spinal manipulation
Vertebral artery dissections (VAD) are a rare but important cause of ischemic stroke, especially in younger patients. Many etiologies have been identified, including motor vehicle accidents, cervical fractures, falls, physical exercise, and, as I have often discussed on this blog, cervical chiropractic manipulation. The goal of this study was to investigate the subgroup of patients who suffered a chiropractor-associated injury and determine how their prognosis compared to other-cause VAD.
The researchers, neurosurgeons from Chicago, conducted a retrospective chart review of 310 patients with vertebral artery dissections who presented at their institution between January 2004 and December 2018. Variables included demographic data, event characteristics, treatment, radiographic outcomes, and clinical outcomes measured using the modified Rankin Scale.
Overall, 34 out of our 310 patients suffered a chiropractor-associated injury. These patients tended to be younger (p = 0.01), female (p = 0.003), and have fewer comorbidities (p = 0.005) compared to patients with other-cause VADs. The characteristics of the injuries were similar, but chiropractor-associated injuries appeared to be milder at discharge and at follow-up. A higher proportion of the chiropractor-associated group had injuries in the 0-2 mRS range at discharge and at 3 months (p = 0.05, p = 0.04) and no patients suffered severe long-term neurologic consequences or death (0% vs. 9.8%, p = 0.05). However, when a multivariate binomial regression was performed, these effects dissipated and the only independent predictor of a worse injury at discharge was the presence of a cervical spine fracture (p < 0.001).
The authors concluded that chiropractor-associated injuries are similar to VADs of other causes, and apparent differences in the severity of the injury are likely due to demographic differences between the two populations.
The authors of the present paper are clear: “chiropractic manipulations are a risk factor for vertebral artery dissections.” This fact is further supported by a host of other investigations. For instance, the Canadian Stroke Consortium found that 28% of strokes following cervical artery dissection were preceded by chiropractic neck manipulation. Dziewas et al. obtained a similar rate in patients with vertebral artery dissections. Many chiropractors are in denial; however, this is merely due to their overt conflicts of interest.
My conclusions from the accumulated evidence are this:
Spinal manipulations of the upper spine should not be routinely used for any condition. Patients who nevertheless insist on having them must be made aware of the risks and give informed consent.
This systematic review assessed the effects and reliability of sham procedures in manual therapy (MT) trials in the treatment of back pain (BP) in order to provide methodological guidance for clinical trial development.
Different databases were screened up to 20 August 2020. Randomized controlled trials involving adults affected by BP (cervical and lumbar), acute or chronic, were included. Hand contact sham treatment (ST) was compared with different MT (physiotherapy, chiropractic, osteopathy, massage, kinesiology, and reflexology) and to no treatment. Primary outcomes were BP improvement, the success of blinding, and adverse effects (AE). Secondary outcomes were the number of drop-outs. Dichotomous outcomes were analyzed using risk ratio (RR), continuous using mean difference (MD), 95% CIs. The minimal clinically important difference was 30 mm changes in pain score.
A total of 24 trials were included involving 2019 participants. Most of the trials were of chiropractic manipulation. Very low evidence quality suggests clinically insignificant pain improvement in favor of MT compared with ST (MD 3.86, 95% CI 3.29 to 4.43) and no differences between ST and no treatment (MD -5.84, 95% CI -20.46 to 8.78).ST reliability shows a high percentage of correct detection by participants (ranged from 46.7% to 83.5%), spinal manipulation is the most recognized technique. Low quality of evidence suggests that AE and drop-out rates were similar between ST and MT (RR AE=0.84, 95% CI 0.55 to 1.28, RR drop-outs=0.98, 95% CI 0.77 to 1.25). A similar drop-out rate was reported for no treatment (RR=0.82, 95% 0.43 to 1.55).
