
Updated Edition!
 for Cancer")





")









![]()

I know, I have reported about the risks of chiropractic manipulations many times before. But I will continue to do so, because the subject is important and mentioning it might save lives.
The purpose of this study from the US was to determine the frequency of patients seen at a single institution who were diagnosed with a cervical vessel dissection related to chiropractic neck manipulation. The researchers identified cases through a retrospective chart review of patients seen between April 2008 and March 2012 who had a diagnosis of cervical artery dissection following a recent chiropractic manipulation. Relevant imaging studies were reviewed by a board-certified neuroradiologist to confirm the findings of a cervical artery dissection and stroke. The investigators also conducted telephone interviews to ascertain the presence of residual symptoms in the affected patients.
Of the 141 patients with cervical artery dissection, 12 had documented chiropractic neck manipulation prior to the onset of the symptoms that led to medical presentation. The 12 patients had a total of 16 cervical artery dissections. All 12 patients developed symptoms of acute stroke. All strokes were confirmed with magnetic resonance imaging or computerized tomography. The researchers obtained follow-up information on 9 patients, 8 of whom had residual symptoms and one of whom died as a result of his injury.
The authors concluded that, in this case series, 12 patients with newly diagnosed cervical artery dissection(s) had recent chiropractic neck manipulation. Patients who are considering chiropractic cervical manipulation should be informed of the potential risk and be advised to seek immediate medical attention should they develop symptoms.
Cerebellar and spinal cord injuries related to cervical chiropractic manipulation were first reported in 1947. By 1974, there were 12 reported cases. Non-invasive imaging has since greatly improved the diagnosis of cervical artery dissection and of stroke, and cervical artery dissection is now recognized as pathogenic of strokes occurring in association with chiropractic manipulation.
The authors also point out that another institution had previously described 13 stroke cases after chiropractic manipulation. The patients at both institutions were relatively young and incurred substantial residual morbidity. A single patient at each institution died. If these findings are representative of other institutions across the United States, the incidence of stroke secondary to chiropractic manipulation may be higher than supposed. To assess this problem further, a randomized prospective cohort study could establish the relative risk of chiropractic manipulation of the cervical spine resulting in a cervical artery dissection. But such a study may be methodologically prohibitive. More feasible would be a case-control study in which patients who had experienced cervical artery dissection were matched with subjects who had not incurred such injuries. Comparing the groups’ odds of having received chiropractic manipulation demonstrated that spinal manipulative therapy is an independent risk factor for vertebral artery dissection and is highly suggestive of a causal association.
I very much agree with the authors when they sate that until the actual level of risk from chiropractic manipulation is known, patients with neck pain may be better served by equally effective passive physical therapy exercises.
In other words: there is very little reason to recommend chiropractic care for neck pain (or any other condition).
Kinesiology tape KT is fashionable, it seems. Gullible consumers proudly wear it as decorative ornaments to attract attention and show how very cool they are.
Am I too cynical?
Perhaps.
But does KT really do anything more?
A new trial might tell us.
The aim of this study was to investigate whether adding kinesiology tape (KT) to spinal manipulation (SM) can provide any extra effect in athletes with chronic non-specific low back pain (CNLBP).
Forty-two athletes (21males, 21females) with CNLBP were randomized into two groups of SM (n = 21) and SM plus KT (n = 21). Pain intensity, functional disability level and trunk flexor-extensor muscles endurance were assessed by Numerical Rating Scale (NRS), Oswestry pain and disability index (ODI), McQuade test, and unsupported trunk holding test, respectively. The tests were done before and immediately, one day, one week, and one month after the interventions and compared between the two groups.
After treatments, pain intensity and disability level decreased and endurance of trunk flexor-extensor muscles increased significantly in both groups. Repeated measures analysis, however, showed that there was no significant difference between the groups in any of the evaluations.
The authors, physiotherapists from Iran, concluded that the findings of the present study showed that adding KT to SM does not appear to have a significant extra effect on pain, disability and muscle endurance in athletes with CNLBP. However, more studies are needed to examine the therapeutic effects of KT in treating these patients.
Regular readers of my blog will be able to predict what I have to say about this study design: A+B versus B is not a meaningful test of anything. I used to claim that it cannot possibly produce a negative result – and yet, here it seems to have done exactly that!
How come?
The way I see it, there are two possibilities to explain this:
- the KT has a mildly negative effect on CNLBP; thus the expected positive placebo-effect was neutralised to result in a null-effect overall;
- the study was under-powered such that the true inter-group difference could not manifest itself.
I think the second possibility is more likely, but it does really not matter at all. Because the only lesson we can learn from this trial is this: inadequate study designs will hardly ever generate anything worthwhile.
And this is, I think, a lesson that would be valuable for many researchers.
_______________________________________________________________________
Reference
Comparing spinal manipulation with and without Kinesio Taping® in the treatment of chronic low back pain.
