quackery
The objective of this study was to compare chronic low back pain patients’ perspectives on the use of spinal manipulative therapy (SMT) compared to prescription drug therapy (PDT) with regard to health-related quality of life (HRQoL), patient beliefs, and satisfaction with treatment.
Four cohorts of Medicare beneficiaries were assembled according to previous treatment received as evidenced in claims data:
- The SMT group began long-term management with SMT but no prescribed drugs.
- The PDT group began long-term management with prescription drug therapy but no spinal manipulation.
- This group employed SMT for chronic back pain, followed by initiation of long-term management with PDT in the same year.
- This group used PDT for chronic back pain followed by initiation of long-term management with SMT in the same year.
A total of 1986 surveys were sent out and 195 participants completed the survey. The respondents were predominantly female and white, with a mean age of approx. 77-78 years. Outcome measures used were a 0-to-10 numeric rating scale to measure satisfaction, the Low Back Pain Treatment Beliefs Questionnaire to measure patient beliefs, and the 12-item Short-Form Health Survey to measure HRQoL.
Recipients of SMT were more likely to be very satisfied with their care (84%) than recipients of PDT (50%; P = .002). The SMT cohort self-reported significantly higher HRQoL compared to the PDT cohort; mean differences in physical and mental health scores on the 12-item Short Form Health Survey were 12.85 and 9.92, respectively. The SMT cohort had a lower degree of concern regarding chiropractic care for their back pain compared to the PDT cohort’s reported concern about PDT (P = .03).
The authors concluded that among older Medicare beneficiaries with chronic low back pain, long-term recipients of SMT had higher self-reported rates of HRQoL and greater satisfaction with their modality of care than long-term recipients of PDT. Participants who had longer-term management of care were more likely to have positive attitudes and beliefs toward the mode of care they received.
The main issue here is that the ‘study’ was a mere survey which by definition cannot establish cause and effect. The groups were different in many respects which rendered them not comparable. For instance, participants who received SMT had higher self-reported physical and mental health on average than those who received PDT. Differences also existed between the SMT and the PDT groups for agreement with the notion that “spinal manipulation for LBP makes a lot of sense”; 96% of the SMT group and 35% of the PDT group agreed with it. Compare this with another statement, “taking /having prescription drug therapy for LBP makes a lot of sense” and we find that only 13% of the SMT cohort agreed with, 95% of the PDT cohort agreed. Thus, a powerful bias exists toward the type of therapy that each person had chosen. Another determinant of the outcome is the fact that SMT means hands-on treatments with time, compassion, and empathy given to the patient, whereas PDT does not necessarily include such features. Add to these limitations the dismal response rate, recall bias, and numerous potential confounders and you have a survey that is hardly worth the paper it is printed on. In fact, it is little more than a marketing exercise for chiropractic.
In summary, the findings of this survey are influenced by a whole range of known and unknown factors other than the SMT. The authors are clever to avoid causal inferences in their conclusions. I doubt, however, that many chiropractors reading the paper think critically enough to do the same.
This randomized, double-blind, placebo-controlled trial investigated whether homeopathic Hypericum leads to a reduction in postoperative pain and a decrease in pain medication compared with placebo. Inpatients undergoing lumbar sequestrectomy surgery were given the homeopathic treatment Hypericum C200 or a placebo in addition to usual pain management. The primary endpoint was pain relief measured with a visual analog scale. Secondary endpoints were the reduction of inpatient postoperative analgesic medication and change in sensory and affective pain perception.
The baseline characteristics were comparable between the two groups. Pain perception between baseline and day 3 did not significantly differ between the study arms. With respect to pain medication, total morphine equivalent doses did not differ significantly. However, a statistical trend and a moderate effect (d = 0.432) in the decrease of pain medication consumption in favor of the Hypericum group was observed.
The authors concluded that this is the first trial of homeopathy that evaluated the efficacy of Hypericum C200 after lumbar monosegmental spinal sequestrectomy. Although no significant differences between the groups could be shown, we found that patients who took potentiated Hypericum in addition to usual pain management showed lower consumption of analgesics. Further investigations, especially with regard to pain medication, should follow to better classify the described analgesic reduction.
I applaud the authors from the Institute of Integrative Medicine, Witten/Herdecke University, Herdecke, Germany (not an institution known for its objectivity in SCAM) to have published this negative study in a journal that is so clearly pro-SCAM that it very rarely contains anything in its pages that is not positive about SCAM. Yet, I am baffled by two things:
- The plant Hypericum is used in SCAM as a painkiller. According to the ‘like cures like’ axiom of homeopathy, it should thus INCREASE the pain of post-op patients.
- The researchers used a C 200 potency. I ask myself, how can anyone assume that such a dilution has any effect at all? C200 means that the plant tincture is diluted at a ratio of 1: 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000 00000000000000000000. Less than one molecule of the plant per several universes!
To believe that such a dilution might work, one really needs to be a convinced disciple of Hahnemann. Yet, to disregard the ‘like cures like’ axiom, one needs to be what he called ‘a traitor’ to his true art of healing.
