a back spasm last summer. “It punctured my lung which isn’t something that happens normally, obviously,” she said. “It was a really traumatic time for me and something that I’m still figuring out now, still working through. I had to wait for the lung to basically inflate again. I had a needle put into my chest to drag all the air out then hopefully the lung would inflate again – which it has. At the time, I think for me, I just got into a zone of: ‘I need to get back playing. We’ve got these games – I want to be back playing for my club; I want to be back playing for England. I went very tunnel vision,” she said. “It wasn’t until a good two or three months later, it just hit me like a train, what actually happened and how traumatic it was.”
Despite her quick return to goalscoring form, which included becoming the Lionesses record goalscorer in November, the striker says she is still affected by the injury and suffers “phantom pain” where it feels like it is happening again. “It’s important for me now to tell my story, and say it was a big factor in my year and leading up to the decision of wanting to retire. Obviously, there are other factors that come into that as well. I don’t want it to happen to anybody else again is my main thing. I don’t want to walk away from the sport having not told it and not say that I want things in place for it not to happen to anyone else.”
______________________________
Pneumothorax is by far the most common of all the serious, potentially fatal complications caused by acupuncture. In thin individuals, several acupuncture points over the upper thorax are just a few centimeters away from the lung. Therefore, it is easily possible to puncture a lung by inserting an acupuncture needle. This is from my 2010 review of the subject:
About 90 deaths after acupuncture have been anecdotally documented in the medical literature. Thus, acupuncture has been associated with more deaths than most other ‘alternative’ therapies except herbal medicine … The fatalities are usually due to an acupuncture needle penetrating a vital organ. This, in turn, can cause pneumothorax, cardiac tamponade, or major haemorrhage. Most instances of this nature are reported in the Asian literature which, for most of us, is not easily accessible.
A 2013 review of ours located 1104 cases that had been reported in the Korean literature alone. However, the truth of the matter is that nobody can be sure of the exact incidence figures. Why? Because there is no monitoring system that would reliably record such incidences.
I would argue that every single case of acupuncture-induced pneumothorax tells us that the acupuncturist was not adequately trained. With proper knowledge of anatomy, such complications should not happen. Therefore, such instances are a rude reminder that so-called alternative medicine (SCAM) is far too often in the hands of “specialists” who are a danger to the public.
It has been reported that the wife of a Northern California congressman died late last year after ingesting a plant that is generally considered safe and is used as an herbal remedy for a variety of ailments, including diabetes, obesity, and high cholesterol. Lori McClintock, the wife of U.S. Rep. Tom McClintock, died from dehydration due to gastroenteritis caused by “adverse effects of white mulberry leaf ingestion.” The coroner’s office ruled her death an accident. The original death certificate, dated Dec. 20, 2021, listed the cause of death as “pending.”
Tom McClintock found his 61-year-old wife unresponsive at their Elk Grove, California, home on Dec. 15, 2021, according to the coroner’s report. He had just returned from Washington, D.C., after voting in Congress the night before. It’s unclear from the autopsy report whether Lori McClintock took a dietary supplement containing white mulberry leaf, ate fresh or dried leaves, or drank them in a tea, but a “partially intact” white mulberry leaf was found in her stomach, according to the report.
McClintock’s death underscores the risks of the vast, booming market of dietary supplements and herbal remedies, which have grown into a $54 billion industry in the United States — one that both lawmakers and health care experts say needs more government scrutiny. “Many people assume if that product is sold in the United States of America, somebody has inspected it, and it must be safe. Unfortunately, that’s not always true,” U.S. Sen. Richard Durbin (D-Ill.) said on the Senate floor this spring when he introduced legislation to strengthen oversight of dietary supplements.
