spinal manipulation
As we have discussed ad nauseam on this blog, spinal manipulation therapy (SMT) can cause serious adverse events, including spinal epidural hematoma (SEH), an emergency that can cause severe neurological dysfunction. Chinese surgeons have reported three cases of SEH after SMT.
- The first case was a 30-year-old woman who experienced neck pain and numbness in both upper limbs immediately after SMT. Her symptoms persisted after 3 d of conservative treatment, and she was admitted to our hospital. Magnetic resonance imaging (MRI) demonstrated an SEH, extending from C6 to C7.
- The second case was a 55-year-old man with sudden back pain 1 d after SMT, numbness in both lower limbs, an inability to stand or walk, and difficulty urinating. MRI revealed an SEH, extending from T1 to T3.
- The third case was a 28-year-old man who suddenly developed symptoms of numbness in both lower limbs 4 h after SMT. He was unable to stand or walk and experienced mild back pain. MRI revealed an SEH, extending from T1 to T2.
All three patients underwent surgery after failed conservative treatment. Blood clots were found during the operation in case 1 and case 2, and the postoperative pathology confirmed a hematoma. In case three, a vein ruptured during the operation, causing massive bleeding. The three patients recovered to ASIA grade E on day 5, 1 wk, and day 10 after surgery, respectively. All patients returned to normal after 3 mo of follow-up.
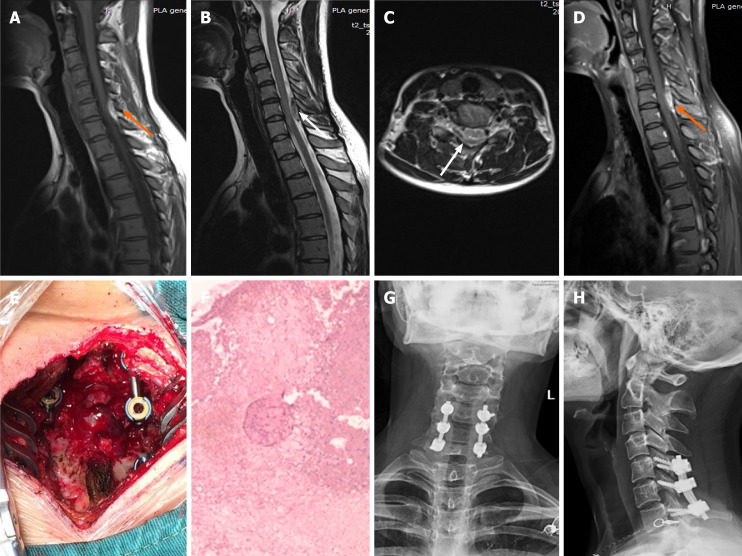
Imaging examinations of case 1. A: T1-weighted preoperative magnetic resonance imaging (MRI) image shows high signal intensity (orange arrow); B and C: Preoperative T2-weighted image shows low signal intensity, and an axial T2-weighted image demonstrates that the hematoma occurred in the posterior region (white arrow); D: Preoperative enhanced MRI suggests an enhanced hematoma signal (orange arrow); E: Intraoperative photograph shows that spinal cord compression has recovered; F: Postoperative pathology suggested a hematoma; G and H: X-ray at the 3-mo follow-up indicated intact internal fixation.
The authors concluded that before proceeding with SMT, each patient should be evaluated in detail and checked for risk factors. In cases where the physical condition changes rapidly, physicians should be alert to the danger and send the patient to the emergency department for a complete MRI examination. We recommend surgery if neurological symptoms appear.
In their paper, the authors also review 15 further cases of SEH that have been previously published. They stress several times in their article that this complication is rare. In my view, this begs the question: how do they know? As there is no post-marketing surveillance of chiropractors or other clinicians doing SMT, I would insist that nobody can be sure about the true incidence of SEH or any other complication after SMT.