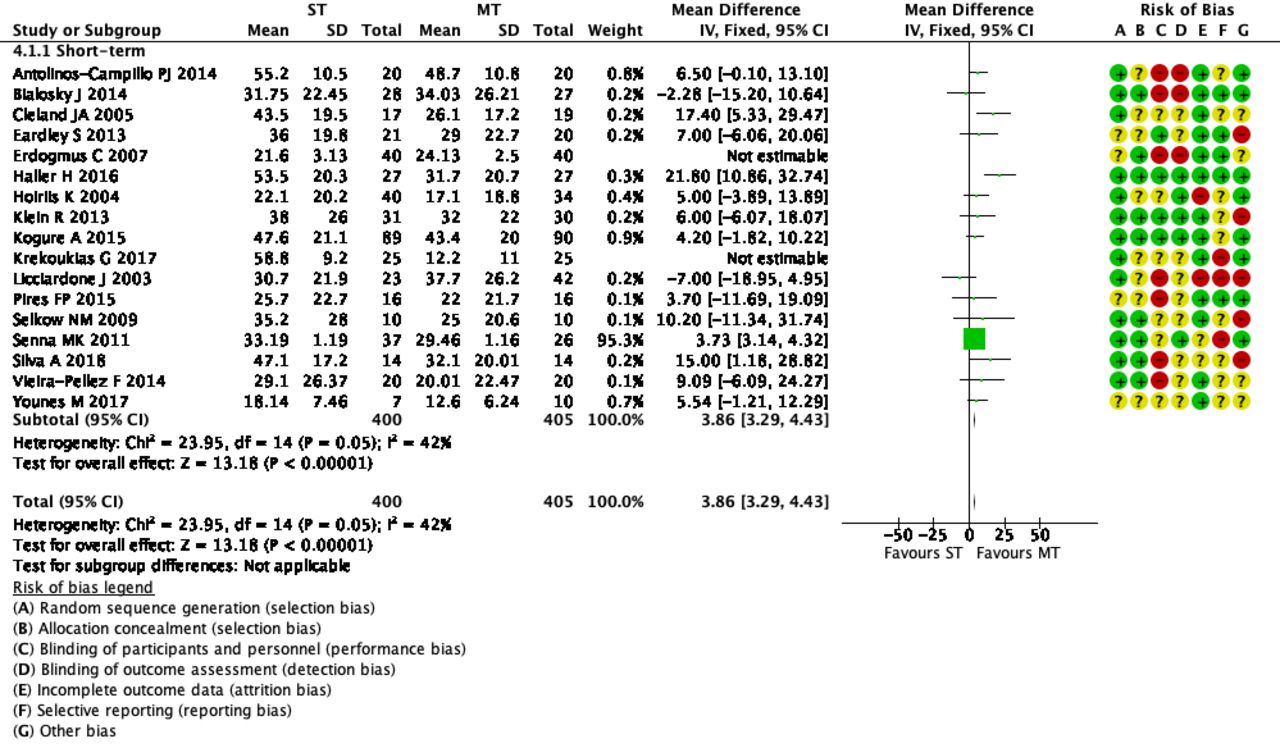 The authors concluded that MT does not seem to have clinically relevant effect compared with ST. Similar effects were found with no treatment. The heterogeneousness of sham MT studies and the very low quality of evidence render uncertain these review findings. Future trials should develop reliable kinds of ST, similar to active treatment, to ensure participant blinding and to guarantee a proper sample size for the reliable detection of clinically meaningful treatment effects.
The authors concluded that MT does not seem to have clinically relevant effect compared with ST. Similar effects were found with no treatment. The heterogeneousness of sham MT studies and the very low quality of evidence render uncertain these review findings. Future trials should develop reliable kinds of ST, similar to active treatment, to ensure participant blinding and to guarantee a proper sample size for the reliable detection of clinically meaningful treatment effects.
The optimal therapy for back pain does not exist or has not yet been identified; there are dozens of different approaches but none has been found to be truly and dramatically effective. Manual therapies like chiropractic and osteopathy are often used, and some data suggest that they are as good (or as bad) as most other options. This review confirms what we have discussed many times previously (e.g. here), namely that the small positive effect of MT, or specifically spinal manipulation, is largely due to placebo.
Considering this information, what is the best treatment for back pain sufferers? The answer seems obvious: it is a therapy that is as (in)effective as all the others but causes the least harm or expense. In other words, it is not chiropractic nor osteopathy but exercise.
My conclusion:
avoid therapists who use spinal manipulation for back pain.
The purpose of this study was to describe changes in opioid-therapy prescription rates after a family medicine practice included on-site chiropractic services. It was designed as a retrospective analysis of opioid prescription data. The database included opioid prescriptions written for patients seeking care at the family medicine practice from April 2015 to September 2018. In June 2016, the practice reviewed and changed its opioid medication practices. In April 2017, the practice included on-site chiropractic services. Opiod-therapy use was defined as the average rate of opioid prescriptions overall medical providers at the practice.
