experience
Autogenic training (AT) is a relaxation technique that has garnered attention for its potential to reduce anxiety and improve psychological well-being. This review aimed to synthesize the findings from a diverse range of studies investigating the relationship between AT and anxiety disorder across different populations and settings.
A comprehensive review of 162 studies, including randomised controlled trials (RCTs), non-randomized controlled trials (N-RCTs), surveys, and meta-analysis, was conducted and 29 studies were selected. Participants in the studies were patients with:
- cancer,
- bulimia nervosa,
- stroke,
- coronary angioplasty,
Others were nursing students, healthy volunteers, athletes, etc.
Anxiety levels were measured before and after the AT intervention using a variety of anxiety assessment scales, including the State Trait Anxiety Inventory (STAI) and the Hospital Anxiety and Depression Scale (HADS). The formats, duration, and delivery of the interventions varied, with some studies utilising guided sessions by professionals and other self-administered practises.
The combined findings of these studies revealed consistent trends in the beneficial effects of AT on anxiety reduction. AT was found to be effective in reducing anxiety symptoms across a wide range of populations and settings. Following AT interventions, participants reported reduced anxiety, improved mood states, and improved coping mechanisms. AT was found to be superior to no treatment or a comparable intervention in a number of cases.
The authors conclused that the body of evidence supports autogenic training as a non-pharmacological approach to reducing anxiety and improving psychological well-being. Despite differences in methodology and participant profiles, the studies show that AT has a positive impact on a wide range of populations. The findings merit further investigation and highlight AT’s potential contribution to anxiety management strategies.
I was taught AT many years ago and have practised it occasionally ever since. I have also co-authored several papers of AT that showed encouraging results, e.g.:
- Autogenic training for tension type headaches: a systematic review of controlled trials. Complement Ther Med. 2006 Jun;14(2):144-50.
- Autogenic training for stress and anxiety: a systematic review. Complement Ther Med. 2000 Jun;8(2):106-10.
- Autogenic training to reduce anxiety in nursing students: randomized controlled trial. Kanji N, White A, Ernst E.J Adv Nurs. 2006 Mar;53(6):729-35.
- Autogenic training to manage symptomology in women with chest pain and normal coronary arteries. Menopause. 2009 Jan-Feb;16(1):60-5.
- Autogenic training reduces anxiety after coronary angioplasty: a randomized clinical trial. Am Heart J. 2004 Mar;147(3)
Thus, I feel that the conclusions of this review might be correct.
Several further recent papers seem to support the notion that AT is a treatment worth trying, e.g.:
- A review concluded that as an add-on intervention psychotherapy technique with beneficial outcome on psychophysiological functioning, AT represents a promising avenue towards expanding research findings of brain-body links beyond the current limits of the prevention and clinical management of number of mental disorders.
- A clinical trial showed that AT seems to improve sleep quality and could improve some dimensions of quality of life and other symptoms among people living with HIV. Further studies are needed to confirm these results.
Why then AT is not better studied and more popular? A short paragraph of my next book (to be published in about 6 months) on the inventors of so-called alternative medicines (SCAMs), including the German psychiatry professor Johannes Schulz (1884-1970), inventor of AT, might give you a clue:
Schultz supported the euthanasia program of the Nazis, i.e. the extermination of disabled and other people considered ‘unworthy of living’ during the Third Reich. He passed death sentences on “hysterical women” through his diagnoses. In 1933, Schultz began research on a guide-book on sexual education in which he focused on homosexuality and explored the topics of sterilization and euthanasia. In 1935, he published an essay about the psychological consequences of sterilization and castration among men; in it he supported compulsory sterilization of men in order to eliminate hereditary illnesses. With a diagnostic scheme developed by him in 1940, Schulz advocated the execution of mentally ill patients by stating: “I personally have to align myself with Mr. Hoche […], by recalling the ‘annihilation of life unworthy of life’ and by raising the hope that the madhouses will soon become emptied and remodelled according to this principle.” Schultz was fully aware of the consequences of his diagnostic assessment and even used the term “death sentence in the form of a diagnosis”.
I came across this evidence only years after having published my papers on AT. Would I have developed an interest in AT, if I had known about Schulz’s Nazi past? Probably not.
