Monthly Archives: April 2019
The most regularly reported serious complication of chiropractic neck manipulation is a stroke due to arterial dissection. Atlantoaxial dislocation (a dislocations of the first and second vertebrae which means that the spinal cord is in danger of being compressed which, in turn, would have devastating consequences) has not been previously reported, but is just as serious.

This new case-report described an 83-year-old man with a history of old cerebellar infarction who presented to the emergency department with acute left hemiplegia after a chiropractic manipulation of the neck and back several hours before symptom onset. Mild hypoesthesia was observed on his left limbs. No speech disturbance, facial palsy, or neck or shoulder pain was observed.
Intravenous thrombolytic treatment was given 238 min after symptom onset. Brown-Sequard syndrome (damage to one side of the spinal cord causing paralysis and loss of feeling on one side) subsequently developed 6 h after thrombolysis with a hypo-aesthetic sensory level below the right C5 dermatome. An emergent brain magnetic resonance angiography did not reveal an acute cerebral infarct but rather an atlantoaxial dislocation causing upper cervical spinal cord compression.
Clinical symptoms did not deteriorate after thrombolysis. He received successful decompressive surgery 1 week later, and his muscle power gradually improved, with partial dependency when performing daily living activities two months later.
A literature review revealed that only 15 patients (including the patient mentioned here) with spinal disorder mimicking acute stroke who received thrombolytic therapy have been reported. Atlantoaxial dislocation may present as acute hemiplegia mimicking acute stroke, followed by Brown-Sequard syndrome. Inadvertent thrombolytic therapy is likely not harmful for patients with atlantoaxial dislocation-induced cervical myelopathy. The neurological deficits of patients should be carefully and continuously evaluated to differentiate between stroke and myelopathy.
The authors of this case report provide no detail about the exact treatment that caused this complication, nor do they elaborate on the type of healthcare professional who administered the cervical manipulation (they focus on the issue of non-indicated thrombolytic therapy). We also do not learn why the patient had neck manipulations in the first place. However, the authors seem confident that the ‘chiropractic manipulation’ was the cause of this atlantoaxial dislocation causing severe upper cervical spinal cord compression.
The patient was treated surgically, with corticosteroids and subsequent rehabilitation. Two months later, his neurological deficits were much improved.
The ‘International Federation of Anthroposophic Medical Associations’ have just published a ‘Statement on Vaccination‘. Here it is in its full beauty:
Vaccines, together with health education, hygiene and adequate nutrition, are essential tools for preventing infectious diseases. Vaccines have saved countless lives over the last century; for example, they allowed the eradication of small pox and are currently allowing the world to approach the elimination of polio.
Anthroposophic Medicine fully appreciates the contribution of vaccines to global health and firmly supports vaccination as an important measure to prevent life threatening diseases. Anthroposophic Medicine is not anti-vaccine and does not support anti-vaccine movements.
Physicians with training in Anthroposophic Medicine are expected to act in accordance with national legislation and to carefully advise patients (or their caregivers) to help them understand the relevant scientific information and national vaccination recommendations. In countries where vaccination is not mandatory and informed consent is needed, this may include coming to agreement with the patient (or the caregivers) about an individualized vaccination schedule, for example by adapting the timing of vaccination during infancy.
Taking into account ongoing research, local infectious disease patterns and socioeconomic risk factors, individual anthroposophic physicians are at times involved in the scientific discussion about specific vaccines and appropriate vaccine schedules. Anthroposophic Medicine is pro-science and continued scientific debate is more important than ever in today’s polarized vaccine environment.
Already in 2010, The European Council for Steiner Waldorf Education published a press release, implying a similar stance:
We wish to state unequivocally that opposition to immunization per se, or resistance to national strategies for childhood immunization in general, forms no part of our specific educational objectives. We believe that a matter such as whether or not to innoculate a child against communicable disease should be a matter of parental choice. Consequently, we believe that families provide the proper context for such decisions to be made on the basis of medical, social and ethical considerations, and upon the perceived balance of risks. Insofar as schools have any role to play in these matters, we believe it is in making available a range of balanced information both from the appropriate national agencies and qualified health professionals with expertise in the filed. Schools themselves are not, nor should they attempt to become, determiners of decisions regarding these matters.
Such statements sound about right. Why then am I not convinced?
Perhaps because there are hundreds of anthroposophic texts that seem to contradict this pro-vaccination stance (not least those from Rudolf Steiner himself). Today, anthroposophy enthusiasts are frequently rampant anti-vax; look at this quote, for instance:
… anthroposophic and conventional medicine have dramatically different viewpoints as to what causes common childhood illnesses. Conventional medicine views childhood illnesses for which vaccines have been developed as a physical disease, inherently bad, to be prevented. Their main goal, therefore, is protection against contracting the disease making one free of illness. In contrast, these childhood illnesses are viewed by anthroposophic medicine as a necessary instrument in dealing with karma and, as discussed by Husemann, and Wolff, 6 the incarnation of the child. During childhood illnesses, anthroposophic medical practitioners administer medical remedies to assist the child in dealing with the illness not only as a disease affecting their physical body in the physical plane, but also for soul spiritual development, thereby promoting healing. In contrast, allopathic medicaments are aimed at suppression of symptoms and not necessarily the promotion of healing.