There was a significant decrease of 22% in the average monthly rate of opioid prescriptions after the inclusion of chiropractic services (F1,40 = 10.69; P < .05). There was a significant decrease of 32% in the prescribing rate of schedule II opioids after the inclusion of chiropractic services (F2,80 = 6.07 for the Group × Schedule interaction; P < .05). The likelihood of writing schedule II opioid prescriptions decreased by 27% after the inclusion of chiropractic services (odds ratio, 0.73; 95% confidence interval, 0.59-0.90). Changes in opioid medication practices by the medical providers included prescribing a schedule III or IV opioid rather than a schedule II opioid (F6,76 = 29.81; P < .05) and a 30% decrease in the daily doses of opioid prescriptions (odds ratio, 0.70; 95% confidence interval, 0.50-0.98).
The authors concluded that this study demonstrates that there were decreases in opioid-therapy prescribing rates after a family medicine practice included on-site chiropractic services. This suggests that inclusion of chiropractic services may have had a positive effect on prescribing behaviors of medical physicians, as they may have been able to offer their patients additional nonpharmaceutical options for pain management.
The authors are correct in concluding the inclusion of chiropractic services MAY have had a positive effect. And then again, it may not!
Cause and effect cannot be established by correlation alone.
CORRELATION IS NOT CAUSATION!
And even if the inclusion of chiropractic services caused the positive effect, it would not prove that chiropractic is effective in the management of pain. It would only mean that the physicians had an option that helped them to write fewer opioid prescriptions. Had they hired a crystal healer or a homeopath or a faith healer or any other practitioner of an ineffective therapy, the findings might have been very similar.
The long and short of it is this: if we want to use fewer opioids, there is only one way to achieve it: we must prescribe less.
Absurd claims about spinal manipulative therapy (SMT) improving immune function have increased substantially during the COVID-19 pandemic. Is there any basis at all for such notions?
The objective of this systematic review was to identify, appraise, and synthesize the scientific literature on the efficacy and effectiveness of SMT in preventing the development of infectious disease or improving disease-specific outcomes in patients with infectious disease and to examine the association between SMT and selected immunological, endocrine, and other physiological biomarkers.
A literature search of MEDLINE, the Cumulative Index to Nursing and Allied Health Literature, the Index to Chiropractic Literature, the Cochrane Central Register of Controlled Trials, and Embase was conducted. Randomized clinical trials and cohort studies were included. Eligible studies were critically appraised, and evidence with high and acceptable quality was synthesized using the Synthesis Without Meta-Analysis guideline.
A total of 2593 records were retrieved; after exclusions, 50 full-text articles were screened, and 16 articles reporting the findings of 13 studies comprising 795 participants were critically appraised. No clinical studies were located that investigated the efficacy or effectiveness of SMT in preventing the development of infectious disease or improving disease-specific outcomes among patients with infectious disease. Eight articles reporting the results of 6 high- and acceptable-quality RCTs comprising 529 participants investigated the effect of SMT on biomarkers. Spinal manipulative therapy was not associated with changes in lymphocyte levels or physiological markers among patients with low back pain or participants who were asymptomatic compared with sham manipulation, a lecture series, and venipuncture control groups. Spinal manipulative therapy was associated with short-term changes in selected immunological biomarkers among asymptomatic participants compared with sham manipulation, a lecture series, and venipuncture control groups.
The authors concluded that no clinical evidence was found to support or refute claims that SMT was efficacious or effective in changing immune system outcomes. Although there were limited preliminary data from basic scientific studies suggesting that SMT may be associated with short-term changes in immunological and endocrine biomarkers, the clinical relevance of these findings is unknown. Given the lack of evidence that SMT is associated with the prevention of infectious diseases or improvements in immune function, further studies should be completed before claims of efficacy or effectiveness are made.