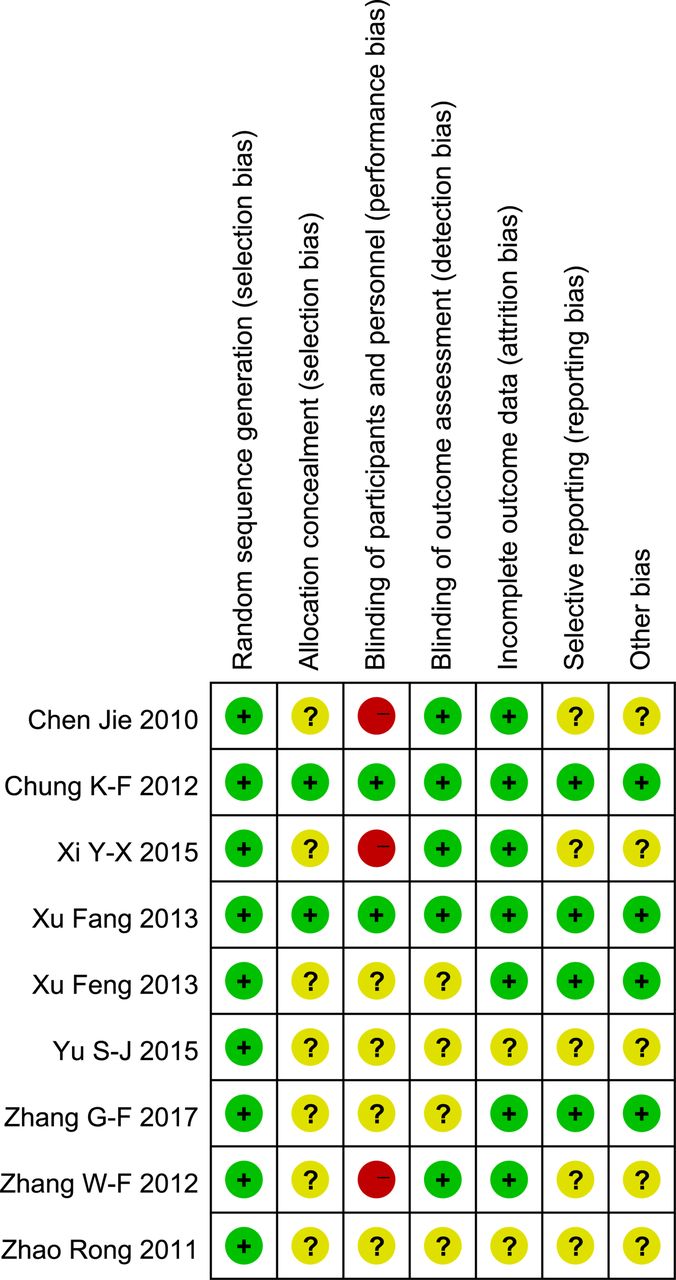
I have often cautioned my readers about the ‘evidence’ supporting acupuncture (and other alternative therapies). Rightly so, I think. Here is yet another warning.
This systematic review assessed the clinical effectiveness of acupuncture in the treatment of postpartum depression (PPD). Nine trials involving 653 women were selected. A meta-analysis demonstrated that the acupuncture group had a significantly greater overall effective rate compared with the control group. Moreover, acupuncture significantly increased oestradiol levels compared with the control group. Regarding the HAMD and EPDS scores, no difference was found between the two groups. The Chinese authors concluded that acupuncture appears to be effective for postpartum depression with respect to certain outcomes. However, the evidence thus far is inconclusive. Further high-quality RCTs following standardised guidelines with a low risk of bias are needed to confirm the effectiveness of acupuncture for postpartum depression.
What a conclusion!
What a review!
What a journal!
What evidence!
Let’s start with the conclusion: if the authors feel that the evidence is ‘inconclusive’, why do they state that ‘acupuncture appears to be effective for postpartum depression‘. To me this does simply not make sense!
Such oddities are abundant in the review. The abstract does not mention the fact that all trials were from China (published in Chinese which means that people who cannot read Chinese are unable to check any of the reported findings), and their majority was of very poor quality – two good reasons to discard the lot without further ado and conclude that there is no reliable evidence at all.
The authors also tell us very little about the treatments used in the control groups. In the paper, they state that “the control group needed to have received a placebo or any type of herb, drug and psychological intervention”. But was acupuncture better than all or any of these treatments? I could not find sufficient data in the paper to answer this question.
Moreover, only three trials seem to have bothered to mention adverse effects. Thus the majority of the studies were in breach of research ethics. No mention is made of this in the discussion.
In the paper, the authors re-state that “this meta-analysis showed that the acupuncture group had a significantly greater overall effective rate compared with the control group. Moreover, acupuncture significantly increased oestradiol levels compared with the control group.” This is, I think, highly misleading (see above).
