Monthly Archives: August 2017
The TIMES HIGHER EDUCATION (THE) reported yesterday that the British School of Osteopathy (BSO) has won university college title, meaning that it could be on the road towards full university status. University college title, awarded by the Privy Council on the advice of the Department for Education (DfE) and the Higher Education Funding Council for England, is usually seen as a step towards full university status. The London-based BSO already secured degree-awarding powers and access to Hefce public teaching and research funding in 2015. The BSO will be known, from September, as the University College of Osteopathy.
The THE quoted me saying “Osteopathy is based on implausible assumptions, and there is no good evidence for its effectiveness. Yet osteopaths regularly make all sorts of therapeutic claims. These facts make the BSO not a candidate for becoming a university; on the contrary, such a move would significantly downgrade the credibility of UK universities and make a mockery of academia and evidence-based healthcare.”
Charles Hunt, the BSO principal, responded: “We recognise that for some of the things that some osteopaths are doing, there is very limited evidence [to demonstrate their effectiveness], and we need to gain more for that. But within medicine, there’s a lot of things that also do not have evidence for them, but some medical practitioners are doing [them anyway].”
What???
The BSO principal should offer a course on logical fallacies and enlist as the first student in it, I thought when reading his response.
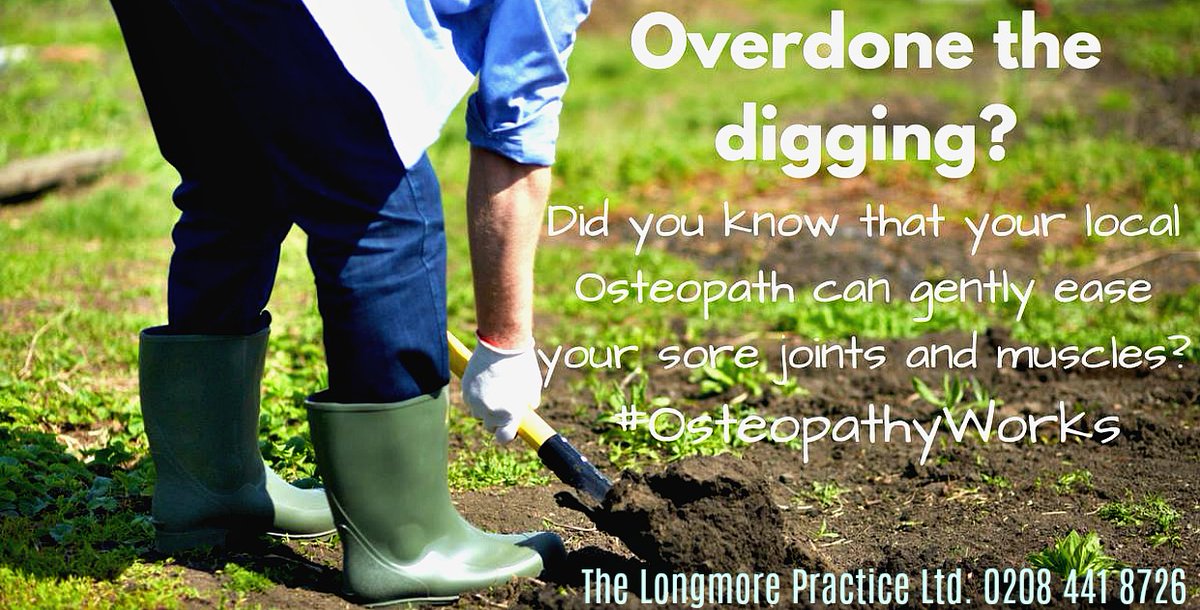
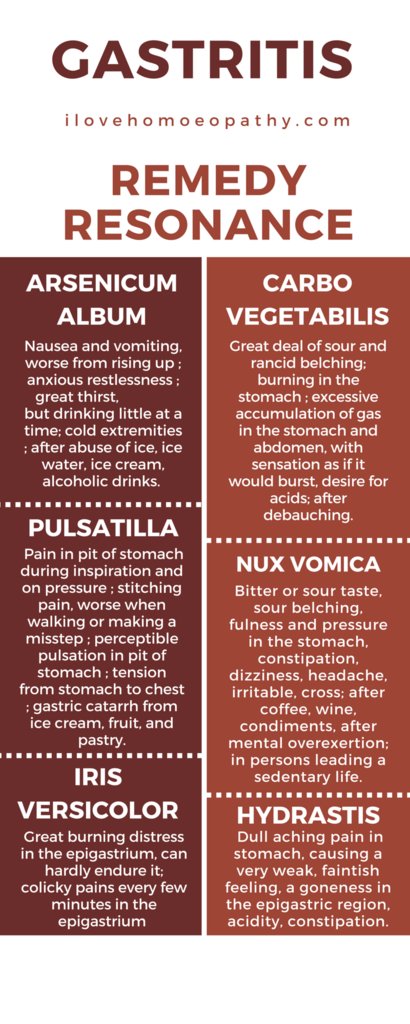
Anyway, having stated that “osteopaths regularly make all sorts of therapeutic claims”, I better provide some evidence. Perhaps another occasion for a slide-show?
