spinal manipulation
Multiple sclerosis (MS) causes a range of different symptoms. Patients with MS have looked for alternative therapies to control their MS progress and treat their symptoms. Non-invasive therapeutic approaches such as massage can have benefits to mitigate some of these symptoms. However, there is no rigorous review of massage effectiveness for patients suffering from MS.
The present systematic review was aimed at examining the effectiveness of different massage approaches on common MS symptoms, including fatigue, pain, anxiety, depression, and spasticity.
A total of 12 studies met the inclusion criteria. The authors rated 5 studies as being of fair and 7 studies of good methodological quality. Fatigue was improved by different massage styles, such as reflexology, nonspecific therapeutic massage, and Swedish massage. Pain, anxiety, and depression were effectively improved by reflexology techniques. Spasticity was reduced by Swedish massage and reflexology techniques.
The authors concluded that different massage approaches effectively improved MS symptoms such as fatigue, pain, anxiety, depression, and spasticity.
Clinical trials of massage therapy face formidable obstacles including:
- difficulties in obtaining funding,
- difficulties in finding expert researchers who are interested in the subject,
- difficulties to control for placebo effects,
- difficulties in blinding patients,
- impossibility of blinding therapists,
- confusion about the plethora of different massage techniques.
Thus, the evidence is often less convincing than one would hope. This, however, does not mean that massage therapy does not have considerable potential for a range of indications. One could easily argue that this situation is similar to spinal manipulation. Yet, there are at least three important differences:
- massage therapy is not as heavily burdened with frequent adverse effects and potentially life-threatening complications,
- massage therapy has a rational basis,
- the existing evidence is more uniformly encouraging.
Consequently, massage therapy (particularly, classic or Swedish massage) is more readily being accepted even in the absence of solid evidence. In fact, in some countries, e.g. Germany and Austria, massage therapy is considered to be a conventional treatment.
A case report was published of a 35-year-old Chinese man with no risk factors for stroke. He presented with a 2-day history of expressive dysphasia and a 1-day history of right-sided weakness. The symptoms were preceded by multiple sessions of the neck, shoulder girdle, and upper back massage for pain relief in the prior 2 weeks. A CT-scan of the brain demonstrated an acute left middle cerebral artery infarct and left internal carotid artery dissection. The MRI cerebral angiogram confirmed left carotid arterial dissection and intimal oedema of bilateral vertebral arteries. In the absence of other vascular comorbidities and risk factors, massage-induced internal carotid arterial dissection was deemed to be the most likely cause of the near-fatal cerebrovascular event.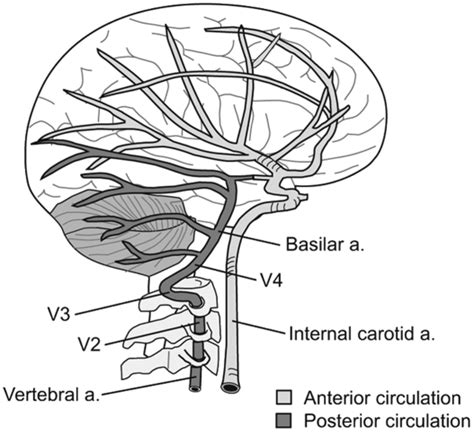
INSIDER reported further details of the case: the patient told the doctors who treated him that he had seen the chiropractor for two weeks before he experienced trouble reading, writing and talking. After experiencing those symptoms for two days and one day of pain on his right side, a friend convinced the patient to consult a neurologist. This led to the hospital admission, the above-named tests, and diagnosis. After three months of therapy and rehab, the patient showed “significant improvement,” according to the doctors.
What remains unclear is the exact nature of the neck treatment that is believed to have caused the arterial dissection. A massage is mentioned but massages have rarely been associated with such problems. Neck manipulations, on the other hand, are the hallmark therapy of chiropractors and have, as I have pointed out regularly, often been reported to cause arterial dissections.