I think this press release might interest you:
Science advocates have filed a groundbreaking lawsuit against Boiron, Inc., one of the largest manufacturers of homeopathic products in the world, for deceiving vulnerable consumers with useless products dressed up to look like real medicine. The Center for Inquiry (CFI), which fights on behalf of consumers against pseudoscience, says Boiron routinely made false claims about what its products will treat and heal, misleading the public about the absurd pseudoscientific basis for Boiron products, and even lying about the ingredients their products contain.
“The facts could not be more clear. Boiron profits massively by deceiving consumers in their time of need,” said CFI Vice President and Legal Counsel Nick Little. “Boiron knows its products are worthless junk, so they do everything they can to obscure the truth in order to offload their snake oil upon the unwitting, the ill-informed, and the vulnerable. They can’t be allowed to get away with it any longer.”
Adherents of homeopathy claim, without evidence, that a substance which causes harm to a healthy person will cure anyone else suffering the same type of harm. In homeopathic products, the “active” ingredients are highly diluted mixtures of the so-called cures; the ingredient ends up so diluted, often literally no trace of the original substance remains. Manufacturers like Boiron then sell miniscule amounts of the already incredibly diluted ingredients and promise astounding results.
In its lawsuit, brought under the District of Columbia Consumer Protection Procedures Act, CFI alleges that Boiron sold a plethora of materially identical products, each made up of sugar pills and powders. Despite no scientifically detectable active ingredient, Boiron falsely promised consumers that each item would treat and cure a particular illness, injury, or health condition.
“Boiron sells little pills of sugar with grandiose claims. It’s hard to believe anyone would try to pass off such junk as a surefire way to treat painful skin problems, heal mental health issues, and even to counteract menopause,” said CFI Staff Attorney Aaron D. Green. “But Boiroin has been doing just that by tricking consumers into risking their health and throwing away their money on its fancy faux ‘medicines.’ It’s time for Boiron and all homeopathy hucksters to be held accountable.”
In its complaint, CFI notes that Boiron sells Saccharum officinale as a treatment for “nervous agitation in children after overindulgence.”
“Most parents would rightfully be skeptical of this product if Boiron told them what Saccharum officinale actually is,” said Green. “Table sugar.”
According to recent industry accounts, 85 percent of consumers who purchased homeopathic products did not realize they were homeopathic, and nine out of ten consumers did not even know what the term homeopathic meant.
Apart from selling products they know are useless, Boiron also misrepresented the products’ ingredients. Four Boiron products were analyzed by an independent lab, and, not only were no traces of the supposed active ingredient found, even one of the inactive ingredients could not be scientifically detected.
The Center for Inquiry is currently engaged in other lawsuits regarding homeopathy, including consumer protection cases against megaretailers CVS and Walmart for their sale and marketing of homeopathic products, the matter recently heard by the DC Court of Appeals. CFI is also engaged in an active Freedom of Information Act lawsuit that demands the Department of Health and Human Services grant the public access to the Homeopathic Pharmacopoeia of the United States (HPUS), the “bible of homeopathy” upon which federal regulation of homeopathy is based and to which the industry restricts access but for those willing to pay thousands of dollars for the privilege.
_________________________
All I can add to this is: good luck to the CFI and let’s hope reason will prevail!
The Lancet is a top medical journal, no doubt. But even such journals can make mistakes, even big ones, as the Wakefield story illustrates. But sometimes, the mistakes are seemingly minor and so well hidden that the casual reader is unlikely to find them. Such mistakes can nevertheless be equally pernicious, as they might propagate untruths or misunderstandings that have far-reaching consequences.
A recent Lancet paper might be an example of this phenomenon. It is entitled “Management of common clinical problems experienced by survivors of cancer“, unquestionably an important subject. Its abstract reads as follows:
_______________________
Improvements in early detection and treatment have led to a growing prevalence of survivors of cancer worldwide.
Models of care fail to address adequately the breadth of physical, psychosocial, and supportive care needs of those who survive cancer. In this Series paper, we summarise the evidence around the management of common clinical problems experienced by survivors of adult cancers and how to cover these issues in a consultation. Reviewing the patient’s history of cancer and treatments highlights potential long-term or late effects to consider, and recommended surveillance for recurrence. Physical consequences of specific treatments to identify include cardiac dysfunction, metabolic syndrome, lymphoedema, peripheral neuropathy, and osteoporosis. Immunotherapies can cause specific immune-related effects most commonly in the gastrointestinal tract, endocrine system, skin, and liver. Pain should be screened for and requires assessment of potential causes and non-pharmacological and pharmacological approaches to management. Common psychosocial issues, for which there are effective psychological therapies, include fear of recurrence, fatigue, altered sleep and cognition, and effects on sex and intimacy, finances, and employment. Review of lifestyle factors including smoking, obesity, and alcohol is necessary to reduce the risk of recurrence and second cancers. Exercise can improve quality of life and might improve cancer survival; it can also contribute to the management of fatigue, pain, metabolic syndrome, osteoporosis, and cognitive impairment. Using a supportive care screening tool, such as the Distress Thermometer, can identify specific areas of concern and help prioritise areas to cover in a consultation.
_____________________________
You can see nothing wrong? Me neither! We need to dig deeper into the paper to find what concerns me.
