experience
The ‘American Heart Association News’ recently reported the case of a 33-year-old woman who suffered a stroke after consulting a chiropractor. I take the liberty of reproducing sections of this article:
Kate Adamson liked exercising so much, her goal was to become a fitness trainer. She grew up in New Zealand playing golf and later, living in California, she worked out often while raising her two young daughters. Although she was healthy and ate well, she had occasional migraines. At age 33, they were getting worse and more frequent. One week, she had the worst headache of her life. It went on for days. She wasn’t sleeping well and got up early to take a shower. She felt a wave of dizziness. Her left side seemed to collapse. Adamson made her way down to the edge of the tub to rest. She was able to return to bed, where she woke up her husband, Steven Klugman. “I need help now,” she said.
Her next memory was seeing paramedics rushing into the house while her 3-year-old daughter, Stephanie, was in the arms of a neighbor. Rachel, her other daughter, then 18 months old, was still asleep. When she woke up in the hospital, Adamson found herself surrounded by doctors. Klugman was by her side. She could see them, hear them and understand them. But she could not move or react.
Doctors told Klugman that his wife had experienced a massive brain stem stroke. It was later thought to be related to neck manipulations she had received from a chiropractor for the migraines. The stroke resulted in what’s known as locked-in syndrome, a disorder of the nervous system. She was paralyzed except for the muscles that control eye movement. Adamson realized she could answer yes-or-no questions by blinking her eyes.
Klugman was told that Adamson had a very minimal chance of recovery. She was put on a ventilator to breathe, given nutrition through a feeding tube, and had to use a catheter. She learned to coordinate eye movements to an alphabet chart. This enabled her to make short sentences. “Am I going to die?” she asked one of her doctors. “No, we’re going to get you into rehab,” he said.
Adamson stayed in the ICU on life support for 70 days before being transferred to an acute rehabilitation facility. She could barely move a finger, but that small bit of progress gave her hope. In rehab, she slowly started to regain use of her right side; her left side remained paralyzed. Therapists taught her to swallow and to speak. She had to relearn to blow her nose, use the toilet and tie her shoes.
She was particularly fond of a social worker named Amy who would incorporate therapy exercises into visits with her children, such as bubble blowing to help her breathing. Amy, who Adamson became friends with, also helped the children adjust to seeing their mother in a wheelchair.
Adamson changed her dream job from fitness trainer to hospital social worker. She left rehab three and a half months later, still in a wheelchair but able to breathe, eat and use the toilet on her own. She continued outpatient rehab for another year. She assumed her left side would improve as her right side did. But it remained paralyzed. She would need to use a brace on her left leg to walk and couldn’t use her left arm and hand. Still, two years after the stroke, which happened in 1995, Adamson was able to drive with a few equipment modifications…
In 2018, Adamson reached another milestone. She graduated with a master’s degree in social work; she’d started college in 2011 at age 49. “It wasn’t easy going to school. I just had to take it a day at a time, a semester at a time,” she said. “The stroke has taught me I can walk through anything.” …
Now 60, she works with renal transplant and pulmonary patients, helping coordinate their services and care with the rest of the medical team at Vanderbilt University Medical Center. “Knowing that you’re making a difference in somebody’s life is very satisfying. It takes me back to when I was a patient – I’m always looking at how I would want to be treated,” she said. “I’ve really come full circle.”
Adamson has adapted to doing things one-handed in a two-handed world, such as cooking and tying her shoes. She also walks with a cane. To stay in shape, she works with a trainer doing functional exercises and strength training. She has a special glove that pulls her left hand into a fist, allowing her to use a rowing machine and stationary bike….
Adamson is especially determined when it comes to helping her patients. “I work really hard to be an example to them, to show that we are all capable of going through difficult life challenges while still maintaining a positive attitude and making a difference in the world.”
________________________
What can we learn from this story?
Mainly two things, in my view:
- We probably should avoid chiropractors and certainly not allow them to manipulate our necks. I know, chiros will say that the case proves nothing. I agree, it does not prove anything, but the mere suspicion that the lock-in syndrome was caused by a stroke that, in turn, was due to upper spinal manipulation plus the plethora of cases where causality is much clearer are, I think, enough to issue that caution.
- Having been in rehab medicine for much of my early career, I feel it is good to occasionally point out how important this sector often neglected part of healthcare can be. Rehab medicine has been a sensible form of multidisciplinary, integrative healthcare long before the enthusiasts of so-called alternative medicine jumped on the integrative bandwagon.
Serbian tennis player Novak Djokovic has made tennis history by winning a record 23rd Grand Slam tournament at the French Open in Paris. The controversial star is well-known for promoting wellness fads and pseudoscience and was spotted wearing a ‘nanotechnology patch’ throughout the tournament in Paris. Djokovic claimed that it was the “biggest secret of his career” and without the device, he would not have achieved what he has professionally.

What on earth is that? You may well ask.
Here is the answer to that question from the manufacturer of the device:
Taopatch uses nanotechnology material. Nanotechnology it is the study and application of exceedingly small things, in the range of 1 to 100 nanometers. It has become important in many fields: chemistry, biology, physics, engineering, medicine, and others. Taopatch® is a small disk, 1 cm in diameters and less than 1 mm thick, containing nanoparticles called “quantum dots” with a hypoallergenic coating. These quantum dots “pick up” infrared radiation from the body and emit another radiation in the range of visible light, like that used by the low-level and ultra-low-level laser therapy (Scoppa et al., 2016) plus far Infrared, near Infrared and nourishing UV light. These photons exert a favorable effect when applied to sensitive points of the human body (acupuncture points). These devices have been certified by an independent laboratory to be free of any substances having a pharmacological action that may be released and absorbed by subjects who place the devices on the skin.
SCIENTIFIC STUDIES AND BENEFITS
Balance, posture, movement, and sports
The upright posture marks a great achievement in its evolutionary path, allowing it to integrate itself more efficiently with the environment. Balance, movement efficiency, and muscle coordination are important for human activity. Electromagnetic fields interact with biological structures and may improve these functions of the organism, as is demonstrated in the following studies. The effect of the Taopatch® on the posture control of 45 healthy subjects and two multiple sclerosis patients was studied by Genua et al. (2015/2016). The purpose of posture is the maintenance of balance. Thus, 15 healthy subjects were given the Taopatch®, 15 a placebo, and 15 were control subjects. The researchers demonstrated an improvement of the relationship between balance and energy expenditure for the subjects using the device relative to placebo and control subjects. These results further suggested the application of nanotechnology devices to rehabilitation protocols and sports. This research is being continued on the use of the devices by multiple sclerosis patients.
A careful analysis of the effect of quantum dot devices (referred to as “H. I. T. postural devices”) was done by Di Summa et al., 2018. The devices were applied to 20 subjects with no equilibrium disorders. The subjects, aged between 25 and 35 years old, underwent standard stabilometric examinations (the study of body sway during quiet standing). The tests showed a statistically significant improvement in posture, meaning an increased accuracy for voluntary movements. The researchers concluded that the electromagnetic devices interact with the human electromagnetic fields, acting on the postural control system’s components.
Malchiodi Albedi et al. (2017) studied the effect of Taopatch® devices on the postural control of a set of 30 female, healthy subjects. As in the previously mentioned study, stabilometric tests were performed. Active patches were applied to 15 subjects, and sham patches to other 15 subjects in a double-blind protocol. The comparison of active patches vs. sham patches (placebos) showed an evident decrease in the sway path for the active patches, strong evidence of improved posture control.
Carbonari et al. (2020) evaluated the effect of occlusal splints and Taopatch® devices on athletes’ muscular performance, balance, and posture. A set of tests were completed: surface electromyography (sEMG), kinesiography, the squat jump and counter movement jump, and the handgrip test. The results demonstrated that the occlusal splint and Taopatch® applied alone or together immediately improved strength and balance.