Robert Jütte, a German medical historian, has long been a defender of homeopathy and other forms of so-called alternative medicine (SCAM). His latest paper refers to the situation in Switzerland where the public was given the chance to vote for or against the reimbursement of several SCAMs, including homeopathy. I reported previously about this unusual situation, e.g.:
- More about homeopathy in Switzerland: “Globuli only cause unnecessary healthcare costs”
- More on the situation of homeopathy in Switzerland
- SCAM in Switzerland: paediatricians couldn’t care less
- It’s official: Switzerland is going holistically round the bend
Unsurprisingly, Prof Jütte’s views are quite different from mine. Here is the abstract of his recent paper:
Behind the principle of involving users and voters directly in decision-making about the health care system are ideas relating to empowerment. This implies a challenge to the traditional view that scientific knowledge is generally believed to be of higher value than tried and tested experience, as it is the case with CAM. The aim of this review is to show how a perspective of the history of medicine and science as well as direct democracy mechanisms such as stipulated in the Swiss constitution can be used to achieve the acceptance of CAM in a modern medical health care system. A public health care system financed by levies from the population should also reflect the widely documented desire in the population for medical pluralism (provided that therapeutical alternatives are not risky). Otherwise, the problem of social inequality arises because only people with a good financial background can afford this medicine.
I think that Jütte’s statement that “a public health care system financed by levies from the population should also reflect the widely documented desire in the population for medical pluralism provided that therapeutical alternatives are not risky. Otherwise, the problem of social inequality arises because only people with a good financial background can afford this medicine” is untenable. Here are my reasons:
- Lay people are not normally sufficiently informed to decide which treatments are effective and which are not. If we leave these decisions to the public, we will end up with all manner of nonsense diluting the effectiveness of our health services and wasting our scarce public funds.
- Jütte seems to assume that SCAMs that are not risky do no harm. He fails to consider that ineffective treatments inevitably do harm by not adequately treating symptoms and diseases. In serious conditions this will even hasten the death of patients!
- Jütte seems concerned about inequity, yet I think this concern is misplaced. Not paying from the public purse for nonsensical therapies is hardly a disadvantage. Arguably, those who cannot affort ineffective SCAMs are even likely to benefit in terms of their health.
I do realize that there might be conflicting ethical principles at play here. I am, however, convinced that the ethical concern of doing more good than harm to as many consumers as possible is best realized by implementing the principles of evidence-based medicine. Or – to put it bluntly – a healthcare system is not a supermarket where consumers can pick and chose any rubbish they fancy.
I wonder who you think is correct, Jütte or I?
Many people believe in and use so-called alternative medicine (SCAM) to address health issues or prevent diseases. Empirical evidence for those treatments is either lacking or controversial due to methodological weaknesses. Thus, practitioners and patients primarily rely on subjective references rather than credible empirical evidence from systematic research.
This study investigated whether cognitive and personality factors explain differences in belief in SCAM and homeopathy. The researchers, German psychologists, investigated the robustness of 21 predictors when examined together to obtain insights into key determinants of such beliefs in a sample of 599 participants (60% female, 18-81 years). A combination of predictors explained 20% of the variance in SCAM belief:
- ontological confusions,
- spiritual epistemology,
- agreeableness,
- death anxiety,
- gender.
Approximately 21% of the variance in belief in homeopathy was explained by the following predictors:
- ontological confusions,
- illusory pattern perception,
- need for cognitive closure,
- need for cognition,
- honesty-humility,
- death anxiety,
- gender,
- age.
The autors concluded that individuals believing in SCAM and homeopathy have cognitive biases and certain individual differences which make them perceive the world differently.
The authors argue that a key characteristic of many SCAM treatments is the spiritual orientation to knowledge and decision-making. For medical decisions, individuals who agree that important knowledge results from religious or spiritual experiences might not rely on evidence as a proof of efficiency but rather explain it in terms of personal experiences. One primary reason for the use of homeopathy is having had good experiences in the past. Own experiences have a high value and persuasive power but are meaningless from a scientific point of view.
Paranormal beliefs and SCAM belief do not only share ontological confusions as a predictor, paranormal beliefs are typically the best predictor of CAM belief. However, comparing those belief forms, it becomes clear that they share many concepts and approaches to explain reality in an unscientific way. Therefore, both belief forms, paranormal beliefs and SCAM beliefs, could also be seen as a result of a world view in which scientific evidence is valued less and, instead, emotional and spiritual explanations are consulted.
