bias
Hypericum perforatum (St John’s wort) is often recommended as a remedy to relieve pain caused by nerve damage. This trial investigated whether homeopathic Hypericum leads to a reduction in postoperative pain and a decrease in pain medication compared with placebo.
The study was designed as a randomized double-blind, monocentric, placebo-controlled clinical trial with inpatients undergoing surgery for lumbar sequestrectomy. Homeopathic treatment was compared to placebo, both in addition to usual pain management. The primary endpoint was pain relief measured with a visual analog scale. Secondary endpoints were the reduction of inpatient postoperative analgesic medication and change in sensory and affective pain perception.
The results show that the change in pain perception between baseline and day 3 did not significantly differ between the study arms. With respect to pain medication, total morphine equivalent doses did not differ significantly. However, a statistical trend and a moderate effect (d = 0.432) in the decrease of pain medication consumption in favor of the Hypericum group was observed.
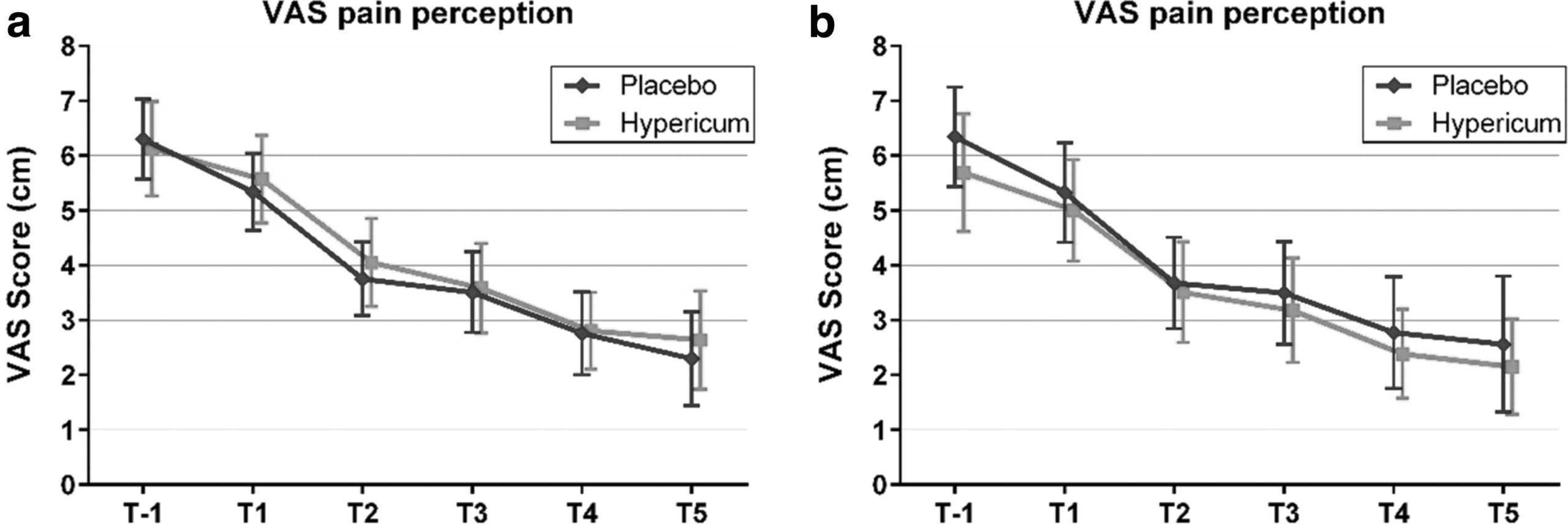
The authors concluded that this is the first trial of homeopathy that evaluated the efficacy of Hypericum C200 after lumbar monosegmental spinal sequestrectomy. Although no significant differences between the groups could be shown, we found that patients who took potentiated Hypericum in addition to usual pain management showed lower consumption of analgesics. Further investigations, especially with regard to pain medication, should follow to better classify the described analgesic reduction.
For a number of reasons, this is a remarkably mysterious and quite hilarious study:
- Hypericum is recommended as an analgesic for neuropathic pain.
- According to the ‘like cures like’ axiom of homeopathy, it therefore must increase pain in such situations.
- Yet, the authors of this trial mounted an RCT to see whether it reduces pain.
- Thus they either do not understand homeopathy or wanted to sabotage it.
- As they are well-known pro-homeopathy researchers affiliated with a university that promotes homeopathy (Witten/Herdecke University, Herdecke, Germany), both explanations are highly implausible.
- The facts that the paper was published in a pro-SCAM journal (J Integr Complement Med), and the study was sponsored by the largest German firm of homeopathics (Deutsche Homoeopathische Union) renders all this even more puzzling.
- However, these biases do explain that the authors do their very best to mislead us by including some unwarranted ‘positive’ findings in their overall conclusions.
In the end, none of this matters, because the results of the study reveal that firstly the homeopathic ‘law of similars’ is nonsense, and secondly one homeopathic placebo (i.e. Hypericum C200) produces exactly the same outcomes as another, non-homeopathic placebo.