Help for patients with multiple sclerosis
Lomeo et al. (2019) evaluated the use of nanotechnological devices for posture control, range of motion of the joints, and general well-being on patients affected by Multiple Sclerosis (MS). Two Taopatch® devices were applied to 28 patients. This research showed that this technology improves movement, proprioception, balance, and general well-being.
The protocols included the self-evaluation test SF-36 Health Survey (a questionnaire to indicate the health status), the international index EDSS (Expanded Disability Status Scale, a method of quantifying disability in multiple sclerosis and monitoring changes over time), and several accelerometer tests (lower limbs, lumbar flexion, and head movements).
The SF-36 and EDSS tests clearly indicated an improvement in the well-being of the patients. In particular, the SF-36 test demonstrated ameliorations in physical activity, pain, general health, vitality, social activities, emotional and mental health. The improvements were maintained after one year.
The accelerometer tests showed significant improvements in the left hip, right hip, and lumbar inflections. It is important to note that the improvements appear at three months and are also maintained after one year.
Help for dental care of handicapped subjects
Patients with motor, psychomotor, sensory, or intellectual handicaps may present problems for dental care administration. A group of seven patients with light-moderate handicaps (2 with autism, 2 unable to walk due to a stroke, 1 with Parkinson, 1 with Martin-Bell syndrome, 1 with 21 trisomy) were treated with and without the application of Taopatch® (Sedran et al., 2017). The device permitted better management of the procedure, with less fatigue for the patients and more comfort for the operator.
Improvement of antioxidative defense of cells and cell proliferation in biological models
Reactive oxygen species (ROS) are significant environmental contaminants. At high ROS concentrations, damage to cellular components occurs, such as proteins, lipids, and nucleic acids. The activity of patches containing nanocrystals in the presence of ROS was studied for two biological models, Saccaromyces cerevisiae colonies and Pisum sativum plants. (Benedetti et al., 2018). The patches were exposed to the radiation of specific routers. The treated colonies showed an active defense against reactive oxygen species, and the plant cells increased proliferation. Thus, the results reported in this research suggest extending the application of this technology to fight the effects of various contaminants and reducing the use `of biological and chemical materials for environmental defense.
REFERENCES
Benedetti, S., Degrassi C., De Martino A., Beninati S., Cappello F., Bonivento P. (2018). Improvement of Antioxidative Defense of Cells Exposed to Radio Frequencies by a Nanotechnology Device. Journal of Biomaterials, 2(1), 20-23. doi:10.11648/j.jb.20180201.15
Carbonari, B., Balducci, F., Cesaretti, G., Cesanelli, L., Botticelli, D., Messina, G. (2020). Performance, balance and posture variations with Occlusal Splint and Taopatch® devices. A retrospettive cross-over study. J Sports Med Phys Fitness, epub Jul. 30. doi: 10.23736/S0022-4707.20.11053-3.
Di Summa, F., Capobianco, F.S., Shevchenko, A., De Martino, A., Beninati, S., Baldoni, E., Lumbau, A.M.I., Chessa, G.I. (2018). Improvement of Postural Reprogramming by a Nanotechnology Device. International Journal of Biomedical Materials Research. 6(3), 57-61. doi: 10.11648/j.ijbmr.20180603.11.
Genua, D., Bruno, F., Caldarera, G., Nanotecnologie e Postura. Master’s Thesis. (Italian). UNIVERSITÀ DEGLI STUDI DI PALERMO, SCUOLA DELLE SCIENZE UMANE E DEL PATRIMONIO CULTURALE, MASTER IN POSTUROLOGIA E BIOMECCANICA (2015/2016).
Lomeo, A., Cacciaguerra, C., Garsia, D., Scolaro, A. (2019). The use of nanotechnological devices in degenerative cerebral pathologies: Perspective study on 28 patients with multiple sclerosis (French). Hegel, 9(2), 114-121.
Malchiodi Albedi, G., 1, Corna, S., Aspesi, A., Clerici, D., Parisio, C., Seitanidis, J., Cau, N., Brugliera, L., Capodaglio, P. (2017). Effects of nanotechnology-based devices on postural control in healthy subjects. J Sports Med Phys Fitness, epub Sep 5. Doi: 10.23736/S0022-4707.17.07530-2.
Scoppa, F., Gallamini, M., Belloni, G. (2016). Treating Balance Disorders with Ulllt Acupuncture Stimulation: A Further Pilot Study on Normal Subjects Confirms Clinical Applicability of Treatment. J Nov Physiother, 6(285). doi:10.4172/2165-7025.1000285.
Sedran, A., Rizzi R., Sindici, E., Sedran, A. Use of TAOPATCH nanotechnology for dental care on HCP subjects (2017). SIOH Meeting, Milan, 5-6-7 October. University of Turing, Department of Surgical Sciences, Dental School.
__________________________
Convinced?
Me neither!
What Novak Djokovic has yet again demonstrated, in my view, is the fact that expectation can influence physical outcomes (and that you don’t need many critical thinking skills to become a tennis star).
The General Chiropractic Council (GCC) “regulates chiropractors in the UK to ensure the safety of patients undergoing chiropractic treatment”. One might have assumed that they thus fulfill the important role of controlling the profession. Yet, one would have assumed wrongly. Instead of controlling, the GCC usually prefers promoting the profession. Their recent Chiropractic Patient Satisfaction and Experience is a good example. Let me show you several important sections of this document:
The outcomes reported here highlight two key findings:
• Overwhelmingly, chiropractic patients report high levels of satisfaction and positive experiences with their care. This was true both in the literature that examined international patient cohorts as well as the specific data collected from UK based chiropractic patients.
• A strong therapeutic relationship and good communication between patient and chiropractor underpins high satisfaction scores and a positive experience. This was confirmed both in the international literature and through both quantitative and qualitative analysis of specific data collected from UK based chiropractic patients.
Conclusion
This report shows that both existing literature and de novo data collection from patients receiving chiropractic care in the UK highlight excellent perceived experience and high satisfaction with such care.
Factors such as therapeutic alliance and communication are strongly associated with these positive perceptions by patients although other factors such as treatment beliefs were also significantly associated with satisfaction scores.
Recommendations
• To offer the highest quality of care, both in terms of clinical outcomes and patient experience, chiropractors should be explicitly skilled at curating excellent therapeutic alliances and communication with patients.
• Such skills and competences within chiropractic care delivery should receive higher visibility within the chiropractic profession generally and more specifically through advocacy within leading institutions and core emphasis within chiropractic curricula.
__________________________
By changing a few words, I have adapted the above excerpts to become a Customer Satisfaction and Experience Report of a fictitious hamburger joint published by the Hamburger General Council (HGC) of Great Britain which regulates hamburger joints in the UK to ensure the safety of consumers undergoing hamburger nutrition:
The outcomes reported here highlight two key findings:
• Overwhelmingly, customers report high levels of satisfaction and positive experiences with their restaurant. This was true both in the literature that examined international consumer cohorts as well as the specific data collected from UK based customers.
• A strong professional relationship and good communication between customer and service personell underpins high satisfaction scores and a positive experience. This was confirmed both in the international literature and through both quantitative and qualitative analysis of specific data collected from UK based hamburger consumers.
Conclusion
This report shows that both existing literature and de novo data collection from consumers eating hamburgers in the UK highlight excellent perceived experience and high satisfaction with such service.
Factors such as personal alliance and communication are strongly associated with these positive perceptions by consumers although other factors such as appetite were also significantly associated with satisfaction scores.
Recommendations
• To offer the highest quality of service, both in terms of profit and patient experience, hamburger vendors should be explicitly skilled at curating excellent professional alliances and communication with customers.
• Such skills and competences within hamburger delivery should receive higher visibility within the gastronomic trade generally and more specifically through advocacy within leading institutions and core emphasis within servers’ curricula.