Daniel Fabricant, CEO and president of the Natural Products Association, which represents the dietary supplements industry, questioned whether McClintock’s death was related to a supplement. “It’s completely speculative. There’s a science to this. It’s not just what a coroner feels,” said Fabricant, who oversaw dietary supplements at the FDA during the Obama administration. “People unfortunately pass from dehydration every day, and there’s a lot of different reasons and a lot of different causes.” Fabricant said it would have been ideal had the coroner or the family reported her death to the FDA so the agency could have launched an investigation. Such reports are voluntary, and it’s not clear whether anyone reported her death to the agency. FDA spokesperson Courtney Rhodes said the agency does not discuss possible or ongoing investigations. The FDA, Fabricant added, has a system in place to investigate deaths that might be linked to a supplement or drug. “It’s casework,” he said. “It’s good, old-fashioned police work that needs to be done.”
Sacramento County spokesperson Kim Nava said via email Wednesday that the law prohibits the coroner’s office from discussing many details of specific cases. As part of any death investigation, the office “attempts to locate and review medical records and speak to family/witnesses to establish events leading up to and surrounding a death,” she said. If any medications or supplements are found at the scene or if pertinent information is in the person’s medical records, those are passed along to the pathologist to help establish cause of death, Nava said. “Any information the office obtains from medical records can’t be disseminated to a third party except by court order,” she said.
_____________
White mulberry (Morus alba) leaves are said to possess various biological activities, including antioxidant, antimicrobial, skin-whitening, cytotoxic, anti-diabetic, glucosidase inhibition, anti-hyperlipidemic, anti-atherosclerotic, anti-obesity, cardioprotective, and cognitive enhancement activities. Rich in anthocyanins and alkaloids, mulberry fruits have pharmacological properties, such as antioxidant, anti-diabetic, anti-atherosclerotic, anti-obesity, and hepatoprotective activities. The root bark of mulberry, containing flavonoids, alkaloids, and stilbenoids, has antimicrobial, skin-whitening, cytotoxic, anti-inflammatory, and anti-hyperlipidemic properties. Other pharmacological properties of M. alba include anti-platelet, anxiolytic, anti-asthmatic, anthelmintic, antidepressant, cardioprotective, and immunomodulatory activities.
Clinical trials on the efficiency of Morus alba extracts in reducing blood glucose and cholesterol levels and enhancing cognitive ability have been conducted. Yet the findings are so far not compelling. There is an extensive history of consumption of Morus alba leaves by humans and animals worldwide. The plant is a frequent ingredient in TCM preparations. This might suggest that the leaves and their extracts have a good safety profile. However systematic investigations into the issue seem to be absent. Reports of serious adverse effects in humans are rare. Thus one might ask whether the supplement in question – if it was a supplement at all that the woman took – might have been contaminated with a toxic substance.
According to the authors of this study, research is lacking regarding osteopathic approaches in treating polycystic ovary syndrome (PCOS), one of the prevailing endocrine abnormalities in reproductive-aged women. Limited movement of pelvic organs can result in functional and structural deficits, which can be resolved by applying visceral manipulation (VM). Already with these two introductory sentences, I have problems. But for the moment, we can leave this aside and have a look at their trial.
The study was aimed at analyzing the effect of VM on dysmenorrhea, irregular, delayed, and/or absent menses, and premenstrual symptoms in PCOS patients.
Thirty Egyptian women with PCOS, with menstruation-related complaints and free from systematic diseases and/or adrenal gland abnormalities, prospectively participated in a single-blinded, randomized controlled trial. They were recruited from the women’s health outpatient clinic in the faculty of physical therapy at Cairo University, with an age of 20-34 years, and a body mass index (BMI) ≥25, <30 kg/m2. Patients were randomly allocated into two equal groups (15 patients); the control group received a low-calorie diet for 3 months, and the study group received the same hypocaloric diet plus VM to the pelvic organs and their related structures, according to assessment findings, for eight sessions over 3 months. Evaluations for body weight, BMI, and menstrual problems were done by weight-height scale, and menstruation-domain of Polycystic Ovary Syndrome Health-Related Quality of Life Questionnaire (PCOSQ), respectively, at baseline and after 3 months of treatments.
