
Updated Edition!
 for Cancer")





")









![]()

If I had a £ for each time I was asked during the last few days whether King Charles is going to treat his cancer with homeopathy, I would have my pockets full of cash. The question seems reasonable because he has been singing the praise of homeopathy for decades. But, as I have pointed out previously, he is unlikely to use homeopathy or any other unproven cancer cure; on the contrary he will certainly receive the most effective therapies available today.
In any case, the homeopathic treatment of cancer is currently a most popular topic. As if on command, an article appeared on my screen that promises to address the subject:
“Homoeopathy and Cancer – An Alternative Approach towards the path of Healing”
Here is the abstract of this remarkable paper:
Homoeopathy is a holistic system of medicine rooted on the principle of “Similia Similibus Curentur”. It has gained attention for its potential therapeutic benefits. It offers a holistic approach that addresses both the physical symptoms and emotional well-being of individuals. While this alternative approach of healing has been explored in various health contexts, a notable gap remains in understanding its application in the realm of cancer care. This review seeks to fill this void by exploring the broader landscape of homoeopathy’s principles and applications. Through a critical examination of existing research and evidence, it aims to offer valuable insights into the potential role of homoeopathy as a complementary approach in cancer care and symptomatic relief. This review underscores the need for further research and a more nuanced understanding of homoeopathy’s place in healthcare, particularly in the context of cancer patients and their well-being.
I am sure you are as impressed as I am and keen to learn more. In the article itself, the authors offer some brand-new, cutting-edge science to back up their views:
According to Samuel Hahnemann, “When a person is ill, it is originally merely the spirit-like, autonomic life force (life principle), which is always there in the organism, that is mistuned by the dynamic effect of a morbific agent inimical to life.Only the life principle, tuned incorrectly to such an anomalyis capable of causing irregular functions the body. Cancer may initially be treated as a one-sided disease because the expanded pathology weakens the Vital Force. According to Hahnemann, “Diseases that seem to have just a few symptoms are called one-sided because only one or two prominent symptoms are indicated. This makes these diseases, which primarily fall under the category of chronic diseases, harder to cure. According to Arthur Hill Grimmer, the biggest challenge in treating advanced cancer cases is getting therapeutic individualization of symptoms. Even with all the typical symptoms, it is quite difficult to create a potent homoeopathic prescription. Burnett considered both the characteristic aspects of the patient as well as the ‘action’ or‘organ affinity’ of the remedy he prescribed.
Eventually, the authors (who are affiliated with prestigeous institutions: Rajasthan Ayurved University, Jodhpur; Swasthya Kalyan Homoeopathic Medical College & Research Centre, Jaipur) arrive at the following conclusion:
In the scientific literature, homoeopathy’s use in the treatment of cancer is still largely unexplored. Pioneers have offered intriguing perspectives on disease origins and treatment challenges. The miasmatic perspective offers a distinctive approach that emphasises individualised strategies based on symptoms and characteristics. Some studies suggest an improvement in quality of life of the individuals suffering from cancer. In the dynamic landscape of cancer treatment, more studies are warranted to enhance the scope of holistic, patient-centered care through homoeopathy.
Yes, homeopathy is a joke. This paper (and the many similar publications out there) could thus be intensely funny – except for the fact that these charlatans are playing with the lives of many vulnerable and desperate patients. I sincerely hope Charles manages to stay well clear of homeopathy and its irresponsible practitioners which clearly is one precondition for making a full recovery.
This study tested whether trigger point acupuncture (TrPA) is beneficial for office workers who have reduced job performance (presenteeism) due to chronic neck and shoulder pain (katakori).
A 4-week single-center randomized clinical trial was conducted on 20 eligible female office workers with chronic neck and shoulder pain of at least 3-month duration. The control group implemented only workplace-recommended presenteeism measures, whereas the intervention group received TrPA up to 4 times per month in addition to the presenteeism measures recommended by each workplace. The major outcome measure was the relative presenteeism score on the World Health Organization Health and Work Performance (WHO-HPQ). The secondary outcome measures were pain intensity (numerical rating scale), absolute presenteeism (WHO-HPQ), anxiety and depression (Hospital Anxiety and Depression Scale; HADS), catastrophic thoughts related to pain (Pain Catastrophizing Scale; PCS), and sleep (Athens Insomnia Scale; AIS).