The ‘International Chiropractors Association’ (ICA) has just issued a statement entitled “International Chiropractors Association Affirms Policy on Health Freedom“. On the background of the fact that US President Biden, issued a series of Executive Orders related to mandating federal employees and federal contractors to receive the COVID-19 vaccine, the ICA try to explain their position regarding vaccinations. Here are a few passages from this statement:
…In a world of public health that promotes evidence-based decision making, we see the importance of natural immunity being ignored and replaced with a totalitarian approach of compulsory vaccination. At a time when the Surgeon General says misinformation has become an urgent threat to public health, misinformation is now being used in an attempt to discredit the chiropractic profession, the International Chiropractors Association, and all chiropractic patients who desire to focus on improving health naturally. After enduring 18 months of shutdowns, lockdowns, flattening the curve, masking, limitations of speech on social media; and a cancel culture environment that threatens the basic freedoms our country was founded upon in 1776, ICA will not compromise on the importance of protecting health freedom…
The ICA Policy on Immunization and Vaccination has remained unchanged for almost 50 years and clearly states:
“The International Chiropractors Association recognizes that the use of vaccines is not without risk and questions the wisdom of mass vaccination programs. Chiropractic principles favor the enhancement of natural immunity over artificial immunization.
The ICA supports each individual’s right to select his or her own health care and to be made aware of the possible adverse effects of vaccines upon a human body. In accordance with such principles and based upon the individual’s right to freedom of choice, the ICA is opposed to compulsory programs which infringe upon such rights.
The International Chiropractors Association is supportive of a conscience clause or waiver in compulsory vaccination laws, providing an elective course of action for all regarding immunization, thereby allowing patients freedom of choice in matters affecting their bodies and health.”
The International Chiropractors Association maintains that all healthcare interventions, including the chiropractic adjustment, are associated with some level of risk and that every individual is entitled to be informed of those risks, no matter how insignificant. All individuals must retain the freedom to accept or reject any healthcare product, procedure, or medication including vaccinations. The International Chiropractors Association therefore strongly opposes the use of medical mandates that violate personal sovereignty, violate the principles of informed consent, and constrain the rights of patients to make their own health care choices…
The ICA encourages the recognition that natural efforts to enhance the innate immune system ability to adapt to novel viruses are grounded in science and rejects the notion that the patients’ freedom to rely on naturally acquired immunity is not based upon unscientific beliefs.
The ICA rejects the premise that the chiropractic profession’s long history of promoting health freedom and supporting conscientious exemptions is based upon unscientific or non-mainstream beliefs…
I find this statement clear as mud and have the following questions:
- Do the ICA recommend vaccinations?
- In particular, do they encourage their members to get vaccinated with the COVID-19 vaccines?
- Do they advise to recommend COVID-19 vaccinations to their patients?
- Or do they think that natural immunity is preferable and advise their members and patients accordingly?
- Do they believe that spinal manipulation enhances natural immunity?
- Do they think that spinal manipulations are an effective alternative to COVID-19 vaccinations?
- Do they believe that scientific evidence trumps dogma or vice versa?
- Which of the two should, according to their conviction, must influence the decision-making processes in healthcare?
- If the ICA object to misinformation about COVID, why do they not stop their members from promoting it?
- What makes them think that information about the possible adverse effects of vaccines upon a human body is unavailable?
- If the ICA recognizes the risks of spinal manipulation, why do they not inform the public about them regularly and objectively?
- If the ICA knows about the importance of informed consent, why do not all of their members adhere to it?
- And finally, why do the ICA insist on the term ‘international’ in the name of their organization, if they purely deal with the US situation?
I do not expect the ICA to give me the answers to these questions. But perhaps their Wiki page goes some way towards answering some of them: “… The ICA supports the efforts of the National Vaccine Information Center (NVIC).[13] The NVIC is known for promoting false and misleading information about vaccines, in particular the discredited claim that vaccines cause autism.
The ICA’s annual conferences have featured anti-vaccination propaganda. In 2018 Guest Speaker Beau Pierce (Pierce co-produced a series entitled Vaccines Revealed) hosted a session entitled Vaccines Revealed.,[14] and Jeff Hays, known for producing the anti-Vaccine propaganda Vaccines Revealed, was invited to host a session the 2017 ICA Council on Chiropractic Pediatrics Annual Conference. In 2016 the widely discredited anti-vaccination propaganda film VAXXED was shown at a conference sponsored by the ICA’s Council on Chiropractic Pediatrics …”
SAY NO MORE!