I think that anyone who has followed the discussions on this blog must agree wholeheartedly.
Charles III is about to pay his first visit to France, his second visit to any state. Earlier this year, he has already visited Germany. Originally, France had been first on his list but the event was cancelled in view of the violent protests that rocked the country at the time. Now he is definitely expected and the French are exited. I am currently in France and have been asked to give several interviews on the king’s love affair with so-called alternative medicine (SCAM).
The French have long been fascinated by our royal family which seems a bit odd considering what they did to their own. Now that Charles and Camilla are about to appear with an entourage of about 50 servants between them, the press is full with slightly bemused reports and comments:
Since childhood, Charles has been accustomed to a luxurious, gilded life, which is reproduced on every trip outside the royal palaces, to ensure maximum service, comfort and security… The new king always travels with his private secretary, Sir Clive Alderton, his press advisor, his steward, his doctor, his personal valets, his security guards, and his private chauffeur, Tim Williams… And, of course, his regular osteopath to relieve his lower back. Since he’s had a lot of falls playing polo, Charles regularly suffers from back pain…”.
Really, just an osteopath?
What about all the other SCAM-practitioners whose businesses Charles so regularly supported in the past:
- · Acupuncture
- · Aromatherapy
- · Ayurveda
- · Chiropractic
- · Detox
- · Gerson therapy
- · Herbal medicine
- · Homeopathy
- · Iridology
- · Marma massage
- · Massage therapy
- · Pulse diagnosis
- · Reflexology
- · Tongue diagnosis
- · Traditional Chinese Medicine
- · Yoga
Will they not be disappointed?
I do wonder who Charles’ osteopath and doctor are. Are they competent? I am sure they both must be well-informed and evidence-based experts. If that is the case, they will have, of course, told Charles that osteopathy is hardly an optimal solution for an injured back.
In any case, now I am concerned about the royal back and therefore urgently recommend that HIS MAJESTY reads some of my previous posts on the subject, e.g.:
- Manual therapy (mainly chiropractic and osteopathy) does not have clinically relevant effects on back pain compared with sham treatment
- Spinal manipulative therapy for older adults with chronic low back pain fails to generate convincing results
- NICE no longer recommends acupuncture, chiropractic or osteopathy for low back pain
- The Effects of Yoga, Naturopathy, and Conventional Medical Treatment in Managing Low Back Pain
- Chronic non-specific low back pain: comparing cognitive functional therapy and movement system impairment (MSI)-based treatment
- Cognitive functional therapy for chronic low back pain
- Meditation for Chronic Low Back Pain Management?
Let’s hope all goes well here in France, and please let’s not be so akward as to ask about the environmental aspects – we all know how worried Charles truly is about not just his health but also the health of the planet – of moving such an entourage for a two-day visit.
PS
Charles flew in a private jet from London to Paris and took his Bentley with him.
The objectives of this randomized double-blind placebo-controlled clinical trial were to determine if there:
- (a) is an overall effect of homeopathic treatment (homeopathic medicines plus consultation) in the treatment of ADHD;
- (b) are any specific effects the homeopathic consultation alone in the treatment of ADHD;
- (c) are any specific effects of homeopathic medicines in the treatment of ADHD.
Children aged 6–16 years diagnosed with ADHD were randomized to one of three arms:
- Arm 1 (Remedy and Consultation);
- Arm 2 (Placebo and Consultation);
- Arm 3 (Usual Care).
The primary outcome measure was the change of the Conner 3 Global Index-Parent T-score (CGI-P T score) between baseline and 28 weeks.
The results showed an improvement in ADHD symptoms as measured by the CGI-P T score in the two groups (Arms 1 and 2) that received consultations with a homeopathic practitioner when compared with the usual care control group (Arm 3). Parents of the children in the study who received homeopathic consultations (Arms 1 and 2) also reported greater coping efficacy compared with those receiving usual care (Arm 3). There was no difference in adverse events among the three study arms.