It’s again the season for nine lessons, I suppose. So, on the occasion of Christmas Eve, let me rephrase the nine lessons I once gave (with my tongue firmly lodged in my cheek) to those who want to make a pseudo-scientific career in so-called alternative medicine (SCAM) research.

- Throw yourself into qualitative research. For instance, focus groups are a safe bet. They are not difficult to do: you gather 5 -10 people, let them express their opinions, record them, extract from the diversity of views what you recognize as your own opinion and call it a ‘common theme’, and write the whole thing up, and – BINGO! – you have a publication. The beauty of this approach is manifold:
-
- you can repeat this exercise ad nauseam until your publication list is of respectable length;
- there are plenty of SCAM journals that will publish your articles;
- you can manipulate your findings at will;
- you will never produce a paper that displeases the likes of King Charles;
- you might even increase your chances of obtaining funding for future research.
- Conduct surveys. They are very popular and highly respected/publishable projects in SCAM. Do not get deterred by the fact that thousands of similar investigations are already available. If, for instance, there already is one describing the SCAM usage by leg-amputated policemen in North Devon, you can conduct a survey of leg-amputated policemen in North Devon with a medical history of diabetes. As long as you conclude that your participants used a lot of SCAMs, were very satisfied with it, did not experience any adverse effects, thought it was value for money, and would recommend it to their neighbour, you have secured another publication in a SCAM journal.
- In case this does not appeal to you, how about taking a sociological, anthropological or psychological approach? How about studying, for example, the differences in worldviews, the different belief systems, the different ways of knowing, the different concepts about illness, the different expectations, the unique spiritual dimensions, the amazing views on holism – all in different cultures, settings or countries? Invariably, you must, of course, conclude that one truth is at least as good as the next. This will make you popular with all the post-modernists who use SCAM as a playground for enlarging their publication lists. This approach also has the advantage to allow you to travel extensively and generally have a good time.
- If, eventually, your boss demands that you start doing what (in his narrow mind) constitutes ‘real science’, do not despair! There are plenty of possibilities to remain true to your pseudo-scientific principles. Study the safety of your favourite SCAM with a survey of its users. You simply evaluate their experiences and opinions regarding adverse effects. But be careful, you are on thin ice here; you don’t want to upset anyone by generating alarming findings. Make sure your sample is small enough for a false negative result, and that all participants are well-pleased with their SCAM. This might be merely a question of selecting your patients wisely. The main thing is that your conclusions do not reveal any risks.
- If your boss insists you tackle the daunting issue of SCAM’s efficacy, you must find patients who happened to have recovered spectacularly well from a life-threatening disease after receiving your favourite form of SCAM. Once you have identified such a person, you detail her experience and publish this as a ‘case report’. It requires a little skill to brush over the fact that the patient also had lots of conventional treatments, or that her diagnosis was never properly verified. As a pseudo-scientist, you will have to learn how to discretely make such details vanish so that, in the final paper, they are no longer recognisable.
- Your boss might eventually point out that case reports are not really very conclusive. The antidote to this argument is simple: you do a large case series along the same lines. Here you can even show off your excellent statistical skills by calculating the statistical significance of the difference between the severity of the condition before the treatment and the one after it. As long as this reveals marked improvements, ignores all the many other factors involved in the outcome and concludes that these changes are the result of the treatment, all should be tickety-boo.
- Your boss might one day insist you conduct what he narrow-mindedly calls a ‘proper’ study; in other words, you might be forced to bite the bullet and learn how to do an RCT. As your particular SCAM is not really effective, this could lead to serious embarrassment in the form of a negative result, something that must be avoided at all costs. I, therefore, recommend you join for a few months a research group that has a proven track record in doing RCTs of utterly useless treatments without ever failing to conclude that it is highly effective. In other words, join a member of my ALTERNATIVE MEDICINE HALL OF FAME. They will teach you how to incorporate all the right design features into your study without the slightest risk of generating a negative result. A particularly popular solution is to conduct a ‘pragmatic’ trial that never fails to produce anything but cheerfully positive findings.
- But even the most cunningly designed study of your SCAM might one day deliver a negative result. In such a case, I recommend taking your data and running as many different statistical tests as you can find; chances are that one of them will produce something vaguely positive. If even this method fails (and it hardly ever does), you can always focus your paper on the fact that, in your study, not a single patient died. Who would be able to dispute that this is a positive outcome?
- Now that you have grown into an experienced pseudo-scientist who has published several misleading papers, you may want to publish irrefutable evidence of your SCAM. For this purpose run the same RCT over again, and again, and again. Eventually, you want a meta-analysis of all RCTs ever published (see examples here and here). As you are the only person who conducted studies on the SCAM in question, this should be quite easy: you pool the data of all your dodgy trials and, bob’s your uncle: a nice little summary of the totality of the data that shows beyond doubt that your SCAM works and is safe.