Here are a few images I found on Twitter that are relevant in this context.
[please click to see them full size]





Guest post by Richard Rawlins MB BS MBA FRCS
Doctors who are registered medical practitioners (RMPs) must comply with the standards of practice set down by the General Medical Council. ‘Homeopathy’ is a specific system of medical care, devised by Dr Samuel Hahnemann in the nineteenth century, and comprises two distinct dimensions: (i) the establishment of a constructive therapeutic relationship between an empathic homeopath and a patient. This may provide benefit due to the non-specific effects of condolence, counselling, and care – and should be a component of the practice of all doctors in any event; (ii) the homeopathically prepared (HP) remedies that are generally prescribed. To avoid confusion, these two dimensions should not be conflated.
HP remedies may be obtained over the counter, prescribed by lay homeopaths and even given out by dentists and nurses on the grounds that “30C homeopathic arnica helps bruising”. The US Federal Trades Commission has stated that “The Commission will carefully scrutinize the net impression of OTC homeopathic advertising or other marketing employing disclosures to ensure that it adequately conveys the extremely limited nature of the health claim being asserted…accordingly, unqualified disease claims made for homeopathic drugs must be substantiated by competent and reliable scientific evidence.” (FTC Policy statement 2017).
Special focus should be brought to bear on the ethical, intellectual and professional obligations of those doctors registered as medical practitioners by the GMC and practicing homeopathy in the UK. Some homeopaths may intend taking advantage of gullible and vulnerable patients. Here I take it that those practitioners who prescribe homeopathic remedies sincerely do believe they have worthwhile effects, but I contend such practice generally fails to comply with ethical and professional standards as set down by the GMC. That is to be deprecated.
Systems to regulate medical practice in the British Isles have been devised since the middle ages. In 1518, Thomas Linacre founded the College of Physicians – based on systems he had seen in Europe. From 1704, the Society of Apothecaries licensed its members to prescribe and dispense medicines, and developed the profession of general practice. In order to protect the public from charlatans, quacks and fraudsters more effectively, the Medical Act of 1858 established formal statutory regulation of doctors by the General Medical Council. Registrants who are not deemed fit to practice may be struck off the register. They can still practice, but not as registered medical practitioners. They can still use the title ‘doctor’ (as can anyone), but not for fraudulent purposes.
Dr Samuel Hahnemann qualified in Saxony in 1781 and was a good doctor, but he became disillusioned with many of the practices and practitioners of his day. He wrote about his fellow doctors: “Precious and fragile human life, so easily destroyed, was frequently placed in jeopardy at the hands of these perverted people, especially since bleedings, emetics, purges, blistering plaster, fontanels, setons, caustics and cauterisations were used.” In 1796 he wrote to a friend, “I renounced the practice of medicine that I might no longer incur the risk of doing injury, and I engaged in chemistry exclusively and in literary occupations.”
Hahnemann went on to develop his own alternative system of health care, which he styled ‘Homoeopathy’. Published as the Organon of the Healing Arts in 1810, Hahnemann set out an idiosyncratic medical system based on identifying ‘remedies’ which in large doses, could produce symptoms comparable to those suffered by the patient. The remedies he prescribed were prepared with serial dilutions so that no active principle remained. Today’s homeopaths hold that a remedy’s ‘vital force’, ‘healing energy’ or ‘memory’ provides therapeutic benefit. That may be the case, but the consensus of informed scientific and medical opinion is that any effects of ‘homeopathy’ are as a result of contextual placebo effects. The remedies themselves cannot and do not have any effect. England’s Chief Medical Officer has described homeopathy’s principles as ‘rubbish’. The government’s Chief Scientific Adviser, Sir Mark Walport has said he would tell ministers, “My view, scientifically, is absolutely clear: homeopathy is nonsense. The most it can have is a placebo effect.” Simon Stevens, CEO of the NHS, when interviewed on Radio 4 said he agrees with Sir Mark – yet failed to explain why he had not included homeopathic remedies in the 2017 list of NHS proscribed medicines. That stance is being reviewed.