All 9 cases in the intervention group and 11 cases in the control group were analyzed. TrPA up to 4 times per month reduced the intensity of neck and shoulder pain by 20% (P < .01, d = 1.65) and improved labor productivity (relative presenteeism value) by 0.25 (P < .01, d = 1.33) compared with the control group over 1 month. No significant differences were observed between the 2 groups in terms of absolute presenteeism score, HADS, PCS, or AIS.
The authors concluded that these results suggest that regular intervention with TrPA may be effective in the relative presenteeism score before and after the intervention and the degree of neck and shoulder pain over 28 days compared with the control group.
Sure, TrPA may be effective.
But is it?
I thought the trial was aimed at answering that question!
But it didn’t!
Why not?
Because, as we have discussed ad nauseam on this blog, the A+B versus B study design cannot answer it. On the contrary, it will always generate a positive result without determining whether the treatment or a nonspecific (placebo) effect caused the outcome (which, of course, is the reason why this study design is so popular in SCAM research).
In view of this, I suggest to re-formulate the conclusions as follows:
The study suggests that the researchers were ill-informed when designing it. Therefore, the findings show nothing of value.
Yestderday, it was announced that King Charles has cancer. He had been in hospital for surgery for his enlarged prostate. Initially, the news was positive, as it was confirmed not to be prostate cancer. However, during the investigations, a cancer was discovered that apparently is unrelated to the prostate. Since the announcement, many journalists and other people have written to me asking what I think about it and what treatment Charles is likely to receive. I therefore decided to write a short post about the matter.
As a physician and human being I am very sorry whenever I hear that anyone has fallen ill, particularly if the condition is serious and potentially life-threatening. That this includes Charles goes without saying. Equally it is self-evident that I wish that all goes well for him, that the treatment he reportedly has already started is not too arduous, that he keeps in good spirit, that he has empathetic support from all his family and recovers quickly and fully.
Charles will, I am sure, have the best treatment anyone could wish for. Will he use so-called alternative medicine (SCAM), for example, the Gerson therapy, one of the SCAMs he once promoted as a cure of cancer? Of course not! He will receive the most effective, evidence-based care that is currently available. Will he thus not try any SCAM at all? I am confident that he will use SCAM wisely, namely not as a cure but as a supportive measure. In my book on this very subject, I go through all the relevant evidence and conclude that, while SCAM is most certainly not a cancer cure, it can have a place in supportive cancer care. Depending on the symptoms that develop during and after the conventional treatments, certain SCAMs can, according to fairly sound evidence, be helpful in improving wellness and quality of life.
Going through a battle against cancer is often a most humbling experience. Therefore, I am hopeful that, as he recovers from his ordeal, Charles will see that modern medicine – he once described it as being out of balance like the leaning tower of Pisa – is not just effective, empathetic and caring but also not nearly as unbalanced and unholistic as he often proclaimed it to be. In that sense, the experience might reform our king, and – who knows? – he might, after all, turn out to be not the self-proclaimed enemy but a true friend of the Enlightenment.
I have to admit that I came across the ‘ARCIM’ (Academic Research in Complementary and Integrative Medicine) Institute only yesterday when writing the post about Buteyko. Naturally, the institution interested me, and I tried to find out more about it. As pointed out previously, the aim of the ARCIM research institute, founded in 2010, is to research complementary and integrative medicine, in particular anthroposophic medicine, on a scientific basis according to rigorous scientific standards established by the Equator Network criteria (http://www.equator-network.org/).
On the ARCIM’s website we furthermore learn that:
- ARCIM exists since 2010.
- Consists of a team of 8 co-workers.
- Its director is the physician Jan Vagedes.
- Who have published a sizable amount of papers.
- Is funded by the following sponsors: Federal Ministry of Education and Research (BMBF), Mahle-Foundation (Mahle Stiftung), Software AG (Software AG), DAMUS-DONATA e.V.
- Is located in the buildings of the ‘Filderclinic’.