Finally, let’s have a quick look at the journal ‘Acupuncture in Medicine’ (AiM). Even though it is published by the BMJ group (the reason for this phenomenon can be found here: “AiM is owned by the British Medical Acupuncture Society and published by BMJ”; this means that all BMAS-members automatically receive the journal which thus is a resounding commercial success), it is little more than a cult-newsletter. The editorial board is full of acupuncture enthusiasts, and the journal hardly ever publishes anything that is remotely critical of the wonderous myths of acupuncture.
My conclusion considering all this is as follows: we ought to be very careful before accepting any ‘evidence’ that is currently being published about the benefits of acupuncture, even if it superficially looks ok. More often than not, it turns out to be profoundly misleading, utterly useless and potentially harmful pseudo-evidence.
Reference
Acupunct Med. 2018 Jun 15. pii: acupmed-2017-011530. doi: 10.1136/acupmed-2017-011530. [Epub ahead of print]
Effectiveness of acupuncture in postpartum depression: a systematic review and meta-analysis.
Li S, Zhong W, Peng W, Jiang G.
It has been shown repeatedly that a ‘conspiracy mentality’ is associated with usage of alternative medicine. But perhaps alternative medicine is itself a conspiracy theory in disguise?
One of the questions I invariably get after a public lecture is the one about alternative medicine being the victim of some sort of sinister plot. This notion can take various shapes and forms:
- The scientific establishment prevents the public from fully benefitting from the effects of alternative medicine.
- The pharmaceutical industry suppresses the good news about alternative treatments.
- The funding agencies refuse to fund research into alternative medicine.
- The media are bent on defaming alternative medicine.
- The regulators do not allow alternative medicine to thrive as much as it would deserve.
- The medical profession is afraid that the benefits of alternative medicine become better known.
I could go on, but I am sure you get the picture.
The amazing thing is that I hear such arguments not just from fanatic proponents of alternative medicine, but also from more reasonable people. These sentiments seem to be entirely common and seemingly logical arguments. Most people I meet seem to believe them at least to some degree.
Having heard them so often, I do wonder: Can one explain alternative medicine as a conspiracy theory?
A conspiracy theory is an erroneous and often difficult to falsify notion that tries to explain a set of circumstances as the result of a secret plot by usually powerful conspirators, while ignoring obvious alternative explanations. The very concept of alternative medicine assumes that there are valuable therapies that conventional healthcare does not allow in its realm.
The reasons for the secret plot that prevents them to be included in conventional healthcare are rarely named by enthusiasts of alternative medicine. So, what are they?
- Professional jealousy?
- Financial interests?
- Lack of interest?
- Lack of caring?
According to proponents of alternative medicine who I have asked, they consist of a mixture of all of these possibilities. And all of these possibilities are, in a way, consistent with alternative medicine being based on a conspiracy theory.
When I ask people why they believe in these theories, they cannot produce any solid evidence for their beliefs. This does not surprise me because, as far as I can see, there is no evidence to support them: they are erroneous. In turn, this means that one important criterium for conspiracy theory is being met.
Another characteristic of conspiracy theories is that they cannot easily been proven to be false. None of the above-listed reasons are, in fact, difficult to falsify.
A final characteristic of conspiracy theories is that its proponents are ignoring obvious alternative explanations.
WHY ARE ALTERNATIVE THERAPIES NOT ADMITTED INTO THE REALM OF CONVENTIONAL MEDICINE?
Simply because they are not supported by sufficiently strong evidence for generating more good than harm.
So, yes, to some extent alternative medicine even is a conspiracy theory in disguise.
How often do we hear this sentence: “I know, because I have done my research!” I don’t doubt that most people who make this claim believe it to be true.
But is it?
What many mean by saying, “I know, because I have done my research”, is that they went on the internet and looked at a few websites. Others might have been more thorough and read books and perhaps even some original papers. But does that justify their claim, “I know, because I have done my research”?
The thing is, there is research and there is research.
The dictionary defines research as “The systematic investigation into and study of materials and sources in order to establish facts and reach new conclusions.” This definition is helpful because it mentions several issues which, I believe, are important.
Research should be:
- systematic,
- an investigation,
- establish facts,
- reach new conclusions.
To me, this indicates that none of the following can be truly called research:
- looking at a few randomly chosen papers,
- merely reading material published by others,
- uncritically adopting the views of others,
- repeating the conclusions of others.
Obviously, I am being very harsh and uncompromising here. Not many people could, according to these principles, truthfully claim to have done research in alternative medicine. Most people in this realm do not fulfil any of those criteria.
As I said, there is research and research – research that meets the above criteria, and the type of research most people mean when they claim: “I know, because I have done my research.”
Personally, I don’t mind that the term ‘research’ is used in more than one way:
- there is research meeting the criteria of the strict definition
- and there is a common usage of the word.
But what I do mind, however, is when the real research is claimed to be as relevant and reliable as the common usage of the term. This would be a classical false equivalence, akin to putting experts on a par with pseudo-experts, to believing that facts are no different from fantasy, or to assume that truth is akin to post-truth.