I fully agree with the data as summarised in this paper. Yet, I find the conclusions a bit odd. The authors of this paper are chiropractors who declare the following conflicts of interest: Dr Côté reported receiving grants from the College of Chiropractors of British Columbia during the conduct of the study and grants from the Canadian Chiropractic Research Foundation, travel expenses from the World Federation of Chiropractic, and personal fees from the Canadian Chiropractic Protective Association outside the submitted work. Dr Cancelliere reported receiving grants from the Canadian Chiropractic Research Foundation outside the submitted work. Dr Mior reported receiving grants from the College of Chiropractors of British Columbia during the conduct of the study and grants from the Canadian Chiropractic Association and the Ontario Chiropractic Association outside the submitted work. Dr Hogg-Johnson reported receiving grants from the College of Chiropractors of British Columbia during the conduct of the study and grants from the Canadian Chiropractic Research Foundation outside the submitted work. No other disclosures were reported. The research was supported by funding from the College of Chiropractors of British Columbia to Ontario Tech University, the Canada Research Chairs program (Dr Côté), and the Canadian Chiropractic Research Foundation (Dr Cancelliere).
Would authors independent of chiropractic influence have drawn the same conclusions? I doubt it! While I do appreciate that chiropractors published these negative findings prominently, I feel the conclusions could easily be put much clearer:
There is no clinical evidence to support claims that SMT is efficacious or effective in changing immune system outcomes. Further studies in this area are not warranted.
Low back pain must be one of the most frequent reasons for patients to seek out some so-called alternative medicine (SCAM). It would therefore be important that the information they get is sound. But is it?
The present study sought to assess the quality of web-based consumer health information available at the intersection of LBP and CAM. The investigators searched Google using six unique search terms across four English-speaking countries. Eligible websites contained consumer health information in the context of CAM for LBP. They used the DISCERN instrument, which consists of a standardized scoring system with a Likert scale from one to five across 16 questions, to conduct a quality assessment of websites.
Across 480 websites identified, 32 were deemed eligible and assessed using the DISCERN instrument. The mean overall rating across all websites 3.47 (SD = 0.70); Summed DISCERN scores across all websites ranged from 25.5-68.0, with a mean of 53.25 (SD = 10.41); the mean overall rating across all websites 3.47 (SD = 0.70). Most websites reported the benefits of numerous CAM treatment options and provided relevant information for the target audience clearly, but did not adequately report the risks or adverse side-effects adequately.
The authors concluded that despite some high-quality resources identified, our findings highlight the varying quality of consumer health information available online at the intersection of LBP and CAM. Healthcare providers should be involved in the guidance of patients’ online information-seeking.
In the past, I have conducted several similar surveys, for instance, this one:
Background: Low back pain (LBP) is expected to globally affect up to 80% of individuals at some point during their lifetime. While conventional LBP therapies are effective, they may result in adverse side-effects. It is thus common for patients to seek information about complementary and alternative medicine (CAM) online to either supplement or even replace their conventional LBP care. The present study sought to assess the quality of web-based consumer health information available at the intersection of LBP and CAM.
Methods: We searched Google using six unique search terms across four English-speaking countries. Eligible websites contained consumer health information in the context of CAM for LBP. We used the DISCERN instrument, which consists of a standardized scoring system with a Likert scale from one to five across 16 questions, to conduct a quality assessment of websites.
Results: Across 480 websites identified, 32 were deemed eligible and assessed using the DISCERN instrument. The mean overall rating across all websites 3.47 (SD = 0.70); Summed DISCERN scores across all websites ranged from 25.5-68.0, with a mean of 53.25 (SD = 10.41); the mean overall rating across all websites 3.47 (SD = 0.70). Most websites reported the benefits of numerous CAM treatment options and provided relevant information for the target audience clearly, but did not adequately report the risks or adverse side-effects adequately.
Conclusion: Despite some high-quality resources identified, our findings highlight the varying quality of consumer health information available online at the intersection of LBP and CAM. Healthcare providers should be involved in the guidance of patients’ online information-seeking.
Or this one:
Background: Some chiropractors and their associations claim that chiropractic is effective for conditions that lack sound supporting evidence or scientific rationale. This study therefore sought to determine the frequency of World Wide Web claims of chiropractors and their associations to treat, asthma, headache/migraine, infant colic, colic, ear infection/earache/otitis media, neck pain, whiplash (not supported by sound evidence), and lower back pain (supported by some evidence).
Methods: A review of 200 chiropractor websites and 9 chiropractic associations’ World Wide Web claims in Australia, Canada, New Zealand, the United Kingdom, and the United States was conducted between 1 October 2008 and 26 November 2008. The outcome measure was claims (either direct or indirect) regarding the eight reviewed conditions, made in the context of chiropractic treatment.