In Manifestations of Karma, Rudolf Steiner states that humans may be able to influence their karma and remove the manifestation of certain conditions, i.e., disease, but they may not be liberated from the karmic effect which attempted to produce them. Says Steiner, “…if the karmic reparation is escaped in one direction, it will have to be sought in another … the souls in question would then be forced to seek another way for karmic compensation either in this or in another incarnation.” 7
In his lecture, Karma of Higher Beings 8, Steiner poses the question, “If someone seeks an opportunity of being infected in an epidemic, this is the result of the necessary reaction against an earlier karmic cause. Have we the right now to take hygienic or other measures?” The answer to this question must be decided by each person and may vary. For example, some may accept the risk of disease but not of vaccine side effects, while others may accept the risk associated with vaccination but not with the disease.
Anthroposophic medicine teaches that to prevent a disease in the physical body only postpones what will then be produced in another incarnation. Thus, when health measures are undertaken to eliminate the susceptibility to a disease, only the external nature of the illness is eliminated. To deal with the karmic activity from within, Anthroposphy states that spiritual education is required. This does not mean that one should automatically be opposed to vaccination. Steiner indicates that “Vaccination will not be harmful if, subsequent to vaccination, a person receives a spiritual education.”
Or consider this little statistic from the US:
Waldorf schools are the leading Nonmedical Exemption [of vaccinations] schools in various states, such as:
- Waldorf School of Mendocino County (California) – 79.1%
- Tucson Waldorf Schools (Arizona) – 69.6%
- Cedar Springs Waldorf School (California) – 64.7%
- Waldorf School of San Diego (California) – 63.6%
- Orchard Valley Waldorf School (Vermont) – 59.4%
- Whidbey Island Waldorf School (Washington) – 54.9%
- Lake Champlain Waldorf School (Vermont) – 49.6%
- Austin Waldorf School (Texas) – 48%
Or what about this quote?
Q: I am a mother who does not immunize my children. I feel as though I have to keep this a secret. I recently had to take my son to the ER for a tetanus shot when he got a fish hook in his foot, and I was so worried about the doctor asking if his shots were current. His grandmother also does not understand. What do you suggest?
A: You didn’t give your reasons for not vaccinating your children. Perhaps you feel intuitively that vaccinations just aren’t good for children in the long run, but you can’t explain why. If that’s the case, I think your intuition is correct, but in today’s contentious world it is best to understand the reasons for our decisions and actions.
There are many good reasons today for not vaccinating children in the United States I recommend you consult the book, The Vaccination Dilemma edited by Christine Murphy, published by SteinerBooks.
So, where is the evidence that anthroposophy-enthusiasts discourage vaccinations?
It turns out, there is plenty of it! In 2011, I summarised some of it in a review concluding that numerous reports from different countries about measles outbreaks centered around Steiner schools seem nevertheless to imply that a problem does exist. In the interest of public health, we should address it.
All this begs a few questions:
- Are anthroposophy-enthusiasts and their professional organisations generally for or against vaccinations?
- Are the statements above honest or mere distractions from the truth?
- Why are these professional organisations not going after their members who fail to conform with their published stance on vaccination?
I suspect I know the answers.
What do you think?
There is much propaganda for homeopathic vaccinations or homeoprophylaxis (as homeopaths like to call it, in order to give it a veneer of respectability), and on this blog we have discussed it repeatedly. The concept is unproven and dangerous. Yet it is being promoted relentlessly. Currently, I get > 12 million websites when I google ‘homeopathic vaccination’, and there are hundreds of dangerously misleading books and newspaper articles on the subject.

One study that I therefore always wanted to conduct was a trial comparing homeopathic ‘vaccines’ to placebo in terms of immunological response in human volunteers. Somehow, I never managed to get it going. Thus, I was delighted when, a few weeks ago, I received an article for peer-review (I hope I am allowed to disclose this fact here); it was almost exactly the trial I had dreamt of doing one day: the first ever study to test whether there is an antibody response to homeopathic vaccines. Now I am even more delighted to see that it has been published.
Its aim was to compare the antibody response of homeopathic and conventional vaccines and placebo in young adults. The authors hypothesized that there would be no significant difference between homeopathic vaccines and placebo, while there would be a significant increase in antibodies in those received conventional vaccines.