Sadly, in the realm of alternative medicine (and alarmingly, in other areas as well), this is exactly what has happened since quite some time. No doubt, this might be one reason why many consumers are so confused and often make wrong, sometimes dangerous therapeutic decisions. And this is why I think it is important to point out the difference between research and research.
The following announcement was made by the NHS on 7 August 2018:
The Governing Body of Bristol, North Somerset and South Gloucestershire (BNSSG) Clinical Commissioning Group (CCG) today approved changes that mean NHS funded homeopathy will only be available in exceptional circumstances in the area. The changes will mean the CCG’s Individual Funding Request (IFR) Panel would need a clinician to set out why the patient is clinically exceptional before treatment could be provided.
The decision comes after the publication of a report, which took evidence from local people, clinicians, patient groups, providers of homeopathic treatments and national guidelines.
CCG Clinical Chair Dr Jonathan Hayes said, “We are working hard to become an evidence-informed organisation because we need to make the best use of all resources to offer treatment and care to the widest range of people. The decision on homeopathy funding today is a step towards this and brings us in line with national guidelines.”
It is estimated that 41 patients receiving NHS funded homeopathic consultations in the area cost the local NHS £109,476 in the 2017/2018 financial year.
END OF QUOTE

The move is the result of 4 years of excellent work by the GOOD THINKING SOCIETY, a charity dedicate to the promotion of rational thinking.
Michael Marshall, its Project Director, said: “We are very pleased to see the Bristol CCGs take this decision to cease funding for homeopathy – every other CCG across the country has made it clear that homeopathic remedies are no better than placebo and such there is simply no place for homeopathy on the NHS.
“With the end to homeopathy funding in Bristol, the region joins NHS bodies across the rest the country in recognising that homeopathy is not a valid use of limited NHS resources. There is now no CCG in England where homeopathic pills or consultations can be routinely funded with NHS money – instead, funding can be directed towards treatments that have been shown to actually work.”
Does that not call for a knighthood for Mr Marshall?
One would have thought so!
Who will tell Prince Charles to get the ball rolling?
And while we are all waiting for the big event, you might as well donate a few £s to this truly splendid charity.
Please be generous!!!
We probably have all heard of predatory journals. The phenomenon of ‘predatory conferences’ seems to be less-well appreciated. Hardly a day goes by that I do not receive emails like the one below:
________________________________________________________
Dear Dr. E Ernst ,
Good day!
After the success of Traditional Medicine-2018 in Rome, Italy, on behalf of the Organizing committee, we are delighted to invite you to be a speaker at our upcoming “3rd World Congress and Expo on Traditional and Alternative Medicine” (Traditional Medicine-2019) which will be held during June 06-08, 2019 in Berlin, Germany.
Traditional Medicine-2019 will focus on the theme “Natural and Scientific Approach for Treatment and Rehabilitation”…
_________________________________________________________
I have chosen this particular one because it refers to the success of a recent conference in Rome. This is a conference where I was a member of the organising committee and have been listed as a keynote speaker. Here is the original entry from the programme:
Keynote Forum 09:15-09:55
Title: Integrative Medicine: Hype or Hope? Ernst Edzard, University of Exeter, United Kingdom
And here is the strange tale how it all came about:
After receiving a barrage of similar invitations and having ignored them for months, I thought that maybe I am unnecessarily suspicious – perhaps these conferences are not as dodgy as they appear to be. So, I responded to one email and stated the usual things:
- I do not insist on a fee,
- I want my expensed paid,
- I need a topic that I feel comfortable with,
- I need to know who else is speaking,
- I must know who is sponsoring the event,
- the whole thing must fit into my time-table.
I got an enthusiastic response and, even though not all my questions were answered, they agreed to fund my travel and hotel costs with a lump sum of 300 Euro. They asked me to act as chair of the entire meeting and as ‘signing authority for the conference’ (I don’t know what this means) but I declined. Yet I wanted to see how the whole thing would play out. So, I accepted a keynote lecture, agreed to be a member of the organising/scientific committee, and send them my abstract.
Then I did not hear anything for a long time (normally, I would, as a member of the organising/scientific committee, have expected to receive abstract submissions for review and other material). When someone sent me an email about it, I noted that the organisers were advertising the conference with my name and photo. I was irritated by that, but decided to play along so that I could get to the bottom of all this. Then, about 6 weeks before the event came this email from the organisers:
Dear Dr. Ernst ,
Greetings of the day!!
We are glad to have your presence at Traditional Medicine 2018.
Hope this mail finds you in good spirits.
Kindly find the attached final program for the Conference.
Could you please confirm us your check in & check out dates.
Revert back to me for further queries…
I replied as follows:
I will look at the possibilities of trains, flights etc., once you send me the promised funds for buying my tickets.
e ernst
________________________________________________________
And the rest was silence!
I did not hear a word from them after telling them that they need to send me the money before I commit myself into buying flight tickets etc. Nor did I expect to hear from them after that.
The run-up to the conference was too bizarre, in my view, for a credible conference:
- The organisers seemed to know next to nothing about the topic of the conference.
