Monthly Archives: May 2018
I am not a regular reader of the ‘HALTERNER ZEITUNG’, I have to admit; but this article from the paper came to me because of my interest in homeopathy. It tells a tragic story of a German women who paid dearly for consulting a homeopath.
Here is an excerpt – as it is in German, I will sum up the essence of the story below in English.
_______________________________________________________________________________________________
…Die traurige Geschichte beginnt im Jahr 2012. Die später verstorbene Frau aus Haltern lässt sich von ihrer Ärztin wegen Heiserkeit behandeln und bekommt homöopathische Mittel. Rund zehn Monate später wechselt die Seniorin den Arzt und muss umgehend ins Krankenhaus: Luftröhrenschnitt, Kehlkopf-Entfernung, Krebs. Die Frau verstirbt nach vierjähriger Leidenszeit.
Für Schwester und Tochter war das nicht nur ein Schock, sie machen der Ärztin nun auch schwere Vorwürfe. Aus ihrer Sicht hätte praktisch sofort eine Überweisung zu einem HNO-Arzt und damit eine schulmedizinische Behandlung erfolgen müssen.
Genau das habe die Patientin aber nicht gewollt, sagte die Ärztin. „Sie hat sich immer dagegen gewehrt.“ Angeblich soll das auch dokumentiert sein. Doch auch das ist umstritten. Die Hinterbliebenen werfen der Ärztin nämlich vor, die Unterlagen gefälscht zu haben.
150.000 Euro haben sie als Schmerzensgeld eingeklagt. Dafür sah die Medizinkammer zum jetzigen Zeitpunkt jedoch keine Grundlage. „Die Haftung ist vollkommen offen“, sagte Richter Norbert Schalla.
Man wolle die Leiden der Frau zwar nicht in Abrede stellen. Die Frage sei jedoch, inwieweit die Behandlung eines krankheitsbedingten Leidens tatsächlich verzögert worden sei. „Wir müssten erstens eine Pflichtverletzung und zweitens die Kausalität feststellen“, so Schalla. Beides sei aber außerordentlich schwierig, weil es außer der Ärztin keine Zeugen gebe.
Trotzdem hatten die Richter am Essener Landgericht am Ende eine „Goodwill-Zahlung“ vorgeschlagen, um einen möglicherweise jahrelangen Rechtsstreit zu verhindern. „Manchmal ist es besser, zu einem Abschluss zu kommen, damit man seinen inneren Frieden wiederfinden kann.“
Genau so hat es die Ärztin am Ende wohl auch gesehen. Ob die 10.000 Euro aber wirklich gezahlt werden, hängt allerdings noch von ihrer Haftpflicht-Versicherung ab. Die kann in den nächsten zwei Wochen noch ihr Veto einlegen.
Auch die Hinterbliebenen können die Einigung noch immer widerrufen. Sie müssen von dem Geld nämlich 94 Prozent der Prozesskosten tragen.
_______________________________________________________________________________________________
Here is my summary:
- An elderly woman with a sore throat consults her doctor who happens to be a homeopath.
- The doctor prescribes homeopathic remedies.
- The homeopathic treatment continues for months, evidently without success.
- 10 months later, the patient changes her doctor, and her new physician sends her straight away into hospital.
- There she is diagnosed with throat cancer.
- After 4 years of suffering, the woman dies.
- The patients relatives sue the homeopath for the relatively modest sum of 150 000 Euros.
- The homeopath claims that the old woman had refused to be referred to a specialist and that the case notes provide proof for that claim.
- The relatives suspect that the case notes have been altered retrospectively.
- The judge suggest a ‘good will’ payment of 10 000 Euro.
- The homeopath accepts, but it remains unclear whether the insurance agrees to pay this sum.
- The relatives have to pay 94% of the costs for the court proceedings.
_______________________________________________________________________________________________
Anyone who claims that homeopathy is harmless should remember this story. Similar (but hopefully less dramatic) things happen almost every time a homeopath treats a patient, we argue in our book. The practice of homeopathy is by and large medical neglect. Because homeopathy is employed mostly for minor, self-limiting conditions, the neglect usually remains invisible. However, as soon as homeopath venture to treat serious diseases, the neglect (the deliberate treatment of a disease with an ineffective therapy) becomes obvious.
“This utter hokum is symptomatic of the crass stupidity of the vacuous classes before the lumpen mob rebelled and chopped off their useless heads. Where, oh where, is our mob?”
No, I am not calling for a British re-run of the French revolution. This is a comment that made me chuckle. I found it under an article in the SUNDAY TIMES. As it is about acupuncture, I thought I mention it here and show you a few experts:
_________________________________________________________________________________
… Prince Harry and Meghan Markle had regular appointments with an acupuncturist in the lead-up to their wedding. They were treated by Ross Barr, acupuncturist to the stars, who has been described as “divertingly handsome” by many of his enthusiastic fans and whose treatments have been lauded as “better than Botox”. Beauty experts say his appointments “go faster than Glastonbury tickets”.
Barr, whose treatments deal with anything from infertility to hair loss and relationship problems, is understood to have been regularly treating the couple since Meghan moved to London last year. The treatments are said to have been so successful that Barr and his wife, the actress Eva Birthistle, were invited to the wedding alongside celebrities including Oprah Winfrey, who had acupuncture live on her television show…
Harry, 33, has spoken of his struggles with anxiety and depression after the death of his mother, Diana, Princess of Wales in 1997. In an interview with The Sunday Times in 2016 he also admitted “my body . . . has basically been ruined over the last 10 years of army service”. His father, the Prince of Wales, is renowned for championing alternative and complementary therapies such as homeopathy and acupuncture…
It is thought Harry was keen to try acupuncture as part of a recent health drive to prepare for his wedding. He is reported to have reduced his alcohol consumption and is now regularly seen exercising at the exclusive KX gym in Chelsea, west London. Meghan, 36, is likely to be a fan of Barr’s “anti-wrinkle acupressure facial”, which aims to smooth fine lines and may have contributed to the American former actress’s radiant complexion on her wedding day…
Both Kensington Palace and Barr declined to comment yesterday.
_________________________________________________________________________________
Well, let me offer a few comments then:
- The article is recklessly promotional and, in my view, very poor journalism.