The GMC states, “Patients must be able to trust doctors with their lives and health. To justify that trust you must show respect for human life and make sure your practice meets the standards expected.” Those standards are set down in the GMC’s Good Medical Practice which advises, “Serious or persistent failure to follow this guidance will put your registration at risk.” The GMC standards are coherent with those of the American Medical Association’s Principles of Medical Ethics (2016).
In précis, the most relevant and important GMC standards are:
- Make the care of your patient your first concern.
- Give patients the information they want or need in a way they can understand.
- Be honest and open and act with integrity.
- Never abuse your patients’ trust in you or the public’s trust in the profession.
- You are personally accountable for your professional practice and must always be prepared to justify your decisions and actions.
- You must prescribe drugs or treatment only when you are satisfied that the drugs or treatment serve the patient’s needs.
- You must provide effective treatments based on the best available evidence.
- You must be satisfied that you have consent or other valid authority before you carry out any examination, investigation or provide treatment.
- You must make good use of the resources available to you.
I contend that medical practitioners who prescribe homeopathic remedies regularly fail to meet these standards. They know perfectly well that the best available evidence indicates no support for the assertion that homeopathic remedies ‘serve the patient’s needs’, except as placebos; that the treatments have no specific effects; that the remedies are placebos; and that resources are wasted by expenditure on these ineffective remedies. Medical homeopaths invariably do not give patients this information; they fail to obtain properly informed consent; they do not justify their decisions and actions rationally; and they may be obtaining financial advantage by misrepresentation to insurance companies or the NHS. This is an abuse of the public’s trust in the medical profession.
The issue of informed consent is particularly important. GMC guidance states that, “The doctor uses specialist knowledge and experience and clinical judgement, and the patient’s views and understanding of their condition, to identify which investigations or treatments are likely to result in overall benefit for the patient. The doctor explains the options to the patient, setting out the potential benefits, risks, burdens and side effects of each option, including the option to have no treatment. The doctor may recommend a particular option which they believe to be best for the patient, but they must not put pressure on the patient to accept their advice. …Before accepting a patient’s consent, you must consider whether they have been given the information they want or need, and how well they understand the details and implications of what is proposed. This is more important than how their consent is expressed or recorded.”
The GMC states that, “in order to have effective discussions with patients about risk, you must identify the adverse outcomes that may result from the proposed options… risks can take a number of forms, but will usually be: side effects; complications; failure of an intervention to achieve the desired aim.” The risk of wasting money on ineffective remedies, whether NHS or private, and of delaying treatment known to be effective should also be discussed.
Homeopaths acknowledge that after ministration of remedies, some patients experience ‘aggravations’ – a worsening of symptoms, but they advise this is evidence that the remedy is ‘working’. Medical consensus is more likely to suggest ‘aggravations’ are evidence of an underlying psychological component to the patient’s condition. Suggestions that remedies themselves have any effect, good or bad, is misrepresentation and may be fraud. Offering patients sugar pills with a claim the pills have therapeutic effects means lying to them, and is an abuse of trust.
Homeopaths’ system of diagnosis and prescription of remedies requires them to have beliefs for which there is no plausible evidence base. The Oxford Dictionary defines ‘belief’ as “assent to a proposition, statement or fact, especially on the grounds of testimony or authority, or in the absence of proof or conclusive evidence.” It might be acceptable to practice ‘homeopathy’ as a counselling modality, providing the practitioner complies with the GMC standard that, “You must not express your personal beliefs to patients in ways that exploit their vulnerability or are likely to cause them distress.”
Homeopaths are invariably non-compliant in obtaining fully informed consent. Such a failing is an abuse of patients’ trust in the medical profession. Doctors might be determined to be unfit to practice unless they clearly justify their prescriptions, and identify the evidence that supports them. All these issues should also be explored during the doctor’s annual appraisal, without which a registered medical practitioner will not be licensed to practice. Even registration without a licence requires compliance with the standards. Appraisal can be carried out by non-homeopaths, as the issue is not the assessment of the standard of ‘homeopathic practice’, but compliance with GMC standards of good medical practice.
If a medical homeopath wishes to be GMC compliant, they must properly inform patients about contentious issues. I suggest that consent should be obtained along the lines: “I propose prescribing you a remedy comprising sugar pills impregnated with a solution which has been diluted to such an extent that a sphere of water the size of the Earth’s average radius to the Sun would probably contain no more than one molecule of the original substance. Nevertheless, my clinical experience suggests to me that this remedy will improve your condition. You need to understand that colleagues who practise conventional evidence-based scientific medicine regard my belief as implausible and the methods I use as ‘alternative.’ I believe the remedy will help you, but I have no evidence accepted by the majority of doctors that the intervention I propose will achieve the desired effects. I do not believe that taking a homeopathic remedy will delay any other treatment which might reasonably help your condition and I invite you to take this remedy with understanding of the issues I have outlined.” A copy of the consent should be placed in the patient’s records.