The year 2022 is drawing to a close, and I am reminded of my ‘WORST PAPER OF 2022 COMPETITION’. As a prize, I am offering the winner (that is the lead author of the winning paper) one of my books that best fits his/her subject. I am sure this will overjoy him or her. I hope to identify about 10 candidates for the prize, and towards the end of the year, I let my readers decide democratically on who should be the winner. In this spirit of democratic voting, let me suggest to you entry No 10 entitled ‘Conventional Homeopathic Medicine and Its Relevance to Modern Medicine‘. Here is the unadulterated abstract:
Context: Homeopathic medicine can be explained as a symptoms-based method of treatment, and it can act as an alternative treatment strategy against allopathy by focusing on the symptoms of illness, as opposed to causative agents as allopathic medicine does. Also, homeopathic medicines are extracted from nature rather than being chemically synthesized as western drugs are.
Objective: The review intended to briefly describe the concept of homeopathic medicine, its emergence from a historical point of view, and its broader healing properties, providing examples of key homeopathic drugs and comparing them to modern medicines.
Design: The research team performed a narrative review by searching databases like Pubmed, Google Scholar, and other national search engines. The search used the keywords homeopathic medicine, alternate medicine, materia medica, allium cepa, Zingiber officinale, penicillium, Agaricus muscaria, Botulinum toxin.
Setting: Dr. D.Y. Patil Homoeopathic Medical College and Research Centre, Dr. D.Y. Patil Vidyapeeth (Deemed to be University), Pimpri, Pune.
Results: This review highlights the rich sources homoeopathic drugs and their corelation with modern medicine. The current review focuses on the significance of the Homeopathic Materia Medica and on notable remedies in homeopathy that align with allopathy in addressing different pathological conditions, including treatments that the two types of medicine have in in common and that are effective in homeopathy.
Conclusions: Many studies are being conducted to prove the mechanism of action of homoeopathic medicines. Droplet Evaporating Method (DEM), Raman, UltraViolet-Visible (UV-VIS) spectroscopy and Transmission Electron Microscopy (TEM) are commonly used methods to characterize homeopathic medicines at ultra-low concentration and many such studies will surely indicate how homoeopathic medicines act. Such research results may subsequently lead to the betterment of treatment procedures and the integration of homeopathic principles into mainstream medical practices.
I find it quite an ‘achievement’ to put so much nonsense into such a short abstract. My ‘favorite’ statement is this one: “many such studies will surely indicate how homoeopathic medicines act.” Since he published this paper, the first author has done another article; it is entitled “Breast Abscess Healing with Homoeopathy: A Case Report” and would be a further contender for my award.
But let’s not give him an unfair chance to win the competition!
PS
The next time I post about this will be about deciding on this year’s winner. So, you might want to give it some consideration.
The INDY and many other news outlets reported that the British Tory MP, Andrew Bridgen, has called on prime minister Rishi Sunak to suspend mRNA covid vaccines after alleging they are “not safe, not effective and not necessary”.
During Wednesday’s PMQs (13 December), Bridgen stated that “since the rollout in the UK of the BioNTech-Pfizer mRNA vaccine, we have had almost half a million reports of adverse effects from the public”, a message he later reiterated on Twitter.
Posting a snippet from his debate, Bridgen tweeted: “Almost half a million yellow card reports of adverse effects following administration of the Biotech Pfizer mRNA vaccine in the UK alone! Answers are desperately needed. #completelyunprecedented”.
Bridgen also claimed that a leading figure in the British Heart Foundation is suppressing evidence that the Covid vaccines cause heart damage, even sending non-disclosure agreements to his research team.
Facebook flagged his post with a notice urging users to ensure that they share “reliable information.” It included two links to “continue sharing” or “get vaccine info.”

The scandals Bridgen has been involved in seem too numerous to mention (e.g. violation of parliamentary standards, homophobic remarks, antisemitic statements). Here is just one of the most recent:
A Leicestershire MP has been ordered to pay £800,000 and been evicted from his five bedroom home by a judge following a legal dispute involving the family vegetable business. It is currently unknown where Andrew Bridgen, Conservative MP for North West Leicestershire, lives after being given final deadline of August 24 to vacate the premises in Coleorton, near Coalville.
The 57-year-old was branded “dishonest” by a High Court judge in March – who ruled that Bridgen “lied” under oath. Judge Brian Rawlings said he was so dishonest that nothing he said about the dispute with AB Produce, a vegetable and potato supplier based in Measham, could be taken at face value.
Bridgen was also said to have behaved in an “abusive”, “arrogant” and “aggressive” way during the dispute, in which he has spent years suing the firm. A later judgment in June, reported by the Times on Sunday, forced the MP to vacate the £1.5 million-valued property owned by AB Produce that he has lived in since 2015…
For a fact check on Bridgeon’s vaccine claims, see here. And below are a few reactions from Twitter users to Bridgen’s Covid proctophsia:
First a High Court judge says Tory MP, Andrew Bridgen, lied under oath, then he evicts him from his home and orders him to pay £800,000 now Facebook flags his posts as Covid misinformation. How’s your week going?