- It does not even include the usual attempt at ‘balance’ where an expert warns at the end of the article that acupuncture is unscientific rubbish.
- There is no good evidence that acupuncture works for any of the conditions mentioned in the article.
- Critical thinking, journalistic ethics, or objective analysis do not seem to be the forte of the author of this regrettable drivel.
Yes, I know … this is not very important. It is merely a little innocent story about some VIPs for gullible consumers.
Innocent?
Perhaps!
But misleading the public about healthcare can also be seen as short-sighted, counter-productive, unethical, and stupid.
The Internet is full of complete nonsense about alternative medicine, as we all know. Much of it could be funny – if it was not so extremely dangerous. Misinformation on health can (and I am afraid does) kill people. One of the worst BS I have seen for a long time is this article entitled ‘Here’s What Oncologists Won’t Tell You About Essential Oils’.
A few excerpts might be of interest:
START OF QUOTES
…The human body resonates at a frequency of 62-78 MHz and scientists believe that diseases start at 58 MHz. Many studies have shown that negative thoughts can reduce our frequency by 12 MHz, while positive thinking raises it by 10.
This means that there are many things that can affect our health in ways we can’t imagine.
According to the latest studies, essential oils can fight cancer thanks to their antibacterial properties and their ability to change the frequency we resonate at.
One of the scientists involved in the study, Bruce Tainio, developed a special Calibrated Frequency Monitor that measures the frequency of essential oils and how they affect us. M. Suhail, an immunologist, says that cancer develops when the DNA in our cells’ nucleus is corrupted.
Essential oils can correct this and repair the code, effectively improving our chances against the terrible disease…
In his book “The Body Electric”, R. O. Becker said that our bodies’ electronic frequency determines our health.
Even Nikola Tesla said that removing outside frequencies can make us more resistant against ailments, while Dr. Otto Warburg discovered over a century ago that our cells have a specific electrical voltage that can drop due to a various factors and trigger diseases such as cancer.
However, science has now discovered that essential oils with higher frequencies can destroy diseases with lower frequencies.
Here’s a list of some of the oils used in the research and their electrical frequencies:
- Juniper – 98 Mhz
- Angelica – 85 Mhz
- Frankincense – 147 MHz
- Rose – 320 Mhz.
- Sandalwood – 96 Mhz
- Helichrysum – 181 MHz
- Peppermint – 78 Mhz
- Lavender – 118 Mhz
In the study, cinnamon, thyme, jasmine and chamomile oils had the best results when put up against breast cancer cells. Chamomile destroyed 93% of the cells in vitro, while thyme destroyed 97% of the cells…
11 oils were examined in total including bitter and sweet fennel, winter savory, peppermint, sage, lavender, chamomile and thyme.
Frankincense oil
According to Suhail, frankincense oil can divide the nucleus of cancer cells from the cytoplasm and prevent it from reproducing. The oil works thanks to the presence of the so-called monoterpenes which have the ability to kill cancer cells.
Frankincense oil works in all stages of cancer and is cytotoxic, meaning it doesn’t destroy healthy cells.
End-stage liver cancer patient
In the study, a patient with end-stage liver cancer was given only a few months left to live. The tumor was inoperable due to the large size, so having nothing to lose, the man decided to try frankincense oil.
He applied a bit under his tongue and topically on the area of the liver, and on his next doctor visit, the tumor has already reduced in size. The patient continued using frankincense oil, and it eventually reduced just enough to be operable. His tumor was later removed and the man is now happily enjoying his life free of cancer.
A child with brain cancer
One of the toughest cases among all the patients in the study was a little girl aged 5 with brain cancer. After exhausting all other options, the parents decided to give the girl a mixture of frankincense and sandalwood oil.
They rubbed the mixture on her feet while also rubbing a bit of lavender on her wrist. After a few months, the cancer was completely defeated!
Bladder cancer patient
Jackie Hogan is a woman suffering from bladder cancer who needed to undergo a surgery for bladder removal due to the cancer.
However, she decided to try using essential oils in her condition and after a few months of applying a mixture of sandalwood and frankincense oil topically on the area, she is cancer-free.
Stage-4 cancer patient
One woman in the research was diagnosed with stage-4 lung cancer which has already spread to other organs in her body.
Instead of agreeing to chemo and surgery, the woman started applying a bit of frankincense oil topically on the affected areas of her body every 2-3 hours and she was completely healthy in 7 months.
Breast cancer patient
A woman diagnosed with advanced breast cancer used a mixture of frankincense and lemongrass oil (topically and under the tongue) to defeat the disease in only a few months.
Cervical cancer patient
A woman with cervical cancer was given only a few months left to live, but thanks to the powers of frankincense oil, she managed to defeat the diseases in a couple of months.
There are many more patients who have managed to defeat different types of cancer using the remarkable powers of various essential oils…
_________________________________________________________________________
END OF QUOTES
Unspeakable nonsense!
I managed to find 4 of the studies this article seems to refer to:
__________________________________________________________________________
Dozmorov MG, Yang Q, Wu W, Wren J, Suhail MM, Woolley CL, Young DG, Fung KM, Lin HK.
Chin Med. 2014 Jul 2;9:18. doi: 10.1186/1749-8546-9-18. eCollection 2014.
- PMID:
- 25006348
Ni X, Suhail MM, Yang Q, Cao A, Fung KM, Postier RG, Woolley C, Young G, Zhang J, Lin HK.
BMC Complement Altern Med. 2012 Dec 13;12:253. doi: 10.1186/1472-6882-12-253.
- PMID:
- 23237355
Woolley CL, Suhail MM, Smith BL, Boren KE, Taylor LC, Schreuder MF, Chai JK, Casabianca H, Haq S, Lin HK, Al-Shahri AA, Al-Hatmi S, Young DG.
J Chromatogr A. 2012 Oct 26;1261:158-63. doi: 10.1016/j.chroma.2012.06.073. Epub 2012 Jun 28.
- PMID:
- 22835693
Suhail MM, Wu W, Cao A, Mondalek FG, Fung KM, Shih PT, Fang YT, Woolley C, Young G, Lin HK.
BMC Complement Altern Med. 2011 Dec 15;11:129. doi: 10.1186/1472-6882-11-129.