- They signed with English names and had a London address, but their language skills seem to be limited.
- They had few of the features that are typical for a serious conference.
- Almost all of their emails seemed strangely vague.
- I got the impression that the entire organisation is not run by a thinking person but by a computer.
- They seemed to organise dozens of conferences at any one time.
- All their conferences were in towns that might seem attractive to visit.
- None were associated with a leading scientist’s place of work.
- They wanted my commitments but never committed themselves to anything tangible.
In a word, they seemed phony!
Of course, in the end, I did not fly to Rome and did not deliver my keynote lecture. Evidently, this did not stop them to email me soon after stating “After the success of Traditional Medicine-2018in Rome, Italy, on behalf of the Organizing committee…”
The reason for writing this is to warn you: there are obviously quite a few (not so) clever people out there who want to get hold of your cash by tempting you to attend an apparently interesting conference in an attractive town which, once you participate, turns out to be a waste of time, money and effort.
They say that minds are like parachutes – they function only when open. Having an open mind means being receptive to new and different ideas or the opinions of others.
I am regularly accused of lacking this quality. Most recently, an acupuncturist questioned whether acupuncture-sceptics, and I in particular, have an open mind. Subsequently, an interesting dialogue ensued:
___________________________________________________________
Tom Kennedy on Wednesday 01 August 2018 at 19:27
the EVIDENCEBASEDACUPUNCTURE site you recommend quotes the Vickers meta-analysis thus:
“A meta-analysis of 17,922 patients from randomized trials concluded, “Acupuncture is effective for the treatment of chronic pain and is therefore a reasonable referral option. Significant differences between true and sham acupuncture indicate that acupuncture is more than a placebo.”
Pity that they forgot a bit. The full conclusion reads:
“Acupuncture is effective for the treatment of chronic pain and is therefore a reasonable referral option. Significant differences between true and sham acupuncture indicate that acupuncture is more than a placebo. However, these differences are relatively modest, suggesting that factors in addition to the specific effects of needling are important contributors to the therapeutic effects of acupuncture.”
AND YOU TRY TO LECTURE US ABOUT AN OPEN MIND?
@Edzard I’m not sure I understand your point. ‘However, these differences are relatively modest, suggesting that factors in addition to the specific effects of needling are important contributors to the therapeutic effects of acupuncture.’ Perhaps the full conclusion should always be quoted, but I don’t think that addendum changes the context significantly. Acupuncture has been shown to be more than a placebo in a large meta-analysis (when compared to arguably active sham controls). The authors put it well I think, in the ‘Interpretation’ section:
‘Our finding that acupuncture has effects over and above sham acupuncture is therefore of major importance for clinical practice. Even though on average these effects are small, the clinical decision made by doctors and patients is not between true and sham acupuncture, but between a referral to an acupuncturist or avoiding such a referral. The total effects of acupuncture, as experienced by the patient in routine practice, include both the specific effects associated with correct needle insertion according to acupuncture theory, non-specific physiologic effects of needling, and non-specific psychological (placebo) effects related to the patient’s belief that treatment will be effective.’
Compare this to Richard’s comment here, for example: ‘Of course the effects of ‘acupuncture’ (if any) are due to placebo responses (and perhaps nocebo responses in some cases). What else?’. And your post tile includes the line ‘the effects of acupuncture are due to placebo’. These are the kinds of comment that to me seem closed-minded in the face of some significant evidence.
edzard on Thursday 02 August 2018 at 12:46
“Perhaps the full conclusion should always be quoted…”
YES, IF NOT, IT’S CALLED ‘BEING ECONOMICAL WITH THE TRUTH’
“…I don’t think that addendum changes the context significantly.”
IT’S NOT AN ADDENDUM, BUT PART OF THE CONCLUSION; AND YOU ARE WRONG, FOR ME, IT CHANGES A LOT.
“…your post tile includes the line ‘the effects of acupuncture are due to placebo’.”
BECAUSE THIS IS WHAT THE PAPER DISCUSSED IN THAT PARTICULAR POST IMPLIED.
‘IT’S CALLED ‘BEING ECONOMICAL WITH THE TRUTH’’
The title of this post is: ‘Yet another confirmation: the effects of acupuncture are due to placebo’. That’s also being economical with the truth I think. You argue ‘BECAUSE THIS IS WHAT THE PAPER DISCUSSED IN THAT PARTICULAR POST IMPLIED’, but is it? The authors state ‘Future studies are needed to confirm or refute any effects of acupuncture in acute stroke’, and that would have been a much more balanced headline. You clearly imply here that it has been CONFIRMED that the effects of acupuncture are due to placebo, and that this trial is further confirmation. This is misleading at best. Yes, you add in brackets ‘(for acute stroke)’ at the end of the post, but why not in the title, unless you want to give the impression this is true for acupuncture in general
Edzard on Thursday 02 August 2018 at 14:09
my post is about critical evaluation of the published literature.
and this is what follows from a critical evaluation of this particular article.