___________________________
If you get the impression that I am taking the Mickey of the GCC, you are not mistaken. Yet, this post also has slightly more serious purposes. I wanted to 1) show how, in the chiropractic profession, pure BS is often disguised as research, and 2) question whether the GCC is fit for purpose.
On a more constructive note: there are many open questions that urgently need addressing in the realm of chiropractic (e.g. do chiropractors more good than harm?). I, therefore, suggest that the GCC stops publishing idiotic promotional documents disguised as research and gets on with its responsibilities.
It has recently been reported that a 39-year-old woman (a mother-of-three died) died after immersing herself in a river as part of a cold water therapy session. The woman died after paramedics were called to attend a riverside in Derbyshire. The session was run by Kevin O’Neill of ‘Breatheolution’, whose previous clients include Coleen Rooney and actor Stephen Graham. The woman, who was visiting with two friends after paying up to £200 for a two-hour cold water therapy session, was rushed to hospital where she died.

Mr. O’Neill commented: “I am heartbroken. I’ve not slept and I’m finding it hard to process. I cannot stop thinking about her family. It’s tragic.” An inquest is expected to be opened into the woman’s death. East Midlands Ambulance Service said they were called to Bankside, in Bridgemont. “The caller reported a medical emergency,” a spokesperson said. “We sent a paramedic in a fast response car and a double-crewed ambulance. The air ambulance was also in attendance.”
Derbyshire Fire and Rescue Service, which was called to assist the paramedics, has warned people about the dangers of entering open water. “While we cannot and will not comment or speculate on the circumstances and cause of this tragic death, we would like to remind people of the dangers of entering open water and cold water shock,” said group manager Lee Williams.
_____________________
Breatheolution’ has a website where a whole page is dedicated to its leader Kevin O’Neill. I wondered what qualifications Kevin has, but all it tells us about him is this: “I struggled for so long with alcohol and other substance abuse that something had to give, I lost my sister Yvonne in 2019 and I think it was enough trauma to make me think a lot more about my own life”
The website also explains what the cold water sessions are about:
1-2-1 Breath Coaching, practice & Cold water session (river or tank)
2 hours @ £110.00
These sessions are proving popular with those who are not keen on group sessions or just prefer to have a more personal experience. The 2-3 hour sessions will be tailored to you and your breathing and will include potentially life-changing tools and methods to allow you to witness your breathing and physiology differently in the future, its all about feeling and awareness.
Another section of the site is dedicated to celebrities who Kevin seems to have treated. And then there is a video of the treatment. What I did not find anywhere, however, are the conditions that Kevin claims to treat with his cold water therapy.
In any case, it would have been wise for Kevin to read up about the risks of cold water immersion (CWI) before going into business. Perhaps this review would have helped:
In 2012, an estimated 372,000 people (42 per hour) died from immersion, assumed to be drowning. Immersion is the third leading cause of unintentional injury-related death, accounting for 7% of all such deaths (World Health Organization, 2014). These figures are underestimations owing to poor reporting in many Third World countries that have a high number of deaths. The data also do not include life-long morbidity caused by immersion-related injuries, estimated to be a much bigger numerical problem.
There is no strict definition of ‘cold water’. Given that some of the hazardous responses to cold water appear to peak on immersion somewhere between 15 and 10°C, it is reasonable to say that cold water is water <15°C (Tipton et al. 1991). However, the thermoneutral water temperature for a resting naked individual is ∼35°C, so it is possible for individuals to become very cold, with time, on immersion in water below this temperature. The corresponding temperature for those exercising (including shivering) is ∼25°C (Tipton & Golden, 1998).
Historically, the threat associated with CWI was regarded in terms of hypothermia or a reduction in deep body temperature below 35°C. This belief was established as a result of the Titanic disaster and supported by data obtained during maritime conflicts of World War II. However, more recently, a significant body of statistical, anecdotal and experimental evidence has pointed towards other causes of death on immersion. For example, in 1977 a Home Office Report revealed that ∼55% of the annual open water deaths in the UK occurred within 3 m of a safe refuge (42% within 2 m), and two-thirds of those who died were regarded as ‘good swimmers’. This evidence suggests more rapid incapacitation than can occur with whole-body cooling and consequent hypothermia.
The following four stages of immersion have been associated with particular risks (Golden & Hervey, 1981; Golden et al. 1991); the duration of these stages and the magnitude of the responses evoked within them vary significantly, depending on several factors, not least of which is water temperature:
- Initial immersion (first 3 min), skin cooling;
- Short-term immersion (3 min plus), superficial neuromuscular cooling;
- Long-term immersion (30 min plus), deep tissue cooling (hypothermia); and
- Circum-rescue collapse: immediately before, during or soon after rescue.
As a result of laboratory-based research, the initial responses to immersion, or ‘cold shock’, were identified as particularly hazardous (Tipton, 1989), accounting for the majority of immersion deaths (Tipton et al. 2014). These deaths have most often been ascribed to drowning, with the physiological responses of a gasp and uncontrollable hyperventilation, initiated by the dynamic response of the cutaneous cold receptors, resulting in the aspiration of the small volume of water necessary to initiate the drowning process (Bierens et al. 2016). Relatively little is known about the minimal rates of change of cold receptor temperature necessary to cause cold shock. The response has been reported to begin in water as warm as 25°C but is easy to suppress consciously at that temperature. In laboratory conditions, the respiratory frequency response (an indication of respiratory drive) peaks on naked immersion in a water temperature between 15 and 10°C, and is no greater on immersion in water at 5°C (Tipton et al. 1991). The corresponding average rates of change of chest skin temperature over the first 20 s of these immersions was 0.42 (water temperature 15°C), 0.56 (water temperature 10°C) and 0.68°C s−1 (water temperature 5°C). This suggests that an average rate of change in chest skin temperature between 0.42 and 0.56°C s−1 on the first 20 s of immersion is sufficient to evoke a maximal respiratory cold shock response.
More recently, it has been suggested (Shattock & Tipton, 2012) that a larger number of deaths than once thought may be attributable to arrhythmias initiated on immersion by the coincidental activation of the sympathetic and parasympathetic division of the autonomic nervous system by stimulation of cutaneous cold receptors around the body [sympathetic activation (cold shock)] and in the oronasal region on submersion or with wave splash [vagal stimulation (diving response)]. This ‘autonomic conflict’ is a very effective way of producing dysrhythmias and arrhythmias even in otherwise young and healthy individuals, particularly, but not necessarily, if a prolonged breath hold is involved in the immersion (Tipton et al. 1994). It seems that predisposing factors, such as long QT syndrome, ischaemic heart disease or myocardial hypertrophy, are necessary for fatal arrhythmias to evolve (Shattock & Tipton, 2012); many of these factors, including drug-induced long QT syndrome, are acquired. Non-fatal arrhythmias could still indirectly lead to death if they cause incapacitation and thereby drowning (Tipton, 2013). The hazardous responses associated with the cold shock response are presented in Fig. 2.