- PMID:
- 22171782
____________________________________________________________________________
I do not think that these papers actually show what is claimed above. Specifically, none of the 4 articles refers to clinical effects of essential oil on cancer patients. In fact, according to a 2014 review, and a 2013 paper (the most recent summaries I found) there are no clinical trials of essential oil as a cure for cancer.
The conclusion therefore must be this: Essential oils might be an interesting area of research, yet one has to tell consumers and patients very clearly:
there is no evidence to suggest that using essential oils will change the natural history of any type of cancer.
I have often mocked the lack of progress in homeopathy. Essentially, it has hardly moved an inch since Hahnemann first dreamt it up 200 years ago.
But now, there has been a breakthrough!
Progress at last!!!
It has been reported that Dr. William Edwin Gray III is selling homeopathic ‘sound files’ that can cure a variety of ailments, including life-threatening infections such as Ebola, SARS, swine flu, malaria, typhoid, and cholera.
Yes, SOUND FILES!!!
Short recordings.
If that is not innovative, I don’t know what is.
And it makes sense, of course: homeopathy does not work by pharmacology – the remedies contain nothing – it transmits information. And what better than to pack it into sounds?
This is a breakthrough that will save millions from disease. One cannot be surprised that such a discovery attracts jealousy. Instead of nominating Dr Gray for a Nobel Prize, the Californian Medical Board has promptly threatened to revoke his license.
Petty bastards!
Short-sighted idiots!
In an accusation filed with the state, the medical board writes that Dr. William Gray III, MD, who is an internist in Saratoga, California and licensed to practice medicine in California, is guilty of gross negligence and requested a hearing in which the board would decide whether to possibly revoke or suspend his license. Understandably, the genius Gray is concerned. In an interview with the Los Angeles Times, Gray said he had decided not to contest the board’s allegations, saying it would cost too much money to fight. He added: “Frankly, I think we’d lose anyway.”
That leaves Gray’s fate entirely in the hands of the board, which will make a decision in coming weeks. The prospect of losing his medical license worries Gray, but he is nevertheless stoically confident. He has focused on homeopathy ever since he finished medical school. Because homeopathy doesn’t require a medical license, he assumes that he can go about his business without a medical licence.
Gray knows that sound waves can carry “the energetic signal in homeopathic remedies” to treat patients. He collects that energy by placing vials of homeopathic remedies in electrified wire coils and recording any emitted sounds. With this method, he produced 263 “eRemedies,” which are 13-second recordings (available as either .wav or .MP3 files) which sound like hissing.
Patients—who are not examined or even seen by Gray—can get his therapy via Gray’s website, mdinyourhand.com. Subsequently, they can “dose” themselves with the recordings to treat a variety of ailments. The website lists 23 ailments the recordings treat. Patients simply answers a series of questions about their condition and the website serves up the appropriate eRemedy. The individual recordings cost $5 a pop and patients can subscribe to receive 25 for $100. Already in 2014, Gray “created [a] campaign to treat Ebola via cellphone, curing 3 out of 3 within 4 hours simply by playing the appropriate eRemedy several times in an hour.”
Cutting edge science, I’d say! But true genius is often dismissed or even ridiculed. What really disappoints me though is that not even Gray’s fellow homeopaths find it in themselves to support him. Robert Stewart, founder of the New York School of Homeopathy, wrote to the Times in an email: “He’s on his own in this.”
Shame on you Robert, and shame on everyone else (I have already seen plenty of scathing/jealous comments on Twitter) who cannot recognise the first true progress in homeopathy since 200 years.
Canadian naturopaths are reported to be under investigation for practising and promoting ‘CEASE’. It might be worth therefore, to explain what this treatment amounts to.
The name ‘CEASE’ is the abbreviation of Complete Elimination of Autistic Spectrum Expression. Here are 7 points that are, I think, relevant:

- CEASE therapy was developed by Dr Tinus Smits (1946-2010) in the Netherlands. Smits had practised as a lay-homeopath for many years before he decided to study medicine.
- Smits became convinced that autism is caused by a child’s exposure to an accumulation of toxic substances and published several books about his theory.
- In his experience (as far as I can see, Smits never published a single scientific paper in the peer-reviewed literature) autism is caused by an accumulation of different toxins. About 70% is due to vaccines, 25% to toxic medication and other toxic substances, 5% to some diseases.
- According to the ‘like cures like’ principle of homeopathy, Smits claimed that autism must be cured by applying homeopathic doses of the substances which caused autism. Step by step all assumed causative factors (vaccines, regular medication, environmental toxic exposures, effects of illness, etc.) are detoxified with the homeopathically prepared substances that has been administered prior to the onset of autism. Smits and his followers believe that this procedure clears out the “energetic field of the patient from the imprint of toxic substances or diseases”.
- One problem with this concept is that it flies in the face of science. There is no reason to believe that autism is caused by the exposure to toxins. In fact, CEASE turns out to be a layered monster of bogus assumption. The first layer is a false theory of the pathogenesis of autism; the second is the ‘like cures like’ myth of homeopathy; the third is the notion that ‘potentisation’ (dilution for you and me) renders substances not less but more potent; the fourth is the nonsensical concept of detoxification.
- Another, perhaps even more important problem is that there is no evidence that the CEASE therapy is clinically effective.
 Despite all this, many homeopaths and naturopaths have enthusiastically adopted the CEASE therapy, and some have discovered that there is money in running courses and awarding diplomas. Alerted to this abuse by concerned consumers, the UK Professional Standards Authority recently forced the UK ‘Society of Homeopaths’ to issue a statement saying: A number of Society members have been trained in CEASE and make reference to it in their marketing. While this is acceptable, members should be aware the title, meaning ‘Complete Elimination of Autistic Spectrum Expression’ is misleading. RSHoms must not suggest that they are capable of a complete cure of autism as this would be unethical and in breach of the Code of Ethics. The Society does not endorse any aspects of CEASE therapy contrary to NHS guidance and nor should RSHoms. In particular on vaccination, homeopathic prophylaxis, and the use of dietary supplements. It is beyond standard homeopathic practice to provide advice on the use of supplements and therefore any guidance given should be in line with the NHS Guidelines. The Society expects its members to comply with its Code of Ethics and statements on vaccination and homeopathic prophylaxis at all times, and any breaches may be treated as disciplinary matters. In order to ensure patient safety and In line with our guidelines, we will check the websites and marketing of all our members on a regular basis to ensure they are adhering to this statement. (Personally I find it astonishing that the SoH seems to declare CEASE ‘acceptable’.)