The authors concluded that, in this study, homeopathic consultations provided over 8 months with the use of homeopathic remedy was associated with a decrease in ADHD symptoms in children aging 6–16 years when compared with usual treatment alone. Children treated with homeopathic consultations and placebo experienced a similar decrease in ADHD symptoms; however, this finding did not reach statistical significance when correcting for multiple comparisons. Homeopathic remedies in and of themselves were not associated with any change in ADHD symptoms.
In the discussion section, the authors make their findings a little clearer: “The findings are generally consistent with a recent meta-analysis that concluded that (i)ndividualized homeopathy showed a clinically relevant and statistically robust effect in the treatment of ADHD. Similar to the meta-analysis, the authors found individualized homeopathy (consultation plus remedy) resulted in improvement in ADHD symptoms. However, the data suggest that this effect is not due to the remedy component of the intervention.”
The authors do not cite the (to the best of my knowledge) only study that had a very similar aim, namely differentiating between the effects of the homeopathic remedy and the homeopathic consultation. It was conducted by the late George Lweith who certainly was not against homeopathy. The conclusions of this trial were as follows: Homeopathic consultations but not homeopathic remedies are associated with clinically relevant benefits for patients with active but relatively stable rheumatoid arthritis.
Both trials confirm what rational thinkers have been saying for many years: the effects that many people experience after homeopathic therapy are not due to the homeopathic remedy but to the usually long and empathetic therapeutic encounter, the placebo effect, and other non-specific effects. To put it bluntly homeopathy is a kind of amateur psychotherapy.
Before someone now claims that this means homeopathy is fine, let me tell you this: no, it is not fine! If someone needs psychotherapy, he/she should see not an amateur but a professional, i.e. a psychologist who is properly trained in what she can and cannot do.
The KFF provides reliable, accurate, and non-partisan information to help inform health policy in the US. The KFF has just released its ‘Health Misinformation Tracking Poll Pilot‘ examining the public’s media use and trust in sources of health information and measuring the reach of specific false and inaccurate claims surrounding three health-related topics: COVID-19 and vaccines, reproductive health, and gun violence. It makes grimm reading indeed. Here are but a few excerpts pertaining to health/vaccination:
Health misinformation is widespread in the US with 96% of adults saying they have heard at least one of the ten items of health-related misinformation asked about in the survey. The most widespread misinformation items included in the survey were related to COVID-19 and vaccines, including that the COVID-19 vaccines have caused thousands of deaths in otherwise healthy people (65% say they have heard or read this) and that the MMR vaccines have been proven to cause autism in children (65%).
Regardless of whether they have heard or read specific items of misinformation, the survey also asked people whether they think each claim is definitely true, probably true, probably false, or definitely false. For most of the misinformation items included in the survey, between one-fifth and one-third of the public say they are “definitely” or “probably true.” The most frequently heard claims are related to COVID-19 and vaccines.
Uncertainty is high when it comes to health misinformation. While fewer than one in five adults say each of the misinformation claims examined in the survey are “definitely true,” larger shares are open to believing them, saying they are “probably true.” Many lean towards the correct answer but also express uncertainty, saying each claim is “probably false.” Fewer tend to be certain that each claim is false, with the exception of the claim that more people have died from the COVID-19 vaccines than from the virus itself, which nearly half the public (47%) recognizes as definitely false.
Across the five COVID-19 and vaccine related misinformation items, adults without a college degree are more likely than college graduates to say these claims are definitely or probably true. Notably, Black adults are at least ten percentage points more likely than White adults to believe some items of vaccine misinformation, including that the COVID-19 vaccines have caused thousands of sudden deaths in otherwise healthy people, and that the MMR vaccines have been proven to cause autism in children. Black (29%) and Hispanic (24%) adults are both more likely than White adults (17%) to say that the false claim that “more people have died from the COVID-19 vaccine than have died from the COVID-19 virus” is definitely or probably true. Those who identify as Republicans or lean towards the Republican Party and pure independents stand out as being more likely than Democratic leaning adults to say each of these items is probably or definitely true. Across community types, rural residents are more likely than their urban and suburban counterparts to say that some false claims related to COVID vaccines are probably or definitely true, including that the vaccines have been proven to cause infertility and that more people have died from the vaccine than from the virus.