This begs, I think, several questions:
Why is the Federal Ministry of Education and Research sponsoring the ARCIM?
As anthroposophical medicine is based on concepts that fly in the face of science, this seems a legitimate question. Sadly, I have no answer to it.
What is the ‘Filderclinic’?
The Filderklinik in Filderstadt-Bonlanden is one of six anthroposophically orientated hospitals in Germany. It is operated by the non-profit organisation Filderklinik gGmbH. The main founders of the Filderklinik, which has existed since 1975, were Hermann and Ernst Mahle, the founders of the Mahle Group. The Mahle-Stiftung GmbH is the main shareholder and also the largest sponsor of Filderklinik gGmbH. The hospital employs around 915 staff and has 300 beds.
Who is Jan Vagedes?
Jan Vagedes is a specialist for paediatrics and adolescent medicine, neonatology and a doctor for anthroposophic medicine. He studied in and graduated from the LMU in Munich (my alma mater) in 1997. He is the Founder and Scientific Director of the ARCIM Institute, a research associate at the University Children’s Hospital Tübingen, and Head of paediatrics and adolescent medicine at the Filderclinic.
He has no ‘habilitation’ (PhD and in Germany precondition for a professorship). Medline currently lists 42 articles in his name most of which are in 3rd class journals. His first Medline-listed article is dated 2012. As the ARCIM was established in 2010, this means that, when he was appointed as its ‘scientific director’, he had exactly zero published science to his name.
Why did he get the job?
I have absolutely no idea?
(If you know more than I do, I’d be grateful to hear about it.)
The Buteyko techniques (known in Russia as ‘Voluntary Elimination of Deep Breathing’) are treatments to control respiration developed by the Russian Konstantin Buteyko (1923–2003). Inspired by the methods of respiratory control in yoga, the original Buteyko technique was specifically aimed at easing the symptoms of respiratory conditions, particularly asthma. Konstantin Buteyko postulated that there is a connection between hyperventilation and asthma and that it should be possible to reduce asthma symptoms by deliberate breath control.
The Eucapnic Buteyko method is an adaptation of Buteyko’s original technique which was first introduced in Australia and is now used worldwide. It includes the same focus on ventilation control, but the approach has been re-designed with the aim of achieving better patient-compliance. Both treatments and further variations depend crucially on the cooperation of the patient who has to attend long sessions of learning the technique and must follow the somewhat tedious programme rigorously.
A Cochrane review of Buteyko and similar breathing techniques concluded that “there is no credible evidence regarding the effectiveness of breathing exercises for the clinical symptoms of dysfunctional breathing/hyperventilation syndrome. It is currently unknown whether these interventions offer any added value in this patient group or whether specific types of breathing exercise demonstrate superiority over others.”
Now, a new study adds to this knowledge. This randomized clinical trial included two groups (n = 30 each) of patients with asthma. They received either:
- Buteyko breathing technique (BBT) together with usual therapy (UT)
- or UT alone over a period of 3 months.
The primary outcome comprised the voluntary control pause (CP) after 3 months, secondary outcomes an additional breathhold parameter, forced expiratory volume in 1 s (FEV1), capnovolumetry, exhaled nitric oxide (FeNO), Asthma Control Questionnaire (ACQ) and Nijmegen Questionnaire (NQ), and the use of medication (β2-agonists; inhaled corticosteroids, ICS).
CP showed significant time-by-group interaction [F(1,58.09) = 28.70, p < 0.001] as well as main effects for study group [F(1,58.27) = 5.91, p = 0.018] and time [F(1,58.36) = 17.67, p < 0.001]. ACQ and NQ scores were significantly (p < 0.05 each) improved with BBT. This was associated with reductions in the use of β2-agonists and ICS (p < 0.05 each) by about 20% each. None of these effects occurred in the UT group. While FEV1 and the slopes of the capnovolumetric expiratory phases 2 and 3 did not significantly change, the capnovolumetric threshold volume at tidal breathing increased (p < 0.05) with BBT by about 10 mL or 10%, compared to baseline, suggesting a larger volume of the central airways. No significant changes were seen for FeNO.