A placebo-controlled, double-blind RCT was conducted where 150 university students who had received childhood vaccinations were assigned to diphtheria, pertussis, tetanus, mumps, measles homeopathic vaccine, placebo, or conventional diphtheria, pertussis, tetanus (Tdap) and mumps, measles, rubella (MMR) vaccines. The primary outcome was a ≥ two-fold increase in antibodies from baseline following vaccination as measured by ELISA. Participants, investigators, study coordinator, data blood drawers, laboratory technician, and data analyst were blinded.
None of the participants in either the homeopathic vaccine or the placebo group showed a ≥ two-fold response to any of the antigens. In contrast, of those vaccinated with Tdap, 68% (33/48) had a ≥ two-fold response to diphtheria, 83% (40/48) to pertussis toxoid, 88% (42/48) to tetanus, and 35% (17/48) of those vaccinated with MMR had a response to measles or mumps antigens (p < 0.001 for each comparison of conventional vaccine to homeopathic vaccine or to placebo). There was a significant increase in geometric mean titres of antibody from baseline for conventional vaccine antigens (p < 0.001 for each), but none for the response to homeopathic antigens or placebo.
The authors concluded that homeopathic vaccines do not evoke antibody responses and produce a response that is similar to placebo. In contrast, conventional vaccines provide a robust antibody response in the majority of those vaccinated.
I think this is in every respect an excellent trial. It should once and for all get rid of what is arguably the homeopathy-cult’s most dangerous idea, namely that highly diluted homeopathic remedies can protect humans against infectious diseases. On this blog, I once called it ‘a danger for both the public and the individual who might believe in it … promoting HP is unethical, irresponsible and possibly even criminal.’
I said it ‘should’ get rid of this nonsense, but will it?
As homeopaths have, for now 200 years, showed themselves utterly impervious to evidence, I for one am not holding my breath. Yet, thanks to this excellent study, we can, when confronted with the notion of homeopathic vaccinations, henceforth point out that it is not just totally implausible but that, in addition, it has also been experimentally shown to be false.
My thanks to the Canadian investigators!
In recent years, I have found myself getting irritated with researchers finishing their evaluation of a so-called alternative medicine (SCAM) with the sentence ‘MORE RESEARCH IS NEEDED’ (or similar). It is irritating because it fails to draw a line under assessments of even the most hopelessly implausible treatment. And, because it leaves things open, it seems to imply that, until further research is available, things can go on as before.
When I realised that plenty of my own papers ended with this statement, I was first taken aback and then even more irritated. How could I have been guilty of repeatedly publishing such nonsense?
Here are just 5 examples of my blundering:
… further trials of high methodological quality with sufficient sample size and follow-up are needed …
Future rigorous randomised clinical trials with larger sample sizes will be necessary …
More and larger long-term, high-quality trials are needed.
But subsequently I re-considered and asked myself: what does ‘MORE RESEARCH IS NEEDED’, a phrase used by so many researchers, really mean?
Contrary to how it seems often to be understood in SCAM, it cannot (should not) mean that, until there is more evidence, we are all free to employ the treatment in question.
Let’s take my first two of my articles quoted above as examples. The first was an assessment of qigong for the primary prevention of cardiovascular disease, and the second an evaluation of acupuncture as a treatment of ankle sprains. When concluding that, in both cases, more research is needed, I did certainly not mean to issue a ‘carte blanche’ to clinicians for carrying on using an evidently unproven SCAM!
What the sentence ‘MORE RESEARCH IS NEEDED’ actually means is almost the opposite:
- at present, the evidence is insufficient;
- more research is needed for a firm verdict;
- currently, the effectiveness of the treatment is unproven;
- it is unwise and possibly even unethical to employ unproven treatments in clinical routine, particularly in situations for which evidence-based therapies are available.
And, if this is so, one also needs to express that NO MORE RESEARCH IS NEEDED, whenever this applies. In the realm of SCAM, this would be the case, if a therapy is hopelessly implausible, for instance. I am glad to say that, occasionally, I did do just that:
… There are hundreds of different homeopathic remedies which can be prescribed for thousands of symptoms in dozens of different dilutions. Thus we would probably need to work flat out for several lifetimes in order to arrive at a conclusion that fully substantiates my opening statement*.
This seems neither possible nor desirable. Perhaps it is preferable to simply combine common sense with the best existing knowledge. These two tell us that 1) homeopathy is biologically implausible, 2) its own predictions seem to be incorrect and 3) the clinical evidence is largely negative…
… the conundrum of homeopathy seems to be solved. ‘Heavens!’ I hear the homeopathic fraternity shout. ‘We need more research!’ But are they correct? How much research is enough to show that any treatment does not work (sorry, is not superior to placebo)? Here we go full circle: should we really spend several lifetimes in order to arrive at a more robust conclusion?