A total of 30 patients were included, with baseline mean age, weight, BMI, and menstruation domain score of 27.5 ± 2.2 years, 77.7 ± 4.3 kg, 28.6 ± 0.7 kg/m2, and 3.4 ± 1.0, respectively, for the control group, and 26.2 ± 4.7 years, 74.6 ± 3.5 kg, 28.2 ± 1.1 kg/m2, and 2.9 ± 1.0, respectively, for the study group. Of the 15 patients in the study group, uterine adhesions were found in 14 patients (93.3%), followed by restricted uterine mobility in 13 patients (86.7%), restricted ovarian/broad ligament mobility (9, 60%), and restricted motility (6, 40%). At baseline, there was no significant difference (p>0.05) in any of the demographics (age, height), or dependent variables (weight, BMI, menstruation domain score) among both groups. Post-study, there was a statistically significant reduction (p=0.000) in weight, and BMI mean values for the diet group (71.2 ± 4.2 kg, and 26.4 ± 0.8 kg/m2, respectively) and the diet + VM group (69.2 ± 3.7 kg; 26.1 ± 0.9 kg/m2, respectively). For the improvement in the menstrual complaints, a significant increase (p<0.05) in the menstruation domain mean score was shown in the diet group (3.9 ± 1.0), and the diet + VM group (4.6 ± 0.5). On comparing both groups post-study, there was a statistically significant improvement (p=0.024) in the severity of menstruation-related problems in favor of the diet + VM group.
The authors concluded that VM yielded greater improvement in menstrual pain, irregularities, and premenstrual symptoms in PCOS patients when added to caloric restriction than utilizing the low-calorie diet alone in treating that condition.
VM involves the manual manipulation by a therapist of internal organs, blood vessels and nerves (the viscera) mostly from outside the body, but sometimes, the therapist also puts his/her fingers into the patient’s vagina. It was developed by the osteopath Jean-Piere Barral. He stated that through his clinical work with thousands of patients, he created this modality based on organ-specific fascial mobilization. And through work in a dissection lab, he was able to experiment with visceral manipulation techniques and see the internal effects of the manipulations. According to its proponents, visceral manipulation is based on the specific placement of soft manual forces looking to encourage the normal mobility, tone, and motion of the viscera and their connective tissues. The idea is that these gentle manipulations may potentially improve the functioning of individual organs, the systems the organs function within, and the structural integrity of the entire body.
I don’t see any reason to believe the concepts of VM are plausible. Thus I find the hypothesis of this trial extremely far-fetched. The results are equally unconvincing. As we have often discussed, the ‘A+B vs B’ design cannot prove a causal relationship between the intervention and the outcome.
The most likely explanation for the findings is that the patients receiving VM experienced or merely reported improvements because the extra attention of mildly invasive treatments produced a powerful placebo effect. To put it bluntly: this is a poor, arguably unethical study where over-enthusiastic researchers reach a conclusion that is not supported by the data.
Many older adults commonly take multivitamin-multimineral (MVM) supplements to promote health. Yet, evidence on the use of daily MVMs on invasive cancer is limited.
The objective of this study was therefore to determine if a daily MVM decreases total invasive cancer among older adults. For this purpose, a team of researchers performed a randomized, double-blind, placebo-controlled, 2-by-2 factorial trial of a daily MVM and cocoa extract for prevention of cancer and cardiovascular disease (CVD) among 21,442 US adults (12,666 women aged ≥65 y and 8776 men aged ≥60 y) free of major CVD and recently diagnosed cancer. The intervention phase was from June 2015 through December 2020. This article reports on the MVM intervention.
Participants were randomly assigned to daily MVM or placebo. The primary outcome was total invasive cancer, excluding nonmelanoma skin cancer. Secondary outcomes included major site-specific cancers, total CVD, all-cause mortality, and total cancer risk among those with a baseline history of cancer.