The authors concluded that BBT was clinically effective, as indicated by the fact that the improvement in symptom scores and the small increase in bronchial volume occurred despite the significant reduction of respiratory pharmacotherapy. As the self-controlled Buteyko breathing therapy was well-accepted by the participants, it could be considered as supporting tool in asthma therapy being worth of wider attention in clinical practice.
I disagree with this conclusion and think it ought to be changed to:
BBT or a placebo effect was clinically effective.
The reason is that, as many readers have heard me say before, the infamous A+B versus B design does not control for placebo effects and thus is guaranteed to produce a positive result.
The research was conducted by an international team evidently led by the relatively new ARCIM Institute which claims on its website:
The acronym ARCIM stands for Academic Research in Complementary and Integrative Medicine.
The bridging between different treatment and research approaches, disciplines and ways of thinking achieved by the research work of the ARCIM Institute can be symbolized by our logo’s bridge arch. ARCIM integrates this bridge-building metaphor within its name since the Latin term “arcus” means “arch” or “bridge.”
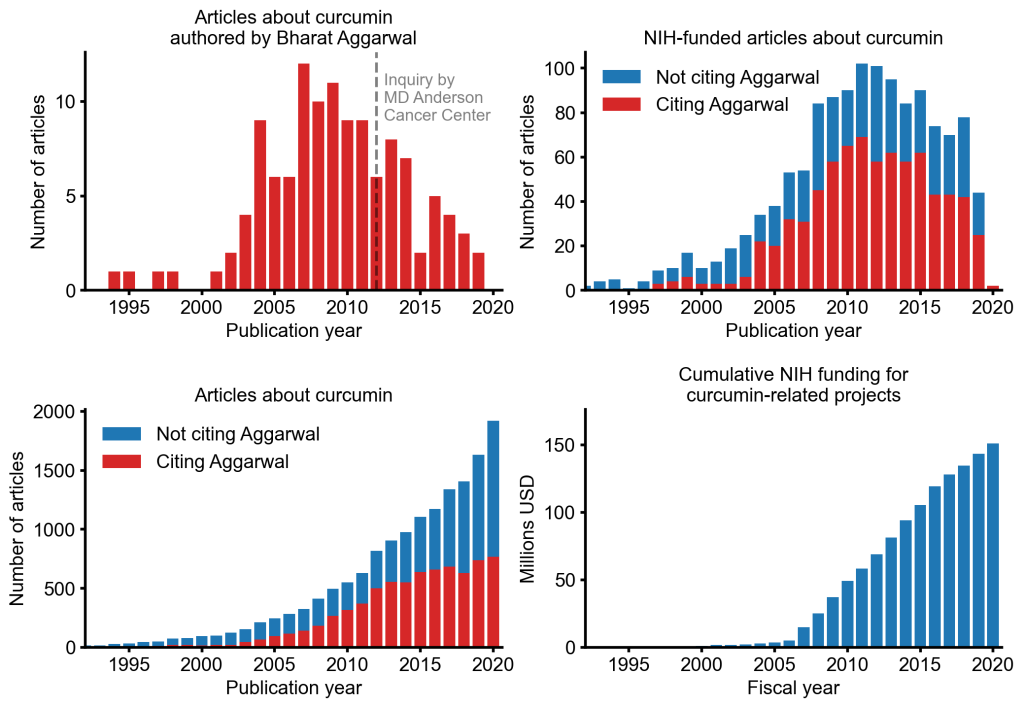
An alarming story of research fraud in the area of so-called alternative medicine (SCAM) is unfolding: Bharat B. Aggarwal, the Indian-American biochemist who worked at MD Anderson Cancer Center, focused his research on curcumin, a compound found in turmeric, and authored more than 125 Medline-listed articles about it. They reported that curcumin had therapeutic potential for a variety of diseases, including various cancers, Alzheimer’s disease and, more recently, COVID-19.
The last of these papers, entitled “Curcumin, inflammation, and neurological disorders: How are they linked?”, was publiched only a few months ago. Here is its abstract:
Background: Despite the extensive research in recent years, the current treatment modalities for neurological disorders are suboptimal. Curcumin, a polyphenol found in Curcuma genus, has been shown to mitigate the pathophysiology and clinical sequalae involved in neuroinflammation and neurodegenerative diseases.