*homeopathy is not better than placebo
This article reported the case of a woman from West Bengal who presented with generalised weakness, weight loss, intermittent diffuse pain abdomen, anorexia, nausea, off and on diarrhoea for eight months. She also noticed darkening of her complexion for six months. Since last 4 months, she had intermittent headache of varying duration, frequency and intensity with tingling and numbness of all four limbs.
Her past medical history was unremarkable except for a chronic anxiety disorder for which she was treated by homeopathy medicine. A neurological examination showed preserved higher mental function, bilateral papilledema with intact other cranial nerves. There was mild motor weakness in both lower limbs, both proximal and distal accompanied by hypotonia without any motor weakness in upper limbs. There was distal sensory deficit in the form of glove and stocking hypoesthesia with reduced deep reflexes in all 4 limbs and bilateral flexor planter response. Gastrointestinal examination revealed non-tender enlarged liver with 16 cm span, mild splenomegaly and mild ascites. Investigations showed mild microcytic hypochromic anaemia (Hb- 9.2 g/dl, MCV-78 fl, MCH-26 pg, MCHC- 31.3 g/dl), low serum iron (27.5 mcg/dl), low TIBC (84.4 mcg/ dl), high serum ferritin (808.6 ng/ml), raised transaminases (AST- 40 IU/L, ALT- 98 IU/L), low serum total protein (4.6 g/dl), low serum albumin (1.9g/dl), globulin (2.7 g/dl) and raised alkaline phosphatase (789 IU/L). Nerve conduction velocity of all four limbs was suggestive of sensorimotor neuropathy.
Unexplained, apparently unrelated multi-system involvement including chronic diarrhoea, presence of liver disease, peripheral neuropathy, idiopathic intracranial hypertension (pseudotumor cerebri ) and characteristic skin lesions suggested chronic arsenicosis. Arsenic level in hair was found to be 1.06 μg/g (N= 0.02-0.2 μg/g) and arsenic level in nail was 1.24 μg/g (N= 0.02-0.5 μg/g) with normal arsenic content (0.03 mg/l) of the drinking water of the locality.

Further questioning revealed that the patient was taking arsenicum album for her anxiety depressive disorder for last one year. The drug was discontinued. Six months later the patient had fully recovered. The authors concluded that an apparently harmless homeopathy medicine may cause multisystem involvement.
The only other case reports of homeopathic arsenic poisoning is this paper:
Case 1 presented with melanosis and keratosis following short-term use of Arsenic Bromide 1-X followed by long-term use of other arsenic-containing homeopathic preparations. Case 2 developed melanotic arsenical skin lesions after taking Arsenicum Sulfuratum Flavum-1-X (Arsenic S.F. 1-X) in an effort to treat his white skin patches. Case 3 consumed Arsenic Bromide 1-X for 6 days in an effort to treat his diabetes and developed an acute gastrointestinal illness followed by leukopenia, thrombocytopenia, and diffuse dermal melanosis with patchy desquamation. Within approximately 2 weeks, he developed a toxic polyneuropathy resulting in quadriparesis. Arsenic concentrations in all three patients were significantly elevated in integument tissue samples. In all three cases, arsenic concentrations in drinking water were normal but arsenic concentrations in samples of the homeopathic medications were elevated. CONCLUSION: Arsenic used therapeutically in homeopathic medicines can cause clinical toxicity if the medications are improperly used.
The authors of the new paper fail to mention the potency of the homeopathic arsenic preparation taken by the patient. As far as I know, in Europe, only high potencies of arsenic are prescribed and dispensed; these remedies contain no or very little arsenic and can thus be considered harmless. In India, however, the 1-X potency seems to be popular, according to the second paper cited above. It describes a dilution of 1: 10 only. It is clear that taking such a remedy would quickly lead to severe toxicity.
This begs the questions: Is it legal to prescribe and dispense such remedies in India or anywhere else? And, in case it is legal, why?
This paper reports a survey amongst European chiropractors during early 2017. Dissemination was through an on-line platform with links to the survey being sent to all European chiropractic associations regardless of European Chiropractors’ Union (ECU) membership and additionally through the European Academy of Chiropractic (EAC). Social media via Facebook groups was also used to disseminate links to the survey.
One thousand three hundred twenty and two responses from chiropractors across Europe representing approximately 17.2% of the profession were collected. Five initial self-determined chiropractic identities were collapsed into 2 groups categorised as orthodox (79.9%) and unorthodox (20.1%); by the latter term, the investigators mean the subluxationists/vitalists.