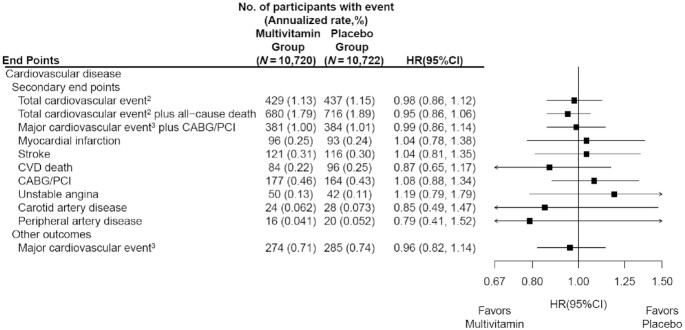
During a median follow-up of 3.6 y, invasive cancer occurred in 518 participants in the MVM group and 535 participants in the placebo group (HR: 0.97; 95% CI: 0.86, 1.09; P = 0.57). No significant effect was observed of a daily MVM on breast cancer (HR: 1.06; 95% CI: 0.79, 1.42) or colorectal cancer (HR: 1.30; 95% CI: 0.80, 2.12). The researchers observed a protective effect of a daily MVM on lung cancer (HR: 0.62; 95% CI: 0.42, 0.92). The composite CVD outcome occurred in 429 participants in the MVM group and 437 participants in the placebo group (HR: 0.98; 95% CI: 0.86, 1.12). MVM use did not significantly affect all-cause mortality (HR: 0.93; 95% CI: 0.81, 1.08). There were no safety concerns.
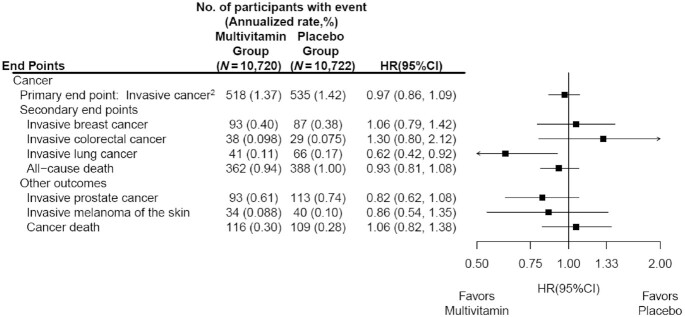
The authors concluded that a daily MVM supplement, compared with placebo, did not significantly reduce the incidence of total cancer among older men and women. Future studies are needed to determine the effects of MVMs on other aging-related outcomes among older adults.
This is an excellent and important study with clear findings. Nevertheless, the authors insist that several limitations should be considered. First, the COSMOS intervention was relatively short to detect a potential small-to-moderate effect on cancer outcomes given the long duration of time typically required for nutritional interventions to potentially reduce cancer risk. Second, the secondary and exploratory analyses should be interpreted with caution, especially given an overall lack of effect of an MVM on the primary outcome of total invasive cancer. Third, the authors successfully leveraged existing cohorts with mass mailings to expedite recruitment and randomization of 21,442 participants into COSMOS. However, generalizability may be limited, with modest diversity of 10% non-Whites and 2.6% Hispanics plus healthy volunteer bias for participants willing and eligible to enroll in a mail-based clinical trial.
While still at Exeter, we had a whole program examining so-called alternative medicines (SCAMs) for weight reduction. I thus can assure you of one thing: there are plenty out there! We also published many papers on the subject. The results can be summarized quite easily:
NONE OF THEM WORK CONVINCINGLY AND MANY ARE OUTRIGHT FRAUDULENT.
So I thought I had seen them all … until I saw this advertisement:
Hourglass S-line Waist Slimming Patch ingredients directly transfers them to your skin which then stimulates your body, kickstarts your metabolism and increases calorific burn. This process tones your skin, busts fat cells giving you a slimmer appearance with radiant looking skin.