In the actual article, the authors state that “there is good evidence of benefit for … acupuncture …”[1]; the same message was conveyed in one of the tables. In support of these categorical statements, the authors quote the current Cochrane review entitled “Acupuncture for cancer pain in adults”. Its abstract reads as follows:
Background: Forty per cent of individuals with early or intermediate stage cancer and 90% with advanced cancer have moderate to severe pain and up to 70% of patients with cancer pain do not receive adequate pain relief. It has been claimed that acupuncture has a role in management of cancer pain and guidelines exist for treatment of cancer pain with acupuncture. This is an updated version of a Cochrane Review published in Issue 1, 2011, on acupuncture for cancer pain in adults.
Objectives: To evaluate efficacy of acupuncture for relief of cancer-related pain in adults.
Search methods: For this update CENTRAL, MEDLINE, EMBASE, PsycINFO, AMED, and SPORTDiscus were searched up to July 2015 including non-English language papers.
Selection criteria: Randomised controlled trials (RCTs) that evaluated any type of invasive acupuncture for pain directly related to cancer in adults aged 18 years or over.
Data collection and analysis: We planned to pool data to provide an overall measure of effect and to calculate the number needed to treat to benefit, but this was not possible due to heterogeneity. Two review authors (CP, OT) independently extracted data adding it to data extraction sheets. Data sheets were compared and discussed with a third review author (MJ) who acted as arbiter. Data analysis was conducted by CP, OT and MJ.
Main results: We included five RCTs (285 participants). Three studies were included in the original review and two more in the update. The authors of the included studies reported benefits of acupuncture in managing pancreatic cancer pain; no difference between real and sham electroacupuncture for pain associated with ovarian cancer; benefits of acupuncture over conventional medication for late stage unspecified cancer; benefits for auricular (ear) acupuncture over placebo for chronic neuropathic pain related to cancer; and no differences between conventional analgesia and acupuncture within the first 10 days of treatment for stomach carcinoma. All studies had a high risk of bias from inadequate sample size and a low risk of bias associated with random sequence generation. Only three studies had low risk of bias associated with incomplete outcome data, while two studies had low risk of bias associated with allocation concealment and one study had low risk of bias associated with inadequate blinding. The heterogeneity of methodologies, cancer populations and techniques used in the included studies precluded pooling of data and therefore meta-analysis was not carried out. A subgroup analysis on acupuncture for cancer-induced bone pain was not conducted because none of the studies made any reference to bone pain. Studies either reported that there were no adverse events as a result of treatment, or did not report adverse events at all.
Authors’ conclusions: There is insufficient evidence to judge whether acupuncture is effective in treating cancer pain in adults.
This conclusion is undoubtedly in stark contrast to the categorical statement of the Lancet authors: “there is good evidence of benefit for … acupuncture …“
What should be done to prevent people from getting misled in this way?
- The Lancet should correct the error. It might be tempting to do this by simply exchanging the term ‘good’ with ‘some’. However, this would still be misleading, as there is some evidence for almost any type of bogus therapy.
- Authors, reviewers, and editors should do their job properly and check the original sources of their quotes.
PS
In case someone argued that the Cochrane review is just one of many, here is the conclusion of an overview of 15 systematic reviews on the subject: The … findings emphasized that acupuncture and related therapies alone did not have clinically significant effects at cancer-related pain reduction as compared with analgesic administration alone.
An article in PULSE entitled ‘ Revolutionising Chiropractic Care for Today’s Healthcare System’ deserves a comment, I think. Here I give you first the article followed by my comments. The references in square brackets refer to the latter and were inserted by me; otherwise, the article is unchanged.
___________________________
This Chiropractic Awareness Week (4th – 10th April), Catherine Quinn, President of the British Chiropractic Association (BCA), is exploring the opportunity and need for a more integrated healthcare eco-system, putting the spotlight on how chiropractors can help alleviate pressures and support improved patient outcomes.
Chiropractic treatment and its role within today’s health system often prompts questions and some debate – what treatments fit under chiropractic care? Is the profession evidence based? How can it support primary health services, with the blend of public and private practice in mind? This Chiropractic Awareness Week, I want to address these questions and share the British Chiropractic Association’s ambition for the future of the profession.
The role of chiropractic today
The need for effective and efficient musculoskeletal (MSK) treatment is clear – in the UK, an estimated 17.8 million people live with a MSK condition, equivalent to approximately 28.9% of the total population.1 Lower back and neck pain specifically are the greatest causes of years lost to disability in the UK, with chronic joint pain or osteoarthritis affecting more than 8.75 million people.2 In addition to this, musculoskeletal conditions also account for 30% of all GP appointments, placing immense pressure on a system which is already under stress.3 The impact of the COVID-19 pandemic is still being felt by these patients and their healthcare professionals alike. Patients with MSK conditions are still having their care impacted by issues such as having clinic appointments cancelled, difficulty in accessing face-to-face care and some unable to continue regular prescribed exercise.
With these numbers and issues in mind, there is a lot of opportunity to more closely integrate chiropractic within health and community services to help alleviate pressures on primary care [1]. This is something we’re really passionate about at the BCA. However, we recognise that there are varying perceptions of chiropractic care – not just from the public but across our health peers too. We want to address this, so every health discipline has a consistent understanding.