Those who defend the right of registered medical practitioners to prescribe HP remedies do so with arguments fatally holed by a myriad of logical fallacies. Some arguments are (with fallacies in parenthesis):
- “Homeopathy has been used for over two hundred years” (appeal to tradition and argument from ignorance);
- “It has become very popular and is what patients want (appeal to popularity);
- “Homeopathy has the capacity to help patients” (red herring, because present consideration is about the value of HP remedies, not relationships);
- “Remedies are cheap” (red herring);
- “Homeopathy does not do any harm” (irrelevant and a red herring);
- “Pharmaceuticals have side effects” (tu quoque and red herring);
- “The Royal Family use it” (appeal to irrelevant authority);
- “The remedies enhance the doctor/patient relationship (straw man);
- “Science does not know everything” (red herring and false dichotomy);
- “Those who oppose us don’t understand homeopathy” (argumentum ad hominem and ‘poisoning the well’);
- “I have the evidence of patients’ anecdotes and testimonials” (pseudoscience, confirmation bias and cherry picking);
- “Homeopathic doctors are caring people” (red herring and straw man);
- “I’ve got much evidence of patients taking remedies and getting better” (post hoc ergo propter hoc – ‘after this, therefore because of this’ – confusion of coincidence with causation).
The latter most perverse fallacy is the foundation of homeopathic practice, based on identifying a remedy whereby ‘like cures like’ – a principle based on post hoc fallacy for which there is no scientifically credible evidence.
Unless and until medical homeopaths understand the intellectual environment in which they practice, are prepared to properly inform their patients, and obtain consent for treatment having done so, they should not prescribe homeopathic remedies. Fortunately, there is no evidence that patients who are prescribed HP remedies by empathic GMC registered homeopaths have any different outcomes from those prescribed pure sugar pills – even if they are told they are placebos. However, trust in the medical profession can only be maintained if deceptive practices are set aside and full explanations for proposed interventions are offered. Given the scientific consensus, patients have to face up to the fact that to the highest degree of probability, HP remedies have no value. Regrettably, too many patients and even homeopaths are in denial. Medical homeopaths should continue to serve their patients with care, compassion and intellectual honesty, but if they are to comply with the standards required for GMC registration, they should not prescribe homeopathically prepared remedies.
The UK ‘Faculty of Homeopathy’ (FoH) is the professional body of British doctors who specialise in homeopathy. As doctors, FoH members have been to medical school and should know about evidence, science etc., I had always thought. But perhaps I was mistaken?
The FoH has a website with an interesting new post entitled ‘Scientific evidence and Homeopathy’. Here I have copied the section on CLINICAL TRIALS OF HOMEOPATHY. I have read it several times and must admit: it is a masterpiece, in my view – not a masterpiece in accurate reporting, but a masterpiece in misleading the public. The first and most obvious thing that struck me is the fact that is cites not a single clinical trial. But read for yourself (the numbers in round brackets were inserted by me and refer to my comments below):
START OF QUOTE
By August 2017 1,138 clinical trials of homeopathy had been published (1). Details can be found on the CORE-HOM database also maintained by the Carstens Foundation and accessible without charge: http://archiv.carstens-stiftung.de/core-hom
Four (2) systematic review/meta-analyses of homeopathy for all conditions have been published.[26],[27],[28] Of these, three (3) reached a positive conclusion: that there is evidence that homeopathy is clinically effective (4). The exception is the review by Shang et al.46 This meta-analysis was controversial, particularly because its conclusions were based on only eight clinical trials whose identity was concealed until several months after the publication, precluding informed examination of its results (5) (6). The only undisputed conclusion (7) of this paper is that clinical trials of homeopathy are of higher quality than matched trials of conventional medicine: of 110 clinical trials each of homeopathy and conventional medicine, 21 trials of homeopathy but only 9 trials of conventional medicine were of ‘higher quality’.[29] [30]
A leading Swedish medical researcher (8) remarked: “To conclude that homeopathy lacks clinical effect, more than 90% of the available clinical trials had to be disregarded. Alternatively, flawed statistical methods had to be applied.”[31] Higher quality equates to less risk of bias, Mathie et al analysed randomized clinical trials of individualized homeopathy, showing that the highest quality trials yielded positive results (9).[32]
Systematic reviews of randomized controlled trials of homeopathy in specific clinical situations have also yielded positive results, including: allergies and upper respiratory tract infections (2 systematic reviews),[33],[34] (10) (11) Arnica in knee surgery,[35] (12) Childhood diarrhoea,[36] Post-operative ileus,[37] (13) Rheumatic diseases,[38] (14) Seasonal allergic rhinitis (hay fever) (2 systematic reviews),[39] [40] (15) (16) and vertigo.[41] (17)
END OF QUOTE
MY COMMENTS:
- This is a wild exaggeration which was made possible by counting all sorts of clinical reports as ‘clinical trials’. A clinical trial “follows a pre-defined plan or protocol to evaluate the effects of a medical or behavioral intervention on health outcomes.” This would exclude most observational studies, case series, case reports. However, the figure cited here includes such reports.