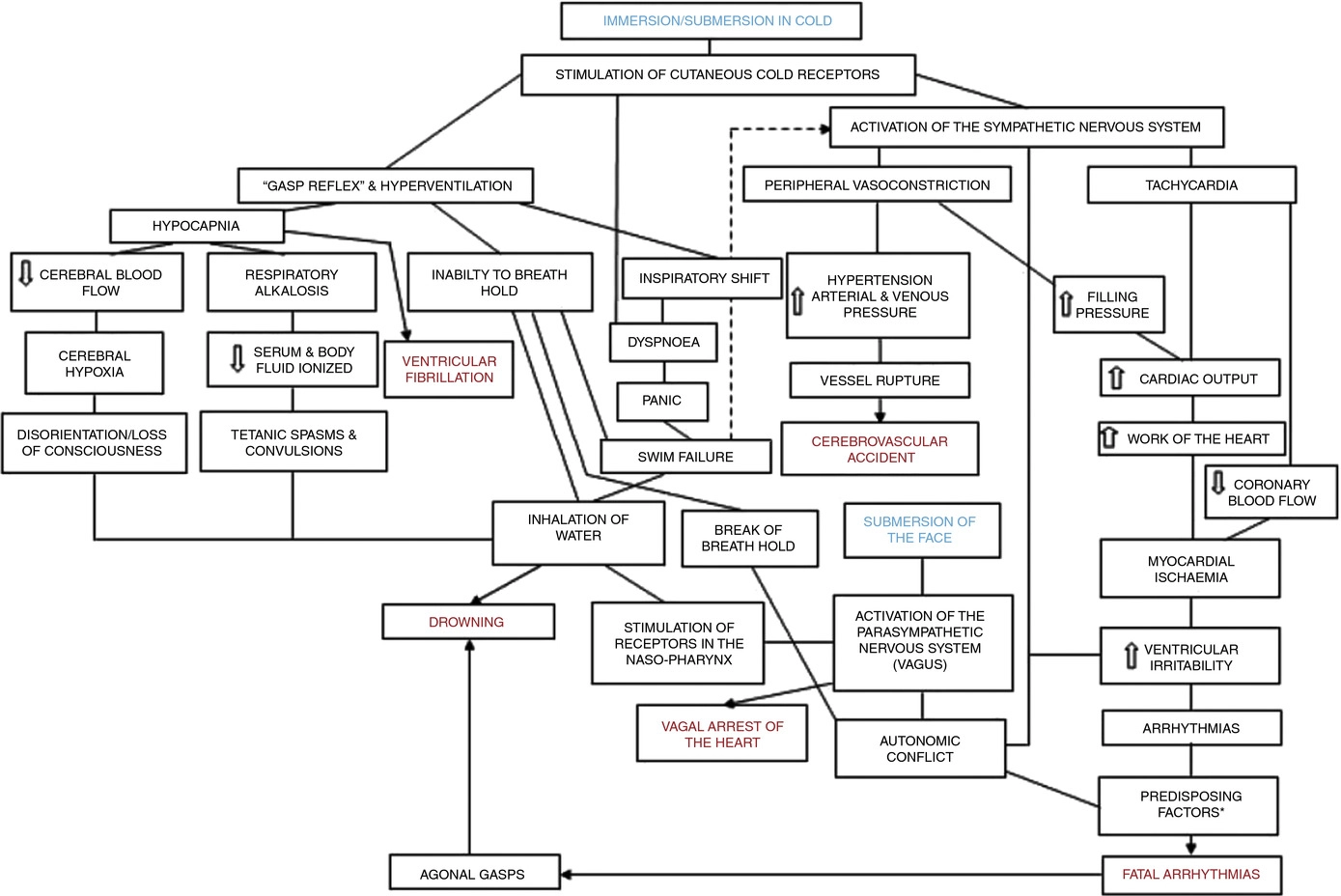
Figure 2. A contemporary view of the initial responses to immersion and submersion in cold water (‘cold shock’)
The problems encountered in short-term immersions are primarily related to physical incapacitation caused by neuromuscular cooling (Castellani & Tipton, 2015). The arms are particularly susceptible because of their high surface area to mass ratio. Low muscle temperatures affect chemical and physical processes at the cellular level. This includes metabolic rate, enzymatic activity, calcium and acetylcholine release and diffusion rate, as well as the series elastic components of connective tissues (Vincent & Tipton, 1988). Maximal dynamic strength, power output, jumping and sprinting performance are related to muscle temperature, with reductions ranging from 4 to 6% per degree Celsius reduction in muscle temperature down to 30°C (Bergh & Ekblom, 1979). At nerve temperatures below ∼20°C, nerve conduction is slowed and action potential amplitude is decreased (Douglas & Malcolm, 1955). Nerve block may occur after exposure to a local temperature of between 5 and 15°C for 1–15 min. This can lead to dysfunction that is equivalent to peripheral paralysis and can, again, result in drowning owing to the inability to keep the airway clear of the water (Clarke et al. 1958; Basbaum, 1973; Golden & Tipton, 2002; Fig. 3).

Figure 3. The ‘physiological pathways to drowning’ after immersion or submersion in cold water, with possible interventions for partial mitigation (dashed)
Abbreviations: EBA, emergency breathing aid; IS, immersion suit; and LJ, lifejacket. Reproduced with permission, from Tipton (2016b).
Even in ice-cold water, the possibility of hypothermia does not arise for at least 30 min in adults. Hypothermia affects cellular metabolism, blood flow and neural function. In severe hypothermia, the patient will be deeply unconscious. The progressive signs and symptoms (approximate deep body temperature) are shivering (36°C), confusion, disorientation, introversion (35°C), amnesia (34°C), cardiac arrhythmias (33°C), clouding of consciousness (33–30°C), loss of consciousness (30°C), ventricular fibrillation (28°C) and death (25°C) (Bierens et al. 2016). There is great variability between deep body temperature and the signs and symptoms of hypothermia. For example, although the deep body temperature associated with death is often quoted as 25°C, the lowest temperature recorded to date after accidental exposure to cold (air) and with full recovery was 12.7°C in a 28-month-old child (Associated Press, 2014). The coldest adult survivor of CWI followed by submersion had a body temperature of 13.7°C (Gilbert et al. 2000). There is also a large amount of variation in the rate at which people cool on immersion in cold water, owing to a combination of thermal factors (including water temperature and water movement, internal and external insulation) and non-thermal factors (including body size and composition, blood glucose, motion illness, racial and sex differences; Haight & Keatinge, 1973; Gale et al. 1981; White et al. 1992; Mekjavic et al. 2001; Golden & Tipton, 2002).
The most significant practical consequence of hypothermia in water is loss of consciousness; this prevents individuals from undertaking physical activity to maintain a clear airway and avoid drowning. Thus, once again, drowning is often the end-point (Fig. 3).
About 17% of those who die as a result of immersion die immediately before, during or after rescue (Golden et al. 1991). The deaths immediately before rescue are intriguing and probably related to behavioural changes at this time or the relief and psychophysiological alterations associated with imminent rescue, including a reduction in circulating stress hormone concentration and an increase in vagal tone. Death during rescue is most commonly associated with a collapse in arterial pressure when lifted vertical from the water and kept in that position for some time (Golden et al. 1991).
_____________________________
The tragic death of the woman should perhaps remind us that
- there is no SCAM or wellness treatment that is entirely harmless,
- and there are only few ‘would-be gurus’ who know what they are doing.
A ‘manifesto’ is not something that I come across often in my area of research, i.e. so-called alternative medicine (SCAM). This one is in German, I, therefore, translated it for you:
Manifesto for healthy medicine
With the Manifesto for healthy medicine, we, the citizens and patients alliance weil’s hilft! (‘BECAUSE IT HELPS’) demand a fundamental change in our healthcare system, towards a diverse medicine that focuses on people and health. Be part of it! Sign the manifesto and become part of the movement.
It’s of paramount importance, the Manifesto for healthy medicine. About the way we live. It’s about our health. It’s about you and it’s about me.
We want our healthcare system to actually focus on health.
We want a medicine that doesn’t ask what’s missing, but what is possible.
We want a medicine that cares about people, that takes care, gets to the bottom of things, and uses innovative technologies to do so.
We want more bio, so that the chemistry is right, and we want naturopathic procedures and naturally effective medicines to be recognized, promoted, and researched further.
We want research that creates knowledge because, in addition to studies, it also takes into account the experience of physicians and the needs of patients.
We want carers and doctors to be able to work in a way that is good for their patients and for themselves.
We want people from all healthcare professions to work together as equals.
We want a medicine that creates awareness for a good and healthy life because climate protection also begins in one’s own body.
We want an integrative medicine that puts people at the center and self-evidently combines conventional and natural healing methods.
And we want this medicine to be accessible and affordable for everyone.
We fight for a healthy medicine of the future.
Be part of it!