Andrew Bridgen MP now promoting Dr David Cartland, a man who aligns himself with claims that Freemasons rule the world; that Covid doesn’t exist; and that medical doctors who don’t share his views should be executed (screenshots H/T
Andrew Bridgen MP now promoting Dr David Cartland, a man who aligns himself with claims that Freemasons rule the world; that Covid doesn’t exist; and that medical doctors who don’t share his views should be executed.
This Andrew Bridgen? ‘A Conservative MP lied under oath, behaved in an abusive, arrogant and aggressive way, and was so dishonest that his claims about a multimillion-pound family dispute could not be taken at face value, a high court judge has ruled.’
Proper tinfoil-hat stuff from Andrew Bridgen, suggesting Covid vaccines are unsafe, misrepresenting data, and implying some sort of conspiracy between ‘Big Pharma’ and MHRA.

Our ‘Memorandum Integrative Medicine‘ seems to be causing ripples. A German website that claims to aim at informing consumers objectively posted a rebuttal. Here is my translation (together with comments by myself inserted via reference numbers in brackets and added below):
With drastic words and narrow-mindedness bordering on ideology (1), the Münster Circle, an association of opponents to complementary therapies such as homeopathy (2), takes issue with the treatment concept of integrative medicine in a memorandum (3). By integrative medicine physicians understand the combination of doctor-led medicine and doctor-led complementary medicine to a meaningful total concept with the goal of reducing side effects and to treating patients individually and optimally (4). Integrative medicine focuses primarily on chronic diseases, where conventional acute medicine often reaches its limits (5)In the memorandum of the Münsteraner Kreis, general practitioner Dr. Claudia Novak criticizes integrative medicine as “guru-like self-dramatization” (6) by physicians and therapists, which undermines evidence-based medicine and leads to a deterioration in patient care. She is joined by Prof. Dr. Edzard Ernst, Professor Emeritus of Alternative Medicine, who has changed from Paul to Saul with regard to homeopathy (7) and is leading a veritable media campaign against proponents of treatment procedures that have not been able to prove their evidence in randomized placebo-controlled studies (8). The professor ignores the fact that this involves a large number of drugs that are used as a matter of course in everyday medicine (9) – for example, beta-blockers or other cardiological drugs (10). “Like the devil fears the holy water” (11), the Münsteraner Kreis seems to fear the concept of integrative medicine (12). The vehemence coupled with fear with which they warn against the treatment concept makes one sit up and take notice (13). “As an experienced gynecologist who has successfully worked with biological medicine as an adjunct in his practice for decades, I can only shake my head at such narrow-mindedness”, points out Fred-Holger Ludwig, MD (14). Science does not set limits for itself, but the plurality of methods is immanent (15). “Why doesn’t Prof. Ernst actually give up his professorial title for alternative medicine? That would have to be the logical consequence of its overloud criticism of established treatment concepts from homeopathy to to integrative medicine”, questions Dr. Ludwig (16).
The concept of integrative medicine is about infiltrating alternative procedures into medicine, claim the critics of the concept, without mentioning that many naturopathic procedures have been used for centuries with good results (17) and that healthcare research gives them top marks (18). “Incidentally, the scientists among the representatives of the Münster Circle should know that it is difficult to capture individualized treatment concepts with the standardized procedures of randomized, placebo-controlled studies (19). Anyone who declares the highest level of evidence to be the criterion for approval makes medicine impossible and deprives patients in oncology or with rare diseases, for example, of chances of successful treatment (20). Even there, drugs are used that cannot be based on high evidence, tested in placebo-controlled studies, because the number of cases is too low (21),” notes Dr. Ludwig .
- Ideology? Evidence is not ideology, in my view.
- We are an association of multidisciplinary experts advocating a level playing field with sound evidence in all areas of healthcare.
- The actual memorandum is not linked in this text; does the author not want his readers to form the own opinion?
- In our memorandum, we offer various definitions of integrative medicine (IM), none of which is remotely similar to this one.
- No, IM is usually being promoted in a much wider sense.
- This term does not appear in our memorandum.
- I am not aware that I changed from Paul to Saul with regard to homeopathy; I know that I was led mostly by the evidence.
- I feel flattered but don’t think that my humble work is a ‘media campaign’.
- True, I do not pretend to understand all areas of medicine and tend to be silent in the ones that I lack up-to-date expertise.
- Is he really saying that beta-blockers are not evidence-based?
- The holy water comparison from a homeopath, who arguably makes a living from dishing out ‘holy water’, made me laugh!
- It is most revealing, I think, that he thinks our motivation is fear.
- Splendid!
- FHL is the author of the article, and it is thus charmingly naive that he cites himself in this way
- I somehow doubt that he understands what he is expressing here.
- I find this rather a bizarre idea but I’ll think about it.
- Argumentum ad traditionem.
- Those that get ‘top marks’ belong to evidence-based medicine and not to IM.
- Here the author reveals that he does not understand the RCT methodology and even fails to know the trial evidence on homeopathy – RCTs of individualised homeopathy are possible and have been published (e.g. this one).
- If he really believes this, I fear for his patients.
- Pity that he does not provide an example.