- The author cites only three!
- Does the author mean ‘two’?
- This is not quite true! I have dedicated an entire post to this issue.
- True, the Shang meta-analysis has been criticised – but exclusively by homeopaths who, for obvious reasons, were unable to accept its negative findings. In fact, it is a solid piece of research.
- Why does the author not mention the most recent systematic review of homeopathy? Perhaps because it concluded: Homeopathy should not be used to treat health conditions that are chronic, serious, or could become serious. People who choose homeopathy may put their health at risk if they reject or delay treatments for which there is good evidence for safety and effectiveness. People who are considering whether to use homeopathy should first get advice from a registered health practitioner. Those who use homeopathy should tell their health practitioner and should keep taking any prescribed treatments.
- Really? Undisputed? Even by the logic of the author’s last sentence, this would be disputed.
- The ‘leading researcher’ is Prof Hahn who has featured many times on my blog. He seems to be more than a little unhinged when it comes to the topic of homeopathy.
- The author forgot to mention that Mathie – who was sponsored by the British Homeopathic Association – included this little caveat in his conclusions: The low or unclear overall quality of the evidence prompts caution in interpreting the findings.
- Reference 33 is the infamous ‘Swiss report’ that has been shown to be fatally flawed over and over again.
- Reference 34 refers to a review that fails to adhere to almost all the criteria of a systematic review.
- This review concluded: In all three trials, patients receiving homeopathic arnica showed a trend towards less postoperative swelling compared to patients receiving placebo. However, a significant difference in favour of homeopathic arnica was only found in the CLR trial. Only a deluded homeopath can call this a ‘positive result’.
- This is a systematic review by my team. It showed that several flawed trials produced a false positive result, while the only large multicentre trial was negative. Our conclusions therefore include the statement that several caveats preclude a definitive judgment. Only a deluded homeopath can call this a ‘positive result’.
- This reference refers to the following abstract: Despite a growing interest in uncovering the basic mechanisms of arthritis, medical treatment remains symptomatic. Current medical treatments do not consistently halt the long-term progression of these diseases, and surgery may still be needed to restore mechanical function in large joints. Patients with rheumatic syndromes often seek alternative therapies, with homeopathy being one of the most frequent. Homeopathy is one of the most frequently used complementary therapies worldwide. Only a deluded homeopath can call this a ‘positive result’.
- The first reference refers to a paper where the author analysed three of his own studies.
- Reference 40 refers to a review that fails to adhere to almost all the criteria of a systematic review.
- This reference refers to a review of Vertigoheel@ that includes observational studies. One of its authors was an employee of the manufacturer of the product. Vertigoheel is not a homeopathic remedy (it does not adhere to the ‘like cures like’ principle) but a homotoxicologic product. Homotoxicology is a method inspired by homeopathy which was developed by Hans Heinrich Reckeweg (1905 – 1985). He believed that all or most illness is caused by an overload of toxins in the body. The toxins originate, according to Reckeweg, both from the environment and from the malfunction of physiological processes within the body. His treatment consists mainly in applying homeopathic remedies which usually consist of combinations of single remedies, because health cannot be achieved without ridding the body of toxins. The largest manufacturer and promoter of remedies used in homotoxicology is the German firm Heel. Our own systematic review of RCTs of homotoxicology included 7 trials which were mostly of a high methodological standard, according to the Jadad score. The trials tested the efficacy of seven different medicines for seven different indications. The results were positive in all but one study. Important flaws were found in all trials. These render the results of the primary studies less reliable than their high Jadad scores might suggest. Despite mostly positive findings and high ratings on the Jadad score, the placebo-controlled, randomised clinical trials of homotoxicology fail to demonstrate the efficacy of this therapeutic approach.
So!
What do we make of all this?
To say that it is disappointing would, I think, be an understatement. The FoH is not supposed to be a lobby group of amateurs ignorant of science and evidence; it is a recognised professional organisation who must behave ethically. Patients and consumers should be able to trust the FoH. The fact that the FoH publish misinformation on such a scale should, in my view, be a matter for the General Medical Council.