When comparing the percentage of new patients chiropractors x-rayed, 23% of the unorthodox group x-rayed > 50% of their new patients compared to 5% in the orthodox group. Furthermore, the proportion of respondents reporting > 150 patient encounters per week in the unorthodox group were double compared to the orthodox (22 v 11%). Lastly the proportion of those respondents disagreeing or strongly disagreeing with the statement “In general, vaccinations have had a positive effect on global public health” was 57 and 4% in unorthodox and orthodox categories respectively. Logistic regression models identified male gender, seeing more than 150 patients per week, no routine differential diagnosis, and not strongly agreeing that vaccines have generally had a positive impact on health as highly predictive of unorthodox categorisation.
The authors concluded that despite limitations with generalisability in this survey, the proportion of respondents adhering to the different belief categories are remarkably similar to other studies exploring this phenomenon. In addition, and in parallel with other research, this survey suggests that key practice characteristics in contravention of national radiation guidelines or opposition to evidence based public health policy are significantly more associated with non-orthodox chiropractic paradigms.
|
Country |
N (%) Orthodox |
N (%) Unorthodox |
|---|---|---|
|
Belgium |
51 (92.7) |
4 (7.3) |
|
Germany |
43 (66.2) |
22 (33.8) |
|
Ireland |
31 (79.5) |
8 (20.5) |
|
Italy |
23 (59.0) |
16 (41.0) |
|
Norway |
132 (93.0) |
10 (7.0) |
|
Spain |
34 (43.6) |
44 (56.4) |
|
Sweden |
101 (82.8) |
21 (17.2) |
|
Switzerland |
102 (90.3) |
11 (9.7) |
|
The Netherlands |
81 (82.7) |
17 (17.3) |
|
UK |
236 (80.0) |
59 (20.0) |
Mr William Harvey Lillard was the janitor contracted to clean the Ryan Building where D. D. Palmer’s magnetic healing office was located. In 1895, he became Palmer’s very first chiropractic patient and thus entered the history books. The very foundations of chiropractic are based on this story.

To call the ‘Chiropractor’ a reliable source would probably be stretching it a bit, and there are various versions of the event, even one where BJ Palmer, DD’s son, changed significant details of the story. Nevertheless, it’s a nice story, if there ever was one. But, like many nice stories, it’s just that: a tall tale, a story that might be not based on reality. In this case, the reality getting in the way of a good story is human anatomy.
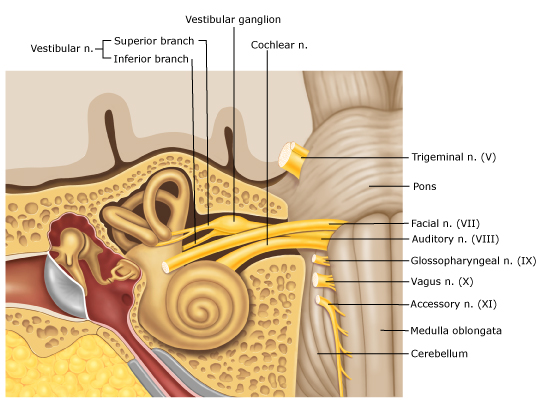
The nerve supply of the inner ear, the bit that enables us to hear, does not, like most other nerves of our body, run through the spine; it comes directly from the brain: the acoustic nerve is one of the 12 cranial nerves.

But chiropractors never let the facts get in the way of a good story! Thus they still tell it and presumably even believe it. Take this website, for instance, as an example of hundreds of similar sources:
… the very first chiropractic patient in history was named William Harvey Lillard, who experienced difficulty hearing due to compression of the nerves leading to his ears. He was treated by “the founder of chiropractic care,” David. D. Palmer, who gave Lillard spinal adjustments in order to reduce destructive nerve compressions and restore his hearing. After doing extensive research about physiology, Palmer believed that Lillard’s hearing loss was due to a misalignment that blocked the spinal nerves that controlled the inner ear (an example of vertebral subluxation). Palmer went on to successfully treat other patients and eventually trained other practitioners how to do the same.
How often have we been told that chiropractors receive a medical training that is at least as thorough as that of proper doctors? But that’s just another tall story, I guess.
Here is the abstract of a paper that makes even the most senior assessor of quackery shudder:
Objective:
The purpose of this report is to describe the manipulation under anesthesia (MUA) treatment of 6 infants with newborn torticollis with a segmental dysfunction at C1/C2.
Clinical Features:
Six infants aged 4 1/2 to 15 months previously diagnosed with newborn torticollis were referred to a doctor of chiropractic owing to a failure to respond adequately to previous conservative therapies. Common physical findings were limited range of motion of the upper cervical spine. Radiographs demonstrated rotational malpositions and translation of atlas on axis in all 6 infants, and 1 had a subluxation of the C1/C2 articulation.