Results: We found evidence that 190 (95%) chiropractor websites made unsubstantiated claims regarding at least one of the conditions. When colic and infant colic data were collapsed into one heading, there was evidence that 76 (38%) chiropractor websites made unsubstantiated claims about all the conditions not supported by sound evidence. Fifty-six (28%) websites and 4 of the 9 (44%) associations made claims about lower back pain, whereas 179 (90%) websites and all 9 associations made unsubstantiated claims about headache/migraine. Unsubstantiated claims were made about asthma, ear infection/earache/otitis media, neck pain,
Conclusions: The majority of chiropractors and their associations in the English-speaking world seem to make therapeutic claims that are not supported by sound evidence, whilst only 28% of chiropractor websites promote lower back pain, which is supported by some evidence. We suggest the ubiquity of the unsubstantiated claims constitutes an ethical and public health issue.
The findings were invariably disappointing and confirmed those of the above paper. As it is nearly impossible to do much about this lamentable situation, I can only think of two strategies for creating progress:
- Advise patients not to rely on Internet information about SCAM.
- Provide reliable information for the public.
Both describe the raison d’etre of my blog pretty well.
The General Chiropractic Council’s (GCC) Registrant Survey 2020 was conducted in September and October 2020. Its aim was to gain valuable insights into the chiropractic profession to improve the GCC’s understanding of chiropractic professionals’ work and settings, qualifications, job satisfaction, responsibilities, clinical practice, future plans, the impact of the COVID-19 pandemic on practice, and optimism and pessimism about the future of the profession.
The survey involved a census of chiropractors registered with the GCC. It was administered online, with an invitation email was sent to every GCC registrant, followed by three reminders for those that had not responded to the survey. An open-access online survey was also available for registrants to complete if they did not respond to the mailings. This was promoted using the GCC website and social media channels. In total, 3,384 GCC registrants were eligible to take part in the survey. A fairly miserable response rate of 28.6% was achieved.
Here are 6 results that I found noteworthy:
- Registrants who worked in clinical practice were asked if performance was monitored at any of the clinical practices they worked at. Just over half (55%) said that it was and a third (33%) said it was not. A further 6% said they did not know and 6% preferred not to say. Of those who had their performance monitored, only 37% said that audits of clinical care were conducted.
- Registrants working in clinical practice were asked if any of their workplaces used a patient safety incident reporting system. Just under six in ten (58%) said at least one of them did, whilst 23% said none of their workplaces did. A further 12% did not know and 7% preferred not to say.
- Of the 13% who said they had a membership of a Specialist Faculty, a third (33%) said it was in paediatric chiropractic, 25% in sports chiropractic, and 16% in animal chiropractic. A further 13% said it was in pain and the same proportion (13%) in orthopaedics.
- Registrants who did not work in chiropractic research were asked if they intended to work in that setting in the next three years. Seven in ten (70%) said they did not intend to work in chiropractic research in the next three years, whilst 25% did not know or were undecided. Only 5% said they did intend to work in chiropractic research.
- Registrants were also asked how easy it is to keep up to date with recommendations and advances in clinical practice. Overall, two-thirds (67%) felt it was easy and 30% felt it was not.
- Registrants were asked in the survey whether they felt optimistic or pessimistic about the future of the profession over the next three years. Overall, half (50%) said they were optimistic and 23% were pessimistic. A further 27% said they were neither optimistic nor pessimistic.
Perhaps even more noteworthy are those survey questions and subject areas that might have provided interesting information but were not included in the survey. Here are some questions that spring into my mind:
- Do you believe in the concept of subluxation?
- Do you treat conditions other than spinal problems?
- How frequently do you use spinal manipulations?
- How often do you see adverse effects of spinal manipulation?
- Do you obtain informed consent from all patients?
- How often do you refer patients to medical doctors?
- Do you advise in favour of vaccinations?
- Do you follow the rules of evidence-based medicine?
- Do you offer advice about prescribed medications?
- Which supplements do you recommend?
- Do you recommend maintenance treatment?
I wonder why they were not included.
Osteopathic manipulative treatment (OMT) is popular, but does it work? On this blog, we have often discussed that there are good reasons to doubt it.