First and foremost, chiropractic is a registered primary healthcare profession [2] and a safe form of treatment [3], qualified individuals in this profession are working as fully regulated healthcare professionals with at least four years of Masters level training. In the UK, chiropractors are regulated by law and required to adhere to strict codes of practice [4], in exactly the same ways as dentists and doctors [5]. At the BCA we want to represent the highest quality chiropractic care, which is encapsulated by a patient centred approach, driven by evidence and science [6].
As a patient-first organisation [7], our primary goal is to equip our members to provide the best treatment possible for those who need our care [8]. We truly believe that working collaboratively with other primary care and NHS services is the way to reach this goal [9].
The benefits of collaborative healthcare
As chiropractors, we see huge potential in working more closely with primary care providers and recognise there’s mutual benefits for both parties [10]. Healthcare professionals can tap into chiropractors’ expertise in MSK conditions, leaning on them for support with patient caseloads. Equally, chiropractors can use the experience of working with other healthcare experts to grow as professionals.
At the BCA, our aim is to grow this collaborative approach, working closely with the wider health community to offer patients the best level of care that we can [11]. Looking at primary healthcare services in the UK, we understand the pressures that individual professionals, workforces, and organisations face [12]. We see the large patient rosters and longer waiting times and truly believe that chiropractors can alleviate some of those stresses by treating those with MSK concerns [13].
One way the industry is beginning to work in a more integrated way is through First Contact Practitioners (FCPs) [14]. These are healthcare professionals like chiropractors who provide the first point of contact to GP patients with MSK conditions [15]. We’ve already seen a lot of evidence showing that primary care services using FCPs have been able to improve quality of care [16]. Through this service MSK patients are also seeing much shorter wait times for treatment (as little as 2-3 days), so the benefits speak for themselves for both the patient and GP [17].
By working as part of an integrated care model, with chiropractors, GPs, physiotherapists and other medical professionals, we’re creating a system that provides patients with direct routes to the treatments that they need, with greater choice. Our role within this system is very much to contribute to the health of our country, support primary care workers and reinforce the incredible work of the NHS [18].
Overcoming integrated healthcare challenges
To continue to see the chiropractic sector develop over the coming years, it’s important for us to face some of the challenges currently impacting progress towards a more integrated healthcare service.
One example is that there is a level of uncertainty about where chiropractic sits in the public/private blend. This is something we’re ready to tackle head on by showing exactly how chiropractic care benefits different individuals, whether that’s through reducing pain, improving physical function or increasing mobility [19]. We also need to encourage more awareness amongst both chiropractors and other healthcare providers about how an integrated workforce could benefit medical professionals and patients alike [20]. For example, there’s only two FCP chiropractors to date, and that’s something we’re looking to change [14].
This is the start of a much bigger conversation and, at the BCA, we’ll continue to work on driving peer acceptance, trust and inclusion to demonstrate the value of our place within the healthcare industry [21]. We’re ready to support the wider health community and primary carers, alleviating some of the pressures already facing the NHS; we’re placed in the perfect position as we have the knowledge and experience to provide essential support [22]. My main takeaway from this year’s Chiropractic Awareness Week would be to simply start a conversation with us about how [23].
About the British Chiropractic Association:
The BCA is the largest and longest-standing association for chiropractors in the UK. As well as promoting international standards of education and exemplary conduct, the BCA supports chiropractors to progress and develop to fulfil their professional ambitions with honour and integrity, at every step [24]. This Chiropractic Awareness Week, the BCA is raising awareness about the rigour, relevance and evidence driving the profession and the association’s ambition for chiropractic to be more closely embedded within mainstream healthcare [25].
- https://bjgp.org/content/70/suppl_1/bjgp20X711497
- https://www.versusarthritis.org/about-arthritis/data-and-statistics/the-state-of-musculoskeletal-health/
- https://www.england.nhs.uk/elective-care-transformation/best-practice-solutions/musculoskeletal/#:~:text=Musculoskeletal%20(MSK)%20conditions%20account%20for,million%20people%20in%20the%20UK
__________________________________
And here are my comments:
- Non sequitur = a conclusion or statement that does not logically follow from the previous argument or statement.
- A primary healthcare profession is a profession providing primary healthcare which, according to standard definitions, is the provision of health services, including diagnosis and treatment of a health condition, and support in managing long-term healthcare, including chronic conditions like diabetes. Thus chiropractors are not in that category.
- This is just wishful thinking. Chiropractic spinal manipulation is not safe!
- “Required to adhere to strict codes of practice”. Required yes, but how often do they not comply?
- This is not true.
- Chiropractic is very far from being “driven by evidence and science”.
- Platitude = a remark or statement, especially one with a moral content, that has been used too often to be interesting or thoughtful.
- Judging from past experience, the primary goal seems to be to protect chiropractors (see, for instance, here).
- Belief is for religion, in healthcare you need evidence. Have you looked at the referral rates of chiropractors to GPs, for instance?
- For chiropractors, the benefit is usually measured in £s.