Dear edzard
I am sending you Richard Eaton’s excellent update on developments around complementary medicine. As you will know, the College is supportive of an integrated approach that offers each patient the best of both worlds – conventional and complementary. In both worlds it is important that treatment and advice offered is safe, appropriate and evidence based…
Thank you for your continued support of the College of Medicine.
With best wishes,
Dr Michael Dixon
Chairman
College of Medicine
I received this via email today, and of course I was interested. The ‘excellent update’ turned out to be truly amazing. For reasons that will become clear when you read on, I will abstain from any criticism – but I urge you to read it in full and perhaps let me know what you think by posting a comment:
START OF QUOTE
The Charity Commission’s Consultation: The use and promotion of complementary and alternative medicine – Making decisions about charitable status, (13.03.17):
The deadline for responses to the Charity Commission’s Consultation about the charitable status of CAM expired on 19th May (see the May edition of this blog). Many responses were filed, including by The Complementary & Natural Healthcare Council (CNHC) and by The College of Medicine.
Confusingly, the Commission’s Consultation Document expressly provided (in the section What the Commission is not consulting on at page 5) that:
‘…This consultation is not about…whether or not CAM therapies in general, or any particular CAM therapies, are effective…’
Yet logic dictates that the effectiveness of CAM and, therefore, the reliability of the evidence for it, will clearly feature significantly in the Commission’s deliberations as it assesses the extent to which CAM is of benefit to the public for charitable purposes.
The submission by The College of Medicine included the following:
‘…the continuing appetite of the public for access to CAM both in the private sector and through NHS organisations, should offer the Commission at least some reassurance that CAM has overall, a beneficial impact for those who use it…’
and further that:
‘…Whilst an RCT can be regarded as the highest level evidence, this type of study is not always the most suitable for assessing the benefits (efficacy/effectiveness) of CAM. Other research designs such as observational studies, surveys and qualitative methods can provide high quality information. In addition, RCTs invariably require very large budgets to underpin their delivery and CAM has not on the whole been the recipient of sufficient grant funding to enable large RCTs to be performed…’
The outcome of this important Charity Commission Consultation is awaited. It will be of huge significance to charitable organisations using or promoting CAM and to CAM practitioners and patients.
The Exclusivity of the Randomised Controlled Trial – the debate:
There is a continuing debate about the exclusivity of the Randomised Controlled Trial (RCT). Research articles about the RCT may be found here [Getting off the “Gold Standard”: Randomised Controlled Trials and Education Research: PMCID-PMC3179209] and here [Fool’s gold, lost treasures, and the randomised controlled trial-PMID: 23587187].
Further observations on the efficacy of the RCT may be found in the (free) April 2017 Newsletter published online by the Alliance for Natural Health International.
The Human effect and its desirability:
Also relevant to the debate about the evidence-base for CAM is the desirability of the Human effect. The Smallwood Report (The Role of Complementary and Alternative Medicine in the NHS: 2005), at page 23, makes the following observation:
‘…While some critics have derided the use of CAM treatments, claiming the success of some therapies to be purely based on a placebo effect, CAM proponents see what Dr Michael Dixon calls the “human effect” as desirable in itself…’
(Dixon & Sweeny, 2000 and see the BMJ book review here)
National Institute for Health & Care Excellence: CAM Updates
Practitioners of complementary and alternative medicine (CAM) may recall my November 2016 blog which referred to confirmation by the National Institute for Health and Care Excellence (NICE) that it had decided to retain its guideline on improving supportive care for adults with cancer, thereby ensuring that, for the time being at least, selected CAM therapies will continue to be available within the NHS in England & Wales. This guideline has been given the new title of End of life care for adults in the last year of life: service delivery and is currently “in development” with a publication date of January 2018 when it is hoped that CAM therapies will continue to be retained.
In the meantime, Further NICE guidelines have been published covering the planning and management of end of life and palliative care for infants, children and young people (aged 0 – 17 years) with life-limiting conditions. These aim to involve children, young people and their families in decisions about their care, and improve the support that is available to them throughout their lives. Recommendations include (paragraph 1.3.25) consideration of non-pharmacological interventions for pain management including music and physical contact such as touch, holding or massage. These Guidelines will next be reviewed in December 2018.