(sorry, if some of it might sound badly translated but the German original is in parts pure gibberish)
_____________________
Who writes such tosh composed of every thinkable platitude and then pompously calls it a MANIFESTO?
BECAUSE IT HELPS! (weil’s hilft!) is a citizens’ movement that demands a change in the health care system – towards the needs and preferences of patients, towards a holistic view of people, and a focus on health instead of disease. The sensible combination of natural medicine and conventional medicine, an integrative medicine, makes an indispensable contribution to this. This is because it relies fully on the patients and involves them as active partners in the treatment. Modern medicine of the future, therefore, needs the equal cooperation of natural medicine and conventional medicine – in the everyday life of physicians and patients, in the reimbursement by the health insurance companies as well as in research and teaching.
On the information platform www.weils-hilft.de weil’s hilft! informs about current developments in integrative medicine, provides background information, and publishes a podcast once a month. The movement is also active on social media at www.facebook.com/weilshilft and www.instagram.com/weilshilft.
weil’s hilft! is supported by the health and patient organizations GESUNDHEIT AKTIV, KNEIPP-BUND, and NATUR UND MEDIZIN. Together, the alliance represents the interests of more than 220,000 people.
_______________________
One could easily disclose the funny side of this, the utter stupidity of the arguments, the platitudes, fallacies, misunderstandings, ignorance, etc. Yes, that would hardly be difficult. But it would ignore how worrying this and similar movements are. They systematically misinform consumers with the sole aim of persuading them that the integration of unproven or disproven treatments into medical routine is in their interest. Yet, if we only scratch the surface of their arguments, we realize that it is exclusively in the interest of those who profit from this type of misinformation.
It is not only practitioners of so-called alternative medicine (SCAM) who can be fraudulent charlatans. The study of medicine does not protect you from joining in. Here is an impressive case in point:
It has been reported that a former doctor convicted of fraudulently submitting nearly $120 million in claims related to the 1-800-GET-THIN Lap-Band surgery business has been sentenced to seven years in federal prison.
Julian Omidi, 58, of West Hollywood was sentenced Monday by U.S. District Court Judge Dolly M. Gee. The judge also imposed a five-year probation period on Surgery Center Management LLC, an Omidi-controlled Beverly Hills-based company. In the coming weeks, Gee is expected to hold a separate hearing to decide on restitution and forfeiture in the case, along with setting a fine for the Beverly Hills company.
“Mr. Omidi made millions at the expense of the multiple victim companies he defrauded, and he violated his oath to ‘do no harm’ by callously misleading patients about the need for a sleep study and subsequent weight loss surgery,” said Donald Alway, the assistant director in charge of the FBI’s Los Angeles field office.
Omidi controlled several entities in the GET-THIN network. Prosecutors say Omidi incentivized employees to ensure patients underwent sleep studies and then falsified the results to show that patients had obstructive sleep apnea to help them qualify for insurance coverage for the weight loss surgery. Those results were then filed with insurance companies to pre-approve the Lap-Band weight-loss surgeries. The 1-800-GET-THIN business received approximately $41 million for those procedures, according to prosecutors. While not all patients were approved to receive the surgery, prosecutors say GET-THIN would bill the patient roughly $15,000 for each sleep study, totaling $27 million in payments from insurance providers.
Omidi and his Beverly Hills-based company, Surgery Center Management, were found guilty of 28 counts of wire fraud, three counts of mail fraud, and one count of conspiracy to commit money laundering. Omidi was also found guilty of two counts of making false statements relating to healthcare matters, one count of aggravated identity theft, and two counts of money laundering after a 48-day trial in downtown Los Angeles.
“As found by the jury, the defendant Julian Omidi deliberately and repeatedly acted with an eye towards business and profits, rather than in the interest of GET-THIN’s medical patients, by inducing patients to undergo medical treatment premised on fraud rather than medical necessity, including surgeries that carry significant risks and life-long health impacts,” said U.S. Atty. Martin Estrada. A series of Los Angeles Times columns from 2010 to 2014 detailed how five patients died after they received Lap-Band surgeries at clinics affiliated with 1-800-GET-THIN. During a 2009 inspection, the Department of Health and Human Services found unsanitary conditions, inoperative scrub sinks, one-time-only equipment being reused, and several other deficiencies. The inspector shut down the clinic for a day, but further action was not taken at the time.
Omidi’s medical license was revoked in 2009, and he was arrested. In 2014, federal agencies seized more than $110 million from the 1-800-GET-THIN network in securities and funds.
______________________________
This is a spectacular case, of course. Yet, I fail to see how it differs in principle from the many instances we see on a daily basis in the realm of SCAM. Let me give you just a few examples:
- A chiropractor diagnoses subluxation and subsequently treats his patient with a series of spinal manipulations.
- A naturopath uses iridology to diagnose a weakness of the liver and subsequently treats it with herbal remedies.
- An acupuncturist diagnoses a blockage of chi and follows it up with a series of acupuncture sessions.
- A Heilpraktiker employs bioresonance to diagnose an intoxication which he then treats with a detox program.
The strategy is always the same:
- Charlatans use bogus diagnostic methods.
- They make bogus diagnoses with them.
- They then start expensive and often dangerous treatments.
- They make good money by defrauding the system.
Could someone please explain what the difference in principle is between the case of the fraudulent surgeon and the average SCAM practitioner?
Imagine you have caught a cold. You think it is not necessary to see a doctor, but you want to take something that helps your body to get better. What is your choice of remedy? There are many options provided by conventional medicine as well as by so-called alternative medicine (SCAM).
Many people opt for SCAM to address health issues or prevent diseases. Yet, the evidence for SCAMs is either lacking or controversial due to methodological weaknesses. Thus, practitioners and patients primarily rely on subjective references rather than credible evidence from systematic research.
This study investigated whether cognitive and personality factors explain the differences in belief in SCAM and homeopathy. The researchers investigated the robustness of 21 predictors when examined together to obtain insights into some key determinants of such beliefs in a sample of 599 participants (60% female, 18-81 years). A combination of predictors explained 20% of the variance in SCAM belief. These predictors were:
- ontological confusions,
- spiritual epistemology,
- agreeableness,
- death anxiety,
- gender.
Approximately 21% of the variance in belief in homeopathy was explained by the following predictors:
- ontological confusions,
- illusory pattern perception,
- need for cognitive closure,
- need for cognition,
- honesty-humility,
- death anxiety,
- gender,
- age.
The authors concluded that some of the predictors from previous research replicated whereas others did not. Demographics and certain cognitive variables seem to be key determinants associated with beliefs in SCAM and homeopathy. Those individual differences and cognitive biases might result in a different perception of the world. However, variables related to abilities did not predict the beliefs. Thus, they might not be a result of inability but rather of ignorance.
Previous studies have shown that SCAM believers tend to believe in paranormal phenomena and conspiracies. I think that, in the discussion sections of this blog, we have ample evidence for this to be true. Paranormal beliefs are usually built on a magical worldview without reasoned review, which is shared by SCAM proponents. Such beliefs advocate emotional criteria for truth instead of data and logical considerations. Another belief, namely spirituality, is closely related to paranormal beliefs and religiosity and also associated with being a SCAM user. Lindeman found that SCAM belief could be best explained by intuitive reasoning, paranormal beliefs, and ontological confusions, defined as category mistakes in which properties of living and lifeless entities are mixed.
The authors point out that their results do not replicate previous findings that showed predictive value of certain cognitive variables such as cognitive style. An explanation could be that rather inattention to accuracy than the inability to consider empirical evidence fosters the beliefs. People might simply not be aware of the absence of evidence. Another possibility is that people are aware of the absence of evidence but are reluctant to engage with it. Practitioners and patients often claim “whatever works is good” or “the main thing is that it works”. Thus, it is ignorance rather than a lack of capacity to appropriately process the evidence.