Interventions and Outcome:
Selection was based on complexity and variety of different clinical cases qualifying for MUA. Treatment consisted of 1 mobilization and was performed in the operating room of a children’s hospital by a certified chiropractic physician with the author assisting. Along with the chiropractor and his assistant, a children’s anesthesiologist, 1 to 2 operating nurses, a children’s radiologist, and in 1 case a pediatric surgeon were present. Before the mobilization, plain radiographs of the cervico-occipital area were taken. Three infants needed further investigation by a pediatric computed tomography scan of the area because of asymmetric bony conditions on the plain radiographs. Follow-up consultations at 2, 3, 5, or 6 weeks were done. Patient records were analyzed for restriction at baseline before MUA compared with after MUA treatment for active rotation, passive rotation, and passive rotation in full flexion of the upper cervical spine. All 3 measurements showed significant differences. The long-term outcome data was collected via phone calls to the parents at 6 to 72 months. The initial clinical improvements were maintained.
Conclusion:
These 6 infants with arthrogenic newborn torticollis, who did not respond to previous conservative treatment methods, responded to MUA.
___________________________________________________________________
After reading the full text, I see many very serious problems and questions with this paper; here are 14 of the most obvious ones.
1. A congenital torticollis (that’s essentially what these kids were suffering from) has a good prognosis and does not require such invasive treatments. There is thus no plausible reason to conduct a case series of this nature.
2. A retrospective case series does not allow conclusions about therapeutic effectiveness, yet in the article the author does just that.
3. The same applies to her conclusions about the safety of the interventions.
4. It is unclear how the 6 cases were selected; it seems possible or even likely that they are, in fact, 6 cases of many more treated over a long period of time.
5. If so, this paper is hardly a ‘retrospective case series’; at best it could be called a ‘best case series’.
6. The X-rays or CT scans are unnecessary and potentially harmful.
7. The anaesthesia is potentially very harmful and unjustifiable.
8. The outcome measure is unreliable, particularly if performed by the chiropractor who has a vested interest in generating a positive result.
9. The follow-up by telephone is inadequate.
10. The range of the follow-up period (6-72 months) is unacceptable.
11. The exact way in which informed consent was obtained is unclear. In particular, we would need to know whether the parents were fully informed about the futility of the treatment and its considerable risks.
12. The chiropractor who administered the treatments is not named. Why not?
13. Similarly, it is unclear why the other healthcare professionals involved in these treatments are not named as co-authors of the paper.
14. It is unclear whether ethical approval was obtained for these treatments.
The author seems inexperienced in publishing scientific articles; the present one is poorly written and badly constructed. A Medline research reveals that she has only one other publication to her name. So, perhaps one should not be too harsh in judging her. But what about her supervisors, the journal, its reviewers, its editor and the author’s institution? The author comes from the Department of Chiropractic Medicine, Medical Faculty University, Zurich, Switzerland. On their website, they state:
The Faculty of Medicine of the University of Zurich is committed to high quality teaching and continuing research-based education of students in health care professions. Excellent and internationally recognised scientists and clinically outstanding physicians are at the Faculty of Medicine devoted to patients and public health, to teaching, to the support of young researchers and to academic medicine. The interaction between research and teaching, and their connection to clinical practice play a central role for us…
The Faculty of Medicine of the University of Zurich promotes innovative research in the basic fields of medicine, in the clinical application of knowledge, in personalised medicine, in health care, and in the translational connection between all these research areas. In addition, it encourages the cooperation between primary care and specialised health care.
It seems that, with the above paper, the UZH must have made an exception. In my view, it is a clear case of scientific misconduct and child abuse.
I hear this notion regularly and I have repeatedly published about it (even on this blog).
In Germany, people often express it succinctly WER HEILT HAT RECHT! The argument is so prevalent that I feel like addressing it yet again by publishing a revised version of my Lancet Oncology paper of 2005.
At first glance, the argument seems disarmingly obvious and ethical – above everything else, clinicians must have the welfare of their patients in their minds. All other concerns are secondary.
However, on closer inspection and reflection the argument is not convincing. For the purpose of this discussion, I shall use healing as an example of a SCAM that fulfils the following three criteria:
- it is associated with perceived benefit to some patients;
- it is apparently without harm;
- it is not supported by convincing evidence of efficacy.
Thus, spiritual healing could be replaced, for instance, by homeopathy, Bach Flower Remedies, craniosacral therapy, shark cartilage, etc.
It is obvious that the above argument can apply only, if the treatment in question does not entail meaningful risks. But how do we know it doesn’t? The fact that we are unaware of risks does not mean that none exist. Indeed, none of the above-named treatments are entirely free of adverse effects. Even healing has been associated with unwanted effects. They may be relatively mild and rare, but in the absence of any reporting schemes, this fact is less than conclusive: absence of evidence is not evidence of absence of an (adverse) effect.