Consist of 3 Key Ingredient For Hourglass S-line Waist Slimming Patch:
- Ay Tsao
- Wormwood
- Mint

Ay Tsao is a flowering plant that is mostly cultivated for its root, it decreases inflammation, stimulates digestion, and suppresses your appetite. These properties are effective ways promote weight loss. Experts says that this plant plays a huge role in providing a person with health benefits, determining decongestion and improving blood circulation.
Wormwood is regarded as a useful remedy for liver and gallbladder problems. Wormwood contains strong bitter agents known as absinthin and anabsinthin, which stimulate digestive and gallbladder function. Wormwood is believed to stimulate digestion and relieve spasms in the intestinal tract
Mint play an essential role in losing weight in a healthy way. Mint leaves promote digestion and boost metabolism to help in losing weight. Mint tea is a great refreshing calorie-free beverage to promote weight loss.
This is why Hourglass S-line Waist Slimming Patch is special
- Effectively prevent forming a waist fat.
- Accelerate the burning of fat.
- Maintaining a perfect body continuously.
- Extracting the essence from pure, safe, and healthy natural plants.
- Better sleep;
- Safe for daily use.
- Relieves gas and bloating.
- Slim down, and increase your energy levels for a better, healthier life.
- Made of high-quality material, with good breathability and adhesion.
Natalie’s Hourglass S-line Waist Slimming Patch report
Natalie Having trouble wearing dress because of her weight. She wanted a body that will make a dress look good for her. She gladly found this product online.
Here is the result…
Week 1

“Having a sexy body is always what I wanted. But what I can only do is light exercise. So I decided to use this Hourglass S-line Waist Slimming Patch. In just a week my body felt light. I still have a medium-sized belly but I’ll keep trying. Improvement is important and I see it with this product.”
Week 4
“I’m on day 30 of using this product. I love it. I combined its use with diet and light exercise. This is a good treatment for my muscles because Hourglass S-line Waist Slimming Patch also helps with muscle cramps or pain. I never feel my waist muscles working as well as they do when I’m using this product. I love feeling my body muscles actually moving in there. I literally KNOW this product is working my muscles for me. It’s incredible.”
Week 6

“After a month and a half, the result is great. I am amazed that the product is just as described. It will surely achieve the body that you want!! A must try for everyone, this patch is restrengthening muscles, or to add an extra kick in the gut for your exercise, this is it!”
Natalie Lopez — Toronto, Canada
This Patch saves you tons of money!
Hourglass S-line Waist Slimming Patch all natural ingredients are carefully made to make a huge impact not only to your skin but also saves you tons of money in the long run.

With this product you can avoid expensive sessions, time consuming appointments and you can use this patch at your home that can save transportations fare.
How to Use:
- Make sure your waist is dry and clean.
- Take 2 pcs patch and tear of the back then stick it to your both side waist.
- Remove after 3 – 8 hours a day.
______________________________________
I find it hard to believe that there are people who actually fall for such an advertisement. And the more I think about it, the sadder I feel. There are quite obviously some who believe such nonsense and get ripped off by irresponsible snake-oil salesmen. Not only does the product not work, but some of the ingredients are also potentially toxic.
I hope that my posing this will prevent a few people from wasting their hard-earned money on outright quackery:
None of the claims made in this advertisement is backed by evidence!
Traditional, complementary, and alternative medicine (TCAM) – as most of my readers know, I prefer the abbreviation SCAM for so-called alternative medicine – refers to a broad range of health practices and products typically not part of the ‘conventional medicine’ system. Its use is substantial among the general population. TCAM products and therapies may be used in addition to, or instead of, conventional medicine approaches, and some have been associated with adverse reactions or other harms.
The aims of this systematic review were to identify and examine recently published national studies globally on the prevalence of TCAM use in the general population, to review the research methods used in these studies, and to propose best practices for future studies exploring the prevalence of use of TCAM.