Educational attainment appears to play a particularly important role when it comes to susceptibility to COVID-19 and vaccine misinformation. Six in ten adults with college degrees say none of the five false COVID-19 and vaccine claims are probably or definitely true, compared to less than four in ten adults without a degree. Concerningly, about one in five rural residents (19%), adults with a high school education or less (18%), Black adults (18%), Republicans (20%), and independents (18%) say four or five of the false COVID-19 and vaccine misinformation items included in the survey are probably or definitely true.
________________________________
If you have followed some of the comments on this blog, you might find it hard to be surprised!
I do encourage you to read the full article.
I don’t usually find reading medical papers scary. An article in the prestigious journal ‘Nature’ is the exception. Here is its abstract:
Long COVID is the patient-coined term for the disease entity whereby persistent symptoms ensue in a significant proportion of those who have had COVID-19, whether asymptomatic, mild or severe. Estimated numbers vary but the assumption is that, of all those who had COVID-19 globally, at least 10% have long COVID. The disease burden spans from mild symptoms to profound disability, the scale making this a huge, new health-care challenge. Long COVID will likely be stratified into several more or less discrete entities with potentially distinct pathogenic pathways. The evolving symptom list is extensive, multi-organ, multisystem and relapsing–remitting, including fatigue, breathlessness, neurocognitive effects and dysautonomia. A range of radiological abnormalities in the olfactory bulb, brain, heart, lung and other sites have been observed in individuals with long COVID. Some body sites indicate the presence of microclots; these and other blood markers of hypercoagulation implicate a likely role of endothelial activation and clotting abnormalities. Diverse auto-antibody (AAB) specificities have been found, as yet without a clear consensus or correlation with symptom clusters. There is support for a role of persistent SARS-CoV-2 reservoirs and/or an effect of Epstein–Barr virus reactivation, and evidence from immune subset changes for broad immune perturbation. Thus, the current picture is one of convergence towards a map of an immunopathogenic aetiology of long COVID, though as yet with insufficient data for a mechanistic synthesis or to fully inform therapeutic pathways.
The paper ends with this gloomy statement: “The oncoming burden of long COVID faced by patients, health-care providers, governments and economies is so large as to be unfathomable, which is possibly why minimal high-level planning is currently allocated to it. If 10% of acute infections lead to persistent symptoms, it could be predicted that ~400 million individuals globally are in need of support for long COVID. The biggest unknowns remain the joined-up scheme of its pathogenesis and thus the best candidate therapeutics to be trialled in randomized controlled trials, along with a better understanding of the kinetics of recovery and the factors influencing this. Some countries have invested in first-round funding for the pilot investigations. From the above, far more will be needed.”
In the context of this blog, we must, of course, ask: HAS SO-CALLED ALTERNATIVE MEDICINE (SCAM) SOMETHING TO OFFER?
I’m afraid that the short answer to this question is No!
However, one does not need to be a clairvoyant to predict that lots of therapeutic claims followed by plenty of methodologically weak (to put it politely) research will emerge from SCAM. Already some time ago, this homeopath indicated, that SCAM providers should see COVID as an opportunity: For homeopathy, shunned during its 200 years of existence by conventional medicine, this outbreak is a key opportunity to show potentially the contribution it can make in treating COVID-19 patients.
We should not hold our breath to see the emergence of convincing evidence, but we must be prepared to warn the public from getting exploited by charlatans.
This systematic review evaluated all available randomized controlled trials (RCTs) investigating the clinical effects of hydrotherapy according to Kneipp which is characterized by cold water applications. All RCTs on therapy and prevention with Kneipp hydrotherapy were included. Study participants were patients and healthy volunteers of all age groups. MEDLINE (via PubMed), Scopus, Central, CAMbase, and opengrey.eu were systematically searched through April 2021 without language restrictions and updated by searching PubMed until April 6th 2023. The risk of bias was assessed using the Cochrane tool version 1.
Twenty RCTs (N=4247) were included. Due to the high heterogeneity of the RCTs, no meta-analysis was performed. The risk of bias was rated as unclear in most of the domains. Of 132 comparisons, 46 showed significant positive effects in favor of hydrotherapy on chronic venous insufficiency, menopausal symptoms, fever, cognition, emotional function, and sickness absenteeism. However, 81 comparisons showed no differences between groups, and 5 were in favor of the respective control group. Only half of the studies reported safety issues.