This study compared the efficacy of standard OMT vs sham OMT for reducing low back pain (LBP)-specific activity limitations at 3 months in persons with nonspecific subacute or chronic LBP. It was designed as a prospective, parallel-group, single-blind, single-center, sham-controlled randomized clinical trial. 400 patients with nonspecific subacute or chronic LBP were recruited from a tertiary care center in France starting and randomly allocated to interventions in a 1:1 ratio.
Six sessions (1 every 2 weeks) of standard OMT or sham OMT delivered by osteopathic practitioners. For both
experimental and control groups, each session lasted 45 minutes and consisted of 3 periods: (1) interview focusing on pain location, (2) full osteopathic examination, and (3) intervention consisting of standard or sham OMT. In both groups, practitioners assessed 7 anatomical regions for dysfunction (lumbar spine, root of mesentery, diaphragm, and atlantooccipital, sacroiliac, temporomandibular, and talocrural joints) and applied sham OMT to all areas or standard OMT to those that were considered dysfunctional.
The primary endpoint was the mean reduction in LBP-specific activity limitations at 3 months as measured by the self-administered Quebec Back Pain Disability Index. Secondary outcomes were the mean reduction in LBP-specific activity limitations; mean changes in pain and health-related quality of life; number and duration of sick leave, as well as the number of LBP episodes at 12 months, and the consumption of analgesics and nonsteroidal anti-inflammatory drugs at 3 and 12 months. Adverse events were self-reported at 3, 6, and 12 months.
A total of 200 participants were randomly allocated to standard OMT and 200 to sham OMT, with 197 analyzed in each group; the median (range) age at inclusion was 49.8 (40.7-55.8) years, 235 of 394 (59.6%) participants were women, and 359 of 393 (91.3%) were currently working. The mean (SD) duration of the current LBP episode had been 7.5 (14.2) months. Overall, 164 (83.2%) patients in the standard OMT group and 159 (80.7%) patients in the sham OMT group had the primary outcome data available at 3 months.
The mean (SD) Quebec Back Pain Disability Index scores were:
- 31.5 (14.1) at baseline and 25.3 (15.3) at 3 months in the OMT-group,
- 27.2 (14.8) at baseline and 26.1 (15.1) at 3 months in the sham group.
The mean reduction in LBP-specific activity limitations at 3 months was -4.7 (95% CI, -6.6 to -2.8) and -1.3 (95% CI, -3.3 to 0.6) for the standard OMT and sham OMT groups, respectively (mean difference, -3.4; 95% CI, -6.0 to -0.7; P = .01). At 12 months, the mean difference in mean reduction in LBP-specific activity limitations was -4.3 (95% CI, -7.6 to -1.0; P = .01), and at 3 and 12 months, the mean difference in mean reduction in pain was -1.0 (95% CI, -5.5 to 3.5; P = .66) and -2.0 (95% CI, -7.2 to 3.3; P = .47), respectively. There were no statistically significant differences in other secondary outcomes. Four and 8 serious adverse events were self-reported in the standard OMT and sham OMT groups, respectively, though none was considered related to OMT.
The authors concluded that standard OMT had a small effect on LBP-specific activity limitations vs sham OMT. However, the clinical relevance of this effect is questionable.
This study was funded the French Ministry of Health and sponsored by the Département de la Recherche Clinique et du Développement de l’Assistance Publique-Hôpitaux de Paris. It is of exceptionally good quality. Its findings are important, particularly in France, where osteopaths have become as numerous as their therapeutic claims irresponsible.
In view of what we have been repeatedly discussing on this blog, the findings of the new trial are unsurprising. Osteopathy is far less well supported by sound evidence than osteopaths want us to believe. This is true, of course, for the plethora of non-spinal claims, but also for LBP. The French authors cite previously published evidence that is in line with their findings: In a systematic review, Rubinstein and colleagues compared the efficacy of manipulative treatment to sham manipulative treatment on LBP-specific activity limitations and did not find evidence of differences at 3 and 12 months (3 RCTs with 573 total participants and 1 RCT with 63 total participants). Evidence was considered low to very low quality. When merging the present results with these findings, we found similar standardized mean difference values at 3months (−0.11 [95% CI, −0.24 to 0.02]) and 12 months (−0.11 [95% CI, −0.33 to 0.11]) (4 RCTs with 896 total participants and 2 RCTs with 320 total participants).
So, what should LBP patients do?