Despite all this, many homeopaths and naturopaths have enthusiastically adopted the CEASE therapy, and some have discovered that there is money in running courses and awarding diplomas. Alerted to this abuse by concerned consumers, the UK Professional Standards Authority recently forced the UK ‘Society of Homeopaths’ to issue a statement saying: A number of Society members have been trained in CEASE and make reference to it in their marketing. While this is acceptable, members should be aware the title, meaning ‘Complete Elimination of Autistic Spectrum Expression’ is misleading. RSHoms must not suggest that they are capable of a complete cure of autism as this would be unethical and in breach of the Code of Ethics. The Society does not endorse any aspects of CEASE therapy contrary to NHS guidance and nor should RSHoms. In particular on vaccination, homeopathic prophylaxis, and the use of dietary supplements. It is beyond standard homeopathic practice to provide advice on the use of supplements and therefore any guidance given should be in line with the NHS Guidelines. The Society expects its members to comply with its Code of Ethics and statements on vaccination and homeopathic prophylaxis at all times, and any breaches may be treated as disciplinary matters. In order to ensure patient safety and In line with our guidelines, we will check the websites and marketing of all our members on a regular basis to ensure they are adhering to this statement. (Personally I find it astonishing that the SoH seems to declare CEASE ‘acceptable’.)
 PS
PS
In case you are interested to consider the arguments from a proponent (one of the Canadian naturopaths who are currently under investigation for practising CEASE), read this article: https://www.drzimmermann.org/blog-vaccines-homeopathy-autism-cease-therapy/cease-therapy-misconceptions-and-truths
My previous post praised the validity and trustworthiness of Cochrane reviews. This post continues in the same line.
Like osteoarthritis, acute stroke has been a condition for which acupuncture-fans prided themselves of being able to produce fairly good evidence. A Cochrane review of 2005, however, was inconclusive and concluded that the number of patients is too small to be certain whether acupuncture is effective for treatment of acute ischaemic or haemorrhagic stroke. Larger, methodologically-sound trials are required.
So, 13 years later, we do have more evidence, and it would be interesting to know what the best evidence tells us today. This new review will tell us because it is the update of the previous Cochrane Review originally published in 2005.
The authors sought randomized clinical trials (RCTs) of acupuncture started within 30 days from stroke onset compared with placebo or sham acupuncture or open control (no placebo) in people with acute ischemic or haemorrhagic stroke, or both. Needling into the skin was required for acupuncture. Comparisons were made versus (1) all controls (open control or sham acupuncture), and (2) sham acupuncture controls.
Two review authors applied the inclusion criteria, assessed trial quality and risk of bias, and extracted data independently. They contacted study authors to ask for missing data and assessed the quality of the evidence by using the GRADE approach. The primary outcome was defined as death or dependency at the end of follow-up.
In total, 33 RCTs with 3946 participants were included. Twenty new trials with 2780 participants had been completed since the previous review. Outcome data were available for up to 22 trials (2865 participants) that compared acupuncture with any control (open control or sham acupuncture) but for only six trials (668 participants) that compared acupuncture with sham acupuncture control. The authors downgraded the evidence to low or very low quality because of risk of bias in included studies, inconsistency in the acupuncture intervention and outcome measures, and imprecision in effect estimates.
When compared with any control (11 trials with 1582 participants), findings of lower odds of death or dependency at the end of follow-up and over the long term (≥ three months) in the acupuncture group were uncertain (odds ratio [OR] 0.61, 95% confidence interval [CI] 0.46 to 0.79; very low-quality evidence; and OR 0.67, 95% CI 0.53 to 0.85; eight trials with 1436 participants; very low-quality evidence, respectively) and were not confirmed by trials comparing acupuncture with sham acupuncture (OR 0.71, 95% CI 0.43 to 1.18; low-quality evidence; and OR 0.67, 95% CI 0.40 to 1.12; low-quality evidence, respectively).In trials comparing acupuncture with any control, findings that acupuncture was associated with increases in the global neurological deficit score and in the motor function score were uncertain (standardized mean difference [SMD] 0.84, 95% CI 0.36 to 1.32; 12 trials with 1086 participants; very low-quality evidence; and SMD 1.08, 95% CI 0.45 to 1.71; 11 trials with 895 participants; very low-quality evidence).
These findings were not confirmed in trials comparing acupuncture with sham acupuncture (SMD 0.01, 95% CI -0.55 to 0.57; low-quality evidence; and SMD 0.10, 95% CI -0.38 to 0.17; low-quality evidence, respectively).Trials comparing acupuncture with any control reported little or no difference in death or institutional care at the end of follow-up (OR 0.78, 95% CI 0.54 to 1.12; five trials with 1120 participants; low-quality evidence), death within the first two weeks (OR 0.91, 95% CI 0.33 to 2.55; 18 trials with 1612 participants; low-quality evidence), or death at the end of follow-up (OR 1.08, 95% CI 0.74 to 1.58; 22 trials with 2865 participants; low-quality evidence).
The incidence of adverse events (eg, pain, dizziness, fainting) in the acupuncture arms of open and sham control trials was 6.2% (64/1037 participants), and 1.4% of these (14/1037 participants) discontinued acupuncture. When acupuncture was compared with sham acupuncture, findings for adverse events were uncertain (OR 0.58, 95% CI 0.29 to 1.16; five trials with 576 participants; low-quality evidence).
The authors concluded that this updated review indicates that apparently improved outcomes with acupuncture in acute stroke are confounded by the risk of bias related to use of open controls. Adverse events related to acupuncture were reported to be minor and usually did not result in stopping treatment. Future studies are needed to confirm or refute any effects of acupuncture in acute stroke. Trials should clearly report the method of randomization, concealment of allocation, and whether blinding of participants, personnel, and outcome assessors was achieved, while paying close attention to the effects of acupuncture on long-term functional outcomes.