I am not surprised that you cannot follow this line of reasoning.
could it be that the lack of an open mind is not my but your problem
‘could it be that the lack of an open mind is not my but your problem?’
Who knows, maybe the problem is both of ours? I’m open to all possibilities!
VERY GOOD!
ok, let’s have a look.
you 1st: learnt acupuncture [a therapy that relies on a 2000 year old dogma], never published anything negative about it, never used any other therapeutic modality, even treated my own daughter with acupuncture when she suffered from infant colic, earn my livelihood by doing acupuncture.
[I MIGHT BE WRONG HERE, AS I DON’T KNOW ALL THAT MUCH ABOUT YOU, SO PLEASE CORRECT ME]
me next: studied acupuncture during my time in med school, used it occasionally, learnt to use dozens of other therapeutic modalities, published lots about acupuncture based on the current evidence [this means that some conclusions – even of my Cochrane reviews – were positive but have since changed], worked with acupuncturists from across the globe, published one book about acupuncture together with several acupuncture fans, now dedicate my time to the critical analysis of the literature and bogus claims, have no conflicts of interest.
[IN CASE YOU KNOW MORE RELEVANT THINGS ABOUT ME, PLEASE ADD]
@Edzard Your summaries seem to be more or less accurate. However, a) I wouldn’t agree with your use of the term ‘dogma’; b) I haven’t published any scientific papers, but I’ve acknowledged various problems in the acupuncture field through informal pieces; c) I’ve used other CAM modalities, and I’ve directly or indirectly experienced many conventional modalities; d) I only earn part of my livelihood by doing acupuncture. Yes, my background makes it more likely that I’ll be biased in favour of acupuncture. But your credentials in no way guarantee open-mindedness on the subject, and personally I don’t see that displayed often on this blog. It still makes for interesting and stimulating reading though.
what problems in the acupuncture field have you acknowledged through informal pieces?
can you provide links?
I want to get a feel for the openness of your mind.
“…your credentials in no way guarantee open-mindedness on the subject, and personally I don’t see that displayed often on this blog.”
1) you seem to forget that blog-posts are not scientific papers, not even close.
2) you also forget that my blog is dedicated to the CRITICAL assessment of alt med.
finally, what would make you think that someone has an open mind towards acupuncture, if not the fact that someone has a track record of publishing positive conclusions about it when the evidence allows?
remember: an open mind should not be so open that your brain falls out!
Tom Kennedy on Friday 03 August 2018 at 11:20
Here’s one example: https://www.tomtheacupuncturist.com/blog/2017/2/24/does-acupuncture-really-work
‘what would make you think that someone has an open mind towards acupuncture, if not the fact that someone has a track record of publishing positive conclusions about it when the evidence allows?’
I think there’s plenty of evidence that allows for positive conclusions about acupuncture, but you don’t report these. I understand the slant of this blog, but I’d say it comes across as ‘negative assessment’ rather than ‘critical assessment’. Perhaps you’ll argue that your critical assessment has led you to a negative assessment? I’ll just have to disagree that that’s a fair and open-minded summary of the evidence.
Out of interest, can I ask what your acupuncture training involved (hours, theory, clinic time etc.)?
I am sorry to say that I see no critical evaluation in the post you linked to.
” I’d say it comes across as ‘negative assessment’ rather than ‘critical assessment’.
have you noticed that criticism is often experienced as negative to the person(s) it is aimed at?
‘I am sorry to say that I see no critical evaluation in the post you linked to’
I’ll just have to live with that. I feel as though it acknowledges some of the problems in the acupuncture world, in an attempt at balance. I don’t feel your posts aim for balance, but as you said, a blog isn’t a scientific paper so it’s your prerogative to skew things as you see fit
Edzard on Friday 03 August 2018 at 13:18
it seems to me that the ‘screwing things as you see fit’ is your game.
____________________________________________________________________
This exchange shows how easily I can be provoked to get stroppy and even impolite – I do apologise.
But it also made me wonder: how can anyone be sure to have an open mind?
And how can we decide that a person has a closed mind?
We probably all think we are open minded, but are we correct?
I am not at all sure that I know the answer. It obviously depends a lot on the subject. There are subjects where one hardly needs to keep an open mind and some where it might be advisable to have a closed mind:
- the notion that the earth is flat,
- flying carpets,
- iridology,
- reflexology,
- chiropractic subluxation,
- the vital force,
- detox,
- homeopathy.
No doubt, there will be people who even disagree with this short list.
Something that intrigues me – and I am here main ly talking about alternative medicine – is the fact that I often get praised by people who say, “I do appreciate your critical stance on therapy X, but on my treatment Y you are clearly biased and unfairly negative!” To me, it is an indication of a closed mind, if criticism is applauded as long as it does not tackle someone’s own belief system.