Methods: We searched PubMed database for relevant publications on curcumin and its uses in treating neurological diseases. We also reviewed relevant clinical trials which appeared on searching PubMed database using ‘Curcumin and clinical trials’.
Results: This review details the pleiotropic immunomodulatory functions and neuroprotective properties of curcumin, its derivatives and formulations in various preclinical and clinical investigations. The effects of curcumin on neurodegenerative diseases such as Alzheimer’s disease (AD), amyotrophic lateral sclerosis (ALS), brain tumors, epilepsy, Huntington’s disorder (HD), ischemia, Parkinson’s disease (PD), multiple sclerosis (MS), and traumatic brain injury (TBI) with a major focus on associated signalling pathways have been thoroughly discussed.
Conclusion: This review demonstrates curcumin can suppress spinal neuroinflammation by modulating diverse astroglia mediated cascades, ensuring the treatment of neurological disorders.
The Anderson Cancer Center initially appeared to approve of Aggarwal’s work. However, in 2012, following concerns about image manipulation raised by pseudonymous sleuth Juuichi Jigen, MD Anderson Cancer Center launched a research fraud probe against Aggarwal which eventually led to 30 of Aggarwal’s articles being retracted. Moreover, PubPeer commenters have noted irregularities in many publications beyond the 30 that have already been retracted. Aggarwal thus retired from M.D. Anderson in 2015.
Curcumin doesn’t work well as a therapeutic agent for any disease – see, for instance, the summary from Nelson et al. 2017:
“[No] form of curcumin, or its closely related analogues, appears to possess the properties required for a good drug candidate (chemical stability, high water solubility, potent and selective target activity, high bioavailability, broad tissue distribution, stable metabolism, and low toxicity). The in vitro interference properties of curcumin do, however, offer many traps that can trick unprepared researchers into misinterpreting the results of their investigations.”
Despite curcumin’s apparent lack of therapeutic promise, the volume of research produced on curcumin grows each year. More than 2,000 studies involving the compound are now published annually. Many of these studies bear signs of fraud and involvement of paper mills. As of 2020, the United States National Institutes of Health (NIH) has spent more than 150 million USD funding projects related to curcumin.
This proliferation of research has fueled curcumin’s popularity as a dietary supplement. It is estimated that the global market for curcumin as a supplement is around 30 million USD in 2020.
The damage done by this epic fraud is huge and far-reaching. Hundreds of millions of taxpayer dollars, countless hours spent toiling by junior scientists, thousands of laboratory animals sacrificed, thousands of cancer patients enrolled in clinical trials for ineffective treatments, and countless people who have eschewed effective cancer treatment in favor of curcumin, were encouraged by research steeped in lies.
Getting old is not nice – but think of the alternative!
I think it was Woody Allen who said something to that extent. But there is a third way, at least this is waht Tai Chi advocates want us to believe.
Utilizing a hybrid design, this study aimed to test whether both long-term and short-term Tai Chi (TC) training are associated with age-related decline in physical function in healthy older adults.
The authors first conducted cross-sectional comparisons among TC-naïve older adults (n = 60, 64.2 ± 7.7 years), TC-expert older adults (n = 27, 62.8 ± 7.6 years, 24.5 ± 12 years experience), and TC-naïve younger adults (n = 15, 28.7 ± 3.2 years) to inform long-term effects of TC training on physical function, including single leg stance time with eyes closed, grip strength, Timed Up and Go, maximum walking speed, functional reach, and vertical jump for lower-extremity power. There were significant differences among the three groups on all the six tests. For most functional tests, TC-experts performed better than age-matched TC-naïve controls and were statistically indistinguishable from young healthy adult controls. Long-term TC training was associated with higher levels of physical function in older adults, suggesting a potential preventative healthy aging effect.
In the randomized longitudinal trial, TC-naïve subjects were randomized (n = 31 to Tai Chi group, n = 29 to usual care control group) to evaluate the short-term effects of TC over 6 months on all outcomes. TC’s short-term impacts on physical function were small and not statistically significant. The impact of short-term training in healthy adults is less clear.