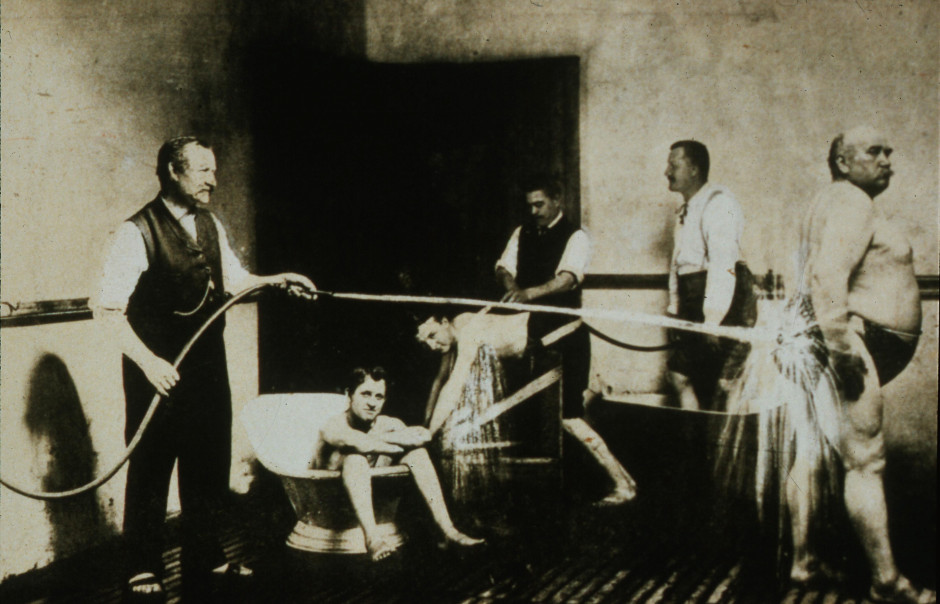
The authors concluded that although RCTs on Kneipp hydrotherapy seem to show positive effects in some conditions and outcomes, it remains difficult to ascertain treatment effects due to the high risk of bias and heterogeneity of most of the considered studies. Further high-quality RCTs on Kneipp hydrotherapy are urgently warranted.
This is certainly the best review of the subject so far. It makes it very clear that the evidence for Kneipp hydrotherapy is weak, mostly because of the many flaws in the primary studies. One needs to add, I think, that 20 RCTs are an absurdly small amount considering that many indications this type of therapy is advocated for – many enthusiasts even consider it a panacea.
It follows, I fear, that Kneipp hydrotherapy is almost entirely not evidence-based. This should be bad news for the numerous institutions and Spa towns (mostly in Germany) that live on employing this treatment and telling patients that it is effective. They usually claim that experience shows this to be true. But this was the mantra of medicine ~100 years ago. Since then, we have learned that experience is a very poor guide that regularly leads us up the garden path.
Kneippians will counter that clinical trials are difficult to conduct and expensive to finance. Both arguments are of course true but, considering that an entire industry lives on telling patients something that essentially amounts to a lie (i.e. the claim that it works), it surely is obligatory to overcome these obstacles.
Guest post by Norbert Aust, Udo Endruscheit, and Edzard Ernst
How do we know whether a treatment is reasonable or just some so-called alternative medicine (SCAM) that is at best useless? A simple answer is that the former is evidence-based, while the latter is not. But how can we tell the difference? High-quality studies, with independent replications or even a systematic review, are the sort of things we are usually looking for. But there is an underlying assumption, namely that, in science, bogus studies are prevented from polluting the scientific database or, if such trials have emerged, there are ways to identify and eliminate them.
And what if this assumption is wrong?
What if respectable universities and research organizations venture into the realm of pseudoscience either knowingly or because it had slipped their attention?
What if the editorial board of a top journal passes bogus studies to peer review?
What if such a paper is eventually reviewed by a proponent of the implausible therapy?
What if the readers of the article, once it is published, are too lethargic to object and do not write letters to the editor in protest?
And what if skeptics do formulate a protest but the journal editor refuses to publish it?