This article from AP News caught my attention. Here it is (I haven’t changed a word):
The flashy postcard, covered with images of syringes, beckoned people to attend Vax-Con ’21 to learn “the uncensored truth” about COVID-19 vaccines.
Participants traveled from around the country to a Wisconsin Dells resort for a sold-out convention that was, in fact, a sea of misinformation and conspiracy theories about vaccines and the pandemic. The featured speaker was the anti-vaccine activist who appeared in the 2020 movie “Plandemic,” which pushed false COVID-19 stories into the mainstream. One session after another discussed bogus claims about the health dangers of mask wearing and vaccines.
The convention was organized by members of a profession that has become a major purveyor of vaccine misinformation during the pandemic: chiropractors.
At a time when the surgeon general says misinformation has become an urgent threat to public health, an investigation by The Associated Press found a vocal and influential group of chiropractors has been capitalizing on the pandemic by sowing fear and mistrust of vaccines.
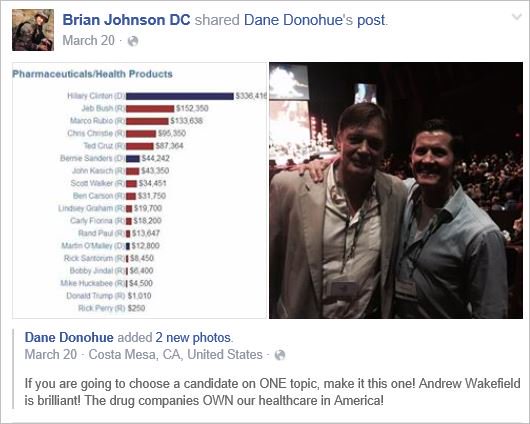
They have touted their supplements as alternatives to vaccines, written doctor’s notes to allow patients to get out of mask and immunization mandates, donated large sums of money to anti-vaccine organizations and sold anti-vaccine ads on Facebook and Instagram, the AP discovered. One chiropractor gave thousands of dollars to a Super PAC that hosted an anti-vaccine, pro-Donald Trump rally near the U.S. Capitol on Jan. 6.
They have also been the leading force behind anti-vaccine events like the one in Wisconsin, where hundreds of chiropractors from across the U.S. shelled out $299 or more to attend. The AP found chiropractors were allowed to earn continuing education credits to maintain their licenses in at least 10 states.
On this blog, I have often discussed that chiropractors tend to be anti-vax. It all goes back to their founding father, DD Palmer, who famously wrote:
- Vaccination and inoculation are pathological; chiropractic is physiological,
- and who in 1894, published his views on smallpox vaccination: ‘…the monstrous delusion … fastened on us by the medical profession, enforced by the state boards, and supported by the mass of unthinking people …’
- and who stated in 1896 that keeping tissue healthy is therefore the best prevention against infections; and this is best achieved by magnetic healing.
But that’s long ago! We are not like that anymore! … say the chiros of today.
Do you believe them?
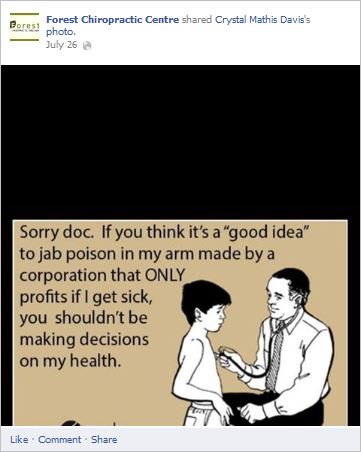
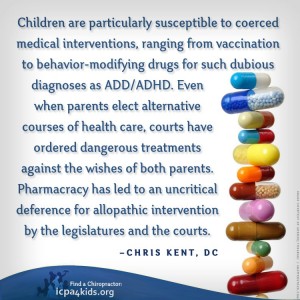
If so, you might want to read this article by Jann Bellamy. Or alternatively, just look at some of my finds from the Internet:

The purpose of this survey was to quantify and describe the clinical practice beliefs and behaviors associated with US chiropractors. A 10% random sample of US chiropractors (n = 8975) was selected from all 50 state regulatory board lists and invited to participate in a survey. The survey consisted of a 7-item questionnaire; 6 items were associated with chiropractic ideological and practice characteristics and 1 item was related to the self-identified role of chiropractic in the healthcare system which was utilized as the dependent variable to identify chiropractic subgroups. Multinomial logistic regression with predictive margins was used to analyze which responses to the 6 ideology and practice characteristic items were predictive of chiropractic subgroups.