These cautious conclusions might be explained by the fact that Chinese researchers are reluctant to state anything overtly negative about any TCM therapy. Recently, one expert who spoke out was even imprisoned for criticising a TCM product! But in truth, this review really shows that acupuncture has no convincing effect in acute stroke.
And for me, this conclusion is fascinating. I have been involved in acupuncture/stroke research since the early 1990s.
Our RCT produced a resounding negative result concluding that acupuncture is not superior to sham treatment for recovery in activities of daily living and health-related quality of life after stroke, although there may be a limited effect on leg function in more severely affected patients.
Our 1996 systematic review concluded that the evidence that acupuncture is a useful adjunct for stroke rehabilitation is encouraging but not compelling.
By 2001, more data had become available but the conclusion became even less encouraging: there is no compelling evidence to show that acupuncture is effective in stroke rehabilitation.
Finally, by 2010, there were 10 RCT and we were able to do a meta-analysis of the data. We concluded that our meta-analyses of data from rigorous randomized sham-controlled trials did not show a positive effect of acupuncture as a treatment for functional recovery after stroke.
Yes, my reviews were on slightly different research questions. Yet, they do reveal how a critical assessment of the slowly emerging evidence had to arrive at more and more negative conclusions about the role of acupuncture in the management of stroke patients. For a long time, this message was in stark contrast to what acupuncture-fans were claiming. I wonder whether they will now finally change their mind.
I have said it often, and I say it again: I do like well-conducted systematic reviews; and Cochrane reviews are usually the best, i. e. most transparent, most thorough and least biased. Thus, I was pleased to see a new Cochrane review of acupuncture aimed at assessing the benefits and harms of acupuncture in patients with hip OA.
The authors included randomized controlled trials (RCTs) that compared acupuncture with sham acupuncture, another active treatment, or no specific treatment; and RCTs that evaluated acupuncture as an addition to another treatment. Major outcomes were pain and function at the short term (i.e. < 3 months after randomization) and adverse events.
Six RCTs with 413 participants were included. Four RCTs included only people with OA of the hip, and two included a mix of people with OA of the hip and knee. All RCTs included primarily older participants, with a mean age range from 61 to 67 years, and a mean duration of hip OA pain from two to eight years. Approximately two-thirds of participants were women. Two RCTs compared acupuncture versus sham acupuncture; the other four RCTs were not blinded. All results were evaluated at short-term (i.e. four to nine weeks after randomization).In the two RCTs that compared acupuncture to sham acupuncture, the sham acupuncture control interventions were judged believable, but each sham acupuncture intervention was also judged to have a risk of weak acupuncture-specific effects, due to placement of non-penetrating needles at the correct acupuncture points in one RCT, and the use of penetrating needles not inserted at the correct points in the other RCT. For these two sham-controlled RCTs, the risk of bias was low for all outcomes.
The combined analysis of two sham-controlled RCTs gave moderate quality evidence of little or no effect in reduction in pain for acupuncture relative to sham acupuncture. Due to the small sample sizes in the studies, the confidence interval includes both the possibility of moderate benefit and the possibility of no effect of acupuncture (120 participants; Standardized Mean Difference (SMD) -0.13, (95% Confidence Interval (CI) -0.49 to 0.22); 2.1 points greater improvement with acupuncture compared to sham acupuncture on 100 point scale (i.e., absolute percent change -2.1% (95% CI -7.9% to 3.6%)); relative percent change -4.1% (95% CI -15.6% to 7.0%)). Estimates of effect were similar for function (120 participants; SMD -0.15, (95% CI -0.51 to 0.21)). No pooled estimate, representative of the two sham-controlled RCTs, could be calculated or reported for the quality of life outcome.
The four other RCTs were unblinded comparative effectiveness RCTs, which compared (additional) acupuncture to four different active control treatments. There was low quality evidence that addition of acupuncture to the routine primary care that RCT participants were receiving from their physicians was associated with statistically significant and clinically relevant benefits, compared to the routine primary physician care alone, in pain (1 RCT; 137 participants; mean percent difference -22.9% (95% CI -29.2% to -16.6%); relative percent difference -46.5% (95% CI -59.3% to -33.7%)) and function (mean percent difference -19.0% (95% CI -24.41 to -13.59); relative percent difference -38.6% (95% CI -49.6% to -27.6%)). There was no statistically significant difference for mental quality of life and acupuncture showed a small, significant benefit for physical quality of life.
The effects of acupuncture compared with either advice plus exercise or NSAIDs are uncertain. The authors are also uncertain whether acupuncture plus patient education improves pain, function, and quality of life, when compared to patient education alone.
In general, the overall quality of the evidence for the four comparative effectiveness RCTs was low to very low, mainly due to the potential for biased reporting of patient-assessed outcomes due to lack of blinding and sparse data.
Information on safety was reported in 4 RCTs. Two RCTs reported minor side effects of acupuncture, which were primarily minor bruising, bleeding, or pain at needle insertion sites.
The authors concluded that acupuncture probably has little or no effect in reducing pain or improving function relative to sham acupuncture in people with hip osteoarthritis. Due to the small sample size in the studies, the confidence intervals include both the possibility of moderate benefits and the possibility of no effect of acupuncture. One unblinded trial found that acupuncture as an addition to routine primary physician care was associated with benefits on pain and function. However, these reported benefits are likely due at least partially to RCT participants’ greater expectations of benefit from acupuncture. Possible side effects associated with acupuncture treatment were minor.
This is an excellent review of data that (because of contradictions, methodological limitations, heterogeneity etc.) are not easy to evaluate fairly. The review shows that previous verdicts about acupuncture for osteoarthritis might have been too optimistic. Acupuncture has no or only very small specific therapeutic effects. As we have much better therapeutic options for this condition, it means that acupuncture can no longer be recommended as an effective therapy.
That surely must be big news in the little world of acupuncture!
I have been personally involved in several similar reviews:
In 1997, I concluded that the most rigorous studies suggest that acupuncture is not superior to sham-needling in reducing pain of osteoarthritis: both alleviate symptoms to roughly the same degree.
In 2006, the balance of evidence seemed to have shifted and more positive data had emerged; consequently our review concluded that sham-controlled RCTs suggest specific effects of acupuncture for pain control in patients with peripheral joint OA. Considering its favourable safety profile acupuncture seems an option worthy of consideration particularly for knee OA. Further studies are required particularly for manual or electro-acupuncture in hip OA.