- To offer the ” best level of care” you need research and evidence, not politically correct statements.
- Platitude = a remark or statement, especially one with a moral content, that has been used too often to be interesting or thoughtful.
- Belief is for religion, in healthcare you need evidence.
- First Contact Practitioners are “regulated, advanced and autonomous health CARE PROFESSIONALS who are trained to provide expert PATIENT assessment, diagnosis and first-line treatment, self-care advice and, if required, appropriate onward referral to other SERVICES.” I doubt that many chiropractors fulfill these criteria.
- Not quite; see above.
- “A lot of evidence”? Really? Where is it?
- “The benefits speak for themselves” only if the treatments used are evidence-based.
- Platitude = a remark or statement, especially one with a moral content, that has been used too often to be interesting or thoughtful.
- Where is the evidence?
- Awareness is not needed as much as evidence?
- Platitude = a remark or statement, especially one with a moral content, that has been used too often to be interesting or thoughtful.
- Platitude = a remark or statement, especially one with a moral content, that has been used too often to be interesting or thoughtful.
- Fine, let’s start the conversation: where is your evidence?
- Judging from past experience honor and integrity seem rather thin on the ground (see, for instance here).
The article promised to ‘revolutionize chiropractic care and to answer questions like what treatments fit under chiropractic care? Is the profession evidence-based? Sadly, none of this emerged. Instead, we were offered politically correct platitudes, half-truths, and obscurations.
The revolution in chiropractic, it thus seems, is not in sight.
Today, several UK dailies report about a review of osteopathy just published in BMJ-online. The aim of this paper was to summarise the available clinical evidence on the efficacy and safety of osteopathic manipulative treatment (OMT) for different conditions. The authors conducted an overview of systematic reviews (SRs) and meta-analyses (MAs). SRs and MAs of randomised controlled trials evaluating the efficacy and safety of OMT for any condition were included.
The literature searches revealed nine SRs or MAs conducted between 2013 and 2020 with 55 primary trials involving 3740 participants. The SRs covered a wide range of conditions including
- acute and chronic non-specific low back pain (NSLBP, four SRs),
- chronic non-specific neck pain (CNSNP, one SR),
- chronic non-cancer pain (CNCP, one SR),
- paediatric (one SR),
- neurological (primary headache, one SR),
- irritable bowel syndrome (IBS, one SR).
Although with different effect sizes and quality of evidence, MAs reported that OMT is more effective than comparators in reducing pain and improving the functional status in acute/chronic NSLBP, CNSNP and CNCP. Due
to the small sample size, presence of conflicting results and high heterogeneity, questionable evidence existed on OMT efficacy for paediatric conditions, primary headaches and IBS. No adverse events were reported in most SRs. The methodological quality of the included SRs was rated low or critically low.
The authors concluded that based on the currently available SRs and MAs, promising evidence suggests the possible effectiveness of OMT for musculoskeletal disorders. Limited and inconclusive evidence occurs for paediatric conditions, primary headache and IBS. Further well-conducted SRs and MAs are needed to confirm and extend the efficacy and safety of OMT.
This paper raises several questions. Here a just the two that bothered me most:
- If the authors had truly wanted to evaluate the SAFETY of OMT (as they state in the abstract), they would have needed to look beyond SRs, MAs or RCTs. We know – and the authors of the overview confirm this – that clinical trials of so-called alternative medicine (SCAM) often fail to mention adverse effects. This means that, in order to obtain a more realistic picture, we need to look at case reports, case series and other observational studies. It also means that the positive message about safety generated here is most likely misleading.
- The authors (the lead author is an osteopath) might have noticed that most – if not all – of the positive SRs were published by osteopaths. Their assessments might thus have been less than objective. The authors did not include one of our SRs (because it fell outside their inclusion period). Yet, I do believe that it is one of the few reviews of OMT for musculoskeletal problems that was not done by osteopaths. Therefore, it is worth showing you its abstract here:
The objective of this systematic review was to assess the effectiveness of osteopathy as a treatment option for musculoskeletal pain. Six databases were searched from their inception to August 2010. Only randomized clinical trials (RCTs) were considered if they tested osteopathic manipulation/mobilization against any control intervention or no therapy in human with any musculoskeletal pain in any anatomical location, and if they assessed pain as an outcome measure. The selection of studies, data extraction, and validation were performed independently by two reviewers. Studies of chiropractic manipulations were excluded. Sixteen RCTs met the inclusion criteria. Their methodological quality ranged between 1 and 4 on the Jadad scale (max = 5). Five RCTs suggested that osteopathy compared to various control interventions leads to a significantly stronger reduction of musculoskeletal pain. Eleven RCTs indicated that osteopathy compared to controls generates no change in musculoskeletal pain. Collectively, these data fail to produce compelling evidence for the effectiveness of osteopathy as a treatment of musculoskeletal pain.
It was published 11 years ago. But I have so far not seen compelling evidence that would make me change our conclusion. As I state in the newspapers:
OSTEOPATHY SHOULD BE TAKEN WITH A SIZABLE PINCH OF SALT.
THE END?
No, it is the start of the ‘HOMEOPATHY AWARENESS WEEK 2022′!