To understand FHL better, it is worth knowing that he claims to treat cancer patients with conventional and homeopathic medicine. He states that this approach reduces side effects – without providing evidence, of course.
Altogether, FHL does not dispute a single fact or argument from our memorandum. In fact, I get the impression that he never actually read it. To me, it feels as though he merely read an article ABOUT the document. In any case, his critique is revealing and important, in my view. It demonstrates that there are no good arguments to defend IM.
So, thank you FHL!
Hardly a day goes by that I am not asked by someone – a friend, colleague, practitioner, journalist, etc. – about the evidence for this or that so-called alternative medicine (SCAM). I always try my best to give a truthful answer, and often it amounts to something like this: TO THE BEST OF MY KNOWLEDGE, THERE IS NO GOOD EVIDENCE TO SHOW THAT IT WORKS.
The reactions to this news vary, e.g.:
- Some ignore it and seem to think ‘what does he know?’.
- Some thank me and make their decisions accordingly.
- Some feel they better do a fact-check.
The latter reaction is perhaps the most interesting because often the person, clearly an enthusiast of that particular SCAM, later comes back to me and triumphantly shows me evidence that contradicts my statement.
This means I now must have a look at what evidence he/she has found.
It can fall into several categories:
- Opinion articles published by proponents of the SCAM in question.
- Papers that are not truly relevant to the SCAM.
- Research that provides data about the SCAM that does not relate to its effectiveness, e.g. surveys, or qualitative studies.
- Studies of the SCAM in question.
It is usually easy to explain why the three first-named categories are irrelevant. Yet, the actual studies can be a problem. Remember, I told that person that no good evidence exists, and now he (let’s assume I am dealing with a man) proudly shows me a study of it suggesting the opposite. There might be the following explanations:
- I did not know this high-quality study (e.g. because it is new) and my dismissive statement was thus questionable or wrong.
- The study draws a positive conclusion about the SCAM but this conclusion is not justified.
In the first instance, do I need to change my mind and apologize for my wrong statement? Perhaps! But I also need to explain that, even with a rigorous study, we really ought to have one (better more than one) independent replication before we start changing our clinical routine.
In the second instance, I need to explain why the conclusion is not justified. The realm of SCAM is plagued by studies with misleading conclusions (as regular readers of this blog know only too well). Therefore, this situation arises with some regularity. There are numerous reasons why a study can generate unreliable findings (as regular readers of this blog know only too well). Some of them are easy to understand others might be more difficult for non-scientists to comprehend. This means that the discussions with the man who proudly brought the ‘evidence’ to my attention can be tedious.
Often he feels that I am unfair to his favorite SCAM. He might argue that:
- I am biased;
- I lack an open mind;
- I am not qualified;
- I am changing the goalpost;
- I am applying double standards because much of the research into conventional medicine is also not flawless.
In such cases, we are likely to eventually end our discussions by agreeing to disagree. He will be convinced of his point of view and I will be convinced of mine. Essentially, we are more or less where we started, and the whole palaver was for nothing.
… a bit like this post?
I hope not!
What I have been trying to demonstrate is that:
- SCAM enthusiasts are often difficult, sometimes impossible to convince;
- research is not always easy to understand and requires a minimum of education and know-how.
Osteopathy is currently regulated in 12 European countries: Cyprus, Denmark, Finland, France, Iceland, Italy, Liechtenstein, Luxembourg, Malta, Portugal, Switzerland, and the UK. Other countries such as Belgium and Norway have not fully regulated it. In Austria, osteopathy is not recognized or regulated. The Osteopathic Practitioners Estimates and RAtes (OPERA) project was developed as a Europe-based survey, whereby an updated profile of osteopaths not only provides new data for Austria but also allows comparisons with other European countries.
A voluntary, online-based, closed-ended survey was distributed across Austria in the period between April and August 2020. The original English OPERA questionnaire, composed of 52 questions in seven sections, was translated into German and adapted to the Austrian situation. Recruitment was performed through social media and an e-based campaign.
The survey was completed by 338 individuals (response rate ~26%), of which 239 (71%) were female. The median age of the responders was 40–49 years. Almost all had preliminary healthcare training, mainly in physiotherapy (72%). The majority of respondents were self-employed (88%) and working as sole practitioners (54%). The median number of consultations per week was 21–25 and the majority of respondents scheduled 46–60 minutes for each consultation (69%).
The most commonly used diagnostic techniques were: palpation of position/structure, palpation of tenderness, and visual inspection. The most commonly used treatment techniques were cranial, visceral, and articulatory/mobilization techniques. The majority of patients estimated by respondents consulted an osteopath for musculoskeletal complaints mainly localized in the lumbar and cervical region. Although the majority of respondents experienced a strong osteopathic identity, only a small proportion (17%) advertise themselves exclusively as osteopaths.
The authors concluded that this study represents the first published document to determine the characteristics of the osteopathic practitioners in Austria using large, national data. It provides new information on where, how, and by whom osteopathic care is delivered. The information provided may contribute to the evidence used by stakeholders and policy makers for the future regulation of the profession in Austria.