Now, it seems that my initial conclusion of 1996 was more realistic. To me this is a fascinating highlight on the fact that in EBM, we change our minds based on the current best evidence. By contrast, in alternative medicine, as we have often lamented on this blog, minds do not easily change and all too often dogma seems to reign.
The new Cochrane review is important in several ways. Firstly, it affirms an appropriately high standard for such reviews. Secondly, it originates from a research team that has, in the past, been outspokenly pro-acupuncture; it is therefore unlikely that the largely negative findings were due to an anti-acupuncture bias. Thirdly – and most importantly – osteoarthritis has been THE condition for which even critical reviewers had to admit that there was at least some good, positive evidence.
It seems therefore, that yet again a beautiful theory has been slain by an ugly fact.
Remember when an international delegation of homeopaths travelled to Liberia to cure Ebola?
Virologists and other experts thought at the time that this was pure madness. But, from the perspective of dedicated homeopaths who have gone through ‘proper’ homeopathic ‘education’ and have the misfortune to believe all the nonsense they have been told, this is not madness. In fact, the early boom of homeopathy, about 200 years ago, was based not least on the seemingly resounding success homeopaths had during various epidemics.
I fully understand that homeopath adore this type of evidence – it is good for their ego! And therefore, they tend to dwell on it and re-hash it time and again. The most recent evidence for this is a brand-new article entitled ‘Homeopathic Prevention and Management of Epidemic Diseases’. It is such a beauty that I present you the original abstract without change:
START OF QUOTE
___________________________________________________________________________
Homeopathy has been used to treat epidemic diseases since the time of Hahnemann, who used Belladonna to treat scarlet fever. Since then, several approaches using homeopathy for epidemic diseases have been proposed, including individualization, combination remedies, genus epidemicus, and isopathy.
METHODS:
The homeopathic research literature was searched to find examples of each of these approaches and to evaluate which were effective.
RESULTS:
There is good experimental evidence for each of these approaches. While individualization is the gold standard, it is impractical to use on a widespread basis. Combination remedies can be effective but must be based on the symptoms of a given epidemic in a specific location. Treatment with genus epidemicus can also be successful if based on data from many practitioners. Finally, isopathy shows promise and might be more readily accepted by mainstream medicine due to its similarity to vaccination.
CONCLUSION:
Several different homeopathic methods can be used to treat epidemic diseases. The challenge for the future is to refine these approaches and to build on the knowledge base with additional rigorous trials. If and when conventional medicine runs out of options for treating epidemic diseases, homeopathy could be seen as an attractive alternative, but only if there is viable experimental evidence of its success.
END OF QUOTE
____________________________________________________________________________________
I don’t need to stress, I think, that such articles are highly irresponsible and frightfully dangerous: if anyone ever took the message that homeopathy has the answer to epidemic seriously, millions might die.
The reasons why epidemiological evidence of this nature is wrong has been discussed before on this blog; I therefore only need to repeat them:
In the typical epidemiological case/control study, one large group of patients [A] is retrospectively compared to another group [B]. In our case, group A has been treated homeopathically, while group B received the treatments available at the time. It is true that several of such reports seemed to suggest that homeopathy works. But this does by no means prove anything; the result might have been due to a range of circumstances, for instance:
- group A might have been less ill than group B,
- group A might have been richer and therefore better nourished,
- group A might have benefitted from better hygiene in the homeopathic hospital,
- group A might have received better care, e. g. hydration,
- group B might have received treatments that made the situation not better but worse.
Because these are RETROSPECTIVE studies, there is no way to account for these and many other factors that might have influenced the outcome. This means that epidemiological studies of this nature can generate interesting results which, in turn, need testing in properly controlled studies where these confounding factors are adequately controlled for. Without such tests, they are next to worthless for recommendations regarding clinical practice.
In essence, this means that epidemiological evidence of this type can be valuable for generating hypotheses which, in turn, need testing in rigorous clinical trials. Without these tests, the evidence can be dangerously misleading.
But, of course, Jennifer Jacobs, the author of the new article, knows all this – after all, she has been employed for many years by the Department of Epidemiology, School of Public Health and Community Medicine, University of Washington, Seattle, Washington, United States!
In this case, why does she re-hash the old myth of homeopathy being the answer to epidemics?
I do not know the answer to this question, but I do know that she is a convinced homeopath with plenty of papers on the subject.
And what sort of journal would publish such dangerous, deeply unethical rubbish?
It is a journal we have discussed several before; its called HOMEOPATHY.