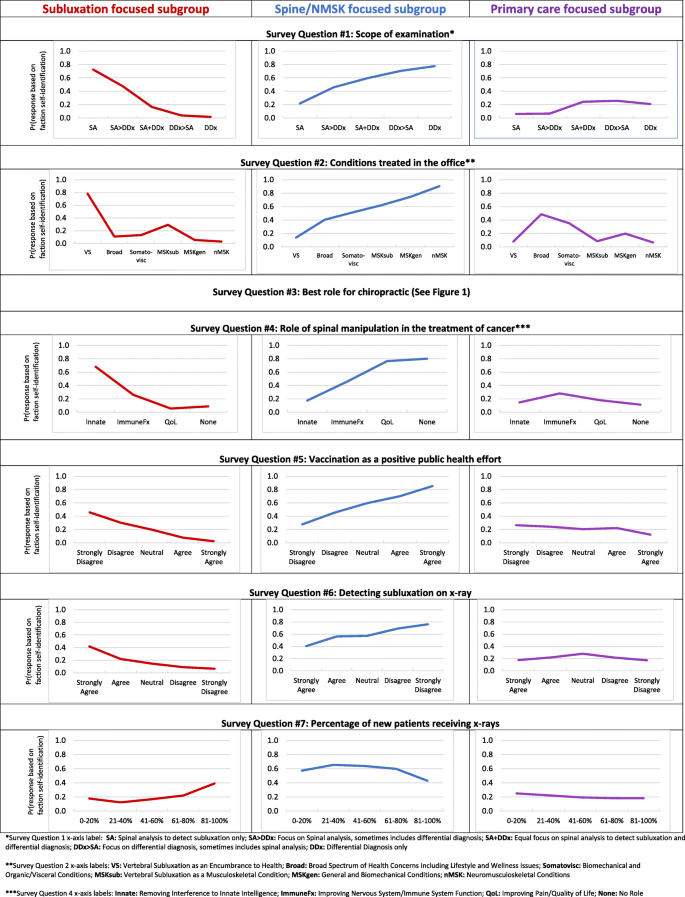
The survey instrument used in this study was developed by the authors and modeled after similar chiropractic identity analyses. The survey instrument included a total of 7 items intended to elicit divergent ideologies and practice behaviors. The figure below is a copy of the survey instrument.

A total of 3538 responses were collected (39.4% response rate). Respondents self-identified into three distinct subgroups based on the perceived role of the chiropractic profession in the greater healthcare system:
- 57% were spine/neuromusculoskeletal focused;
- 22% were primary care focused;
- 21% were vertebral subluxation focused.
Patterns of responses to the 6 ideologies and practice characteristic items were substantially different across the three professional subgroups.
The authors concluded that respondents self-identified into one of three distinct intra-professional subgroups. These subgroups can be differentiated along themes related to clinical practice beliefs and behaviors.
Here are the results in more detail as sated by the authors:
Regarding scope of examination (survey question 1), respondents reporting the scope of their clinical examination to only include spinal analysis for the assessment of vertebral subluxation had a 70% probability of belonging to the subluxation focused subgroup, a 20% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup. Conversely, respondents who reported the scope of their clinical examination only includes a differential diagnosis had a 0% probability of belonging to the vertebral subluxation focused subgroup, an 80% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup.