The answer is, as I have often mentioned, simple: exercise!
And what will the osteopaths do?
The answer to this question is even simpler: they will find/invent reasons why the evidence is not valid, ignore the science, and carry on making unsupported therapeutic claims about OMT.
This study compared the effectiveness of two osteopathic manipulative techniques on clinical low back symptoms and trunk neuromuscular postural control in male workers with chronic low back pain (CLBP).
Ten male workers with CLBP were randomly allocated to two groups: high-velocity low-amplitude (HVLA) manipulation or muscle energy techniques (MET). Each group received one therapy per week for both techniques during 7 weeks of treatment.

Pain and function were measured by using the Numeric Pain-Rating Scale, the McGill Pain Questionnaire, and the Roland Morris Disability Questionnaire. The lumbar flexibility was assessed by Modified Schober Test. Electromyography (EMG) and force platform measurements were used for evaluation of trunk muscular activation and postural balance, respectively at three different times: baseline, post-intervention, and 15 days later.
Both techniques were effective (p < 0.01) in reducing pain with large clinical differences (-1.8 to -2.8) across immediate and after 15 days. However, no significant effect between groups and times was found for other variables, namely neuromuscular activation, and postural balance measures.
The authors concluded that both techniques (HVLA thrust manipulation and MET) were effective in reducing back pain immediately and 15 days later. Neither technique changed the trunk neuromuscular activation patterns nor postural balance in male workers with LBP.
There is, of course, another conclusion that fits the data just as well: both techniques were equally ineffective.
A report just published by the UK GENERAL CHIROPRACTIC COUNCIL (the regulator of chiropractors in the UK) entitled Public perceptions research Enhancing professionalism, February 2021 makes interesting reading. It is based on a consumer survey for which the national online public survey was conducted by djs research in 2020 with a nationally representative sample of 1,002 UK adults (aged 16+). From this sample, 243 UK adults had received chiropractic treatment and were surveyed on their experiences of visiting a chiropractor.
Hidden amongst intensely boring stuff, we find a heading entitled Communicating potential risks. This caught my interest. Here is the unabbreviated section:
The findings show that patients want to understand the potential risks of treatment – alongside information on cost, this is the most important factor for patients considering chiropractic care. In fact, having any risks communicated before embarking on treatment scores 83 out of 100 on a scale of importance.
Many patients report receiving this information from their chiropractor. Seventy per cent of those who have received chiropractic treatment agree that risks were communicated before treatment commenced.
What does that suggest?
- Patients want to know about the risks of the treatments chiropractors administer.
- 30% of all patients are not being given this information.
This roughly confirms what has long been known:
MANY CHIROPRACTORS DO NOT OBTAIN INFORMED CONSENT FROM THEIR PATIENTS AND THUS VIOLATE MEDICAL ETHICS.
The questions that arise from this information are these:
- As the GCC has long known about this situation, why have they not adequately addressed it?
- Now that they are reminded of this flagrant ethical violation, what are they planning to do about it?
- What measures will they put in place to make sure that all chiropractors observe the elementary rules of medical ethics in the future?
- What reprimands do they plan for members who do not comply?
Guest post by Ken McLeod
On 31 March 2020, the Chiropractic Board of Australia issued a statement1 to all Australian chiropractors that they:
“should not make advertising claims on preventing or protecting patients and health consumers from contracting COVID-19 or accelerating recovery from COVID-19. To do so involves risk to public safety and may be unlawful advertising. For example, we are seeing some advertising claims that spinal adjustment/manipulation, acupuncture and some products confer or boost immunity or enhance recovery from COVID-19 when there is no acceptable evidence in support.
“Advertisers must be able to provide acceptable evidence of any claims made about treatments that benefit patients/health consumers. We will consider taking action against anyone found to be making false or misleading claims about COVID-19 in advertising. If the advertiser is a registered health practitioner, breaching advertising obligations is also a professional conduct matter which may result in disciplinary action, especially where advertising is clearly false, misleading or exploitative.”
What could be clearer than that?