This journal is, I think, remarkable: not even homeopaths would deny that homeopathy is a most controversial subject. One would therefore expect that the editorial board of the leading journal of homeopathy (Impact Factor = 1.16) has a few members who are critical of homeopathy and its assumptions. Yet, I fail to spot a single such person of the board of HOMEOPATHY. Please have a look yourself and tell me, if you can identify such an individual:
Editor
Peter Fisher
FRCP, FFHom, London, UK
Senior Deputy Editor
Robert T. Mathie
BSc (Hons), PhD, London, UK
Deputy Editors
Leoni Bonamin
Paulista University, São Paulo, Brazil
Menachem Oberbaum
Shaare Zedek Medical Center, Jerusalem, Israel
Ethics Adviser
Kate Chatfield
University of Central Lancashire, Preston, UK
Editorial Advisory Board
Cees Baas
Centre for Integrative Psychiatry, Groningen, The Netherlands
Stephan Baumgartner
University of Witten-Herdecke, Germany
Iris R. Bell
University of Arizona, USA
Jayesh Bellare
Indian Institute of Technology, Mumbai, India
Philippe Belon
Centre de Recherche et de Documentation Thérapeutique, France
Brian Berman
University of Maryland, School of Medicine, USA
Martien Brands
Centre for Integrative Care, Amsterdam, The Netherlands
Michael Carlston
University of California, Santa Rosa, USA
Kusum S. Chand
Pushpanjali Crosslay Hospital, Ghaziabad, India
Martin Chaplin
London South Bank University, UK
Flávio Dantas
University of Uberlândia, Brazil
Peter Darby
Faculty of Homeopathy, UK
Jonathan Davidson
Duke University, USA
Jean-Louis Demangeat
Haguenau Hospital, France
Christian Endler
Interuniversity College Graz/Castle of Seggau, Austria
Madeleine Ennis
Queen’s University Belfast, UK
Edoardo Felisi
Milan, Italy
Peter Gregory
Veterinary Dean, Faculty of Homeopathy, UK
German Guajardo-Bernal
University of Baja California, Mexico
Carla Holandino Quaresma
Universidade Federal do Rio de Janeiro, Brazil
Jennifer Jacobs
University of Washington, USA
Wayne Jonas
Samueli Institute, Alexandria, USA
Lee Kayne
Faculty of Homeopathy, UK
Steven Kayne
Glasgow Homoeopathic Hospital, UK
David Lilley
Pretoria, South Africa
Klaus Linde
Technical University, Munich, Germany
Russell Malcolm
Faculty of Homeopathy, UK
Raj K. Manchanda
Central Council for Research in Homoeopathy, New Delhi, India
David Peters
University of Westminster, London, UK
Bernard Poitevin
Association Française pour la Recherche en Homéopathie, France
David Reilly
Glasgow Homoeopathic Hospital, UK
David Riley
Integrative Medicine Institute, Portland, USA
ALB Rutten
Breda, The Netherlands
Jürgen Schulte
University of Technology, Sydney, Australia
Trevor Thompson
University of Bristol, UK
André Thurneysen
Centre de médecines intégrées, Switzerland
Alexander Tournier
Homeopathy Research Institute, UK
Francis Treuherz
London, UK
Robbert van Haselen
International Institute for Integrated Medicine, Kingston, UK
Michel Van Wassenhoven
Unio Homeopathica Belgica, Belgium
Harald Walach
University of Witten-Herdecke, Germany
Fred Wiegant
University of Utrecht, The Netherlands
___________________________________________________________________________
I rest my case.
 Once upon a time, the University of Exeter prided itself of having the ‘1st chair in complementary medicine’ in the country. That was in 1993, when I was appointed to that position. I then recruited a team of motivated researchers, and we soon managed to become the world’s leading research group in our field. Together, we published more papers on alternative medicine in the peer reviewed medical literature than any other team before or since, and we managed to get an international reputation for high-quality critical assessments of alternative medicine. Unfortunately, not all people were happy; some even seemed to be distinctly unhappy because few of our findings were as they had hoped.
Once upon a time, the University of Exeter prided itself of having the ‘1st chair in complementary medicine’ in the country. That was in 1993, when I was appointed to that position. I then recruited a team of motivated researchers, and we soon managed to become the world’s leading research group in our field. Together, we published more papers on alternative medicine in the peer reviewed medical literature than any other team before or since, and we managed to get an international reputation for high-quality critical assessments of alternative medicine. Unfortunately, not all people were happy; some even seemed to be distinctly unhappy because few of our findings were as they had hoped.
In 2012/13, I retired under circumstances that, I am afraid, were not to the credit or integrity of my peers (the full and rather sad story has been told in my memoir). Since then, I have the status of Emeritus Professor; in that role, I give occasional lectures, publish about one book per year, run this blog, and generally enjoy life. There is not much that can bother me these days…
…at least, this is what I thought until I saw this announcement by Exeter University.
It informed me that the University of Exeter has decided to “offer a range of complementary therapies at a discounted rate to Staff at both Streatham and St Lukes Campus.”
Treatments are not cheap but members will receive the following reductions:
- 60 minutes + treatments £5.00 discount
- 45 minute treatments £4.00 discount
- 30 minute treatments £3.00 discount.
You want to know which therapies precisely are on offer?
Here is a selection of the treatments they are providing:
- Hot Stone Back Massage
- Reflexology
- Pregnancy Massage
- Indian Head Massage
- Acupressure points
- Yoga movements
- Somatic movements
- Chi Qong
- Nutrition based Ayurvedic system of health
- Tai Yoga massage
Impressive?
Yes, most impressive – particularly as none of the therapies listed above are supported by anything that looks remotely like good evidence!
So, has my University gone raving mad?
Have they joined the legion of charlatans promoting nonsense?
Do they perhaps want to score even more brownie-points with HRH, the Prince of Wales?
One would assume so … but wait … they added a disclaimer to their announcement:
Whilst the University is pleased to welcome complementary practitioners to the campus and support greater access to a range of wellbeing services, we are not in a position to actively condone the effectiveness of such treatments. However, Reed Mews Wellbeing Centre wants to promote choice and encourage individuals to make informed decisions regarding the management of their health needs.
AHHH – I AM SO PLEASED – THAT’S ALRIGHT THEN!
Many of you will know that JAMA is one of the most respected medical journals. It is therefore surprising that, within the period of a few days, they published not one but two dodgy RCTs of alternative treatments.
The new trial was aimed at determining whether the addition of chiropractic care to usual medical care results in better pain relief and pain-related function when compared with usual medical care alone.
The study was designed as a pragmatic comparative effectiveness clinical trial using adaptive allocation was conducted from September 28, 2012, to February 13, 2016, at three US military medical centres. Eligible participants were active-duty US service members aged 18 to 50 years with low back pain from a musculoskeletal source. The intervention period was 6 weeks. Usual medical care included self-care, medications, physical therapy, and pain clinic referral. Chiropractic care included spinal manipulative therapy in the low back and adjacent regions and additional therapeutic procedures such as rehabilitative exercise, cryotherapy, superficial heat, and other manual therapies.
Primary outcomes were low back pain intensity (Numerical Rating Scale; scores ranging from 0 [no low back pain] to 10 [worst possible low back pain]) and disability (Roland Morris Disability Questionnaire; scores ranging from 0-24, with higher scores indicating greater disability) at 6 weeks. Secondary outcomes included perceived improvement, satisfaction (Numerical Rating Scale; scores ranging from 0 [not at all satisfied] to 10 [extremely satisfied]), and medication use.