Concerning conditions treated (survey question 2), respondents who reported predominantly treating vertebral subluxation as an encumbrance to health had an 80% probability of belonging to the vertebral subluxation focused subgroup, a 10% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup. In contrast, respondents reporting predominantly treating neuromusculoskeletal conditions had a 0% probability of belonging to the vertebral subluxation focused subgroup, a 90% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup.
Regarding the role of spinal manipulation for those with cancer (survey question 4), respondents reporting the role of spinal manipulation for those with cancer is to remove interference to innate intelligence had a 70% probability of belonging to the vertebral subluxation focused subgroup, a 20% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup. Respondents reporting there is no role of spinal manipulation in those with cancer also had a 10% probability of belonging to the subluxation focused subgroup, an 80% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup.
Regarding vaccination (survey question 5), respondents who strongly disagreed that vaccinations have had a positive effect on global public health had a 50% probability of belonging to the vertebral subluxation focused subgroup, an approximately 25% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and an approximately 25% probability of belonging to the primary care focused subgroup. In contrast, respondents who strongly agreed that vaccinations have had a positive effect on global public health had a 0% probability of belonging to the vertebral subluxation focused subgroup, a 90% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 10% probability of belonging to the primary care focused subgroup.
Concerning the detection of vertebral subluxation on x-ray (survey question 6), respondents who strongly agreed that x-ray is helpful in detecting vertebral subluxations had a 40% probability of belonging to the vertebral subluxation focused subgroup, a 40% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup. Respondents who strongly disagreed that x-ray is helpful in detecting vertebral subluxations had a near 0% probability of belonging to the vertebral subluxation focused subgroup, an 80% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and slightly below a 20% probability of belonging to the primary care focused subgroup.
Regarding use of x-rays for new patients (survey question 7), respondents who reported prescribing x-rays for 0–20% of new patients had a 20% probability of belonging to the vertebral subluxation focused subgroup, a 60% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup. Respondents reporting prescribing x-rays for 81–100% of new patients had a 40% probability of belonging to the vertebral subluxation focused subgroup, a 40% probability of belonging to the spine and neuromusculoskeletal focused subgroup, and a 20% probability of belonging to the primary care focused subgroup.
END OF QUOTE
While I am not sure that the division into the 3 subgroups is valid and suspect that there must be a substantial overlap between them, I must admit that the paper is rich in fascinating information. Generally speaking, I find all subgroups somewhat mysterious and would ask them the following questions:
Subgroup 1: why did you not study medicine or physiotherapy?
Subgroup 2: does it not bother you that your education and training are woefully insufficient for primary care?
Subgroup 3: is it not time to abandon the obsolete nonsense of your guru, the old charlatan DD Palmer?
Static or motion manual palpation tests of the spine are commonly used by chiropractors and osteopaths to assess pain location and reproduction in low back pain (LBP) patients. But how reliable are they?
The purpose of this review was to evaluate the reliability and validity of manual palpation used for the assessment of LBP in adults. The authors systematically searched five databases from 2000 to 2019 and critically appraised the internal validity of studies using QAREL and QUADAS-2 instruments.
A total of 2023 eligible articles were identified, of which 14 were at low risk of bias. Evidence suggests that reliability of soft tissue structures palpation is inconsistent, and reliability of bony structures and joint mobility palpation is poor. Preliminary evidence was found to suggest that gluteal muscle palpation for tenderness may be valid in differentiating LBP patients with and without radiculopathy.
The authors concluded that the reliability of manual palpation tests in the assessment of LBP patients varies greatly. This is problematic because these tests are commonly used by manual therapists and clinicians. Little is known about the validity of these tests; therefore, their clinical utility is uncertain. High quality validity studies are needed to inform the clinical use of manual palpation tests.
I have repeatedly drawn attention to the fact that the diagnostic methods used by chiropractors and osteopaths are of uncertain or disproven validity (see for instance here, or here). Why is that important?
Imagine you consult a chiropractor or osteopath. Simply put, this is what is likely to happen:
- They listen to your complaint.
- They do a few tests which are of dubious validity.
- They give you a diagnosis that is meaningless.