The authors of this study are well aware of the limitations of their research:
“As with most cross-sectional studies using questionnaires, our results are based on self-reports. Additionally, single items were used for measuring belief strength. Even if multi-item measures often have advantages, single items can be advantageous in terms of practical benefits, e.g., adapting to subjects’ limited attention and time resources. There are several single item measures successfully used to measure diverse concepts including attitudes. Also, the variance on those items in our sample shows that participants were able to reflect their beliefs and rank them on the scale provided. Another limitation is that the findings are based on regression analyses, which do not provide insight into causality. Thus, the relationship remains correlational. Even if our sample was broader than in many other psychological studies—it was slightly unbalanced, especially in comparison to the German population. It over-represented educated individuals which may lead to an inadequate variation of the cognitive variables if we consider the relationship between cognition and education. However, education and the cognitive variables are only weakly correlated. Thus, it can be assumed that the unbalanced sample did not affect the distribution of cognitive variables to a great extent.”
I came across an article entitled “Consent for Paediatric Chiropractic Treatment (Ages 0-16)“. Naturally, it interested me. Here is the full paper; I have only inserted a few numbers in square brackets which refer to my comments below:
By law, all Chiropractors are required to inform you of the risks and benefits of chiropractic spinal manipulation and the other types of care we provide. Chiropractors use manual therapy alongside taking a thorough history, and doing a neurological, orthopaedic and chiropractic examination to both diagnose and to treat spinal, cranial and extremity dysfunction. This may include taking joints to the end range of function, palpating soft tissues (including inside the mouth and the abdomen), mobilisation, soft tissue therapy and very gentle manipulation [1]. Our Chiropractors have been educated to perform highly specific types of bony or soft tissue manipulation and we strive to follow a system of evidence-based care [2]. At the core of our belief system is “Do No Harm”. We recognise that infants and children are not tiny adults. The force of an adjustment used in a child is at least less than half of what we might use with a fully grown adult. Studies by Hawk et al (2016) and Marchand (2013) agreed that Chiropractors use 15 – 35 x less force in the under 3-month age group when compared to medical practitioners doing manipulation (Koch, 2002) [3]. We also use less force in all other paediatrics groups, especially when compared to adults (Marchand, 2013). In addition to using lower force, depth, amplitude and speed in our chiropractic adjustments [4], we utilise different techniques. We expect all children under the age of 16 years to be accompanied by a responsible adult during appointments unless prior permission to treat without a consenting adult e.g., over the age of 14 has been discussed with the treating chiropractor.
Risks
- Research into chiropractic care for children in the past 70 years has shown it to have a low risk of adverse effects (Miller, 2019) [5]. These effects tend to be mild and of short duration e.g., muscular or ligament irritation. Vorhra et al (2007) found the risk of severe of adverse effects (e.g. fracture, quadriplegia, paraplegia, and death) is very, very rare and was more likely to occur in individuals where there is already serious underlying pathology and missed diagnosis by other medical profession [6]. These particular cases occurred more than 25 years ago and is practically unheard of now since research and evidence-based care has become the norm [7].
- The most common side effect in infants following chiropractic treatment includes fussiness or irritability for the first 24 hours, and sleeping longer than usual or more soundly. (Miller and Benfield, 2008) [8]
- In older children, especially if presenting with pain e.g., in the neck or lower back, the greatest risk is that this pain may increase during examination due to increasing the length of involved muscles or ligaments [9]. Similarly, the child may also experience pain, stiffness or irritability after treatment (Miller & Benfield, 2008) [10]. Occasionally children may experience a headache.[11] We find that children experience side effects much less often than adults.[12]
Benefits
- Your child might get better with chiropractic care. [13] If they don’t, we will refer you on [14].
- Low risk of side effects and very rare risk of serious adverse effects [15].
- Drug-free health care. We are not against medication, but we do not prescribe [16].
- Compared with a medical practitioner, manual therapy carried out by a chiropractor is 20 x less likely to result in injury (Koch et al 2002, Miller 2009).[17]
- Children do not often require long courses of treatment (>3 weeks) unless complicating factors are present.[18]
- Studies have shown that parents have a high satisfaction rate with Chiropractic care [19].
- Physical therapies are much less likely to interfere with biomedical treatments. (McCann & Newell 2006) [20]
- You will have a better understanding of diagnosis of any complain and we will let you know what you can do to help.[21]
We invite you to have open discussions and communication with your treating chiropractor at all times. Should you need any further clarification please just ask.
References
- Hawk, C. Shneider, M.J., Vallone, S and Hewitt, E.G. (2016) – Best practises recommendations for chiropractic care of children: A consensus update. JMPT, 39 (3), 158-168.
- Marchand, A. (2013) – A Proposed model with possible implications for safety and technique adaptations for chiropractic spinal manipulative therapy for infants and children. JMPT, 5, 1-14
- Koch L. E., Koch, H, Graumann-Brunnt, S. Stolle, D. Ramirez, J.M., & Saternus, K.S. (2002) – Heart rate changes in response to mild mechanical irritation of the high cervical cord region in infants. Forensic Science International, 128, 168-176
- Miller J (2019) – Evidence-Based Chiropractic Care for Infants: Rational, Therapies and Outcomes. Chapter 11: Safety of Chiropractic care for Infants p111. Praeclarus Press
- Vohra, S. Johnston, B.C. Cramer, K, Humphreys, K. (2007) – Adverse events associated with paediatric spinal manipulation: A Systematic Review. Pediatrics, 119 (1) e275-283
- Miller, J and Benfield (2008) – Adverse effects of spinal manipulative therapy in children younger than 3 years: a retrospective study in a chiropractic teaching clinic. JMPT Jul-Aug;31(6):419-23.
- McCann, L.J. & Newell, S.J. (2006). Survey of paediatric complementary and alternative medicine in health and chronic disease. Archives of Diseases of Childhood, 91, 173-174
- Corso, M., Cancelliere, C. , Mior., Taylor-Vaise, A. Côté, P. (2020) – The safety of spinal manipulative therapy in children under 10 years: a rapid review. Chiropractic Manual therapy 25: 12
___________________________________
- “taking joints to the end range of function” (range of motion, more likely) is arguably not “very gently”;
- “we strive to follow a system of evidence-based care”; I do not think that this is possible because pediatric chiropractic care is hardy evidence-based;
- as a generalizable statement, this seems to be not true;
- ” lower force, depth, amplitude and speed”; I am not sure that there is good evidence for that;
- research has foremost shown that there might be significant under-reporting;
- to blame the medical profession for diagnoses missed by chiropractors seems odd;
- possibly because of under-reporting;
- possibly because of under-reporting;
- possibly because of under-reporting;
- possibly because of under-reporting;
- possibly because of under-reporting;
- your impressions are not evidence;
- your child might get even better without chiropractic care;
- referral rates of chiropractors tend to be low;
- possibly because of under-reporting;
- chiropractors have no prescription rights but some lobby hard for it;
- irrelevant if we consider the intervention useless and thus obsolete;
- any evidence for this statement?;
- satisfaction rates are no substitute for real evidence;
- that does not mean they are effective, safe, or value for money;
- this is perhaps the strangest statement of them all – do chiropractors think they are the optimal diagnosticians for all complaints?
_____________________________________
According to its title, the paper was supposed to deal with consent for chiropractic pediatric care. It almost totally avoided the subject and certainly did not list the information chiropractors must give to parents before commencing treatment.
Considering the arguments that the article did provide has brought me to the conclusion that chiropractors who treat children are out of touch with reality and seem in danger of committing child abuse.
I had come across them so often that I had almost stopped noticing them: the ‘little extras‘ that make ineffective so-called alternative medicines (SCAMs) seem effective. Then, recently, during an interview about detox diets, the interviewer responded to my explanation of the ineffectiveness of these treatments by saying: “but these diets include stopping the consumption of alcohol, cigarettes, and other harmful stuff; therefore they must be good.” This seemingly convincing argument reminded me of a phenomenon – I call it here the ‘little extra‘ – that applies to so many (if not most) SCAMs.