The above argument can also be viewed as an endorsement for use of SCAM. If widespread, such endorsements could lead to many patients trusting the many unsubstantiated claims made about SCAM. This would mislead patients into using such therapies as alternatives to conventional treatments—the promotion of alternative cancer cures is rife with recommendations for abandoning conventional cancer therapy, and the effects have repeatedly been shown to be disastrous. Used as an alternative, even the most harmless treatment can become positively life-threatening.
The above argument clearly presupposes that the treatment in question works. But what is meant by this phraseology? Certainly there is no convincing trial evidence that spiritual healing works for cancer or indeed any other condition. “It works” therefore could mean that the treatment helps some patients via a placebo response. There is, of course, nothing wrong with patients benefiting from placebo effects. But do we need placebo treatments to generate a placebo response? The answer is no; even effective therapies will evoke a placebo response. In other words, patients don’t need healing or any other such treatment to profit from a placebo effect. It follows that administering pure placebos to sick patients means cheating them out of an essential element of an effective therapy.
If patients feel better after consulting a healer, they most likely respond to factors like empathy, sympathy, and time provided to them by that therapist. Again, there is absolutely nothing wrong with such a response. To the contrary, responsible orthodox healthcare professionals should cultivate the attitudes that generate it. By directly or indirectly sending our patients to healers to benefit from empathy, etc, we effectively delegate these core qualities of a good therapeutic relationship to others. But delegating empathy to SCAM practitioners would be a most serious mistake for modern medicine to make.
Healers often charge £100 or more per session. Because a placebo response is a free add-on to any well-administered treatment, this seems an unjustifiably high amount of money. Financial exploitation is a subject not much talked about in SCAM – in our recent new book, we included a whole chapter on this issue. We all should think twice before endorsing exploitation.
Perhaps the most detrimental effect of the above argument is outside the realm of medicine. Spiritual healing, like astrology, clairvoyance, mind-reading, etc, is not merely implausible it is mystical nonsense based on ideas that are demonstrably incorrect. Promotion of such nonsense undermines rationality and supports the growth of anti-science and superstition in our society at large. Arguments like that above therefore amount to an endorsement of anti-science. They might sound liberal, tolerant and politically correct but, in truth, they undermine the foundation of rational thinking, hinder progress and lead us back to the Dark Ages.
I have just given two lectures on so-called alternative medicine (SCAM) in France.
Why should that be anything to write home about?
Perhaps it isn’t; but during the last 25 years I have been lecturing all over the world and, even though I live partly in France and speak the language, I never attended a single SCAM-conference there. I have tried for a long time to establish contact with French SCAM-researchers, but somehow this never happened.
Eventually, I came to the conclusion that, although the practice of SCAM is hugely popular in this country, there was no or very little SCAM-research in France. This conclusion seems to be confirmed by simple Medline searches. For instance, Medline lists just 171 papers for ‘homeopathy/France’ (homeopathy is much-used in France), while the figures for Germany and the UK are 490 and 448.
These are, of course, only very rough indicators, and therefore I was delighted to be invited to participate for the first time in a French SCAM-conference. It was well-organised, and I am most grateful to the organisers to have me. Actually, the meeting was about non-pharmacological treatments but the focus was clearly on SCAM. Here are a few impressions purely on the SCAM-elements of this conference.
TERMINOLOGY
Already the title of the conference, ‘Non-pharmacological Interventions: Integrative, Preventive, Complementary and Personalised Medicines‘, contained a confusing shopping-list of terms. The actual lectures offered even more. Clear definitions of these terms were not forthcoming and are, as far as I can see, impossible. This meant that much of the discussion lacked focus. In both my presentations, I used the term ‘alternative medicine’ and stressed that all such umbrella terms are fairly useless. In my view, it is therefore best to name the precise modality (acupuncture, osteopathy, homeopathy etc.) one wants to discuss.
INTEGRATIVE MEDICINE
The term that seemed to dominate the conference was ‘INTEGRATIVE MEDICINE’ (IM). I got the impression that it was employed uncritically by some for bypassing the need for proper evaluation of any specific SCAM. The experts seemed to imply that, because IM is the politically and socially correct approach, there is no longer a need for asking whether the treatments to be integrated actually generate more good than harm. I got the impression that most of these researchers were confusing science with promotion.
RESEARCH METHODOLOGY
The discussions regularly touched upon research methodology – but they did little more than lightly touch it. People tended to lament that ‘conventional research methodology’ was inadequate for assessing SCAM, and that we therefore needed different methods and even paradigms. I did not hear any reasonable explanations in what respect the ‘conventional methodology’ might be insufficient, nor did I understand the concept of an alternative science or paradigm. My caution that double standards in medicine can only be detrimental, seemed to irritate and fell mostly on deaf ears.