- They treat you with manual therapies that are neither effective nor safe.
- You pay.
- They persuade you that you need many more sessions.
- You pay regularly.
- When eventually your pain has gone away, they persuade you to have useless maintenance treatment.
- You pay regularly.
In a nutshell, they have very little to offer … which explains why they attack everyone who dares to disclose this.
Prior research has generated inconsistent results regarding vaccination rates among patients using so-called alternative medicine (SCAM). Given that SCAM includes a wide range of therapies – about 400 different treatments have been counted – variable vaccination patterns may occur within consultations with different types of SCAM practitioners.
A recent analysis aimed to evaluate differences between categories of SCAM regarding vaccination behavior among US adults.
Data from the 2017 National Health Interview Survey (NHIS; n = 26,742; response rate 80.7%) were used. Prevalences of flu vaccination, consultations with SCAM practitioners in the past 12 months, and their potential interactions were examined. 42.7% of participants had received the flu vaccination in the past 12 months, 32.4% had seen one or more SCAM practitioners. Users of any type of SCAM were as likely as non-users to have received a flu vaccination (44.8% users versus 41.7% non-users; p = 0,862; adjusted odds ratio [AOR] = 1.01, 95% confidence interval [CI] = 0.95–1.07).
Regarding specific SCAM types,
- individuals consulting with naturopaths (p < 0.001; AOR = 0.67, 95 %CI = 0.54–0.82),
- homeopaths (p < 0.001; AOR = 0.55; 95 %CI = 0.44–0.69)
- chiropractors (p = 0.016; AOR = 0.9, 95 %CI = 0.83–0.98)
were less likely to be vaccinated. Other SCAMs showed no significant association with flu vaccination behavior. Independent predictors for a flu shot were prior diabetes, cancer, current asthma, kidney disease, overweight and current pregnancy. As well, higher educational level, age, ethnicity, health insurance coverage, and having seen a general physician or medical specialist in the past 12 months were also associated with a higher vaccination rate.
The authors concluded that SCAM users were equally likely to receive an influenza vaccination compared with non-users. Different SCAM therapies showed varied associations with vaccination behavior. Further analyses may be needed to distinguish influencing factors among patients’ vaccination behavior.
This survey confirms what we have discussed repeatedly on this blog (see, for instance here, here, here, here, and here). The reason why consumers who consult naturopaths, homeopaths, or chiropractors get vaccinated less regularly is presumably that these practitioners tend to advise against vaccinations. And why do they do that?
- Naturopaths claim that vaccines are toxic and their therapeutic options protect against infections.
- Homeopaths claim that vaccines are toxic and their therapeutic options protect against infections.
- Chiropractors claim that vaccines are toxic and their therapeutic options protect against infections.
Do these ‘therapeutic options’ – detox, nosodes, spinal manipulation – have anything in common?
Yes, they are bogus!
Conclusion:
Many naturopaths, homeopaths, and chiropractors seem to be a risk to public health.
The General Chiropractic Council (GCC) regulates chiropractors in the UK, Isle of Man, and Gibraltar to ensure the safety of patients undergoing chiropractic treatment. The GCC sets the standards of chiropractic practice and professional conduct that all chiropractors must meet.

By providing a lengthy ruling in the case of the late John Lawler and his chiropractor, Arlene Scholten, the GCC has recently established new standards for chiropractors working in the UK, Isle of Man, and Gibraltar (see also today’s article in The Daily Mail). If I interpret the GCC’s ruling correctly, a UK chiropractor is henceforth allowed to do all of the following things without fearing to get reprimanded, as long as he or she produces evidence that the deeds were done not with malicious intentions but in a state of confusion and panic:
- Treat a patient with treatments that are contraindicated.
- Fail to obtain informed consent.
- Pose as a real doctor without informing the patient that the practitioner is just a chiropractor who has never been near a medical school.
- Cause the death of a patient by treatment to the neck.
- Administer first aid in a way that makes matters worse.
- Tell lies to the ambulance men who consequently failed to employ a method of transport that would save the patient’s life.