Chiropractors usually deny this fact; alternatively, they claim that only poorly trained practitioners cause these adverse events or that their frequency is exceedingly small. However, without a proper post-marketing surveillance system, this argument is hardly convincing.
Subluxation is … a displacement of two or more bones whose articular surfaces have lost, wholly or in part, their natural connection. (D. D. Palmer, 1910)
The definition of ‘subluxation’ as used by chiropractors differs from that in conventional medicine where it describes a partial dislocation of the bony surfaces of a joint readily visible via an X-ray. Crucially, a subluxation, as understood in conventional medicine, is not the cause of disease. Spinal subluxations, according to medical terminology, are possible only if anatomical structures are seriously disrupted.
Subluxation, as chiropractors understand the term, has been central to chiropractic from its very beginning. Despite its central role in chiropractic, its definition is far from clear and has changed significantly over time.
DD Palmer (the guy who invented chiropractic) was extremely vague about most of his ideas. Yet, he remained steadfast about his claims that 95% of all diseases were due to subluxations of the spine, that subluxations hindered the flow of the ‘innate intelligence’ which controlled the vital functions of the body. Innate intelligence or ‘inate’, he believed, operated through the nerves, and subluxated vertebra caused pinched nerves, which in turn blocked the flow of the innate and thus led to abnormal function of our organs. For Palmer and his followers, subluxation is the sole or at least the main cause of all diseases (or dis-eases, as Palmer preferred).
Almost exactly 4 years ago, I published this post:
Is chiropractic subluxation a notion of the past? SADLY NOT!
In it, I provided evidence that – contrary to what we are often told – chiropractors remain fond of the subluxation nonsense they leant in school. This can be shown by the frequency by which chiropractors advertise on Twitter the concept of chiropractic subluxation.
Today, I had another look. The question I asked myself was: has the promotion of the obsolete subluxation concept by chiropractors subsided?
The findings did not surprise me.
Even a quick glance reveals that there is still a plethora of advertising going on that uses the subluxation myth. Many chiros use imaginative artwork to get their misleading message across. Below is a small selection.








Yes, I know, this little display is not very scientific. In fact, it is a mere impression and does not intend to be anything else. So, let’s look at some more scientific data on this subject. Here are the last 2 paragraphs from the chapter on subluxation in my recent book on chiropractic:
A 2018 survey determined how many chiropractic institutions worldwide still use the term in their curricula.[1] Forty-six chiropractic programmes (18 from US and 28 non-US) participated. The term subluxation was found in all but two US course catalogues. Remarkably, between 2011 and 2017, the use of subluxation in US courses even increased. Similarly, a survey of 7455 US students of chiropractic showed that 61% of them agreed or strongly agreed that the emphasis of chiropractic intervention is to eliminate vertebral subluxations/vertebral subluxation complexes.[2]
Even though chiropractic subluxation is at the heart of chiropractic, its definition remains nebulous and its very existence seems doubtful. But doubt is not what chiropractors want. Without subluxation, spinal manipulation seems questionable – and this will be the theme of the next chapter.
[1] https://chiromt.biomedcentral.com/articles/10.1186/s12998-018-0191-1
[2] https://www.ncbi.nlm.nih.gov/pubmed/25646145
In a nutshell: chiros cannot give up the concept of subluxation because, if they did, they would be physios except with a much narrower focus.
I recently came across this paper by Prof. Dr. Chad E. Cook, a physical therapist, PhD, a Fellow of the American Physical Therapy Association (FAPTA), and a professor as well as director of clinical research in the Department of Orthopaedics, Department of Population Health Sciences at the Duke Clinical Research Institute at Duke University in North Carolina, USA. The paper is entitled ‘The Demonization of Manual Therapy‘.
Cook introduced the subject by stating: “In medicine, when we do not understand or when we dislike something, we demonize it. Well-known examples throughout history include the initial ridicule of antiseptic handwashing, percutaneous transluminal coronary angioplasty (i. e., balloon angioplasty), the relationships between viruses and cancer, the contribution of bacteria in the development of ulcers, and the role of heredity in the development of disease. In each example, naysayers attempted to discredit the use of each of the concepts, despite having no evidence to support their claims. The goal in each of the aforementioned topics: demonize the concept.”