MEDLINE, Embase, CINAHL, PsycINFO, and AMED were searched to identify relevant studies published since 2010. Reports describing the prevalence of TCAM use in a national study among the general population were included. The quality of included studies was assessed using a risk of bias tool developed by Hoy et al. Relevant data were extracted and summarised.
Forty studies from 14 countries, comprising 21 national surveys and one cross-national survey, were included. Studies explored the use of TCAM products (e.g. herbal medicines), TCAM practitioners/therapies, or both. Included studies used different TCAM definitions, prevalence time frames and data collection tools, methods and analyses, thereby limiting comparability across studies. The reported prevalence of use of TCAM (products and/or practitioners/therapies) over the previous 12 months was 24–71.3%.
The authors concluded that the reported prevalence of use of TCAM (products and/or practitioners/therapies) is high, but may underestimate use. Published prevalence data varied considerably, at least in part because studies utilise different data collection tools, methods and operational definitions, limiting cross-study comparisons and study reproducibility. For best practice, comprehensive, detailed data on TCAM exposures are needed, and studies should report an operational definition (including the context of TCAM use, products/practices/therapies included and excluded), publish survey questions and describe the data-coding criteria and analysis approach used.
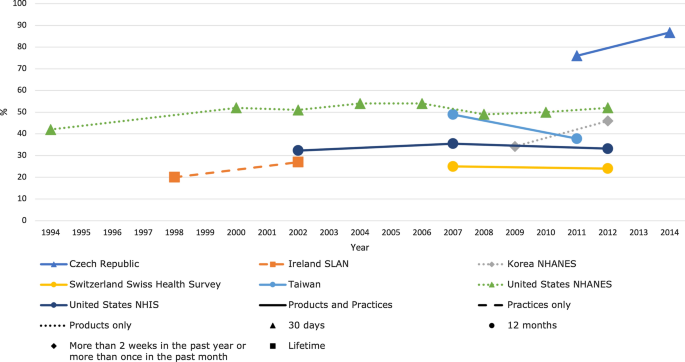
[Trends in prevalence of TCAM use by country for countries with at least two data collection waves from a nationally representative study. For data collected over several years (e.g. 2007–2009), the prevalence data are plotted at the end of the data collection period (e.g. 2009). Solid and perforated lines between consecutive points are for illustrative purposes only and are not intended to represent linearity. NHANES National Health and Nutrition Examination Survey, NHIS National Health and Interview Survey, SLAN Survey of Lifestyle, Attitudes and Nutrition.]
The review discloses that the prevalence reported across countries ranges from 24 to 71%. This huge variability is not very surprising; some of the many reasons for this phenomenon include:
- different TCAM definitions,
- different prevalence time frames,
- different data collection tools,
- different methods of analyzing the data.
Despite these problems, the information summarized in the review is fascinating in several respects. For me, the most interesting message here is this: the plethora of claims that SCAM use is increasing are not supported by sound evidence.
An article in THE TIMES seems worth mentioning. Here are some excerpts:
… Maternity care at Nottingham University Hospitals NHS Trust (NUH) is the subject of an inquiry, prompted by dozens of baby deaths. More than 450 families have now come forward to take part in the review, led by the expert midwife Donna Ockenden. The trust now faces further scrutiny over its use of aromatherapy, after experts branded guidelines at the trust “shocking” and not backed by evidence. Several bereaved families have said they recall aromatherapy being heavily promoted at the trust’s maternity units.