On the subject of homeopathy, Prof M Baum and I once published a paper entitled ‘Should we maintain an open mind about homeopathy?’ Its introduction explains the problem quite well, I think:
Once upon a time, doctors had little patience with the claims made for alternative medicines. In recent years the climate has changed dramatically. It is now politically correct to have an open mind about such matters; “the patient knows best” and “it worked for me” seem to be the new mantras. Although this may be a reasonable approach to some of the more plausible aspects of alternative medicine, such as herbal medicine or physical therapies that require manipulation, we believe it cannot apply across the board. Some of these alternatives are based on obsolete or metaphysical concepts of human biology and physiology that have to be described as absurd with proponents who will not subject their interventions to scientific scrutiny or if they do, and are found wanting, suggest that the mere fact of critical evaluation is sufficient to chase the healing process away. These individuals have a conflict of interest more powerful than the requirement for scientific integrity and yet defend themselves by claiming that those wanting to carry out the trials are in the pocket of the pharmaceutical industry and are part of a conspiracy to deny their patients tried and tested palliatives….
END OF QUOTE
And this leads me to try to define 10 criteria indicative for an open mind.
- to be free of conflicts of interest,
- integrity,
- honesty,
- to resist the temptation of applying double standards,
- to have a track record of having changed one’s views in line with the evidence,
- to not cling to overt absurdities,
- to reject conspiracy theories,
- to be able to engage in a meaningful dialogue with people who have different views,
- to avoid fallacious thinking,
- to be willing to learn more on the subject in question.
I would be truly interested to hear, if you have further criteria, or indeed any other thoughts on the subject.
This recent announcement by the Society of Homeopaths (SoH), the organisation of non-doctor homeopaths in the UK, seems worthy of a short comment. Here is the unabbreviated text in question:
Two new members have been appointed to the Society’s Public Affairs (PAC) and Professional Standards (PSC) committees for three-year terms of office.
Selina Hatherley RSHom is joining the PAC. She has been a member since 2004 and works in three multi-disciplinary practices in Oxfordshire and previously ran a voluntary clinic working with people with drug, alcohol and mental health issues for 12 years. She has also been involved in the acute trauma clinics following the Grenfell Tower fire in 2017.
New to the PSC is Lynne Howard. She became a RSHom in 1996 and runs a practice in three locations in east London and a major London hospital. She specialises in pregnancy, birth and mother-and-baby issues.
“Following an open and comprehensive appointment process, we are delighted to welcome Selina and Lynne ‘on-board’ as brand-new committee members who will bring new ideas, experiences and knowledge to the society,” said Chief Executive Mark Taylor.
END OF QUOTE
It seems to me that the SoH might be breaching its very own Code of Ethics with these appointments.
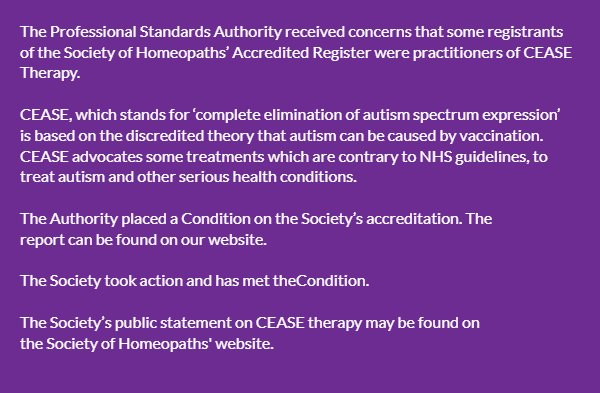
1) Lynne Howard BA, LCH, MCH, RSHom tells us on her website that she has been practising homeopathy for 25 years, she has run many children’s clinics and is a registered CEASE practitioner with a special interest in fertility and children’s health.
CEASE therapy has been discussed before on this blog. It is highly unethical and the SoH have been warned about it before. They even pretended to take the warning seriously.
 2) Selina Hatherley has a website where she tells us this: In 2011 I trained as a Vega practitioner – enabling me to use the Vega machine to test for food sensitivity and allergens. I use homeopathic remedies to support the findings and to help restore good health… I am a registered member of the Society of Homeopaths – the largest organisation registering professional homeopaths in Europe, I abide by their Code of Ethics and Practice and am fully insured.
2) Selina Hatherley has a website where she tells us this: In 2011 I trained as a Vega practitioner – enabling me to use the Vega machine to test for food sensitivity and allergens. I use homeopathic remedies to support the findings and to help restore good health… I am a registered member of the Society of Homeopaths – the largest organisation registering professional homeopaths in Europe, I abide by their Code of Ethics and Practice and am fully insured.
Vega, or electrodermal testing for allergies has been evaluated by the late George Lewith (by Jove not a man who was biased against such things) and found to be bogus. Here are the conclusions of his study published in the BMJ: “Electrodermal testing cannot be used to diagnose environmental allergies.” That’s pretty clear, I think. As the BMJ is not exactly an obscure journal, the result should be known to everyone with an interest in Vega-testing. And, of course, disregarding such evidence is unethical.
But perhaps, in homeopathy, ethics can be diluted like homeopathic remedies?
Perhaps the SoH’s Code of Ethics even allows such behaviour?