In total, 750 patients were enrolled. Statistically significant site × time × group interactions were found in all models. Adjusted mean differences in scores at week 6 were statistically significant in favour of usual medical care plus chiropractic care compared with usual medical care alone overall for low back pain intensity (mean difference, −1.1; 95% CI, −1.4 to −0.7), disability (mean difference, −2.2; 95% CI, −3.1 to −1.2), and satisfaction (mean difference, 2.5; 95% CI, 2.1 to 2.8) as well as at each site. Adjusted odd ratios at week 6 were also statistically significant in favour of usual medical care plus chiropractic care overall for perceived improvement (odds ratio = 0.18; 95% CI, 0.13-0.25) and self-reported pain medication use (odds ratio = 0.73; 95% CI, 0.54-0.97). No serious adverse events were reported.
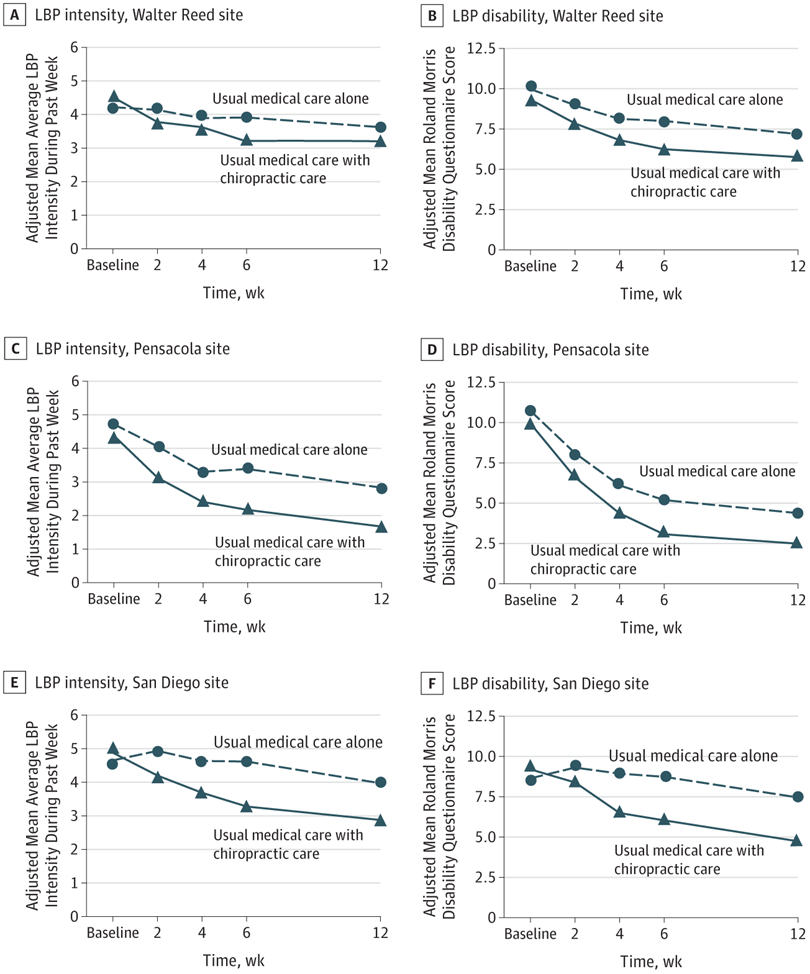
The authors concluded that chiropractic care, when added to usual medical care, resulted in moderate short-term improvements in low back pain intensity and disability in active-duty military personnel. This trial provides additional support for the inclusion of chiropractic care as a component of multidisciplinary health care for low back pain, as currently recommended in existing guidelines. However, study limitations illustrate that further research is needed to understand longer-term outcomes as well as how patient heterogeneity and intervention variations affect patient responses to chiropractic care.
Regular readers will have spotted it straight away: This trial follows the infamous ‘A+B versus B’ design. It will almost always generate a positive result – so much so that it is a waste of time to run the study because we know its findings before it has started. And if this is so, the trial is arguably even unethical.
The reason is, of course, that the study design does not control for placebo effects. And this means that even an utterly useless treatment will produce a (false-positive) result as long as it generates a placebo effect. Some of the authors of the present study are experienced researchers and clearly know all this. This is why they call their study a ‘pragmatic’ trial. But even with pragmatic trials, one cannot get away with murder!
As far as I can see, there are even two ‘murders’ here:
- The authors stated that their aim was to determine whether the addition of chiropractic care to usual medical care results in better pain relief and pain-related function when compared with usual medical care alone. I would argue that their study did not live up to this aim. As it did not control for placebo effects, it cannot possibly test the effectiveness of chiropractic care per se.
- The authors concluded that their trial provides additional support for the inclusion of chiropractic care as a component of multidisciplinary health care for low back pain. I would argue that this is quite simply wrong. The results are in perfect agreement with the assumption that chiropractic care is a placebo, and few would argue that the inclusion of a pure placebo can be recommended.
Compared to these major issues, my other concerns are mere trivialities:
- The trial tested spinal manipulation plus a whole bunch of physiotherapeutic intervention. I bet my last shirt that the chiro-community will claim that it demonstrated the effectiveness of chiropractic spinal manipulations. Already the very first sentence of the present paper’s discussion section goes into this direction: The changes in patient-reported pain intensity and disability as well as satisfaction with care and low risk of harms favoring UMC with chiropractic care found in this pragmatic clinical trial are consistent with the existing literature on spinal manipulative therapy…
- In their abstract, the authors (several of whom are chiropractors) state that there were no serious adverse effects (the paper is extremely thin on providing details about how adverse effects were assessed, verified, categorised etc.). What about non-serious adverse effects (arguably LBP is a minor condition, so minor adverse effects are relevant!)? In the paper, they enlighten us that of the 43 adverse effects reported by participants receiving UMC with chiropractic care, 38 were described as muscle or joint stiffness attributed to chiropractic care (37 events) or physical therapy (1 event), 1 was reported as indistinct symptoms following an epidural injection, 3 were described as pain, tingling, or sensitivity in an extremity without reference to a specific treatment, and 1 was a lower-extremity burning sensation for 20 minutes following spinal manipulative therapy. In my view, this is sufficiently important to be mentioned also in the abstract.
- The authors remain totally silent when it comes to the discussion of the effect sizes. To me, they seem to be moderate. Are they at all clinically relevant. I feel that the discussion of a PRAGMATIC trial must include this pragmatically important issue.