- Keep inaccurate patient records that conceal what treatments were administered.
In previous years, the job of a chiropractor had turned out to be demanding, difficult, and stressful. This was due not least to the GCC’s professional standards which UK chiropractors were obliged to observe. The code of the GCC stated prominently that “our overall purpose is to protect the public.”
All this is now a thing of the past.
The new ruling changed everything. Now, UK chiropractors can relax and can happily pursue their true devotion, namely to keep their bank manager happy, while not worrying too much about the welfare and health of their patients.
In the name of all UK chiropractors, I herewith express my thanks to the GCC for unashamedly protecting first and foremost the interests of their members, while tacitly discarding medical ethics and evidently not protecting the public.
MAKE CHIROPRACTIC GREAT AGAIN!
In their 2019 systematic review of spinal manipulative therapy (SMT) for chronic back pain, Rubinstein et al included 7 studies comparing the effect of SMT with sham SMT.
They defined SMT as any hands-on treatment of the spine, including both mobilization and manipulation. Mobilizations use low-grade velocity, small or large amplitude passive movement techniques within the patient’s range of motion and control. Manipulation uses a high-velocity impulse or thrust applied to a synovial joint over a short amplitude near or at the end of the passive or physiological range of motion. Even though there is overlap, it seems fair to say that mobilization is the domain of osteopaths, while manipulation is that of chiropractors.
The researchers found:
- low-quality evidence suggesting that SMT does not result in a statistically better effect than sham SMT at one month,
- very low-quality evidence suggesting that SMT does not result in a statistically better effect than sham SMT at six and 12 months.
- low-quality evidence suggesting that, in terms of function, SMT results in a moderate to strong statistically significant and clinically better effect than sham SMT at one month. Exclusion of an extreme outlier accounted for a large percentage of the statistical heterogeneity for this outcome at this time interval (SMD −0.27, 95% confidence interval −0.52 to −0.02; participants=698; studies=7; I2=39%), resulting in a small, clinically better effect in favor of SMT.
- very low-quality evidence suggesting that, in terms of function, SMT does not result in a statistically significant better effect than sham SMT at six and 12 months.
This means that SMT has effects that are very similar to placebo (the uncertain effects on function could be interpreted as the result of residual de-blinding due to a lack of an optimal placebo or sham intervention). In turn, this means that the effects patients experience are largely or completely due to a placebo response and that SMT has no or only a negligibly small specific effect on back pain. Considering the facts that SMT is by no means risk-free and that less risky treatments exist, the inescapable conclusion is that SMT cannot be recommended as a treatment of chronic back pain.
This systematic review assessed the effect of spinal manipulative therapy (SMT), the hallmark therapy of chiropractors, on pain and function for chronic low back pain (LBP) using individual participant data (IPD) meta-analyses.
Of the 42 RCTs fulfilling the inclusion criteria, the authors obtained IPD from 21 (n=4223). Most trials (s=12, n=2249) compared SMT to recommended interventions. The analyses showed moderate-quality evidence that SMT vs recommended interventions resulted in similar outcomes on
- pain (MD -3.0, 95%CI: -6.9 to 0.9, 10 trials, 1922 participants)
- and functional status at one month (SMD: -0.2, 95% CI -0.4 to 0.0, 10 trials, 1939 participants).
Effects at other follow-up measurements were similar. Results for other comparisons (SMT vs non-recommended interventions; SMT as adjuvant therapy; mobilization vs manipulation) showed similar findings. SMT vs sham SMT analysis was not performed, because data from only one study were available. Sensitivity analyses confirmed these findings.
The authors concluded that sufficient evidence suggest that SMT provides similar outcomes to recommended interventions, for pain relief and improvement of functional status. SMT would appear to be a good option for the treatment of chronic LBP.
In 2019, this team of authors published a conventional meta-analysis of almost the same data. At this stage, they concluded as follows: SMT produces similar effects to recommended therapies for chronic low back pain, whereas SMT seems to be better than non-recommended interventions for improvement in function in the short term. Clinicians should inform their patients of the potential risks of adverse events associated with SMT.