So what was published by a registered chiropractor on 16 March 2020, two weeks before the Board’s warning, and is still on his website 10 months later? You guessed it, a video on the website of chiropractor Morgan Weber, a video ‘Coronavirus – Balancing the hysteria…’, 2 in which he says:
– the COVID-19 19 pandemic is all ‘hysteria’ and ‘what have we got to worry about’, because ‘Our body, (has) 51 trillion cells’ vs ‘A one single-cell virus,’ (sic.) ‘51 trillion cells that orchestrate our immune system, every function. Yet we seem to have more faith and trust in ‘medicine’ than we do in this amazing body we call home. Crazy, right? Crazy.’
Weber further downplays the crisis by saying ‘Enough of this nonsense about the big bad bug and all the worry about washing your hands.’
Weber, after denigrating evidence-based medicine, recommends instead:
– ‘Keep up with your chiropractic adjustments….’
Weber is a registered chiropractor practicing at Wave Chiropractic, Maroochydore, Queensland, Australia. His AHPRA registration is CHI0001601286. Weber’s webpage home site is at https://www.wavechiropractic.com.au/index.php
WEBER’S VIDEO:
Since 16 March 2020 Weber has posted a video on his website a video ‘Coronavirus – Balancing the hysteria…’. 3
Weber says:
BEGINS TRANSCRIPT
00:00. Hi everyone. Hasn’t it been fascinating lately? The news, the hysteria. Everything has gone almost upside-down. Crazy. I found it so fascinating.
00:12. So today we thought we would have a bit of a chat and sort of balance the scales and the story getting told out there in the mass media. I hope you’ve got your toilet paper stockpiled and sorted ha ha ha ha. It’s hilarious to see people coming and going with huge amounts under their arms as they come out of the grocery store. Crazy isn’t it, crazy times.
00:42. So let’s think about if for a second, and if we bypass all that hysteria and noise and just think a little bit about this. Our body, 51 trillion cells. A one single-cell virus. My gosh. What have we got to worry about? We have this amazing system. 51 trillion cells that orchestrate our immune system, every function. Yet we seem to have more faith and trust in ‘medicine’ than we do in this amazing body we call home. Crazy, right? Crazy.
01:20 ‘The other story, the other sort of facts behind what we do, and I (unintelligible) told a fair few of you of this already, how the immune system works. So, across the road from Waves, we have a really kind of bare patch of grass, just before you go onto the beach. Now if I took a handful of seeds. Now this is an analogy for how our system works, and how amazing our body’s immune system is. If I took a bunch of seeds and dropped them onto the ground, some grass seeds, not all of those seeds would take. There needs to be a hospitable environment, a moist warm sunlit area for those seeds to take, then root and grow into a fully mature grass and perpetuate on and on and on. However that area across the road is barren rocky sandy and yuck. You drop those seeds, most of those are going to blow off and away because that area is a no-go, it’s got a strong resistance, a barrier, a non-hospitable environment.
02:18. Now that is how our immune system works. Now the story I feel that should be out there, is what are you doing to nurture your body to do the best it can be, to have the strongest barrier it can be.
02: 30. Enough of this nonsense about the big bad bug and all the worry about washing your hands. ‘Cause I tell you what, if you are neglecting to nurture your body and the 51 trillion cells to be the best they can be, watch out, that may not be enough, washing your hands.
02:47. So let’s talk about that. How do we orchestrate a healthy system that has a strong immune barrier to anything that’s out there? And really guys, this should be a day-to-day forte (?) for everyone who just wants to be their best.
03:00. So let’s go through it. Boosting your barriers. You need to trust your body. First and foremost, the 51 trillion cells are remarkable. Trust in that.
03: 12. You’ve gotta eat well. Eat well with nutrient-dense, mineral-dense foods. Stay well hydrated. Move. You’ve gotta move well. Exercise your body regularly, moving all parts in all directions. Enjoy healthy sunlight exposure. You’ve gotta think well. Follow your passions and purpose. Think positively. Perhaps switch off the TV.
03:41. Keep up with your chiropractic adjustments. An optimal brain and body communication via the nervous system is vital so ensuring your body is in a surviving state. Do all these things guys. Up the ante of them. Go in harder with your (unintelligible) exercises, your hydration etcetera, and trust in your body. It’s amazing. It’s built with this in-built protective mechanism. Foster it. Help to balance that story out there, and help people to take on a more useful interpretation of this current crisis out there.
04:19. I hope this was of value and you guys enjoy.
END TRANSCRIPT
The regulator has been informed. As the world’s death toll rockets past 2 million, we wait to see if they really meant what they said about disciplinary action.