Have a look yourself; here are the 16 core principles of the SoH’s CODE OF ETHICS:
1.1 Put the individual needs of the patient first.
1.2 Respect the privacy and dignity of patients.
1.3 Treat everyone fairly, respectfully, sensitively and appropriately without discrimination.
1.4 Respect the views of others and, when stating their own views, avoid the disparagement of others either professionally or personally.
1.5 Work to foster and maintain the trust of individual patients and the public.
1.6 Listen actively and respect the individual patient’s views and their right to personal choice.
1.7 Encourage patients to take responsibility for their own health, through discussion and provision of information.
1.8 Comprehensively record any history the patient may give and the advice and treatment the registered or student clinical member has provided.
1.9 Provide comprehensive clear and balanced information to allow patients to make informed choices.
1.10 Respect and protect the patients’ rights to privacy and confidentiality.
1.11 Maintain and develop professional knowledge and skills.
1.12 Practise only within the boundaries of their own competence.
1.13 Respond promptly and constructively to concerns, criticisms and complaints.
1.14 Respect the skills of other healthcare professionals and where possible work in cooperation with them.
1.15 Comply with the current statutory legislation in relation to their practice as a homeopath of the country, state or territory where they are practising.
1.16 Practise in accordance with the Core Criteria for Homeopathic Practice and the Complementary and Natural Healthcare National Occupational Standards for Homeopathy.
______________________________________________________
I let you decide whether or not the code was broken by the new appointments and, if so, on how many accounts.
It is no secret to regular readers of this blog that chiropractic’s effectiveness is unproven for every condition it is currently being promoted for – perhaps with two exceptions: neck pain and back pain. Here we have some encouraging data, but also lots of negative evidence. A new US study falls into the latter category; I am sure chiropractors will not like it, but it does deserve a mention.
This study evaluated the comparative effectiveness of usual care with or without chiropractic care for patients with chronic recurrent musculoskeletal back and neck pain. It was designed as a prospective cohort study using propensity score-matched controls.
Using retrospective electronic health record data, the researchers developed a propensity score model predicting likelihood of chiropractic referral. Eligible patients with back or neck pain were then contacted upon referral for chiropractic care and enrolled in a prospective study. For each referred patient, two propensity score-matched non-referred patients were contacted and enrolled. We followed the participants prospectively for 6 months. The main outcomes included pain severity, interference, and symptom bothersomeness. Secondary outcomes included expenditures for pain-related health care.
Both groups’ (N = 70 referred, 139 non-referred) pain scores improved significantly over the first 3 months, with less change between months 3 and 6. No significant between-group difference was observed. After controlling for variances in baseline costs, total costs during the 6-month post-enrollment follow-up were significantly higher on average in the non-referred versus referred group. Adjusting for differences in age, gender, and Charlson comorbidity index attenuated this finding, which was no longer statistically significant (p = .072).
The authors concluded by stating this: we found no statistically significant difference between the two groups in either patient-reported or economic outcomes. As clinical outcomes were similar, and the provision of chiropractic care did not increase costs, making chiropractic services available provided an additional viable option for patients who prefer this type of care, at no additional expense.
This comes from some of the most-renowned experts in back pain research, and it is certainly an elaborate piece of investigation. Yet, I find the conclusions unreasonable.
Essentially, the authors found that chiropractic has no clinical or economical advantage over other approaches currently used for neck and back pain. So, they say that it a ‘viable option’.
I find this odd and cannot quite follow the logic. In my view, it lacks critical thinking and an attempt to produce progress. If it is true that all treatments were similarly (in)effective – which I can well believe – we still should identify those that have the least potential for harm. That could be exercise, massage therapy or some other modality – but I don’t think it would be chiropractic care.
References
Elder C, DeBar L, Ritenbaugh C, Dickerson J, Vollmer WM, Deyo RA, Johnson ES, Haas M.
J Gen Intern Med. 2018 Jun 25. doi: 10.1007/s11606-018-4539-y. [Epub ahead of print]
PMID: 29943109
@Rich It sounds to me as if you are at least partly open-minded, and take a more genuinely scientific approach than most here – i.e. rather than dismissing something with a lot of intriguing evidence behind it (even if much of this evidence is still hotly debated) mainly on the grounds that it ‘sounds a bit silly’, you understand that it’s possible to look at something like acupuncture objectively without being put off by the strange terminology associated with it. I strongly urge you to consult various other outlets as well as this one before coming to any final judgement. http://www.evidencebasedacupuncture.org/ for example is run by intelligent people genuinely trying to present the facts as they see them. Yes, they have an ‘agenda’ in that they are acupuncturists, but I can assure you, having had detailed discussions with some of them, that they are motivated by the urge to see acupuncture help more people rather than anything sinister, and they are trying to present an honest appraisal of the evidence. No doubt virtually everyone here will dismiss everything there with (or without) a cursory glance, but perhaps you won’t fall into that category. I hope you find something of interest there, and come to a balanced opinion.