As mentioned in my blogs posted in September 2016 and February 2017, NICE Guidelines regarding the assessment and management of low back pain and sciatica in people aged 16 or over (published in November 2016) have stopped recommending acupuncture. The removal of acupuncture from the guidelines conflicts with research published (in January 2017) by MacPherson H, Vickers A (and others) in The National Institute for Health Research Journals Library: Programme Grants for Applied Research, Volume 5, issue 3 (“Acupuncture for chronic pain and depression in primary care: a programme of research”), which concludes as follows:
‘…We have provided the most robust evidence from high-quality trials on acupuncture for chronic pain. The synthesis of high-quality IPD found that acupuncture was more effective than both usual care and sham acupuncture. Acupuncture is one of the more clinically effective physical therapies for osteoarthritis and is also cost-effective if only high-quality trials are analysed. When all trials are analysed, TENS is cost-effective. Promising clinical and economic evidence on acupuncture for depression needs to be extended to other contexts and settings. For the conditions we have investigated, the drawing together of evidence on acupuncture from this programme of research has substantially reduced levels of uncertainty. We have identified directions for further research. Our research also provides a valuable basis for considering the potential role of acupuncture as a referral option in health care and enabling providers and policy-makers to make decisions based on robust sources of evidence…’
These Guidelines will next be reviewed in November 2018 when, again it is hoped, acupuncture will be reinstated and that Alexander Technique together with other beneficial CAM therapies will be included.
Professional Standards Authority: Accredited Registers Programme
Practitioners will already be aware of the Accredited Registers Programme which is overseen by the Professional Standards Authority for Health and Social Care (PSAHSC). This programme aims to provide assurance to the public, care commissioners and patients who are seeking health practitioners (including complementary therapists) who are not regulated by statute. The President of the Federation of Holistic Therapists (FHT), Jennifer Wayte, has suggested that:
‘…By signposting the Accredited Registers programme in relevant Guidelines, NICE would help to ensure better safety and standards of care…’ (International Therapist Journal, Issue 117 at page 17: Summer 2016).
Commissioning cost-saving CAM: The future for Integrated Medicine
In March 2016, The Kings Fund published its report Bringing together physical and mental health: A new frontier for integrated health about which a discussion can be viewed here and a blog by the FHT may be read here. In the News & Analysis section of its Health and Wellbeing Board Bulletin (06.06.17), The Kings Fund also highlighted the article published in The Lancet on 23.05.17 titled Forecasted trends in disability and life expectancy in England & Wales up to 2025: a modelling study which concludes:
‘…The rising burden of age-related disability accompanying population ageing poses a substantial societal challenge and emphasises the urgent need for policy development that includes effective prevention interventions…’
In the light of this and having regard to research such as that relating to the worsening mental well-being of year 10 school children, practitioners and their patients could lobby relevant Government departments, NICE and the PSAHSC regarding the potential of CAM as a cost-saving contributor to preventative and integrated medicine. In his Economic Outlook published in The Sunday Times on 23.04.17 (Business Section, page 4), Economist David Smith predicted frightening health spending as doubling from (roughly) 7% of gross domestic product to over 12.5% over the next 40-50 years and that social care costs will also double to 2% of GDP. Health spending policy makers and Clinical Commissioning Groups would do well to keep these (long-term) numbers in mind when assessing the potential of CAM and integrated medicine.
Further information about integrated and complementary medicine may be found in the Elsevier publications Advances in Integrative Medicine and the European Journal of Integrative Medicine and by accessing British Medical Journal (BMJ) articles such as Complementary therapies for labour and birth study: a randomised controlled trial of antenatal integrative medicine for pain management in labour (as amended), which concludes:
‘…The Complementary Therapies for Labour and Birth study protocol significantly reduced epidural use and caesarean section. This study provides evidence for integrative medicine as an effective adjunct to antenatal education, and contributes to the body of best practice evidence…’
For further research and debate about the cost-effective integration of CAM into the NHS, please refer to the February 2017 issue of this blog.
Adopting a business approach to practising CAM
Turning to a very different topic, my message to Practitioners and especially to those who are in the process of starting or establishing their CAM practice, is that adopting a business approach to practice management is crucial. By doing so and without compromising their professionalism, practitioners can help to defend their freedom to practice.
The past year has been challenging for practitioners. It looks like next few years will be even more so as those working in the health and social care sectors continue to assess the implications of ‘Brexit’ and how these may affect their freedom to practise and their patient’s right to receive a CAM treatment of their choice.
As ever, much of the popular press continues to present an unbalanced and misrepresentative view of CAM. For instance, I have yet to see popular print or broadcast journalism properly cover The World Health organisation Traditional Medicine Strategy 2014 to 2023: Strategy Document which states (at page 19; note: italics added by me):
‘…As the uptake of T&CM (Traditional and Complementary medicine) increases, there is a need for its closer integration into health systems…’
(refer to my November 2016 blog for more information).
Contrast this with the column in the Times Newspaper (by a Times leader writer and columnist) on Tuesday 13th December last year, captioned:
‘…Prince Charles’s homeopathy fad is joke medicine…’
I suggest there has never been greater need for practitioners to ‘fight their corner’, including by effectively organising the management of their practice and promoting the health benefits of their treatments.