Well, if all the checks that should prevent faulty results from entering the scientific knowledge fail, we have fake evidence: a study that looks like sound science but that, in fact, is invalid. It is not hard to imagine what would happen if SCAM therapies are supported by seemingly respectable studies published in top journals. The fake evidence would accumulate as part of the body of evidence and eventually enter mainstream clinical practice, education, politics, etc., etc. Thus the reputation of bogus therapies would grow unjustifiably.
If you think this cannot happen, you are in the wrong. After the infamous study by Frass et al about homeopathy as an add-on treatment for lung cancer, another homeopathy paper was published in 2022 by Gaertner et al. in Pediatric Research (PR), a Medline-indexed journal with a two-year impact factor of 3.95 belonging to the nature-group of journals. According to this meta-analysis ‘individualized homeopathy showed a clinically relevant and statistically robust effect in the treatment of ADHD’. Shortly after the publication of this paper, we sent a letter to the editor to point out the shortcomings of this study. Here it is:
Sir,
with this letter we like to comment on the systematic review and meta-analysis on childhood ADHD by Gaertner et al. recently published in your journal.
First off, we are surprised, that your journal that is connected to nature does publish a paper on a treatment that has no a-priory probability at all and thus can only contain false positives if any. And this review is no exception as will be seen presently.
Our concerns are:
Out of the six studies included three were mere pilot trials (Fibert_2019, Jacobs_2005, Oberai_2013, ) which cannot provide any evidence for the shortcomings involved in pilots. Three of the six trials show severe issues in blinding (Fibert_2016, Fibert_2019, Oberai_2013), with two of them concerning both of the participants and the test personnel. This usually leads to massive bias in favour of the treatment [Zitat Cochrane Handbook].
Then we compared data from two trials with the data reported in the review and found some major misrepresentations:
(1) Jacobs et al. report an improvement in the T-score of their main outcome (CGI-P) of 4.1 for homeopathy and 9.1 for controls, that is placebo outperformed the homeopathic intervention. But the authors give an effect size of 0.272 in favour of homeopathy which is the opposite of the findings in the trial.
(2) Oberai et al. report effect sizes for their three main outcomes of 0.22, 0.59 and 0.54 (CPRS-R, CGISS, CGIIS repectively). There is no way that this yields a pooled effect size of 1.436 as given in the review.
We conclude that the positive result obtained by the authors is due to a combination of the inclusion of biased trials unsuitable to build evidence together with some major misreporting of study outcomes.
Our recommendation would be that the authors reconsider their review and improve their report. Maybe the editors would like to add a caution-notice to the paper – if not to withdraw it completely.
In June 2023, a full year after our submission, we were informed that Pediatric Research would not publish our criticism because the priority given to it was not sufficient to justify publication. But we were assured, that the journal would take the matter seriously, that they will investigate this matter and take appropriate editorial action. But as of today (End of June 2023) no expression of concern has been published.
Did the journal receive other comments or criticisms related to the paper in question? No, apparently there were none, at least none was published and the paper remains unchallenged to this day. This means that it might be taken for reliable evidence on the effectiveness of homeopathy and mislead patients, carers, practitioners, decision-makers, etc.
We feel this is unacceptable and therefore again wrote to the editors asking to reconsider their decision. Here is our letter:
Dear …
together with my co-authors we would like to comment your decision about our letter to the editor about an extremely faulty and misleading paper that may well create harm to patients. In fact we find it very hard to accept your decision not to publish our comment.
We understand that Pediatric Research is a high impact journal with a 2-year IF of nearly 4. Your journal is member of COPE and is indexed with quite a few first rank institutions. By all standards, any reader will be convinced that a paper published in Pediatric Research is based on solid research and the results are derived by rigorous methodology and are as reliable as can be. Especially if this paper remains unchallenged by any reader’s comments for a full year after publication. This is your responsibility to the scientific community. And to the children that might receive treatment based on knowledge spread through your journal.
How then can it be, that an article about homeopathy, a thoroughly implausible lore, in the treatment of ADHD is published in Pediatric Research, where the authors come to the conclusion “that individualized homeopathy showed a clinically relevant and statistically robust effect in the treatment of ADHD”?
In our comment we point out that the authors made a lot of errors – to say it mildly. They deny the doubtful quality of the studies they included in their meta-analysis, they did not stick to their own exclusion criteria, the data the authors report do not resemble the findings of the studies they were allegedly taken from, the one study setting the results is a mere pilot study.