This paper reveals several findings that are, I think, noteworthy:
- Visceral osteopathy was used often or very often by 84% of the osteopaths.
- Muscle energy techniques were used often or very often by 53% of the osteopaths.
- Techniques applied to the breasts were used by 59% of the osteopaths.
- Vaginal techniques were used by 49% of the osteopaths.
- Rectal techniques were used by 39% of the osteopaths.
- “Taping/kinesiology tape” was used by 40% of osteopaths.
- Applied kinesiology was used by 17% of osteopaths and was by far the most-used diagnostic approach.
Perhaps the most worrying finding of the entire paper is summarized in this sentence: “Informed consent for oral techniques was requested only by 10.4% of respondents, and for genital and rectal techniques by 21.0% and 18.3% respectively.”
I am lost for words!
I fail to understand what meaningful medical purpose the fingers of an osteopath are supposed to have in a patient’s vagina or rectum. Surely, putting them there is a gross violation of medical ethics.
Considering these points, I find it impossible not to conclude that far too many Austrian osteopaths practice treatments that are implausible, unproven, potentially harmful, unethical, and illegal. If patients had the courage to take action, many of these charlatans would probably spend some time in jail.
Earlier this year, I started the ‘WORST PAPER OF 2022 COMPETITION’. As a prize, I am offering the winner (that is the lead author of the winning paper) one of my books that best fits his/her subject. I am sure this will overjoy him or her. I hope to identify about 10 candidates for the prize, and towards the end of the year, I let my readers decide democratically on who should be the winner. In this spirit of democratic voting, let me suggest to you entry No 9. Here is the unadulterated abstract:
Background
With the increasing popularity of traditional Chinese medicine (TCM) by the global community, how to teach basic knowledge of TCM to international students and improve the teaching quality are important issues for teachers of TCM. The present study was to analyze the perceptions from both students and teachers on how to improve TCM learning internationally.
Methods
A cross-sectional national survey was conducted at 23 universities/colleges across China. A structured, self-reported on-line questionnaire was administered to 34 Chinese teachers who taught TCM course in English and to 1016 international undergraduates who were enrolled in the TCM course in China between 2017 and 2021.
Results
Thirty-three (97.1%) teachers and 900 (88.6%) undergraduates agreed Chinese culture should be fully integrated into TCM courses. All teachers and 944 (92.9%) undergraduates thought that TCM had important significance in the clinical practice. All teachers and 995 (97.9%) undergraduates agreed that modern research of TCM is valuable. Thirty-three (97.1%) teachers and 959 (94.4%) undergraduates thought comparing traditional medicine in different countries with TCM can help the students better understand TCM. Thirty-two (94.1%) teachers and 962 (94.7%) undergraduates agreed on the use of practical teaching method with case reports. From the perceptions of the undergraduates, the top three beneficial learning styles were practice (34.3%), teacher’s lectures (32.5%), case studies (10.4%). The first choice of learning mode was attending to face-to-face teaching (82.3%). The top three interesting contents were acupuncture (75.5%), Chinese herbal medicine (63.8%), and massage (55.0%).
Conclusion
To improve TCM learning among international undergraduates majoring in conventional medicine, integration of Chinese culture into TCM course, comparison of traditional medicine in different countries with TCM, application of the teaching method with case reports, and emphasization of clinical practice as well as modern research on TCM should be fully considered.
I am impressed with this paper mainly because to me it does not make any sense at all. To be blunt, I find it farcically nonsensical. What precisely? Everything:
- the research question,
- the methodology,
- the conclusion
- the write-up,
- the list of authors and their affiliations: Department of Chinese Integrative Medicine, Women’s Hospital, School of Medicine, Zhejiang University, Hangzhou, China, Department of Traditional Chinese Medicine, School of Basic Medicine, Qingdao University, Qingdao, China, Department of Chinese Integrative Medicine, The Second Affiliated Hospital of Kunming Medical University, Kunming, China, Department of Traditional Chinese Medicine, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, China, Department of Traditional Chinese Medicine, Medical College, China Three Gorges University, Yichang, China, Basic Teaching and Research Department of Acupuncture and Moxibustion, College of Traditional Chinese Medicine, Xinjiang Medical University, Urumqi, China, Institute of Integrative Medicine, Dalian Medical University, Dalian, China, Department of Chinese and Western Medicine, Chongqing Medical University, Chongqing, China, Department of Chinese and Western Medicine, North Sichuan Medical College, Nanchong, China, Department of Chinese and Western Medicine, School of Medicine, Xiamen University, Xiamen, China, School of Traditional Chinese Medicine, Capital Medical University, Beijing, China, School of Traditional Chinese Medicine, Southern Medical University, Guangzhou, China, Department of Traditional Chinese Medicine, The First Affiliated Hospital of Soochow University, Suzhou, China, Department of Traditional Chinese Medicine, School of Medicine, Xiamen University, Xiamen, China, Department of Chinese Medicine/Department of Chinese Integrative Medicine, The First Affiliated Hospital of Anhui Medical University, Hefei, China, Department of Traditional Chinese Medicine, Shengjing Hospital Affiliated to China Medical University, Shenyang, China, Department of Acupuncture, Affiliated Hospital of Jiangsu University, Zhenjiang, China, Teaching and Research Section of Traditional Chinese Medicine, The Second Affiliated Hospital of Soochow University, Suzhou, China, Department of Traditional Chinese Medicine, The Second Affiliated Hospital of Harbin Medical University, Harbin, China, Department of Chinese Medicine, The First Affiliated Hospital of Anhui Medical University, Hefei, China, Department of Chinese Medicine, The First Affiliated Hospital of Kunming Medical University, Kunming, China, Department of Traditional Chinese Medicine, Shengli Clinical Medical College of Fujian Medical University, Fuzhou, China, Department of Chinese Medicine, The First Affiliated Hospital of Jinzhou Medicine University, Jinzhou, China, Department of Integrated Traditional and Western Medicine, The First Affiliated Hospital of Harbin Medical University, Harbin, China, Department of Chinese Medicine, The Second Affiliated Hospital of Guangzhou Medical University, Guangzhou, China, Department of Traditional Chinese Medicine, The First Affiliated Hospital of Fujian Medical University, Fuzhou, China.