But, running a quick search for new evidence, I came across an abstract that seems like signaling the end of homeopathy. Here it is in its full beauty:
Acne is estimated to affect 9.4% of the global population, making it the 8th most prevalent disease worldwide. Acne vulgaris (AV) is among the diseases that directly affect quality of life. This trial evaluated the efficacy of individualized homeopathic medicines (IHM) against placebo in AV.
Methods: In this double-blind, randomized, placebo-controlled trial conducted at the National Institute of Homoeopathy, India, 126 patients suffering from AV were randomized in a 1:1 ratio to receive either IHM (verum) in centesimal potencies or identical-looking placebo (control). The primary outcome measure was the Global Acne Grading System score; secondary outcomes were the Cardiff Acne Disability Index and Dermatology Life Quality Index questionnaires – all measured at baseline and 3 months after the intervention. Group differences and effect sizes (Cohen’s d) were calculated on the intention-to-treat sample.
Results: Overall, improvements were greater in the IHM group than placebo, with small to medium effect sizes after 3 months of intervention; however, the inter-group differences were statistically non-significant. Sulphur (17.5%), Natrum muriaticum (15.1%), Calcarea phosphorica (14.3%), Pulsatilla nigricans (10.3%), and Antimonium crudum (7.1%) were the most frequently prescribed medicines; Pulsatilla nigricans, Tuberculinum bovinum and Natrum muriaticum were the most effective of those used. No harms, unintended effects, homeopathic aggravations or any serious adverse events were reported from either group.
Conclusion: There was non-significant direction of effect favoring homeopathy against placebo in the treatment of AV. 
And why do I suggest that this signals the end of anything?
Two reasons:
- It is a negative study of homeopathy from India, and by Jove, there are not many of those (mind you, the authors did try their best to squeeze in a glimpse of positivity, but I shall ignore this for their benefit [I particularly liked the sentence: “Pulsatilla nigricans, Tuberculinum bovinum and Natrum muriaticum were the most effective of those used” which is remarkable considering that the inter-group results – the only ones that matter in a controlled trial – were negative).
- It was published in the journal ‘HOMEOPATHY‘, the flagship publication of homeopathy.
I reckon that, if this journal (remember, its editor, the late Peter Fisher, fired me from the ed-board because of my criticism of the history of homeopathy) runs out of positive papers and starts publishing negative trials, it must be close to the end.
This study explored the curative effects of remote home management combined with ‘Feng’s spinal manipulation’ on the treatment of elderly patients with lumbar disc herniation (LDH). (LDH is understood by the investigators to be a condition where lumbar disc degeneration or trauma causes the nucleus pulposus and annulus fibrosus to protrude towards the spinal canal and to constrict the spinal cord or nerve root.)
The clinical data of 100 patients with LDH were retrospectively reviewed. The 100 patients were equally divided into a routine treatment group and an interventional group according to the order of admission. The routine treatment group received conventional rehabilitation training, and the interventional group received remote home management combined with Feng’s spinal manipulation. The Oswestry disability index (ODI) and straight leg raising test were adopted for the assessment of the degrees of dysfunction and straight leg raising angles of the two groups after intervention. The curative effects of the two rehabilitation programs were evaluated.
Compared TO the routine treatment group, the interventional group had a remarkably higher excellent and good rate (P < 0.05), a significantly lower average ODI score after intervention (P < 0.001), notably higher straight leg raising angle, surface AEMG (average electromyogram) during stretching and tenderness threshold after intervention (P < 0.001), markedly lower muscular tension, surface AEMG during buckling, and flexion-extension relaxation ratio (FRR; (P < 0.001)), and much higher quality of life scores after intervention (P < 0.001).
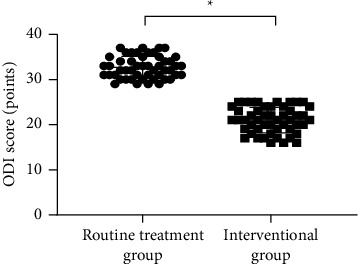
The authors concluded that remote home management combined with Feng’s spinal manipulation, as a reliable method to improve the quality of life and the back muscular strength of the elderly patients with LDH, can substantially increase the straight leg raising angle and reduce the degree of dysfunction. Further study is conducive to establishing a better solution for the patients with LDH.
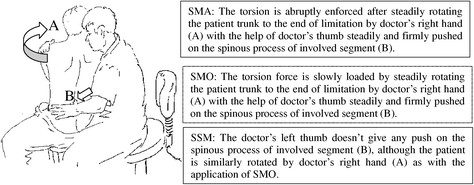
The authors state that “Feng’s spinal manipulation adopts spinal fixed-point rotation reduction to correct the vertebral displacement, and its curative effects have been confirmed in the treatment of sequestered LDH.” This is an odd statement: firstly, there is no vertebral displacement in LDH; secondly, if the treatment had been confirmed to be curative, why conduct this study?
Moreover, I don’t quite understand how the authors conducted a retrospective chart review and equally divide the 100 patients into two groups treated differently. What I do understand, however, is this:
- a retrospective review does not lend itself to conclusions about the effectiveness of any therapy;
- no type of spinal manipulation can hope to cure a lumbar disc degeneration or trauma that causes a herniation of the nucleus pulposus and annulus fibrosus.