The reason you give for our letter not being published is that it was not given enough priority to justify publication. We would like to know: Which issues can conceivably receive higher priority than the fact that a paper in your journal is downright wrong and misleading?
What do you need to deem a comment important? Up to now the paper is unchallenged by any reader’s comments, so apparently there was no other letter to the editor that might be given higher priority than ours.
We ask you to review your decision, or better still, consider a retraction of the paper altogether. If so, an expression of concern should be issued at once. After all, the COPE-guidelines for retraction state “clear evidence, that the findings are unreliable, either as a result of major error (…), or as a result of fabrication (…) or faslification (…)’ as a reason to consider retraction.
Otherwise the malpractice of homeopathy will have a first class evidence that will be helpful to promote homeopathy to parents and their children.
Watch this space!
This article by a Postgraduate Trainee (Dept. of Case Taking and Repertory, National Institute of Homoeopathy, Govt. of India) an Assistant Professor (Dept. of Surgery, National Institute of Homoeopathy Govt. of India) and another Assistant Professor (Dept. of Obstetrics & Gynaecology, Midnapore Homoeopathic Medical College & Hospital, Govt. of West Bengal) might not be available online (Clinical Medicine and Health Research Journal, Volume 03, Issue 03, May – June 2023 Page No. 444-446) but it is I think worth discussing. Here is its abstract:
Warts are one of the common dermatological disorders caused by human papilloma viruses encountered in our day to day life. These are cutaneous or mucosal infection needs proper care and treatment to prevent its transmission and complete healing. Although mostly warts are dealt with the therapeutic approach, i.e. on the basis of its peculiar type and location but it can even be successfully treated by constitutional approach. This article is regarding a case of warts treated successfully with Rhus Tox followed by Ferrum Met selected as the simillimum and proved its effectiveness in a short period of time.
As the abstract is not very informative, let me show you also some sections from the paper itself:
The patient presented with warts on right wrist for 1 year. There were plane warts at back of wrist, which was smooth, slightly elevated and skin coloured. There was no history of warts or other benign skin disease in the family. This case treated with individualized homoeopathic medicine showed complete resolution of the warts. There is no cure for wart in conventional medicine except removal of them with various methods. Although it does not rule out the chance of recurrence, later on may deep organic disease. That is why a substantial number of warts patients resort to Complementary and Alternative Medicine (CAM), especially homoeopathy.
In this case, Ferrum Metallicum 0/1 was selected as a ‘similimum’ based on totality of symptoms, repertorial analysis and consultation with Homoeopathic Materia Medica, which was given more priority in this case. After seeing improvement, succeeding potency was prescribed. After Ferrum Met 0/4 all her complaints including warts disappeared. Thus, the outcome of this case of Plane Warts of the lady shows the success of individualized homoeopathic medicine in treatment of wart.
Conclusion:
This case report suggests homoeopathic treatment as a promising complementary or alternative therapy and emphasizes the need of repertorisation in individualized homoeopathic prescription. This case shows a positive role of homoeopathic in treating Warts. However, this is a single case study and requires well designed studies which may be taken up for future scientific validation.
This case report reminded me of an exciting and quite lovely story: at Exeter, we once conducted a wart study. It was a placebo-controlled, double-blind trial where the verum group received distant healing and the controls nothing at all. After planning the study, I was no longer involved in its running. As I happened to have a wart at the time, I offered myself to my team as a patient. They checked me out and admitted me into the study. For the next weeks, I either received the distant healing energy or nothing; neither I nor my team knew which. My wart was photographed and measured regularly.
And then it happened: shortly after the treatment period was over, my wart had gone. Everyone was excited, especially the UK healing scene. But we had to wait until the trial was finished, the results were calculated, and the random code was opened. The result: no difference between verum and placebo! We concluded that distant healing from experienced healers had no effect on the number or size of patients’ warts.
And my own, very personal wart?
It had disappeared spontaneously – I had been in the control group!
I know Indian homeopaths have a thing about healing warts (we discussed this before) but I am afraid the conclusions of this new paper ought to be re-written:
This case report does not suggest that homeopathic treatment is a promising complementary or alternative therapy. It shows the natural history of the condition in the disappearance of warts.