Cook then discussed 8 ‘demonizations’ of manual therapy. Number 7 is entitled “Causes as Much Harm as Help“. Here is this section in full:
By definition, harms include adverse reactions (e. g., side effects of treatments), and other undesirable consequences of health care products and services. Harms can be classified as “none”, minor, moderate, serious and severe [67]. Most interventions have some harms, typically minor, which are defined as a non-life-threatening, temporary harm that may or may not require efforts to assess for a change in a patient’s condition such as monitoring [67].
There are harms associated with a manual therapy intervention, but they are generally benign (minor). Up to 20 –40 % of individuals will report adverse events after the application of manual therapy. The most common adverse events were soreness in muscles, increased pain, stiffness and tiredness [68]. There are rare occasions of several harms associated with manual therapy and these include spinal or neurological problems as well as cervical arterial strokes [9]. It is critical to emphasize how rare these events are; serious adverse event incidence estimates ranged from 1 per 2 million manipulations to 13 per 10,000 patients [69].
Cook then concludes that “manual therapy has been inappropriately demonized over the last decade and has been associated with inaccurate assumptions and false speculations that many clinicians have acquired over the last decade. This paper critically analyzed eight of the most common assumptions that have belabored manual therapy and identified notable errors in seven of the eight. It is my hope that the physiotherapy community will carefully re-evaluate its stance on manual therapy and consider a more evidence-based approach for the betterment of our patients.
REFERENCES
[9] Ernst E. Adverse effects of spinal manipulation: a systematic review. J R Soc Med 2007; 100: 330–338.doi:10.1177/014107680710000716 [68] Paanalahti K, Holm LW, Nordin M et al. Adverse events after manual therapy among patients seeking care for neck and/or back pain: a randomized controlled trial. BMC Musculoskelet Disord 2014; 15: 77. doi:10.1186/1471-2474-15-77 [69] Swait G, Finch R. What are the risks of manual treatment of the spine? A scoping review for clinicians. Chiropr Man Therap 2017; 25: 37. doi:10.1186/s12998-017-0168-5
_________________________________
Here are a few things that I find odd or wrong with Cook’s text:
- The term ‘demonizing’ seems to be a poor choice. The historical examples chosen by Cook were not cases of demonization. They were mostly instances where new discoveries did not fit into the thinking of the time and therefore took a long time to get accepted. They also show that sooner or later, sound evidence always prevails. Lastly, they suggest that speeding up this process via the concept of evidence-based medicine is a good idea.
- Cook then introduces the principle of risk/benefit balance by entitling the cited section “Causes as Much Harm as Help“. Oddly, however, he only discusses the risks of manual therapies and omits the benefit side of the equation.
- This omission is all the more puzzling since he quotes my paper (his reference [9]) states that “the effectiveness of spinal manipulation for most indications is less than convincing.5 A risk-benefit evaluation is therefore unlikely to generate positive results: with uncertain effectiveness and finite risks, the balance cannot be positive.”
- In discussing the risks, he seems to assume that all manual therapies are similar. This is clearly not true. Massage therapies have a very low risk, while this cannot be said of spinal manipulations.
- The harms mentioned by Cook seem to be those of spinal manipulation and not those of all types of manual therapy.
- Cook states that “up to 20 –40 % of individuals will report adverse events after the application of manual therapy.” Yet, the reference he uses in support of this statement is a clinical trial that reported an adverse effect rate of 51%.
- Cook then states that “there are rare occasions of several harms associated with manual therapy and these include spinal or neurological problems as well as cervical arterial strokes.” In support, he quotes one of my papers. In it, I emphasize that “the incidence of such events is unknown.” Cook not only ignores this fact but states in the following sentence that “it is critical to emphasize how rare these events are…”
Cook concludes that “manual therapy has been inappropriately demonized over the last decade and has been associated with inaccurate assumptions and false speculations …” He confuses, I think, demonization with critical assessment.
Cook’s defence of manual therapy is clumsy, inaccurate, ill-conceived, misleading and often borders on the ridiculous. In the age of evidence-based medicine, therapies are not ‘demonized’ but evaluated on the basis of their effectiveness and safety. Manual therapies are too diverse to do this wholesale. They range from various massage techniques, some of which have a positive risk/benefit balance, to high-velocity, low-amplitude thrusts, for which the risks do not demonstrably outweigh the benefits.
Spinal manipulation therapy (SMT) is widely used worldwide to treat musculoskeletal and many other conditions. The evidence that it works for any of them is weak, non-existent, or negative. What is worse, SMT can – as we have discussed so often on this blog – cause adverse events some of which are serious, even fatal.
Spinal epidural hematoma (SEH) caused by SMT is a rare emergency that can cause neurological dysfunction. Chinese researchers recently reported three cases of SEH after SMT. 
- The first case was a 30-year-old woman who experienced neck pain and numbness in both upper limbs immediately after SMT. Her symptoms persisted after 3 d of conservative treatment, and she was admitted to our hospital. Magnetic resonance imaging (MRI) demonstrated an SEH, extending from C6 to C7.
- The second case was a 55-year-old man with sudden back pain 1 d after SMT, numbness in both lower limbs, an inability to stand or walk, and difficulty urinating. MRI revealed an SEH, extending from T1 to T3.
- The third case was a 28-year-old man who suddenly developed symptoms of numbness in both lower limbs 4 h after SMT. He was unable to stand or walk and experienced mild back pain. MRI revealed an SEH, extending from T1 to T2.
All three patients underwent surgery after failed conservative treatment and all recovered to ASIA grade E on day 5, 1 wk, and day 10 after surgery, respectively. All patients returned to normal after 3 mo of follow-up.
The authors concluded that SEH caused by SMT is very rare, and the condition of each patient should be evaluated in full detail before operation. SEH should be diagnosed immediately and actively treated by surgery.
These cases might serve as an apt reminder of the fact that SMT (particularly SMT of the neck) is not without its dangers. The authors’ assurance that SEH is VERY RARE is a little puzzling, in my view (the paper includes a table with all 17 previously published cases). There is, as we often have mentioned, no post-marketing surveillance, surgeons only see those patients who survive such complications long enough to come to the hospital, and they publish such cases only if they feel like it. Consequently, the true incidence is anyone’s guess.
As pointed out earlier, the evidence that SMT might be effective is shaky for most indications. In view of the potential for harm, this can mean only one thing:
The risk/benefit balance for SMT is not demonstrably positive.
In turn, this leads to the conclusion that patients should think twice before having SMT and should inquire about other therapeutic options that have a more positive risk/benefit balance. Similarly, the therapists proposing SMT to a patient have the ethical and moral duty to obtain fully informed consent which includes information about the risk/benefit balance of SMT and other options.
These days, I live in France (some of my time) and I am often baffled by the number of osteopaths and the high level of acceptance of osteopathy in this country. The public seems to believe everything osteopaths claim and even most doctors have long given up to object to the idiocies they proclaim.
The website of the Institute of Osteopathy in Renne is but one of many examples. The Institute informed us as follows (my translation):
In addition to back pain, the osteopath can act on functional disorders of the digestive, neurological, cardiovascular systems or conditions related to ear, nose and throat. Osteopaths can promote recovery in athletes, relieve migraines, musculoskeletal disorders such as tendonitis, or treat sleep disorders. Less known for its preventive aspect, osteopathy also helps maintain good health. It can be effective even when everything is going well because it will prevent the appearance of pain. Osteopathy is, in fact, a manual medicine that allows the rebalancing of the major systems of the body, whatever the age of the patient and his problems. The osteopath looks for the root cause of your complaint in order to develop a curative and preventive treatment.
Who are osteopathic consultations for?
Osteopathic consultations at the Institute of Osteopathy of Rennes-Bretagne are intended for the following types of patients and pathologies
BABY / CHILD
GERD (gastric reflux), plagiocephaly (cranial deformities), recurrent ENT disorders (sinusitis, ear infections…), digestive, sleep and behavioural disorders, motor delay, following a difficult birth…
ADULT
Prevention, comfort treatment of osteoarthritis, musculoskeletal pain, functional abdominal pain, digestive disorders, headaches, dizziness, postural deficiency, facial pains…
PREGNANT WOMAN
Musculoskeletal pain (lumbago, back pain), digestive disorders, preparation for childbirth, post-partum check-up.
COMPANY
Prevention and treatment of MSDs (musculoskeletal disorders) linked to workstation ergonomics, stress, pain due to repetitive movements, poor posture at work, etc.
ADOLESCENT
Scoliosis, prevention of certain pathologies linked to growth, fatigue, stress, follow-up of orthodontic treatment.
SPORTSMAN
Musculoskeletal pain, tendonitis, osteopathic preparation for competition, osteopathic assessment according to the sport practised, repetitive injury.
In case you are not familiar with the evidence for osteopathy, let me tell you that as good as none of the many claims made in the above text is supported by anything that even resembles sound evidence.
So, how can we explain that, in France, osteopathy is allowed to thrive in a virtually evidence-free space?
In France, osteopathy started developing in the 1950s. In 2002, osteopathy received legislative recognition in France, and today, it is booming; between 2016 and 2018, 3589 osteopaths were trained in France. Osteopaths can be DO doctors, DO physiotherapists, DO nurses, DO midwives, DO chiropodists, or even DO dentists.
Thus, in 2018, and out of a total of 29,612 professionals practising osteopathy, there were 17,897 osteopaths DO and 11,715 DO health professionals. The number of professionals using the title of osteopath has roughly tripled in 8 years (11608 in 2010 for 29612 in 2018). There are currently around 30 osteopathic schools in France. About 3 out of 5 French people now consult osteopaths.
But this does not answer my question why, in France, osteopathy is allowed to thrive in a virtually evidence-free space! To be honest, I do not know its answer.
Perhaps someone else does?
If so, please enlighten me.
The aims of this bibliometric analysis are to describe the characteristics of articles published on the efficacy of osteopathic interventions and to provide an overall portrait of their impacts in the scientific literature. A bibliometric analysis approach was used. Articles were identified with searches using a combination of relevant MeSH terms and indexing keywords about osteopathy and research designs in MEDLINE and CINAHL databases. The following indicators were extracted: country of the primary author, year of publication, journals, impact factor of the journal, number of citations, research design, participants’ age group, system/body part addressed, primary outcome, indexing keywords and types of techniques.
A total of 389 articles met the inclusion criteria. The number of empirical studies doubled every 5 years, with the United States, Italy, Spain, and the United Kingdom being the most productive countries. Twenty-three articles were cited over 100 times. Articles were published in 103 different indexed journals, but more than half (53.7%) of articles were published in one of three osteopathy-focused readership journals. Randomized control trials (n = 145; 37.3%) and case reports (n = 142; 36.5%) were the most common research designs. A total of 187 (48.1%) studies examined the effects of osteopathic interventions using a combination of techniques that belonged to two or all of the classic fields of osteopathic interventions (musculoskeletal, cranial, and visceral).
The authors concluded that this bibliometric analysis shows that publications about efficacy of osteopathy are relatively recent and have increased at a rapid pace over the last three decades. More than half of these publications are published in three osteopathic journals targeting a limited, disciplinary-focused readership. Our results highlight important needs for large efficacy and effectiveness trials, as well as study designs to further understanding of the mechanisms of action of the techniques being investigated. Finally, this bibliometric analysis can assist to identify osteopathy techniques and populations where further clinical research is required.
What the authors fail to state is that their analysis discloses osteopathy to be an area of utter unimportance. Less than 400 studies in 52 years is a dismal result. The fact that they were mostly published in journals of no impact makes it even worse. Twenty-three articles were cited more than 100 times; this is dismal! To put it in perspective, I have ~250 articles that were cited more than 100 times. Does that suggest that my work has made about 10 times more impact than the entire field of osteopathy?
A substantial number of patients globally receive spinal manipulative therapy (SMT) to manage non-musculoskeletal disorders. However, the efficacy and effectiveness of these interventions to prevent or treat non-musculoskeletal disorders remain controversial.
A Global Summit of international chiropractors and scientists conducted a systematic review of the literature to determine the efficacy and effectiveness of SMT for the primary, secondary and tertiary prevention of non-musculoskeletal disorders. The Global Summit took place on September 14-15, 2019 in Toronto, Canada. It was attended by 50 chiropractic researchers from 8 countries and 28 observers from 18 chiropractic organizations. Participants met the following criteria: 1) chiropractor with a PhD, or a researcher with a PhD (not a chiropractor) with research expertise in chiropractic; 2) actively involved in research (defined as having published at least 5 peer-reviewed papers over the past 5 years); and 3) appointed at an academic or educational institution. In addition, a small group of researchers who did not meet these criteria were invited. These included three chiropractors with a strong publication and scientific editorial record who did not have a PhD (SMP, JW, and HS) and two early career researchers with expertise within the area of chiropractic and pseudoscience (ALM, GG). Participants were invited by the Steering Committee using purposive and snowball sampling methods. At the summit, participants critically appraised the literature and synthesized the evidence.
They searched MEDLINE, Embase, the Cochrane Central Register of Controlled Trials, the Cumulative Index to Nursing and Allied Health, and the Index to Chiropractic Literature from inception to May 15, 2019, using subject headings specific to each database and free text words relevant to manipulation/manual therapy, effectiveness, prevention, treatment, and non-musculoskeletal disorders. Eligible for review were randomized controlled trials published in English. The methodological quality of eligible studies was assessed independently by reviewers using the Scottish Intercollegiate Guidelines Network (SIGN) criteria for randomized controlled trials. The researchers synthesized the evidence from articles with high or acceptable methodological quality according to the Synthesis without Meta-Analysis (SWiM) Guideline. The final risk of bias and evidence tables were reviewed by researchers who attended the Global Summit and 75% (38/50) had to approve the content to reach consensus.
A total of 4997 citations were retrieved, and 1123 duplicates were removed, and 3874 citations were screened. Of those, the eligibility of 32 articles was evaluated at the Global Summit and 16 articles were included in the systematic review. The synthesis included 6 randomized controlled trials with acceptable or high methodological quality (reported in 7 articles). These trials investigated the efficacy or effectiveness of SMT for the management of
- infantile colic,
- childhood asthma,
- hypertension,
- primary dysmenorrhea,
- migraine.
None of the trials evaluated the effectiveness of SMT in preventing the occurrence of non-musculoskeletal disorders. A consensus was reached on the content of all risk of bias and evidence tables. All randomized controlled trials with high or acceptable quality found that SMT was not superior to sham interventions for the treatment of these non-musculoskeletal disorders.
Six of 50 participants (12%) in the Global Summit did not approve the final report.
The authors concluded that our systematic review included six randomized clinical trials (534 participants) of acceptable or high quality investigating the efficacy or effectiveness of SMT for the treatment of non-musculoskeletal disorders. We found no evidence of an effect of SMT for the management of non-musculoskeletal disorders including infantile colic, childhood asthma, hypertension, primary dysmenorrhea, and migraine. This finding challenges the validity of the theory that treating spinal dysfunctions with SMT has a physiological effect on organs and their function. Governments, payers, regulators, educators, and clinicians should consider this evidence when developing policies about the use and reimbursement of SMT for non-musculoskeletal disorders.
I would have formulated the conclusions much more succinctly:
As has already been shown repeatedly, there is no sound evidence that SMT is effective for non-musculoskeletal conditions.
Two chiropractors conducted a retrospective review of publicly available data from the California Board of Chiropractic Examiners. Their aim was to determine categories of offense, experience, and gender of disciplined doctors of chiropractic (DC) in California and compare them with disciplined medical physicians in California.
Retrospective reviews of publicly available data from the California Board of Chiropractic Examiners.
The DC disciplinary categories, in descending order, were
- fraud (44%),
- sexual boundary issues (22%),
- other offences (13%),
- abuse of alcohol or drugs (10%),
- negligence or incompetence (6%),
- poor supervision (2%),
- mental impairment (.3%).
The authors concluded that the professions differ in the major reasons for disciplinary actions. Two thirds (67%) of the doctors of chiropractic were disciplined for fraud and sexual boundary issues, compared with 59% for negligence and substance misuse for medical physicians. Additional study in each profession may reveal methods to identify causes and possible intervention for those who are at high risk.
The two authors of this paper should be congratulated for their courage to publish such a review. These figures seem shocking. But I think that in reality some of them might be far higher. Take the important matter of competence, for instance. If you consider it competent that chiropractors treat conditions other than back pain, you might arrive at the above-mentioned figure of 6%. If you consider this as incompetent, as I do, the figure might be one order of magnitude higher (for more on unprofessional conduct by chiropractors see here).
The abstract of the paper does not provide comparisons to the data related to the medical profession. Here they are; relative to doctors, chiropractors are:
- 2x more likely to be involved in malpractice,
- 9x more likely to be practising fraud,
- 2x more likely to transgress sexual boundaries.
The frequency of fraud is particularly striking. Come to think of it, however, it is not all that amazing. I have said it before: chiropractic is in my view mostly about money.
It has been reported that B.C.’s chiropractors are deeply divided about the future of their profession, disagreeing on everything from false advertising to the use of routine X-rays.
Chiropractors attending an extraordinary general meeting of the College of Chiropractors of B.C. were split nearly down the middle on a series of non-binding resolutions addressing actions the College has taken in recent years. By the narrowest of margins, with at most 54% support, the members voted in favor of the college’s moves to limit the use of diagnostic X-rays and ban claims that aren’t supported by scientific evidence. The question that remains is who represents the bulk of the profession in B.C. — chiropractors advocating for what they describe as evidence-based practice targeting the musculoskeletal system, or “vitalists” who argue that chiropractic treatment can help with everything from immunity to brain function.
The modernizers see it as “a deliberate attempt to take over the college by a small group of chiropractors with no respect or knowledge of regulation … funded by organizations out of the province and out of the country,” Victoria chiropractor Clark Konczak told the virtual meeting.
At issue was a series of policies the college introduced in the wake of what Konczak called “the smoothie episode.” He was referring to a video posted on Facebook in 2017 by the then-vice chair of the college’s board, Avtar Jassal, in which he falsely suggested fruit smoothies are better than vaccines at preventing the flu.
Earlier this year, the college introduced amendments that bar chiropractors from performing routine and repeat X-rays, saying radiography is only scientifically supported when there are red flags that something is seriously wrong. The policy change on X-rays was the flashpoint in the long-simmering tension within the profession. A group of chiropractors has filed a petition in B.C. Supreme Court, alleging the college is preventing them from providing “safe, ethical, and effective care to their patients.” Their legal action has backing from national and international vitalistic organizations. During the recent meeting, a group of chiropractors argued unsuccessfully for the new X-ray policy to be tossed. Some suggested that chiropractors who don’t perform X-rays as a matter of routine are actually harming their patients. Another extraordinary general meeting has been called for July 20 to vote on resolutions calling for the removal of four college board members.
As I have often pointed out, chiropractic is all about money. The ‘chiro-wars’ have been going on for quite a while now, and they are by no means confined to B. C. or Canada. In a nutshell, they suggest to me that a significant proportion of chiropractors prefer money to progress.