- the journal that had this paper peer-reviewed and published.
But what impressed me most with this paper is the way the authors managed to avoid even the slightest hint of critical thinking. They even included a short paragraph in the discussion section where they elaborate on the limitations of their work without ever discussing the true flaws in the conception and execution of this extraordinary example of pseudoscience.
Is acupuncture more than a theatrical placebo? Acupuncture fans are convinced that the answer to this question is YES. Perhaps this paper will make them think again.
A new analysis mapped the systematic reviews, conclusions, and certainty or quality of evidence for outcomes of acupuncture as a treatment for adult health conditions. Computerized search of PubMed and 4 other databases from 2013 to 2021. Systematic reviews of acupuncture (whole body, auricular, or electroacupuncture) for adult health conditions that formally rated the certainty, quality, or strength of evidence for conclusions. Studies of acupressure, fire acupuncture, laser acupuncture, or traditional Chinese medicine without mention of acupuncture were excluded. Health condition, number of included studies, type of acupuncture, type of comparison group, conclusions, and certainty or quality of evidence. Reviews with at least 1 conclusion rated as high-certainty evidence, reviews with at least 1 conclusion rated as moderate-certainty evidence and reviews with all conclusions rated as low- or very low-certainty evidence; full list of all conclusions and certainty of evidence.
A total of 434 systematic reviews of acupuncture for adult health conditions were found; of these, 127 reviews used a formal method to rate the certainty or quality of evidence of their conclusions, and 82 reviews were mapped, covering 56 health conditions. Across these, there were 4 conclusions that were rated as high-certainty evidence and 31 conclusions that were rated as moderate-certainty evidence. All remaining conclusions (>60) were rated as low- or very low-certainty evidence. Approximately 10% of conclusions rated as high or moderate-certainty were that acupuncture was no better than the comparator treatment, and approximately 75% of high- or moderate-certainty evidence conclusions were about acupuncture compared with a sham or no treatment.
Three evidence maps (pain, mental conditions, and other conditions) are shown below
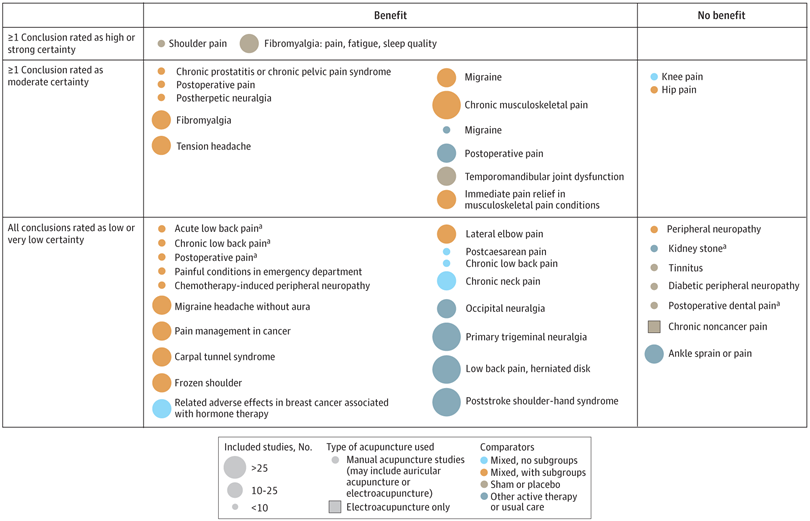
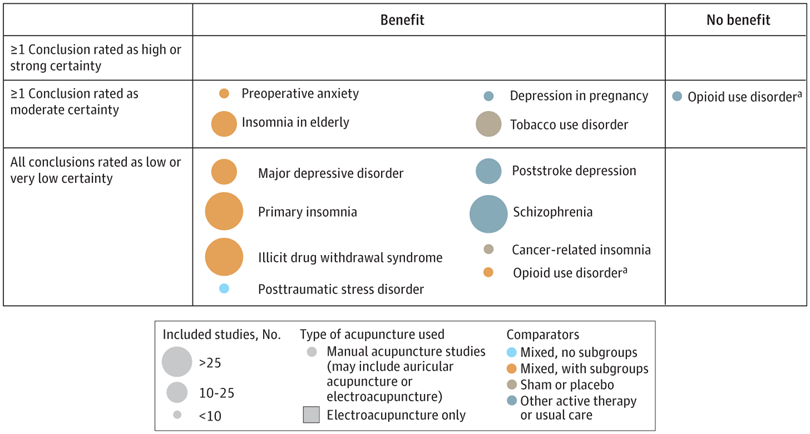

The authors concluded that despite a vast number of randomized trials, systematic reviews of acupuncture for adult health conditions have rated only a minority of conclusions as high- or moderate-certainty evidence, and most of these were about comparisons with sham treatment or had conclusions of no benefit of acupuncture. Conclusions with moderate or high-certainty evidence that acupuncture is superior to other active therapies were rare.