The authors concluded that both potential longer-term preventive effects and shorter-term restorative effects warrant further research with rigorous, adequately powered controlled clinical trials.
Even though the authors imply that their cross-sectional comparison points to a causal effect, this is clearly not true. For instance, it could easily be that people who are somehow destined to keep fit and agile are the ones who keep up Tai Chi. So, rather than being the result of Tai Chi, the proneness to fitness and agility could be the cause for doing Tai Chi.
The authors laudably were aware of these problems and therefore also did an RCT. Sadly this RCT did not yield significant findings. Essentially this means that eitherTai Chi did not work, or the study was naively inadequate, e.g. too small and too short-term.
Thus the authors finish with the usual statement that MORE RESEARCH IS NEEDED. This might be true, but is a definitive RCT likely?
I don’t think so.
A long time ago I had designed such a definitive study. It needed to be very large considering that many participants might drop out. Crucially, it also had to be long- term, i.e. years, not months.
And what happened to my study?
I never managed to get it funded, mainly because the costs would have been astronomical.
Supportive care is often assumed to be beneficial in managing the anxiety symptoms common in patients in sterile hematology unit. The authors of this study hypothesize that personal massage can help the patient, particularly in this isolated setting where physical contact is extremely limited.
The main objective of this study therefore was to show that anxiety could be reduced after a touch-massage performed by a nurse trained in this therapy.
A single-center, randomized, unblinded controlled study in the sterile hematology unit of a French university hospital, validated by an ethics committee. The patients, aged between 18 and 65 years old, and suffering from a serious and progressive hematological pathology, were hospitalized in sterile hematology unit for a minimum of three weeks. They were randomized into either a group receiving 15-minute touch-massage sessions or a control group receiving an equivalent amount of quiet time once a week for three weeks.
In the treated group, anxiety was assessed before and after each touch-massage session, using the State-Trait Anxiety Inventory questionnaire with subscale state (STAI-State). In the control group, anxiety was assessed before and after a 15-minute quiet period. For each patient, the difference in the STAI-State score before and after each session (or period) was calculated, the primary endpoint was based on the average of these three differences. Each patient completed the Rosenberg Self-Esteem Questionnaire before the first session and after the last session.
Sixty-two patients were randomized. Touch-massage significantly decreased patient anxiety: a mean decrease in STAI-State scale score of 10.6 [7.65-13.54] was obtained for the massage group (p ≤ 0.001) compared with the control group. The improvement in self-esteem score was not significant.
The authors concluded that this study provides convincing evidence for integrating touch-massage in the treatment of patients in sterile hematology unit.
I find this conclusion almost touching (pun intended). The wishful thinking of the amateur researchers is almost palpable.
Yes, I mean AMATEUR, despite the fact that, embarrassingly, the authors are affiliated with prestigeous institutions:
- 1Nantes Université, CHU Nantes, Service Interdisciplinaire Douleur, Soins Palliatifs et de Support, Médecine intégrative, UIC 22, Nantes, F-44000, France.
- 2Université Paris Est, EA4391 Therapeutic and Nervous Excitability, Creteil, F-93000, France.
- 3Nantes Université, CHU Nantes, Hematology Department, Nantes, F-44000, France.
- 4Nantes Université, CHU Nantes, CRCI2NA – INSERM UMR1307, CNRS UMR 6075, Equipe 12, Nantes, F-44000, France.
- 5Institut Curie, Paris, France.
- 6Université Paris Versailles Saint-Quentin, Versailles, France.
- 7Nantes Université, CHU Nantes, Direction de la Recherche et l’Innovation, Coordination Générale des Soins, Nantes, F-44000, France.
- 8Methodology and Biostatistics Unit, DRCI CHU Nantes CHD Vendée, La Roche Sur Yon, F-85000, France.
- 9Nantes Université, CHU Nantes, Service Interdisciplinaire Douleur, Soins Palliatifs et de Support, Médecine intégrative, UIC 22, Nantes, F-44000, France. [email protected].
So, why do I feel that they must be amateurs?
- Because, if they were not amateurs, they would know that a clinical trial should not aim to show something, but to test something.