Thus, I recommend we take this study with a sizable pinch of salt.
The Anglo-European College of Chiropractic (AECC) has been promoting pediatric chiropractic for some time, and I have posted about the subject before (see, for instance, here). Now the AECC has gone one decisive step further. On the website, the AECC announced an MSc ‘Musculoskeletal Paediatric Health‘:
The MSc Musculoskeletal Paediatric Health degree is designed to develop your knowledge and skills in the safe and competent care of children of all ages. Our part-time, distance-based course blends live online classes with ready to use resources through our virtual learning environment. In addition, you will have the opportunity to observe in the AECC University College clinical services at our Bournemouth campus. The course covers topics in paediatric musculoskeletal practice with specific units on paediatric development, paediatric musculoskeletal examination, paediatric musculoskeletal interventions, and paediatric musculoskeletal management. You will address issues such as risk factors and public health, including breastfeeding, supine sleep in infancy, physical activity in children and conditions affecting the musculoskeletal health of children from birth. The paediatric specific topics are completed by other optional units such as professional development, evidence-based practice, and leadership and inter-professional collaboration. In the dissertation unit you will conduct a study relevant to musculoskeletal paediatric health.
Your learning will happen through a mix of live and recorded lectures, access to online reading materials, and access to the literature through our learning services. You will also engage with the contents taught through guided activities with your peers and staff. Clinical paediatric experience is recommended to fully engage with the course. For students with limited access to a suitable clinical environment to support their studies, or for student who wants to add to their clinical experience, we are able to offer a limited number of opportunities to observe and work alongside our clinical educators within the AECC University College clinical services. Assessments are tailor made to each unit and may include a variety of methods such as critical reviews, reflective accounts, portfolios and in the last year a research dissertation.
___________________________
The AECC emphasizes its commitment to being a leading higher education institution in healthcare disciplines, nationally and internationally recognised for quality and excellence. Therefore, it seems only fair to have another look at the science behind pediatric chiropractic. Specifically, is there any good science to show that would justify a Master of Science in ‘Musculoskeletal Paediatric Health’?
So, let’s have a look and see whether there are any good review articles supporting such a degree. Here is what I found with several Medline searches (date of the review on chiropractic for any pediatric conditions, followed by its conclusion + link [so that the reader can look up the evidence]):
2008
I am unable to find convincing evidence for any of the above-named conditions.
2009
Previous research has shown that professional chiropractic organisations ‘make claims for the clinical art of chiropractic that are not currently available scientific evidence…’. The claim to effectively treat otitis seems to
be one of them. It is time now, I think, that chiropractors either produce the evidence or abandon the claim.
2009
The … evidence is neither complete nor, in my view, “substantial.”
2010
2018
What seems to emerge is rather disappointing:
- There are no really new reviews.
- Most of the existing reviews are not on musculoskeletal conditions.
- All of the reviews cast considerable doubt on the notion that chiropractors should go anywhere near children.
But perhaps I was too ambitious. Perhaps there are some new rigorous clinical trials of chiropractic for musculoskeletal conditions. A few further searches found this (again year and conclusion):
2019
2018
I might have missed one or two trials because I only conducted rather ‘rough and ready’ searches, but even if I did: would this amount to convincing evidence? Would it be good science?
No! and No!
So, why does the AECC offer a Master of Science in ‘Musculoskeletal Paediatric Health’?
Search me!
…
…
It wouldn’t have something to do with the notion that it is good for business?
Or perhaps they just want to give science a bad name?
Anyone who has been following this blog will have noticed that we have our very own ‘resident chiro’ who comments every single time I post about spinal manipulation/chiropractic/back pain. He uses (mostly?) the pseudonym ‘DC’. Recently, DC explained why he is such an avid poster of comments:
” I read and occasionally comment on this blog for two main reasons. 1. In my opinion Ernst doesn’t do a balance reporting on the papers his shares regarding spinal manipulation and chiropractic. Thus, I offer additional insight, a more balanced perspective for the readers. 2. There are a couple of skeptics who occasionally post that do a good job of analyzing papers or topics and they do so in a respectful manner. I enjoy reading their comments. I will add a third. 3. Ernst, from what I can tell, doesn’t censor people just because they have a different view.”
So, DC aims at offering additional insights and a more balanced perspective. That would certainly be laudable and welcome. Yet, over the years, I have gained a somewhat different impression. Almost invariably, my posts on the named subjects cast doubt on the notion that chiropractic generates more good than harm. This, of course, cannot be to the liking of chiropractors, who therefore try to undermine me and my arguments. In a way, that is fair enough.
DC, however, seems to have long pursued a very specific and slightly different strategy. He systematically attempts to distract from the evidence and arguments I present. He does that by throwing in the odd red herring or by deviating from the subject in some other way. Thus he hopes, I assume, to distract from the point that chiropractic fails to generate more good than harm. In other words, DC is a tireless (and often tiresome) fighter for the chiropractic cause and reputation.