Let me schematically summarise it as follows:
- A practitioner applies an ineffective SCAM to a patient.
- Because it is ineffective, it has little effect other than a small placebo response.
- The ineffective SCAM comes with a ‘little extra‘ which is unrelated to the SCAM.
- The ‘little extra‘ is effective.
- The end result is that the ineffective SCAM appears to be effective.
The above example makes it quite clear: the detox diet is utter nonsense but, as it goes hand in hand with effective lifestyle changes, it appears to be effective. A classic case. But SCAM offers no end of similar examples:
- Acupuncture is useless but it involves touch, time, attention, and empathy all of which are effective in making a patient feel better.
- Chiropractic is useless but it involves touch, time, attention, and empathy all of which are effective in making a patient feel better.
- Homeopathy is useless but it involves a long, empathic consultation and attention which are effective in making a patient feel better.
- Osteopathy is useless but it involves touch, time, attention, and empathy all of which are effective in making a patient feel better.
- Reflexology is useless but it involves touch, time, attention, and empathy all of which are effective in making a patient feel better.
Do I need to continue?
Probably not!
The ‘little extras‘ are often forgotten or subsumed under the heading ‘placebo’. Yet, they are not part of the placebo effect. Strictly speaking, they are concomitant treatments comparable to a pain patient using SCAM and also taking a few paracetamols. In the end, she forgets about the painkillers and thinks that her SCAM worked wonders.
Even ardent SCAM proponents have long realized this phenomenon. Here, for example, is a paper entitled ‘Acupuncture as a complex intervention: a holistic model’ by ex-colleagues of mine at Exeter looking at it but coming up with a very different perspective:
Objectives: Our understanding of acupuncture and Chinese medicine is limited by a lack of inquiry into the dynamics of the process. We used a longitudinal research design to investigate how the experience, and the effects, of a course of acupuncture evolved over time.
Design and outcome measures: This was a longitudinal qualitative study, using a constant comparative method, informed by grounded theory. Each person was interviewed three times over 6 months. Semistructured interviews explored people’s experiences of illness and treatment. Across-case and within-case analysis resulted in themes and individual vignettes.
Subjects and settings: Eight (8) professional acupuncturists in seven different settings informed their patients about the study. We interviewed a consecutive sample of 23 people with chronic illness, who were having acupuncture for the first time.
Results: People described their experience of acupuncture in terms of the acupuncturist’s diagnostic and needling skills; the therapeutic relationship; and a new understanding of the body and self as a whole being. All three of these components were imbued with holistic ideology. Treatment effects were perceived as changes in symptoms, changes in energy, and changes in personal and social identity. The vignettes showed the complexity and the individuality of the experience of acupuncture treatment. The process and outcome components were distinct but not divisible, because they were linked by complex connections. The paper depicts these results as a diagrammatic model that illustrates the components and their interconnections and the cyclical reinforcement, both positive and negative, that can occur over time.
Conclusions: The holistic model of acupuncture treatment, in which “the whole being greater than the sum of the parts,” has implications for service provision and for research trial design. Research trials that evaluate the needling technique, isolated from other aspects of process, will interfere with treatment outcomes. The model requires testing in different service and research settings.
I think the perspective of viewing SCAMs as complex interventions is needlessly confusing and deeply unhelpful. The truth is that there is no treatment that is not complex. Take a surgical treatment, for instance, it involves dozens of ‘little extras‘ that are known to be effective. Should we, therefore, try to use this fact for justifying useless surgical interventions? Or take a simple prescription of medication from a doctor. It involves time, empathy, attention, explanations, etc. all of which will affect the patient’s symptoms. Should we thus use this to justify a useless drug? Certainly not!
And for the same reason, it is nonsense to use the ‘little extras‘ that come with all the numerous ineffective SCAMs as a smokescreen that makes them look effective.
It has been reported that Goop founder Gwyneth Paltrow now has taken to promoting the weirdest wellness thing she’s ever done: rectal ozone therapy. ‘I have used ozone therapy, rectally. Can I say that?’ she told Dear Media podcast The Art of Being Well. ‘It’s pretty weird. It’s pretty weird, yeah. But it’s been very helpful.’
The benefits of rectal ozone therapy are said to be reduced pain/inflammation, increased energy, improved metabolism/circulation, stimulated immune system, detoxification, anti-aging, and fighting bacterial/viral infections.
But who am I to criticize an authority like Gwyneth?
Therefore, I better look up the evidence! And if you had speculated that there is none, you would have been mistaken. Here are some of the more recent clinical studies listed in Medline:
Objective: Fibromyalgia is a chronic disorder with a very complex symptomatology. Although generalized severe pain is considered to be the cardinal symptom of the disease, many other associated symptoms, especially non-restorative sleep, chronic fatigue, anxiety, and depressive symptoms also play a relevant role in the degree of disability characteristic of the disease. Ozone therapy, which is used to treat a wide range of diseases and seems to be particularly useful in the treatment of many chronic diseases, is thought to act by exerting a mild, transient, and controlled oxidative stress that promotes an up-regulation of the antioxidant system and a modulation of the immune system. According to these mechanisms of action, it was hypothesized that ozone therapy could be useful in fibromyalgia management, where the employed therapies are very often ineffective.
Patients and methods: Sixty-five patients with fibromyalgia, according to the definition of the American College of Rheumatology (Arthritis Rheum 1990; 33: 160-172), were treated at the MEDE Clinic (Sacile, Pordenone, Italy) from February 2016 to October 2018. Females were 55 and males were 10; age ranged from 30 to 72 years, and the time from fibromyalgia diagnosis ranged from 0.5 to 33 years. Treatment was made by autohemotransfusion in 55 patients and by ozone rectal insufflations in 10 patients, according to SIOOT (Scientific Society of Oxygen Ozone Therapy) protocols, twice a week for one month and then twice a month as maintenance therapy.
Results: We found a significative improvement (>50% of symptoms) in 45 patients (70%). No patient reported important side effects. In conclusion, at our knowledge, this is the largest study of patients with fibromyalgia treated with ozone therapy reported in the literature and it demonstrates that the ozone therapy is an effective treatment for fibromyalgia patients without significant side effects.
Conclusions: At the moment, ozone therapy seems a treatment that, also because without any side effect, is possible to be proposed to patients with fibromyalgia that are not obtaining adequate results from other available treatments and it can be considered as complementary/integrative medicine.
No2:
Introduction: The Corona virus disease 19 (COVID-19) has accounted for multiple deaths and economic woes.While the entire medical fraternity and scientists are putting their best feet forward to find a solution to contain this deadly pandemic, there is a growing interest in integrating other known alternative therapies in to standard care. This study is aimed at evaluating the safety and efficacy of ozone therapy (OT), as an adjuvant to the standard of care (SOC).
Methods: In the current randomized control trial, 60 patients with mild to moderate score NEWS score were included in two parallel groups (n = 30/group). The interventional group (OZ) received ozonized rectal insufflation and minor auto haemotherapy, daily along with SOC, while the control group (ST) received SOC alone. The main outcome measures included changes in clinical features, oxygenation index (SpO2), NEWS score, Reverse transcription polymerase chain reaction(RT-PCR), inflammatory markers, requirement of advanced care, and metabolic profiles.
Results: The OZ group has shown clinically significant improvement in the mean values of all the parameters tested compared to ST Group. However, statistical significance were only observed in RT-PCR negative reaction (P = 0.01), changes in clinical symptoms (P < 0.05) and requirement for Intensive care (P < 0.05). No adverse events were reported in OZ group, as against 2 deaths reported in ST group.
Conclusion: OT when integrated with SOC can improve the clinical status and rapidly reduce the viral load compared to SOC alone, which facilitate early recovery and check the need for advanced care and mortality as demonstrated in this study.