Why was the warning about risks dropped in the new paper?
I have no idea.
But the risks are crucial here. If we are told that SMT is as good or as bad as recommended therapies, such as exercise, responsible clinicians need to decide which treatment they should recommend to their patients. If effectiveness is equal, other criteria come into play:
- cost,
- risk,
- availability.
Can any reasonable person seriously assume that SMT would do better than exercise when accounting for costs and risks?
I very much doubt it!
The objective of this systematic review was to assess the effects and reliability of sham procedures in manual therapy (MT) trials in the treatment of back pain (BP) in order to provide methodological guidance for clinical trial development. Different databases were screened up to 20 August 2020. Randomised clinical trials involving adults affected by BP (cervical and lumbar), acute or chronic, were included. Hand contact sham treatment (ST) was compared with different MT (physiotherapy, chiropractic, osteopathy, massage, kinesiology, and reflexology) and to no treatment. Primary outcomes were BP improvement, the success of blinding, and adverse effect (AE). Secondary outcomes were the number of drop-outs. Dichotomous outcomes were analysed using risk ratio (RR), continuous using mean difference (MD), 95% CIs. The minimal clinically important difference was 30 mm changes in pain score.
A total of 24 trials were included involving 2019 participants. Different manual treatments were provided:
- SM/chiropractic (7 studies, 567 participants).
- Osteopathy (5 trials, 645 participants).
- Kinesiology (1 trial, 58 participants).
- Articular mobilisations (6 trials, 445 participants).
- Muscular release (5 trials, 304 participants).
Very low evidence quality suggests clinically insignificant pain improvement in favour of MT compared with ST (MD 3.86, 95% CI 3.29 to 4.43) and no differences between ST and no treatment (MD -5.84, 95% CI -20.46 to 8.78).ST reliability shows a high percentage of correct detection by participants (ranged from 46.7% to 83.5%), spinal manipulation being the most recognised technique. Low quality of evidence suggests that AE and drop-out rates were similar between ST and MT (RR AE=0.84, 95% CI 0.55 to 1.28, RR drop-outs=0.98, 95% CI 0.77 to 1.25). A similar drop-out rate was reported for no treatment (RR=0.82, 95% 0.43 to 1.55).

Forest plot of comparison ST versus MT in back pain outcome at short term. MT, manual therapy; ST, sham treatment.
The authors concluded that MT does not seem to have clinically relevant effect compared with ST. Similar effects were found with no treatment. The heterogeneousness of sham MT studies and the very low quality of evidence render uncertain these review findings. Future trials should develop reliable kinds of ST, similar to active treatment, to ensure participant blinding and to guarantee a proper sample size for the reliable detection of clinically meaningful treatment effects.
Essentially these findings suggest that the effects patients experience after MT are not due to MT per see but to placebo effects. The review could be criticised because of the somewhat odd mix of MTs lumped together in one analysis. Yet, I think it is fair to point out that most of the studies were of chiropractic and osteopathy. Thus, this review implies that chiropractic and osteopathy are essentially placebo treatments.
The authors of the review also provide this further comment:
Similar findings were found in other reviews conducted on LBP. Ruddock et al included studies where SM was compared with what authors called ‘an effective ST’, namely a credible sham manipulation that physically mimics the SM. Pooled data from four trials showed a very small and not clinically meaningful effect in favour of MT.52
Rubinstein et al 53 compared SM and mobilisation techniques to recommended, non-recommended therapies and to ST. Their findings showed that 5/47 studies included attempted to blind patients to the assigned intervention by providing an ST. Of these five trials, two were judged at unclear risk of participants blinding. The authors also questioned the need for additional studies on this argument, as during the update of their review they found recent small pragmatic studies with high risk of bias. We agree with Rubinstein et al that recent studies included in this review did not show a higher quality of evidence. The development of RCT with similar characteristic will probably not add any proof of evidence on MT and ST effectiveness.53
If we agree that chiropractic and osteopathy are placebo therapies, we might ask whether they should have a place in the management of BP. Considering the considerable risks associated with them, I feel that the answer is obvious and simple: