quackery
“The decline of homeopathy, the ‘medicine’ that doesn’t cure anything” is the title of a remarkable article in EL PAIS of which I take the liberty of showing you a few key passages:
In the more than 200 years that have passed since its invention, no one has been able to prove that homeopathy is actually capable of curing anything with its alleged medicines that have no active ingredients…
…EL PAÍS reached out to some of its main promoters, such as the pharmaceutical company Boiron, leader in the sector; the Spanish Association of Homeopathy Pharmacists and the Spanish Society of Homeopathic Doctors. In the absence of a response from all three, the explanations are given by experts who are more critical of the discipline.
Many people who used to consume homeopathy were not even aware that this was the case. Fernando Frías, one of the activists who worked to undermine the discipline’s remaining prestige, recalls that people did not believe them when they were told that compounds with diluted Berlin Wall were sold to overcome the feelings of oppression and anxiety. This was actually commercialized under the premise that “like cures like”: if the Berlin Wall oppressed, a piece of it diluted in water should remedy it. “Many were under the impression that it was just a natural therapy and that we were making things up to attack it,” says Frías…
… There has been a lot of debate about how to regulate an alleged drug whose only effect is, in truth, the placebo effect. In 2001, the European Parliament issued a directive that covered its use in countries with a homeopathic tradition; sources explain that this happened due to the pressure exerted by both the industries and the governments of countries where pseudoscience is deep-rooted, such as France (where Boiron is headquartered) or Germany, where its consumption is much higher than in others, such as Spain.
“Having regard to the particular characteristics of these homeopathic medicinal products, such as the very low level of active principles they contain and the difficulty of applying to them the conventional statistical methods relating to clinical trials, it is desirable to provide a special, simplified registration procedure for those homeopathic medicinal products which are placed on the market without therapeutic indications in a pharmaceutical form and dosage which do not present a risk for the patient,” states the directive.
In its more than two centuries of history, this is not the first time that homeopathy loses ground. Still, Frías warns, it cannot be ruled out that at some point something will come up that will make it fashionable again. “Look at the example of chemtrails [the condensation trails left by airplanes that some conspiracy theorists believe are a way of poisoning the population from the air]. It seemed that no one remembered them anymore, but now they’re back,” he says. Frías cites the astrophysicist and disseminator Javier Armentia, who states that beliefs are like a rubber duck: no matter how much they sink, they always resurface. “Especially if there is money behind,” he adds.
______________________
As reported previously, homeopathy and other forms of so-called alternative medicine (SCAM) have come under fire in Spain. In 2017, ‘HOMEOPATHY PLUS‘ reported that “in a reversal of the 2015 Royal Legislative Decree, the Minister of Health has withdrawn homeopathic remedies and outlawed the practice in Spain’s national health services.” In 2018, more than 400 people signed an open letter triggered by the case of a cancer patient who died after preferring homeopathy to regular treatment. “Let’s be clear: pseudoscience kills,” begins the letter. Since then, the struggle of Spanish rational thinkers to stop misleading information about SCAM in general and homeopathy, in particular, has only intensified.
Spain is thus joining other European countries in opposing misinformation about homeopathy. Contrary to what some have claimed (for instance, in the comments section of this blog), most of the opponents do not want to restrict the public’s choice. People who wish to use homeopathy should be able to do so (but should pay for it themselves). However, the choice must be based on evidence-based information.
Semen retention is a so-called alternative medicine (SCAM) that involves intentionally avoiding ejaculating. A person can do this by abstaining from any sexual activity, stopping before the point of ejaculation, or teaching themselves to orgasm without ejaculating.
Although this practice may seem new, this is likely only due to recent internet popularity. In fact, semen retention is an ancient practice, believed to boost male physical and spiritual energy.
Some other names for semen retention include:
- coitus reservatus
- seminal conservation
- sexual continence
It is also known as or included in practices called:
- karezza (Italian)
- maithuna (Hindu Tantra)
- sahaja (Hindu Yoga)
- tantra (Hinduism and Buddhism)
- cai Yin pu Yang and cai Yang pu Yin (Taoist)
Semen retention is said to be good for a range of things:
Mental health
- increased motivation
- improved energy and focus
- more self-confidence
- reduced anxiety
- better memory
- improved concentration
Physical health
- clearer skin
- increased testosterone
- more weight loss
- increased muscle mass
- physical rejuvenation
- a deeper voice
Spiritual health
- a greater sense of purpose
- stronger or deeper emotional bonds in relationships
- a stronger sense of overall harmony
________________________
Yes, I agree, this sounds weird!
But is there any evidence?
Yes, e.g.:
Males of some species use mate retention behavior and investment in ejaculate quality as anti-cuckoldry tactics concurrently while others do so in a compensatory fashion. Leivers, Rhodes, and Simmons (2014) reported that men who performed mate retention less frequently produced higher-quality ejaculates, suggesting that humans use these tactics compensatorily. We conducted a conceptual replication of this research in a sample of 41 men (18-33 years; M = 23.33; SD = 3.60). By self-report, participants had not had a vasectomy and had never sought infertility treatment. We controlled for several covariates known to affect ejaculate quality (e.g., abstinence duration before providing an ejaculate) and found no statistically significant relationships between mate retention behavior and four components of ejaculate quality: sperm velocity, sperm concentration, slow motility, and ejaculate volume. The present results provide little support for the hypothesis that human males deploy mate retention behavior and ejaculate quality investment compensatorily. We discuss the limitations of this study and highlight the need for research to address questions about the nature of anti-cuckoldry tactic deployment in humans, especially concerning investment in ejaculate quality.
In species where females mate with multiple males, the sperm from these males must compete to fertilise available ova. Sexual selection from sperm competition is expected to favor opposing adaptations in males that function either in the avoidance of sperm competition (by guarding females from rival males) or in the engagement in sperm competition (by increased expenditure on the ejaculate). The extent to which males may adjust the relative use of these opposing tactics has been relatively neglected. Where males can successfully avoid sperm competition from rivals, one might expect a decrease in their expenditure on tactics for the engagement in sperm competition and vice versa. In this study, we examine the relationship between mate guarding and ejaculate quality using humans as an empirical model. We found that men who performed fewer mate guarding behaviors produced higher quality ejaculates, having a greater concentration of sperm, a higher percentage of motile sperm and sperm that swam faster and less erratically. These effects were found independent of lifestyle factors or factors related to male quality. Our findings suggest that male expenditure on mate guarding and on the ejaculate may represent alternative routes to paternity assurance in humans.
The uncritical application of western psychiatric concepts in non-western societies resulting in culturally invalid psychiatric syndromes, have been extensively documented. Such instances are considered ‘category errors’. In contrast, ‘reverse category errors’ although theoretically postulated, have never been empirically demonstrated. Diagnostic criteria of an established South Asian culture specific neurosis, Dhāt syndrome, were deployed by a psychiatrist of South Asian origin, amongst 47 white Britons in London, UK, presenting for the first time with a clinic diagnosis of ICD-9 Depressive Neurosis (Dysthymic Disroder, ICD-11). The proceedure yielded a new disorder, Semen Retention Syndrome. Based on narrative accounts and quantitative scores on the Hamilton Depression Rating Scale, the evidence suggests that a significant subset of white British subjects diagnosed with Dysthymic Disorder, may in fact be expressing a psychological variation of a previously unknown local White British somatisation phenomena labelled Semen Retention Syndrome. Anxiety and depressive symptoms presented by this subset of subjects were primarily attributed to a core irrational belief and a cognitive error centered around misunderstood concepts of semen physiology. Consequently, the undue focus on mood idioms by both white British patients and their health professionals, leads to a mistaken diagnosis of Mood Disorder, and results in incorrect treatment. The implications of this ethnocentric mode of reasoning raises concerns about existing concepts in psychiatric phenomenology and for official international diagnostic classificatory systems. The paper concludes by arguing that category errors in both directions are instances of cultural iatrogenesis, and underscore the importance of a culturally valid psychiatry.
_________________________
I was unable to find support for any of the above-listed effects of semen retention. So, claims like “Semen Retention is life-changing, especially for men. Not only, it help you turn into a real alpha male but also offers great health benefits” need to be taken with a pinch of salt. Yet, it did occur to me that semen retention might have one positive outcome:
It reduces the chances of stupid people multiplying!
An explanatory sequential mixed methods study with three separate phases was conducted in Danish patients with lumbar radiculopathy receiving a standardized chiropractic care package (SCCP). Lumbar radiculopathy is pain and other neurological symptoms caused by the pinching of nerve roots where they leave your spinal cord in the lumbar region. 
Phase one of the study was a quantitative analysis based on a survey in a prospective cohort of patients with lumbar radiculopathy in an SCCP from 2018 to 2020. Patients rated their satisfaction with the examination, information, treatment effect, and overall management of their problem on a 0–10 scale. In phase two, six semi-structured interviews conducted in 2021 were used to gain further explanatory insights into the findings from phase one. Data were analyzed using systematic text condensation. In phase three, the quantitative and qualitative data were merged in a narrative joint display to obtain a deeper understanding of the overall results.
Here I am only interested in the patients’ perception of the treatment effect. Of 303 eligible patients, 238 responded to the survey. Of these, 50% were very satisfied with the treatment effect.
The authors stated that patients in their study expected a rapid and persistent decrease in symptoms, which, unfortunately, does not match the prognosis of lumbar radiculopathy. Although the prognosis is considered good, the improvement happens gradually and often with fluctuating pain patterns, and it is not unusual to have milder symptoms for three months or longer.
So, only half of the patients who had chosen to consult chiropractors for their lumbar radiculopathy were very satisfied with the treatment results. In most patients, the symptoms decreased only gradually often with fluctuating pain patterns, and the authors comment that symptoms frequently last for three months or longer with a SCCP.
Impressive?
Might I point out that what is being described here looks to me very much like the natural history of lumbar radiculopathy? About 90% of patients with back pain caused by disc herniation see improvements within three months without therapy. Are the authors aware that their observational study is in accordance with the notion that the SCCP does nothing or very little to help patients suffering from lumbar radiculopathy?
It has been reported, at the German Medical Congress (DÄT) a year ago, that it was decided to delete the additional title of homeopathy from the model further training regulations of the German Medical Association. And Federal Health Minister Karl Lauterbach (SPD) tweeted applause: “Homeopathy has no place in modern medicine.”
Now the ‘ Bundesverband der Pharmaziestudierenden in Deutschland’ (BPhD), the German Pharmacists Organization, even goes a few steps further. The position paper distinguishes between evidence-based medicine (EBM) and unproven therapeutic methods. According to the BPhD, these include homeopathy, but also anthroposophy, traditional Chinese medicine, and traditional medicines.
Among other things, the BPhD is disturbed by the way homeopathy presents itself as an alternative, because an alternative means “a choice between two equally suitable possibilities” to achieve a goal, and this is not the case. Compared to evidence-based medicine (EBM), homeopathy is a “constructed, illusory concept” and “the principles of homeopathic teachings and principles” are to be rejected as “unscientific”. According to the BPhD, a designation as “alternative” for advertising purposes should no longer be allowed.
They would also like to see a demarcation from naturopathy; the clear distinction between homeopathy and phytopharmacy has been lacking up to now. The advertising attribute “natural” should therefore also be banned in order to prevent equalization in advertising, the position paper states.
Like doctors, pharmacy students point to the lack of proof of efficacy beyond the placebo effect. According to the BPhD, the dogma WER HEILT HAT RECHT, “he who heals is right” would “disregard all processes that work towards healing and glorify the result”. The “gold standard” of EBM – randomized, double-blind studies with placebo control – should in future also have to be fulfilled by homeopathic medicines, experience reports are not sufficient, it continues.
Homeopathic medicines are only registered as medicinal products without indication, which requires neither proof of efficacy nor clinical studies. The BPhD, therefore, demands that a warning be placed on the preparations that they have “no proven efficacy beyond the placebo effect”. Up to now, without this warning, patients have been “deceived about the efficacy”, and there is an “urgent need for detailed public information and counseling on homeopathy since its unjustified reputation poses a danger of not seeking treatment”. The BPhD also demands that the status of homeopathic medicines is withdrawn and that the pharmacy obligation for the preparations is abolished…
“In the health professions, no trivialization of unproven therapeutic procedures should be tolerated, as inadequate counseling or ignorance poses a danger to patients,” the BPhD said.
_________________________
When I first read this article – I translated and shortened it for those who cannot read German- I was truly dazzled. These are the suggestions that I have been making for around 20 years now, not specifically for Germany but for pharmacists in general. For many years, the Germans seemed the least likely to agree with me. But now they seem to be ahead of everyone else in Europe!
How come?
I suspect and hope that our recent initiative might have something to do with it.
Let’s hope that the pharmacists of other countries follow the German example.
A team of French researchers assessed whether a conflict of interest (COI) might be associated with the direction of the results of meta-analyses of homoeopathy trials. Their analysis (published as a ‘letter to the editor) is complex, therefore, I present here only their main finding.
The team conducted a literature search until July 2022 on PubMed and Embase to identify meta-analyses of randomized clinical trials assessing the efficacy of homoeopathy. They then assessed the existence of potential COI, defined by the presence of at least one of the following criteria:
- affiliation of one or more authors to an academic homoeopathy research or care facility, or to the homoeopathy industry;
- research sponsored or funded by the homoeopathy industry;
- COI declared by the authors.
The researchers also evaluated and classified any spin in meta-analyses conclusions into three categories (misleading reporting, misleading interpretation and inappropriate extrapolation). Two reviewers assessed the quality of meta-analyses and the risk of bias based. Publication bias was evaluated by the funnel plot method. For all the studies included in these meta-analyses, the researchers checked whether they reported a statistically significant result in favour of homoeopathy. Further details about the methods are provided on OSF (https://osf.io/nqw7r/) and in the preregistered protocol (CRD42020206242).
Twenty meta-analyses were included in the analysis (list of references available at https://osf.io/nqw7r/).
- Among the 13 meta-analyses with COI, a significantly positive effect of homoeopathy emerged (OR=0.60 (95% CI 0.50 to 0.70)).
- There was no such effect for meta-analyses without COI (OR=0.96 (95% CI 0.75 to 1.23)).
The authors concluded that in the presence of COI, meta-analyses of homoeopathy trials are more likely
to have favourable results. This is consistent with recent research suggesting that systematic reviews with financial COI are associated with more positive outcomes.
Meta-analyses are systematic reviews (critical assessments of the totality of the available evidence) where the data from the included studies are pooled. For a range of reasons, this may not always be possible. Therefore the number of meta-analyses (20) is substantially lower than that of the existing systematic reviews (>50).
Both systematic reviews and meta-analyses are theoretically the most reliable evidence regarding the value of any intervention. I said ‘theoretically’ because, like any human endeavour, they need to be done in an unbiased fashion to produce reliable results. People with a conflict of interest by definition struggle to be free of bias. As we have seen many times, this would include homoeopaths.
This new analysis confirms what many of us have feared. If proponents of homeopathy with an overt conflict of interest conduct a meta-analysis of studies of homeopathy, the results tend to be more positive than when independent researchers do it. The question that emerges from this is the following:
Are the findings of those researchers who have an interest in producing a positive result closer to the truth than the findings of researchers who have no such conflict?
I let you decide.
In response to yesterday’s post, I received a lengthy comment from ‘Stan’. Several readers have already commented on it. Therefore, I can make my arguments short. In this post, will repeat Stan’s points each followed by my comments (in bold). Here we go:
Seven Reasons Homœopathy is Not Placebo Effect
Sorry, Stan, but your heading is not proper English; I have therefore changed it for the title of this post.
1. Homeopathic remedies work on babies, animals, plants and people in a coma. Biodynamic farmers use homeopathic remedies to repel pests and treat plant diseases. Some organic ranchers rely on homeopathic remedies to treat their herds. Some “placebo by proxy” effect has been shown for children but its doubtful that it could be shown for a herd of cattle or crops in a field. Farmers can’t rely on wishful thinking to stay in business.
As discussed ad nauseam on this blog, homeopathic remedies do not work on babies or animals better than placebos. I don’t know of any studies with “people in a coma” (if you do, Stan, please let me know). The fact that ranchers rely on homeopathy is hilarious but does not prove anything.
2. The correct curative remedy will initially cause a worsening of the condition being cured if it is given in too strong (i.e. too dilute) a dose. A placebo might only cause a temporary improvement of the condition being treated; certainly not an aggravation.
The ‘homeopathic aggravation’ is a myth created by homeopaths. It disappears if we try to systematically research it; see here, for instance.
3. One can do a “proving” of an unknown homeopathic remedy by taking it repeatedly over several days and it will temporarily cause symptoms that one has never experienced previously – symptoms it will cure in a sick person. This is a repeatable scientific experiment used to determine the scope of a new remedy, or confirm the effects of an already proven remedy. A placebo might possibly have an effect if the individual taking it has been “prepared” by being told what they are taking but it likely wouldnt match previously recorded symptoms in the literature.
Homeopathic provings are rubbish and not reproducible when done rigorously; see here.
4. One can treat simple acute (self-limiting) conditions (e.g. minor burns, minor injuries, insect bites, etc.) and see unusually rapid cures with homeopathic remedies. A placebo might only cause a temporary improvement of the condition being treated while taken. Placebos have been found mostly effective in conditions with a strong psychological component like pain.
You mean like using Arnica for cuts and bruises? Sadly, it does not work.
5. One can get homeopathic treatment for long term chronic (non self-limiting) conditions and see a deep lasting cure, as has been documented clinically for a couple centuries. A placebo might only cause a temporary partial improvement of the condition being treated while the placebo is being taken.
You mean like asthma, eczema, or insomnia?
6. There is over 200 years worth of extensive documentation from around the world, of the clinical successes of homeopathy for both acute and chronic conditions of all types. As Dr Hahn has said you have throw out 90% of the evidence to conclude that homeopathy doesnt work. The Sheng et al meta-analysis in 2005 Lancet that was supposedly the death knell of homeopathy used only 8 studies, excluding hundreds of others. Unsurprisingly homeopathy was found wanting. So-called Skeptics see what they want to see in the science. There is relatively little documentation of placebo usage. A few recent studies have been done showing the limited temporary benefits of placebos.
What Hahn wrote is understandably liked by homeopaths but it nevertheless is BS. If you don’t trust me, please rely on independent bodies from across the world.
7. Homeopathic remedies have been shown to have a very weak electromagnetic signature and contain some nano-particles. Some believe this explains their mechanism. An exciting new potential field of research is the subtle cell signalling that has been found to direct the development of stem cells. Scientists have created double-headed planeria worms and this trait has been found to be inherited by their offspring without any change in the genes or epigenetics. Until now we had no idea how a single fertilized ovum could evolve into a complex creature that is bilateral and has multiple cell types. It is possible that the very subtle electromagnetic signature or some other unknown effect of homeopathic remedies is effecting this subtle cell signalling.
The homeopathic nano-myth is nonsense. And so is the rest of your assumptions.
Every conventional drug has “side effects” that match the symptoms for which it is indicated! Aspirin can cause headaches and fever, ritalin can cause hyperactive effects, radiation can cause cancer. Conventional doctors are just practicing bad homeopathy. They are prescribing Partially similar medicines. If their drugs were homeopathic (i.e. similar) to the patients symptoms on all levels they would be curative. Radiation sometimes does cure cancer instead of just suppressing it per usual.
Even if this were true, what would it prove? Certainly not that homeopathy works!
Dr Hahneman did forbid mixing homeopathy and conventional medicine. In his day doctors commonly used extensive blood letting and extreme doses of mercury. Its not Quite as bad now.
You evidently did not read Hahnemann’s writings.
Just because we dont know how extremely dilute homeopathic remedies work, doesn’t discount that they Do work. Homeopathy seems to fly in the face of Known science. In no way is it irrational or unscientific. There are lots of phenomena in the universe that cant be explained yet, like dark energy and dark matter effects and even consciousness!
Not knowing how a treatment works has not stopped science to test whether it works (e.g. Aspirin). In the case of homeopathy, the results of these endeavors were not positive.
The assumption that the moon is made of cheese also flies in the face of science; do you perhaps think that this makes it true?
The actions of homeopathy can and have been well-explained: they are due to placebo effects.
________________________
Stan, thank you for this entertaining exercise. But, next time, please remember to supply evidence for your statements.
After all these years, I am still fascinated by what proponents of homeopathy try to tell others about their trade. Recently I found a long article in this vein. It is aimed at an audience of HEILPRAKTIKER and their patients. It should therefore be responsible, thorough, and evidence-based (yes, I am an optimist).
“With this article”, the authors state, “we aim to provide a comprehensive overview of homeopathy and help people make informed decisions about their health. Whether you already have experience with homeopathy or simply want to inform yourself, we hope that this article will provide you with valuable insights and information” (my translation).
Here I present to you just the relatively short section dedicated to the ‘pros and cons’ of homeopathy. Here we go:
Advantages of homeopathy:
- Holistic approach: homeopathy considers the human being as a whole and takes into account both physical and emotional aspects. It aims to support individual balance and the body’s self-healing powers.
- Gentle and non-invasive treatment: Homeopathic remedies are usually taken as globules, drops, or tablets and are therefore easy and convenient to use. They rarely cause side effects and are generally well tolerated.
- Individualized treatment: In homeopathy, each patient is considered unique and treatment is based on individual symptoms and characteristics. There is no “one-size-fits-all” solution, but a personalized approach.
- Support for chronic diseases: Homeopathy can be an alternative or complementary treatment for chronic conditions where conventional medicines offer limited relief. It can help improve quality of life and promote overall well-being.
Limitations of homeopathy:
- Placebo effect: Much of the effect of homeopathy is attributed to the placebo effect. It is argued that the improvements patients experience occur because of belief in the efficacy of the remedies and positive expectations, rather than due to a specific effect of the diluted substances.
- Lack of scientific evidence: The scientific evidence for the efficacy of homeopathy is limited and controversial. Many studies have failed to demonstrate benefits beyond the placebo effect. There is a lack of well-conducted randomized controlled trials that clearly show the effectiveness of homeopathy.
- Delay or rejection of conventional treatments: In some cases, the choice of homeopathy as the sole method of treatment may lead to delays in the diagnosis and timely treatment of serious or acute illnesses. It is important that serious illnesses are examined by a doctor and treated appropriately.
- Difficulties in standardization: Homeopathy involves a variety of remedies used in different potencies and dilutions. This makes standardization and the conduct of reproducible studies difficult. There are also controversial debates about whether the dilutions go beyond the extent to which molecules of the original substance are still present.
__________________________
I am sure that you have heard the BS about the alleged advantages of homeopathy often enough. Therefore, I will here not bother to comment on them again. More interesting, in my view, are the limitations of homeopathy, as seen by its proponents. Please allow me, therefore, to discuss them briefly.
- The authors state that “it is argued that the improvements patients experience occur because of belief in the efficacy of the remedies and positive expectations”. This sounds as though this is a mere aberrant opinion or at least an ongoing debate amongst scientists. In fact, it is the scientific consensus supported by tons of evidence.
- This is the same point expressed differently.
- The admission that “the choice of homeopathy as the sole method of treatment may lead to delays in the diagnosis and timely treatment” is yet another way of stating that homeopathy is not effective. What is, however, not expressed clearly enough, in my view, is the fact that homeopathic treatment usually amounts to medical neglect which is unethical and can cause serious harm, in extreme cases even death.
- It is not true that the range of potencies renders “the conduct of reproducible studies difficult”. There are plenty of examples to demonstrate this, for instance, this study. “There are also controversial debates about whether the dilutions go beyond the extent to which molecules of the original substance are still present.” Yes, I did translate this correctly. I am sorry to say that this sentence does make no sense in German or in English.
What I find particularly interesting is that the authors do not mention disadvantages that non-homeopaths would rate as quite important, e.g.:
- The assumptions of homeopathy fly in the face of science.
- Hahnemann strictly forbade homeopathy to be combined with ‘allopathy’ (yet proponents now claim this option to be an advantage).
- Treating a patient with homeopathy violates even the most basic rules of medical ethics.
- Homeopaths have no choice but to lie to their patients on a daily basis.
- Many homeopaths have the nasty habit of advising their patients against using effective treatments, e.g. vaccinations.
- Homeopathy undermines rational thinking in a general way.
In summary, the authors’ “aim to provide a comprehensive overview of homeopathy and help people make informed decisions about their health” has not been reached.
It has recently been reported that a 39-year-old woman (a mother-of-three died) died after immersing herself in a river as part of a cold water therapy session. The woman died after paramedics were called to attend a riverside in Derbyshire. The session was run by Kevin O’Neill of ‘Breatheolution’, whose previous clients include Coleen Rooney and actor Stephen Graham. The woman, who was visiting with two friends after paying up to £200 for a two-hour cold water therapy session, was rushed to hospital where she died.

Mr. O’Neill commented: “I am heartbroken. I’ve not slept and I’m finding it hard to process. I cannot stop thinking about her family. It’s tragic.” An inquest is expected to be opened into the woman’s death. East Midlands Ambulance Service said they were called to Bankside, in Bridgemont. “The caller reported a medical emergency,” a spokesperson said. “We sent a paramedic in a fast response car and a double-crewed ambulance. The air ambulance was also in attendance.”
Derbyshire Fire and Rescue Service, which was called to assist the paramedics, has warned people about the dangers of entering open water. “While we cannot and will not comment or speculate on the circumstances and cause of this tragic death, we would like to remind people of the dangers of entering open water and cold water shock,” said group manager Lee Williams.
_____________________
Breatheolution’ has a website where a whole page is dedicated to its leader Kevin O’Neill. I wondered what qualifications Kevin has, but all it tells us about him is this: “I struggled for so long with alcohol and other substance abuse that something had to give, I lost my sister Yvonne in 2019 and I think it was enough trauma to make me think a lot more about my own life”
The website also explains what the cold water sessions are about:
1-2-1 Breath Coaching, practice & Cold water session (river or tank)
2 hours @ £110.00
These sessions are proving popular with those who are not keen on group sessions or just prefer to have a more personal experience. The 2-3 hour sessions will be tailored to you and your breathing and will include potentially life-changing tools and methods to allow you to witness your breathing and physiology differently in the future, its all about feeling and awareness.
Another section of the site is dedicated to celebrities who Kevin seems to have treated. And then there is a video of the treatment. What I did not find anywhere, however, are the conditions that Kevin claims to treat with his cold water therapy.
In any case, it would have been wise for Kevin to read up about the risks of cold water immersion (CWI) before going into business. Perhaps this review would have helped:
In 2012, an estimated 372,000 people (42 per hour) died from immersion, assumed to be drowning. Immersion is the third leading cause of unintentional injury-related death, accounting for 7% of all such deaths (World Health Organization, 2014). These figures are underestimations owing to poor reporting in many Third World countries that have a high number of deaths. The data also do not include life-long morbidity caused by immersion-related injuries, estimated to be a much bigger numerical problem.
There is no strict definition of ‘cold water’. Given that some of the hazardous responses to cold water appear to peak on immersion somewhere between 15 and 10°C, it is reasonable to say that cold water is water <15°C (Tipton et al. 1991). However, the thermoneutral water temperature for a resting naked individual is ∼35°C, so it is possible for individuals to become very cold, with time, on immersion in water below this temperature. The corresponding temperature for those exercising (including shivering) is ∼25°C (Tipton & Golden, 1998).
Historically, the threat associated with CWI was regarded in terms of hypothermia or a reduction in deep body temperature below 35°C. This belief was established as a result of the Titanic disaster and supported by data obtained during maritime conflicts of World War II. However, more recently, a significant body of statistical, anecdotal and experimental evidence has pointed towards other causes of death on immersion. For example, in 1977 a Home Office Report revealed that ∼55% of the annual open water deaths in the UK occurred within 3 m of a safe refuge (42% within 2 m), and two-thirds of those who died were regarded as ‘good swimmers’. This evidence suggests more rapid incapacitation than can occur with whole-body cooling and consequent hypothermia.
The following four stages of immersion have been associated with particular risks (Golden & Hervey, 1981; Golden et al. 1991); the duration of these stages and the magnitude of the responses evoked within them vary significantly, depending on several factors, not least of which is water temperature:
- Initial immersion (first 3 min), skin cooling;
- Short-term immersion (3 min plus), superficial neuromuscular cooling;
- Long-term immersion (30 min plus), deep tissue cooling (hypothermia); and
- Circum-rescue collapse: immediately before, during or soon after rescue.
As a result of laboratory-based research, the initial responses to immersion, or ‘cold shock’, were identified as particularly hazardous (Tipton, 1989), accounting for the majority of immersion deaths (Tipton et al. 2014). These deaths have most often been ascribed to drowning, with the physiological responses of a gasp and uncontrollable hyperventilation, initiated by the dynamic response of the cutaneous cold receptors, resulting in the aspiration of the small volume of water necessary to initiate the drowning process (Bierens et al. 2016). Relatively little is known about the minimal rates of change of cold receptor temperature necessary to cause cold shock. The response has been reported to begin in water as warm as 25°C but is easy to suppress consciously at that temperature. In laboratory conditions, the respiratory frequency response (an indication of respiratory drive) peaks on naked immersion in a water temperature between 15 and 10°C, and is no greater on immersion in water at 5°C (Tipton et al. 1991). The corresponding average rates of change of chest skin temperature over the first 20 s of these immersions was 0.42 (water temperature 15°C), 0.56 (water temperature 10°C) and 0.68°C s−1 (water temperature 5°C). This suggests that an average rate of change in chest skin temperature between 0.42 and 0.56°C s−1 on the first 20 s of immersion is sufficient to evoke a maximal respiratory cold shock response.
More recently, it has been suggested (Shattock & Tipton, 2012) that a larger number of deaths than once thought may be attributable to arrhythmias initiated on immersion by the coincidental activation of the sympathetic and parasympathetic division of the autonomic nervous system by stimulation of cutaneous cold receptors around the body [sympathetic activation (cold shock)] and in the oronasal region on submersion or with wave splash [vagal stimulation (diving response)]. This ‘autonomic conflict’ is a very effective way of producing dysrhythmias and arrhythmias even in otherwise young and healthy individuals, particularly, but not necessarily, if a prolonged breath hold is involved in the immersion (Tipton et al. 1994). It seems that predisposing factors, such as long QT syndrome, ischaemic heart disease or myocardial hypertrophy, are necessary for fatal arrhythmias to evolve (Shattock & Tipton, 2012); many of these factors, including drug-induced long QT syndrome, are acquired. Non-fatal arrhythmias could still indirectly lead to death if they cause incapacitation and thereby drowning (Tipton, 2013). The hazardous responses associated with the cold shock response are presented in Fig. 2.
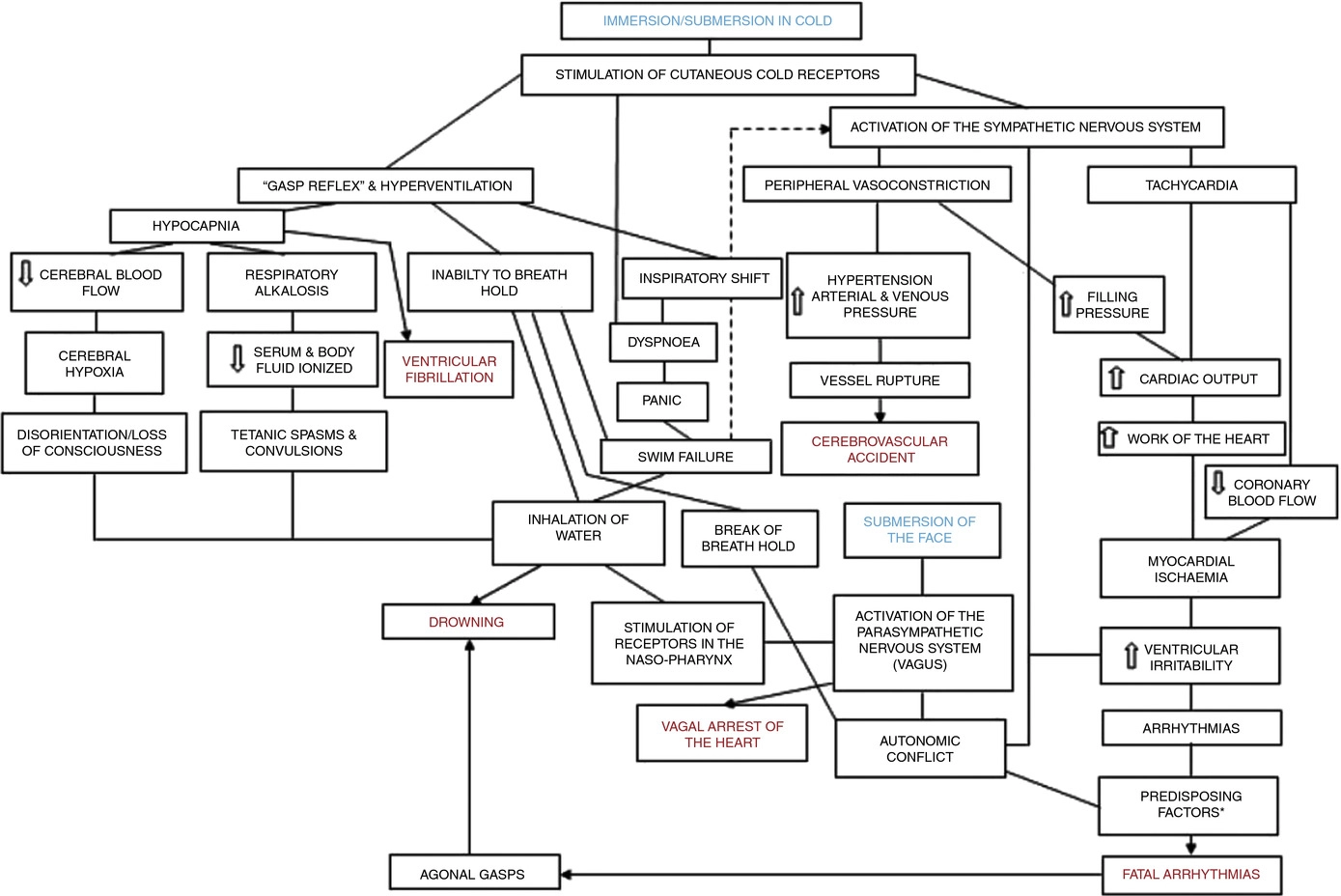
Figure 2. A contemporary view of the initial responses to immersion and submersion in cold water (‘cold shock’)
The problems encountered in short-term immersions are primarily related to physical incapacitation caused by neuromuscular cooling (Castellani & Tipton, 2015). The arms are particularly susceptible because of their high surface area to mass ratio. Low muscle temperatures affect chemical and physical processes at the cellular level. This includes metabolic rate, enzymatic activity, calcium and acetylcholine release and diffusion rate, as well as the series elastic components of connective tissues (Vincent & Tipton, 1988). Maximal dynamic strength, power output, jumping and sprinting performance are related to muscle temperature, with reductions ranging from 4 to 6% per degree Celsius reduction in muscle temperature down to 30°C (Bergh & Ekblom, 1979). At nerve temperatures below ∼20°C, nerve conduction is slowed and action potential amplitude is decreased (Douglas & Malcolm, 1955). Nerve block may occur after exposure to a local temperature of between 5 and 15°C for 1–15 min. This can lead to dysfunction that is equivalent to peripheral paralysis and can, again, result in drowning owing to the inability to keep the airway clear of the water (Clarke et al. 1958; Basbaum, 1973; Golden & Tipton, 2002; Fig. 3).

Figure 3. The ‘physiological pathways to drowning’ after immersion or submersion in cold water, with possible interventions for partial mitigation (dashed)
Abbreviations: EBA, emergency breathing aid; IS, immersion suit; and LJ, lifejacket. Reproduced with permission, from Tipton (2016b).
Even in ice-cold water, the possibility of hypothermia does not arise for at least 30 min in adults. Hypothermia affects cellular metabolism, blood flow and neural function. In severe hypothermia, the patient will be deeply unconscious. The progressive signs and symptoms (approximate deep body temperature) are shivering (36°C), confusion, disorientation, introversion (35°C), amnesia (34°C), cardiac arrhythmias (33°C), clouding of consciousness (33–30°C), loss of consciousness (30°C), ventricular fibrillation (28°C) and death (25°C) (Bierens et al. 2016). There is great variability between deep body temperature and the signs and symptoms of hypothermia. For example, although the deep body temperature associated with death is often quoted as 25°C, the lowest temperature recorded to date after accidental exposure to cold (air) and with full recovery was 12.7°C in a 28-month-old child (Associated Press, 2014). The coldest adult survivor of CWI followed by submersion had a body temperature of 13.7°C (Gilbert et al. 2000). There is also a large amount of variation in the rate at which people cool on immersion in cold water, owing to a combination of thermal factors (including water temperature and water movement, internal and external insulation) and non-thermal factors (including body size and composition, blood glucose, motion illness, racial and sex differences; Haight & Keatinge, 1973; Gale et al. 1981; White et al. 1992; Mekjavic et al. 2001; Golden & Tipton, 2002).
The most significant practical consequence of hypothermia in water is loss of consciousness; this prevents individuals from undertaking physical activity to maintain a clear airway and avoid drowning. Thus, once again, drowning is often the end-point (Fig. 3).
About 17% of those who die as a result of immersion die immediately before, during or after rescue (Golden et al. 1991). The deaths immediately before rescue are intriguing and probably related to behavioural changes at this time or the relief and psychophysiological alterations associated with imminent rescue, including a reduction in circulating stress hormone concentration and an increase in vagal tone. Death during rescue is most commonly associated with a collapse in arterial pressure when lifted vertical from the water and kept in that position for some time (Golden et al. 1991).
_____________________________
The tragic death of the woman should perhaps remind us that
- there is no SCAM or wellness treatment that is entirely harmless,
- and there are only few ‘would-be gurus’ who know what they are doing.
Richard Rasker has been one of our most loyal commentators with hundreds of sensible contributions to his credit. And now he has published a book! “This book”, he writes in his introduction, “is perhaps best described as a kind of travel guide for exploring different worlds, some of which are probably familiar, while others may be completely alien to you. Some of those worlds only exist in the minds of people, while others are very real indeed, yet often go unnoticed or have unexpected things to offer. This journey is also my personal exploration, during which I try to look through the eyes of the inhabitants of worlds that are wildly different from my own, to try and understand why those people believe certain things, and why I myself believe different things.”
Richard is not a medic, he is a man who understands science and empathizes with the many people who try to make sense of the often confusing concepts of healthcare. In his book, he takes the reader by the hand and carefully guides him or her through some of the issues that are of concern to so many of us. The journey takes us to so-called alternative medicine (SCAM) and beyond. At its end, the reader is wiser, more knowledgeable, and has learned the art of critical thinking.
Most chapters start with a story or anecdote that enables the reader to identify with the subject at hand. This serves the purpose of focusing the reader’s mind on the issue at hand which is then explained in full detail. The fact that Richard is not a medic turns out to be a strength of this book. Richard is not even tempted (as medics invariably are) to use jargon or to assume that the reader has prior knowledge of the subject. Instead, he starts from first principles and makes it impossible to get lost on the journey. What may seem complicated and confusing thus becomes clear and straightforward; what might have appeared to be dry and off-putting thus becomes lively and fascinating.
The range of topics that this book tackles is vast. It covers much of SCAM, of course. But it also includes topics that are way beyond SCAM, such as radiation and vaccination. In essence, the book deals with most things that people concerned about their health tend to worry about. Because Richard is a gifted writer who can render things simple without making them unduly simplistic, the book is a joy to read.
In my view, this book is a MUST-READ for anyone who wants to find his/her way safely through the maze of seemingly complex problems in healthcare.
‘Spagyric’ is a so-called alternative medicine (SCAM) based on the alchemy of Paracelsus (1493-1541). Paracelsus borrowed the term from “separate” (spao) and “combine” (ageiro) to indicate that spagyric preparations are based on the “separation”, “extraction” and “recombination” of the active ingredients of a substance. Plant, mineral as well as animal source materials are used.
The production of spagyric remedies is based on a complex process of maceration and fermentation of a plant extract in alcohol. It takes place in dark, thick-walled glass flasks that are hermetically sealed and kept at a controlled temperature of 37 °C for 28 days. The tincture thus obtained is then decanted and the drug residue is removed from the solution, completely dried, and burned to ash to recover the inorganic components of the plant material. The ash is subsequently dissolved in the alcoholic solution of maceration, and the finished spagyric preparation is left for 12 days before use.
Spagyric is not the most popular of all SCAMs but it certainly does have a significant following. One enthusiast claims that “spagyric essences work on a vibrational level in their action upon the emotional/mind and physical spheres and can be employed in numerous situations. Most people seek help to relieve physical symptoms. Even so, it is often necessary to address the emotional and psychological aspects which may predispose the illness or imbalance. In an era where many people are experiencing life-changing events, the ability to transition smoothly is essential for well-being and vitality. Guidance and help are required to maintain homeostasis. These medicines can help the patient to understand the root cause of their illness and learn to regain control of their lives. Some medicine systems appear to be less effective than in previous times. It has been suggested that the energetic frequency of both the earth and human organism are changing. Therefore these systems may no longer be a vibrational match for the changing frequencies. Spagyric Medicine is designed to ‘tune in with’ these current frequencies. Research suggests that the Spagyric essences may instigate improved health by energetically influencing DNA.”
After reading such weird statements, I ask myself, is there any evidence that spagyric remedies work? In my search for robust studies, I was unsuccessful. There does not seem to be a single controlled study on the subject. However, there are fragmentary reports of a study initiated and conducted by a now largely unknown healer named Karl Hann von Weyhern.
Von Weyhern (1882 – 1954) had taken a few semesters of pharmacy and medicine in Freiburg but remained without a degree. In 1930, he became a member of the NSDAP (Hitler’s Nazi party) and in 1940 he joined the SS. Around 1935, he settled in Munich as a non-medical practitioner (Heilpraktiker), and Heinrich Himmler who has a soft spot for SCAM enlisted as one of his patients. By then von Weyhern had by then made a steep career in the Nazi hierarchy, and he managed to convince Himmler that his spagyric remedies could cure tuberculosis, which was still rampant at the time. They decided to carry out experiments in this regard in the Dachau concentration camp.
Thus, von Weyhern was allowed to test spagyric remedies on forcibly recruited concentration camp prisoners. These experiments lasted for about one year and included around 150 patients who, according to von Weyhern’s iridology diagnosis, suffered from tuberculosis. Half of them were treated with spagyric remedies and the others with conventional treatments. At the end of the experiment, 27 persons were reportedly released into everyday concentration camp life as ‘fit for work’. How many of the 150 prisoners lost their lives due to these experiments is not known. Von Weyhern never filed a final report. It is to be feared that the death toll was considerable. [1]
After the war, von Weyhern denied belonging to the SS, claimed that he had ‘sacrificed himself’ for his patients in the concentration camp, merely had to pay a fine, and was ‘denazified’ in 1948. Subsequently, he resumed his work as a ‘Heilpraktiker’ in Olching, a village near Dachau. [1]
Of course, these infamous experiments cannot be blamed on spagyric medicine. Yet, I feel they are nevertheless important, not least because they seem to reveal the only thing remotely resembling something like evidence.
[1] Die Ärzte der Nazi-Führer: Karrieren und Netzwerke : Mathias Schmidt (Hg.), Dominik Groß (Hg.), Jens Westemeier (Hg.): Amazon.de: Books