To check whether my impression is correct, I went through the last 10 blogs on spinal manipulation/ chiropractic/ back pain. Here are my findings (first the title of and link to the blog in question, followed by one of DC’s originals distractions)
No 1
Chiropractic: “a safe form of treatment”? (edzardernst.com)
“It appears conventional medicine has a greater number of AE. This is not surprising.”
correct!
real doctors treat really sick patients
So the probability of an AE increases based upon how sick a patient is? Is there research that supports that?
No 2
Malpractice Litigation Involving Chiropractic Spinal Manipulation (edzardernst.com)
It would be interesting to know more about these 38 cases that weren’t included since that’s almost half of the 86 cases. What percentage of those cases involved SMT by a non chiropractor?
“Query of the VerdictSearch online legal database for “chiropractor” OR “chiropractic” OR “spinal manipulation” within the 22,566 listed cases classified as “medical malpractice” yielded 86 cases. Of these, 48 cases met the inclusion criteria by featuring a chiropractic practitioner as the primary defendant.”
No 3
there are three basic types of disc herniation
contained herniation
non-contained herniation
sequestered herniation
Some add a forth which are:
disc protrusion
prolapsed disc
disc extrusion
sequestered disc
where the first two are considered incomplete (contained) and the last two are called complete (non-contained) but they are all classified as a disc herniation.
You’re welcome
No 4
Multidisciplinary versus chiropractic care for low back pain (edzardernst.com)
Elaborate on what you think was my mistake regarding clinical significance.
No 5
An evidence based approach has three legs. If you wish to focus on the research leg, what does the research reveal regarding maintenance care and LBP? Have you even looked into it?
No 6
Meditation for Chronic Low Back Pain Management? (edzardernst.com)
CRITERIA in assessing the credibility of subgroup analysis.
https://www.nature.com/articles/s41433-022-01948-0/tables/1
No 7
Acute Subdural Hemorrhage Following Cervical Chiropractic Manipulation (edzardernst.com)
sigh, my use of the word require was pointing out that different problems require different solutions.
You confuse a lack of concern with my critical analysis of what some use as evidence of serious harm.
I have only used one other identifier on this blog. Some objected to my use of the word Dr in that identifier so I changed it to DC as it wasn’t worth my time to argue with them (which of course DC still refers to Doctor but it seemed to appease them).
In healthcare and particularly in manual therapy we look at increasing comfort and function because most come to us because…wait for it…a loss of comfort and function.
Yes, there is the potential to cause harm, I have never said otherwise. Most case reports suggest that serious harm is due to an improper history and exam (although other reasons may exist such as improper technique). Thus, most cases appear to be preventable with a proper history, exam and technique. That, is a different problem that, yes, requires a different solution.
So yes, spinal manipulation isn’t “required” anymore than physical therapy, NSAIDs, etc for most cases. The question is: does the intervention increase comfort and function over doing nothing and is that justified due the potential risk of harm….benefit vs risk.
Now, i shall excuse my self to prepare for a research presentation that deals with a possible new contraindication to cSMT (because I have a lack of concern, right?)
No 8
Hmmm, let’s change that a bit…
The best approach is to consider the totality of the available evidence. By doing this, one cannot exclude the possibility that NSAIDs and opioids cause serious adverse effects. If that is so, we must abide by the precautionary principle which tells us to use other treatments that seem safer and at least as effective.
So based upon the totality of the available evidence, which is safer and at least as effective: cervical spinal manipulation vs NSAIDs/opioids?
No 9
Chiropractic spinal manipulation is not safe! (edzardernst.com)
getting the patient to sign something describing the risks. This is apparently something chiropractors don’t do before a neck manipulation.
Apparently?
No 10
Vertebral artery dissection in a pregnant woman after cervical spine manipulation (edzardernst.com)
Most case reports fail on one of two criteria, sometimes both.
1. No clear record of why the patient sought chiropractic care (symptoms that may indicate a VAD in progress or not)
2. Eliminating any other possible causes of the VAD especially in the week prior to SMT.
I would have to search but I recall a case report of a woman presenting for maintenance care (no head or neck symptoms at the time) and after cSMT was dx with a VAD. Asymptomatic VADs are very rare thus there is a high probability that cSMT induced the VAD in that case, IMO.
Although not published I had a dialogue with a MD where a patient underwent a MRI, had cSMT the next day and developed new symptoms thus another MRI was shortly done and was dx with a VAD. I encouraged her to publish the case but apparently she did not.
There was a paper published that looked at the quality of these case reports, most are poor.
__________________________________
I might be mistaken but DC systematically tries to distract from the fact that chiropractic does not generate more good than harm and that there is a continuous flow of evidence suggesting it does, in fact, the exact opposite. He (I presume he is male) might not even do this consciously in which case it would suggest to me that he is full of quasi-religious zeal and unable to think critically about his own profession and creeds.
Reviewing the material above, I also realized that, by engaging with DC (and other zealots of this type), it is I who often gives him the opportunity to play his game. Therefore, I will from now on try harder to stick to my own rules that say:
- Comments must be on-topic.
- I will not post comments which are overtly nonsensical.
- I will not normally enter into discussions with people who do not disclose their full identity.