RESEARCH QUESTIONS
My own research agenda has always been the efficacy and safety of SCAM; and I still have no doubt that these are the issues that need addressing more urgently than any others. My impression was that, during this conference, the researchers seemed to aim in entirely different directions. One speaker even explained that, if a homeopath is fully convinced of the assumptions of homeopathy, he is entirely within the ethical standards to treat his patients homeopathically, regardless of the fact that homeopathy is demonstrably wrong. Another speaker claimed that there is no doubt any longer about the efficacy of acupuncture; the research question therefore must be how to best implement it in routine healthcare. And yet another expert tried to explain TCM with quantum physics. I have, of course, heard similar nonsense before during such conferences, but rarely did it pass without objection or debate.
RESEARCH FUNDING
The lack of research funding was bemoaned repeatedly. Most researchers seemed to think that they needed dedicated funding streams for SCAM to take account of the need of softer methodologies and the unique nature of SCAM. The argument that there should be only one set of standards for spending scarce research funds – scientific rigor and relevance – was not one shared by the French SCAM enthusiasts. The US example was frequently cited as the one that we ought to follow. In my view, the US example foremost shows impressively that a ring-fenced funding stream for SCAM is a wasteful mistake.
THE COLLEGE
To my surprise I learnt during a conference presentation that there is such a thing as the ‘Collège Universitaire de Médecines Intégratives et Complémentaires‘ (How could I have been unaware of it all those years? Why did I never see any of their published work? Why did they never contact me and cooperate?). Its president is Prof Jacques Kopferschmitt from the University of Strasbourg, and many French Universities are members of this organisation. Here is the abstract of Kopferschmitt’s lecture on the topic of this College:
The multitude of complementary therapies or non-pharmacological interventions (NPIs) first requires pedagogical semantic harmonization to bring down the historical tensions that persist. If users often remain very or too seduced, it is not the same with health professionals! Behind the words, there are concepts that disturb because between efficiency and efficiency the nuances are subtle. However, nothing really stands in the way of modern western medicine, but there are really gaps that we could fill in the face of the growing scale of chronic diseases, the prerogative of the Western world. The need for a university investment in verification, validation and certification is essential in the face of the diversity of offers. The main beneficiaries are health professionals who need to invest in an integrative approach, particularly in France. The CUMIC promotes a different vision of efficiency and effectiveness with a broader vision of multidisciplinary evaluation, which we will discuss the main targets.
Kopferschmitt is Professor of Medical Therapy, which introduced him to a pluralism of approach to health concerns, including innovative by the introduction of the CT in the first and second cycle of medical studies. He is responsible for the teaching of Acupuncture, Auriculotherapy and hypnosis clinic. He is vice President of the Groupe d’Évaluation des Thérapies complémentaires Personnalisées (GETCOP). By founding the association of complementary Therapies at the University hospitals of Strasbourg he coordinates the introduction, teaching and research in both in Hospital and in University, who was organized many seminars on CT. He currently chairs the French University of Integrative and Complementary Medicine College (CUMIC).
This sounded odd to me; however, it got truly bizarre after I looked up what SCAM-research Kopferschmitt or any of the other officers of the College have published. I could not find a single SCAM-article authored by him/them.
DIFFERENT PLANET
Altogether I found the conference enjoyable and was pleased to meet many interesting and very kind people. But I often felt like having arrived on a different planet. Many of the discussions, lectures, ideas, comments, etc. reminded me of 1993, the year I had arrived in the UK to start our research in SCAM. What is more, I fear that French experts involved in real science might feel the same about those colleagues who seem to engage themselves in SCAM research with more enthusiasm than expertise, scientific rigour or track record. The planet I had landed on was one where critical thinking was yet to be discovered, I felt.
ADVICE
Who am I to teach others what to do?
Yes, I do hesitate to give advice – but, after all, I have researched SCAM for 25 years and published more on the subject that any researcher on the planet; and I too was once more of a SCAM-enthusiast as is apparent today. So, for what it’s worth, here is some hopefully constructive advice that crossed my mind while driving home through the beautiful French landscape:
- Sort out the confusion in terminology and define your terms as accurately as you can.
- Try to focus on the research questions that are justifiably the most important ones for improving healthcare.
- Do not attempt to re-invent the wheel.
- Once you have identified a truly relevant research question, read up what has already been published on it.
- While doing this, differentiate between rigorous research and fluff that does not meet this criterion.
- Remember to abandon your own prejudices; research is about finding the truth and not about confirming your beliefs.
- Avoid double standards like the pest.
- Publish your research in top journals and avoid SCAM-journals that nobody outside SCAM takes seriously.
- If you do not have a track record of publishing articles in top journals, please do not pretend to be an expert.
- Involve sceptics in discussions and projects.
- Remember that criticism is a precondition of progress.
I sincerely hope that this advice is not taken the wrong way. I certainly do not mean to hurt anyone’s feelings. What I do want is foremost that my French colleagues don’t have to repeat all the mistakes we did in the UK and that they are able to make swift progress.