These findings are sobering for those who had hoped that acupuncture might be effective for a range of conditions. Despite the fact that, during recent years, there have been numerous systematic reviews, the evidence remains negative or flimsy. As 34 reviews originate from China, and as we know about the notorious unreliability of Chinese acupuncture research, this overall result is probably even more negative than the authors make it out to be.
Considering such findings, some people (including the authors of this analysis) feel that we now need more and better acupuncture trials. Yet I wonder whether this is the right approach. Would it not be better to call it a day, concede that acupuncture generates no or only relatively minor effects, and focus our efforts on more promising subjects?
An international team of researchers described retracted papers originating from paper mills, including their characteristics, visibility, and impact over time, and the journals in which they were published. The term paper mill refers to for-profit organizations that engage in the large-scale production and sale of papers to researchers, academics, and students who wish to, or have to, publish in peer-reviewed journals. Many paper mill papers included fabricated data.
All paper mill papers retracted from 1 January 2004 to 26 June 2022 were included in the study. Papers bearing an expression of concern were excluded. Descriptive statistics were used to characterize the sample and analyze the trend of retracted paper mill papers over time, and to analyze their impact and visibility by reference to the number of citations received.
In total, 1182 retracted paper mill papers were identified. The publication of the first paper mill paper was in 2004 and the first retraction was in 2016; by 2021, paper mill retractions accounted for 772 (21.8%) of the 3544 total retractions. Overall, retracted paper mill papers were mostly published in journals of the second highest Journal Citation Reports quartile for impact factor (n=529 (44.8%)) and listed four to six authors (n=602 (50.9%)). Of the 1182 papers, almost all listed authors of 1143 (96.8%) paper mill retractions came from Chinese institutions, and 909 (76.9%) listed a hospital as a primary affiliation. 15 journals accounted for 812 (68.7%) of 1182 paper mill retractions, with one journal accounting for 166 (14.0%). Nearly all (n=1083, 93.8%) paper mill retractions had received at least one citation since publication, with a median of 11 (interquartile range 5-22) citations received.
The authors concluded that papers retracted originating from paper mills are increasing in frequency, posing a problem for the research community. Retracted paper mill papers most commonly originated from China and were published in a small number of journals. Nevertheless, detected paper mill papers might be substantially different from those that are not detected. New mechanisms are needed to identify and avoid this relatively new type of misconduct.
China encourages its researchers to publish papers in return for money and career promotions. Furthermore, medical students at Chinese universities are required to produce a scientific paper in order to graduate. Paper mills openly advertise their services on the Internet and maintain a presence on university campuses. The authors of this analysis reference another recent article (authored by two Chinese researchers) that throws more light on the problem:
This study used data from the Retraction Watch website and from published reports on retractions and paper mills to summarize key features of research misconduct in China. Compared with publicized cases of falsified or fabricated data by authors from other countries of the world, the number of Chinese academics exposed for research misconduct has increased dramatically in recent years. Chinese authors do not have to generate fake data or fake peer reviews for themselves because paper mills in China will do the work for them for a price. Major retractions of articles by authors from China were all announced by international publishers. In contrast, there are few reports of retractions announced by China’s domestic publishers. China’s publication requirements for physicians seeking promotions and its leniency toward research misconduct are two major factors promoting the boom of paper mills in China.
As the authors of the new analysis point out: “Fraudulent papers have negative consequences for the scientific community and the general public, engendering distrust in science, false claims of drug or device efficacy, and unjustified academic promotion, among other problems.” On this blog, I have often warned of research originating from China (some might even think that this is becoming an obsession of mine but I do truly think that this is very important). While such fraudulent papers may have a relatively small impact in many areas of healthcare, their influence in the realm of TCM (where the majority of research comes from China) is considerable. In other words, TCM research is infested by fraud to a degree that prevents drawing meaningful conclusions about the value of TCM treatments.
I feel strongly that it is high time for us to do something about this precarious situation. Otherwise, I fear that in the near future no respectable scientist will take TCM seriously.