It is being prosecuted over the death of baby Wynter Andrews just 23 minutes after she was born in September 2019. Her mother Sarah Andrews wrote on Twitter that she remembered aromatherapy being seen as “the answer to everything”. Internal guidelines, first highlighted by the maternity commentator Catherine Roy, suggest using essential oils if the placenta does not follow the baby out of the womb quickly enough… the NUH guidelines say aromatherapy can help expel the placenta, and suggest midwives ask women to inhale oils such as clary sage, jasmine, lavender or basil, while applying others as an abdominal compress. They also describe the oils as “extremely effective for the prevention of and, in some cases, the treatment of infection”. The guidelines also suggest essential oils to help women suffering from cystitis, or as a compress on a caesarean section wound. Nice guidelines for those situations do not recommend aromatherapy…
The NUH adds frankincense “may calm hysteria” and is “recommended in situations of maternal panic”. Roy said: “It is shocking that dangerous advice seemed to have been approved by a team of healthcare professionals at NUH. There is a high tolerance for pseudoscience in NHS maternity care … and it needs to stop. Women deserve high quality care, not dangerous quackery.” …
________________________________
The journalist who wrote the article also asked me for a comment, and I emailed her this quote: “Aromatherapy is little more than a bit of pampering; no doubt it is enjoyable but it is not an effective therapy for anything. To use it in medical emergencies seems irresponsible to say the least.” The Times evidently decided not to include my thoughts.
Having now read the article, I checked again and failed to find good evidence for aromatherapy for any of the mentioned conditions. However, I did find an article and an announcement both of which are quite worrying, in my view:
Aromatherapy is often misunderstood and consequently somewhat marginalized. Because of a basic misinterpretation, the integration of aromatherapy into UK hospitals is not moving forward as quickly as it might. Aromatherapy in UK is primarily aimed at enhancing patient care or improving patient satisfaction, and it is frequently mixed with massage. Little focus is given to the real clinical potential, except for a few pockets such as the Micap/South Manchester University initiative which led to a Phase 1 clinical trial into the effects of aromatherapy on infection carried out in the Burns Unit of Wythenshawe Hospital. This article discusses the expansion of aromatherapy within the US and follows 10 years of developing protocols and policies that led to pilot studies on radiation burns, chemo-induced nausea, slow-healing wounds, Alzheimers and end-of-life agitation. The article poses two questions: should nursing take aromatherapy more seriously and do nurses really need 60 hours of massage to use aromatherapy as part of nursing practice?
My own views on aromatherapy are expressed in our now not entirely up-to-date review:
Aromatherapy is the therapeutic use of essential oil from herbs, flowers, and other plants. The aim of this overview was to provide an overview of systematic reviews evaluating the effectiveness of aromatherapy. We searched 12 electronic databases and our departmental files without restrictions of time or language. The methodological quality of all systematic reviews was evaluated independently by two authors. Of 201 potentially relevant publications, 10 met our inclusion criteria. Most of the systematic reviews were of poor methodological quality. The clinical subject areas were hypertension, depression, anxiety, pain relief, and dementia. For none of the conditions was the evidence convincing. Several SRs of aromatherapy have recently been published. Due to a number of caveats, the evidence is not sufficiently convincing that aromatherapy is an effective therapy for any condition.
In this context, it might also be worth mentioning that we warned about the frequent usage of quackery in midwifery years ago. Here is our systematic review of 2012 published in a leading midwifery journal:
Background: in recent years, several surveys have suggested that many midwives use some form of complementary/alternative therapy (CAT), often without the knowledge of obstetricians.
Objective: to systematically review all surveys of CAT use by midwives.
Search strategy: six electronic databases were searched using text terms and MeSH for CAT and midwifery.
Selection criteria: surveys were included if they reported quantitative data on the prevalence of CAT use by midwives.
Data collection and analysis: full-text articles of all relevant surveys were obtained. Data were extracted according to pre-defined criteria.
Main results: 19 surveys met the inclusion criteria. Most were recent and from the USA. Prevalence data varied but were usually high, often close to 100%. Much use of CATs does not seem to be supported by strong evidence for efficacy.
Conclusion: most midwives seem to use CATs. As not all CATs are without risks, the issue should be debated openly.
I am tired of saying ‘I TOLD YOU SO!’ but nevertheless find it a pity that our warning remained (yet again) unheeded!