Introduction: IgA deficiency is a primary immunodeficiency predominantly due to an antibody defect, for which there is no replacement therapy. Treatment consists of prevention and treatment of infections and other associated conditions. Given the immunomodulatory and regulatory properties of the redox balance of ozone therapy in infectious and inflammatory conditions, evaluation of its effect on IgA deficiency is of interest.
Objective: Assess the benefits and possible adverse effects of ozone treatment in patients with IgA deficiency.
Methods: A monocentric randomized controlled phase 2 clinical trial (RPCEC 00000236) was carried out, after approval by the Institutional Ethics Committee of the Roberto Rodríguez Fernández Provincial General Teaching Hospital in Morón, Ciego de Ávila Province, Cuba. Included were 40 patients aged 5-50 years, distributed in 2 groups of 20, after agreeing to participate and signing informed consent. The experimental group received 2 cycles of ozone by rectal insufflation for 20 days (5 times a week for 4 weeks each cycle) with a 3-month interval between cycles, for a total of 40 doses, with age-adjusted dose ranges. The control group was treated with leukocyte transfer factor (Hebertrans), 1 U per m2 of body surface area subcutaneously, once weekly for 12 weeks. Frequency of appearance and severity of clinical symptoms and signs of associated diseases, serum immunoglobulin concentrations and balance of pro-oxidant and antioxidant biomarkers were recorded at treatment initiation and one month after treatment completion. Therapeutic response was defined as complete, partial, stable disease or progressive disease. Descriptive statistics and significance were calculated to compare groups and assess effect size.
Results: One month after treatment completion, 70% of patients in the experimental group experienced significant increases in IgG(p = 0.000) and IgM (p = 0.033). The experimental group also displayed decreased pro-oxidation biomarkers, glutathione modulation and increased antioxidant enzymes, with reduced oxidative stress; none of these occurred in the control group. Complete therapeutic response was achieved in 85% of patients in the experimental group and only 45% in the control group. Mild, transient adverse events were reported in both groups.
Conclusions: Ozone therapy by rectal insufflation is a suitable therapeutic option for treating IgA deficiency because it produces antioxidant and immunomodulatory effects and is feasible, safe and minimally invasive.
Background: Ozone therapy may stimulate antioxidant systems and protect against free radicals. It has not been used formerly in patients with pulmonary emphysema.
Aim: To assess the effects of rectal ozone therapy in patients with pulmonary emphysema.
Material and methods: Sixty four patients with pulmonary emphysema, aged between 40 and 69 years, were randomly assigned to receive rectal ozone in 20 daily sessions, rectal medicinal oxygen or no treatment. Treatments were repeated three months later in the first two groups. At baseline and at the end of the study, spirometry and a clinical assessment were performed.
Results: fifty patients completed the protocol, 20 receiving ozone therapy, 20 receiving rectal oxygen and 10 not receiving any therapy. At baseline, patients on ozone therapy had significantly lower values of forced expiratory volume in the first second (fEV1) and fEV1/forced vital capacity. At the end of the treatment period, these parameters were similar in the three treatment groups, therefore they only improved significantly in the group on ozone therapy. No differences were observed in other spirometric parameters.
Conclusions: Rectal ozone therapy may be useful in patients with pulmonary emphysema.
Background: Pain secondary to chemotherapy-induced peripheral neuropathy (CIPN) can limit the administration of chemotherapy, cancer-treatment outcomes, and the quality of life of patients. Oxidative stress and inflammation are some of the key mechanisms involved in CIPN. Successful treatments for CIPN are limited. This report shows our preliminary experience using ozone treatment as a modulator of oxidative stress in chronic pain secondary to CIPN. Methods: Ozone treatment, by rectal insufflation, was administered in seven patients suffering from pain secondary to grade II or III CIPN. Pain was assessed by the visual analog scale (VAS). Results: All patients, except one, showed clinically relevant pain improvement. Median pain score according to the VAS was 7 (range: 5-8) before ozone treatment, 4 (range: 2-6) at the end of ozone treatment (p = 0.004), 5.5 (range: 1.8-6.3) 3 months after the end of ozone treatment (p = 0.008), and 6 (range: 2.6-6.6) 6 months after the end of ozone treatment (p = 0.008). The toxicity grade, according to the Common Terminology Criteria for Adverse Events (CTCAE v.5.0), improved in half of the patients. Conclusion: This report shows that most patients obtained clinically relevant and long-lasting improvement in chronic pain secondary to CIPN after treatment with ozone. These observed effects merit further research and support our ongoing randomized clinical trial.
Background: Medical ozone is more bactericidal, fungicidal, and virucidal than any other natural substance. Some studies proved that ozone infused into donated blood samples can kill viruses 100% of the time. Ozone, because of its special biologic properties, has theoretical and practical attributes to make it a potent hepatitis C virus (HCV) inactivator, which suggests an important role in the therapy for hepatitis C.
Aim: The study aim is to evaluate the role of ozone therapy in decreasing HCV ribonucleic acid (HCV RNA) load and its effect on the liver enzymes among patients with chronic hepatitis C.
Methods: This study included 52 patients with chronic hepatitis C (positive polymerase chain reaction [PCR] for HCV RNA and raised serum alanine transaminase [ALT] for more than 6 months). All patients were subjected to meticulous history taking and clinical examination. Complete blood count, liver function tests, and abdominal ultrasonography were requested for all patients. The ozone group included 40 patients who received major autohemotherapy, minor autohemotherapy, and rectal ozone insufflation. The other 12 patients (conventional group) received silymarin and/or multivitamins.
Results: There were significant improvements of most of the presenting symptoms of the patients in the ozone group in comparison to the conventional group. ALT and aspartate transaminase (AST) levels normalized in 57.5% and 60% in the ozone group, respectively, in comparison to 16.7% and 8% in the conventional group, respectively. Polymerase chain reaction (PCR) for HCV RNA was negative among 25% and 44.4% after 30 and 60 sessions of ozone therapy, respectively, in comparison to 8% among the conventional group.
Conclusions: Ozone therapy significantly improves the clinical symptoms associated with chronic hepatitis C and is associated with normalized ALT and AST levels among a significant number of patients. Ozone therapy is associated with disappearance of HCV RNA from the serum (-ve PCR for HCV RNA) in 25%-45% of patients with chronic hepatitis C.
Oxidative stress is suggested to have an important role in the development of complications in diabetes. Because ozone therapy can activate the antioxidant system, influencing the level of glycemia and some markers of endothelial cell damage, the aim of this study was to investigate the therapeutic efficacy of ozone in the treatment of patients with type 2 diabetes and diabetic feet and to compare ozone with antibiotic therapy. A randomized controlled clinical trial was performed with 101 patients divided into two groups: one (n = 52) treated with ozone (local and rectal insufflation of the gas) and the other (n = 49) treated with topical and systemic antibiotics. The efficacy of the treatments was evaluated by comparing the glycemic index, the area and perimeter of the lesions and biochemical markers of oxidative stress and endothelial damage in both groups after 20 days of treatment. Ozone treatment improved glycemic control, prevented oxidative stress, normalized levels of organic peroxides, and activated superoxide dismutase. The pharmacodynamic effect of ozone in the treatment of patients with neuroinfectious diabetic foot can be ascribed to the possibility of it being a superoxide scavenger. Superoxide is considered a link between the four metabolic routes associated with diabetes pathology and its complications. Furthermore, the healing of the lesions improved, resulting in fewer amputations than in control group. There were no side effects. These results show that medical ozone treatment could be an alternative therapy in the treatment of diabetes and its complications.
___________________________
What does that tell us?
That rectal ozone therapy is a panacea?
No, I don’t think so.
In my view, it tells us that strange journals publish a lot of dodgy research from strange research groups that use dodgy methodologies to confirm their odd belief that bogus treatments work for everything.
PS
I wonder which orifice Gwyneth will employ next to get the attention of the public.