- Also, if they were not amateurs, they would know that perhaps the touch-massage itself had nothing to do with the outcome, but that the attention, sympathy and empathy of a therapist or a placebo effect can generate the observed effect.
- Lastly, if they were not amateurs, they would not speak of convincing evidence based on a single, small, and flawed study.
After the nationwide huha created by the BBC’s promotion of auriculotherapy and AcuSeeds, it comes as a surprise to learn that, in Kent (UK), the NHS seems to advocate and provide this form of quackery. Here is the text of the patient leaflet:
Kent Community Health, NHS Foundation Trust
Auriculotherapy
This section provides information to patients who might benefit from auriculotherapy, to complement their acupuncture treatment, as part of their chronic pain management plan.
What is auriculotherapy?
In traditional Chinese medicine, the ear is seen as a microsystem representing the entire body. Auricular acupuncture focuses on ear points that may help a wide variety of conditions including pain. Acupuncture points on the ear are stimulated with fine needles or with earseeds and massage (acupressure).
How does it work?
Recent research has shown that auriculotherapy stimulates the release of natural endorphins, the body’s own feel good chemicals, which may help some patients as part of their chronic pain management plan.
What are earseeds?
Earseeds are traditionally small seeds from the Vaccaria plant, but they can also be made from different types of metal or ceramic. Vaccaria earseeds are held in place over auricular points by a small piece of adhesive tape, or plaster. Applying these small and barely noticeable earseeds between acupuncture treatments allows for patient massage of the auricular points. Earseeds may be left in place for up to a week.
Who can use earseeds?
Earseeds are sometimes used by our Chronic Pain Service to prolong the effects of standard acupuncture treatments and may help some patients to self manage their chronic pain.
How can I get the most out my treatment with earseeds?
It is recommended that the earseeds are massaged two to three times a day or when symptoms occur by applying gentle pressure to the earseeds and massaging in small circles.
Will using earseeds cure my chronic pain?
As with any treatment, earseeds are not a cure but they can reduce pain levels for some patients as part of their chronic pain management programme.
________________________
What the authors of the leaflet forgot to tell the reader is this:
- Auriculotherapy is based on ideas that fly in the face of science.
- The evidence that auriculotherapy works is flimsy, to say the least.
- The evidence earseeds work is even worse.
- To arrive at a positive recommendation, the NHS had to heavily indulge in the pseudo-scientific art of cherry-picking.
- The positive experience that some patients report is due to a placebo response.
- For whichever condition auriculotherapy is used, there are treatments that are much more adequate.
- Advocating auriculotherapy is therefore not in the best interest of the patient.
- Arguably, it is unethical.
- Definitely, it is not what the NHS should be doing.
- an immediate osteopathic manipulative therapy (OMT) intervention group,
- a delayed OMT (waiting period) group.
The intervention consisted of three to four OMT sessions over 4–6 weeks, after which the participants switched (crossed-over) groups. The OMT techniques included a mandatory HVLA thrust technique to the lumbar spine region and any (or none) combination of the following four techniques: (i) soft tissue, (ii) muscle energy, (iii) myofascial, and (iv) articulatory. For patients who could not tolerate the HVLA treatment, a physician had to attempt this technique, minimally by attempting to place the patient in the position to perform this maneuver.
The primary clinical outcomes were average pain, current pain, Patient-Reported Outcomes Measurement Information System (PROMIS) 29 v1.0 pain interference and physical function, and modified Oswestry Disability Index (ODI). Secondary outcomes included the remaining PROMIS health domains and the Fear Avoidance Beliefs Questionnaire (FABQ). These measures were taken at baseline (T0), after one OMT session (T1), at the crossover point (T2), and at the end of the trial (T3). Due to the carryover effects of OMT intervention, only the outcomes obtained prior to T2 were evaluated utilizing mixed-effects models and after adjusting for baseline values.
- This study is far too small to allow conclusions about safety.
- The trial compared OMT with no therapy; it is likely that the observed outcomes have little to do with OMT but are due to a placebo response.
- The primary outcome measure showed no effect which essentially means that the study finding was that OMT is ineffective.
My conclusion:
a poor study conducted by wishful thinkers.