To this end, I suggest that practitioners need to accept that running a CAM practice is, in essence, the same as trading in any (small) business. The knowledge, experience, professionalism and ethical standards of a qualified, insured and properly regulated CAM practitioner are acknowledged and to be congratulated. Nevertheless, now more than ever, practitioners need to embrace business processes.
The following are some straightforward business processes that could assist your business and thereby enhance the health and care of your patients.
Business planning will help you to prepare for most eventualities, including when, like most businesses, your practice encounters financial losses or failures. Don’t delay taking good business advice and realise that it is sometimes what you don’t want to hear that constitutes the most valuable advice.
Remember, “people buy from people” so you need to build good rapport with your patients. Listen to what they have to say about you and how you provide your practice specialism(s). If appropriate, adapt the structure and delivery of your business to their needs and requirements. Give them the opportunity to provide feedback [maybe use: surveymonkey]
While established practitioners may have the well-deserved and hard-earned luxury of relying on ‘word of mouth’ recommendations to find them new clients, this will rarely be an option for a new practitioner. So, whether you are practising alone or in association with other practitioners, for instance at a Health Centre, do not wait for patients to find you. You need to go out and find them. Recruit them by actively promoting yourself and your expertise.
Join local and national business support organisations such as the Federation of Small Businesses and the Chamber of Commerce. Always attend their meetings, networking events and, if appropriate, Trade Shows. As the contacts you make get to know and to trust you, they are likely to seek your professional help for themselves and their family and possibly for their colleagues and employees, too. Encourage this by offering to give a presentation [maybe use: presentme] about your practice to local businesses, to community groups and to the employees and students of local colleges and universities. Introduce them to your practice.
Sign-up to (often free) supportive online business newsletters and memberships like enterprisenation.
Using, among other things, the feedback from your patients (see above), prepare a patient database and create a Marketing Plan and a Business Plan, including a cash-flow forecast. You will have a much better chance of achieving your business goals if you first write them down.
Ask yourself: when and why did my patients seek my services and how can I keep in touch with them? Distribute print or e-newsletters [maybe use constantcontact]. Write articles about your practice and its treatments for professional journals and general healthcare-focused magazines. Produce a well-designed, good quality brochure and publicity material, both in print [see, for instance, moo.com] and also online.
Make use of social media platforms. Although new practitioners are likely to be familiar with how this is done, it’s possible this may not be the case with established practitioners. Record a video about you and your business and post it on YouTube. Link this to your Twitter and Facebook accounts. Your “followers” might then “comment”, “like” or “re-tweet” to their “followers”, thereby promoting your professional status and practice. Create, or, if you already have one, keep updated a (free) LinkedIn business account profile.
A website that is well designed and informative is a vital marketing tool. It is a worldwide ‘shop window’ as it informs your patients (existing and prospective) about you, where you are located, what you do and when you do it. If, when starting your business, you cannot afford a professionally built site, then build you own (maybe try wordpress].
Keep your cyber security under constant review and seek advice and support from websites like cyberware and getsafeonline. Your business will be processing your patients personal and health information/patient records, so ensure that you comply with data protection legislation including the new General Data Protection Regulation.
There are other business processes that could assist your practice, especially if you decided to diversify into the manufacture and sale of CAM-based products (e.g. first-aid kits, aromatherapy oils/preparations, books/course material, meditation audio-packs, therapy tools and devices) or to associate your business with other health professionals (e.g. at a veterinary practice, NHS Practice or Hospital, as appropriate for your specialism).
I hope that you have found this focus on the business aspects of practising CAM useful and thought provoking. My further thoughts can be found as either a paperback or as an e-book (the latter including hyperlinks to business and CAM websites) and at the amazon.co.uk bookstore. Information about business guides for complementary medicine may be found online.
I anticipate that, in the coming years, the freedom to practise CAM (whether or not independently of the conventional medicine sector or as a contribution to the provision of integrated healthcare and medicine) will depend upon the adoption of a business-focused approach by practitioners.
Established practitioners might be prepared to mentor new members to help them to adopt this approach.
Veterinary CAM Practitioners: Review of guidance by the RCVS
The Royal College of Veterinary Surgeons has announced a review of its position statement and guidance regarding the prescribing of CAM by its members (see my November 2016 blog). A campaign by is underway by www.vets4informedchoice.org to:
‘…raise the awareness of the Evidence Base (or lack of) for many current Veterinary Practices, enabling animal owners and guardians to make considered responsible choices without pressure from the Veterinary Industry…concerns over frequent and unnecessary Vaccination, Corporatisation of Veterinary Clinics, Pressure Selling of products and services, etc, are widespread and growing…’
A facility is available on the campaign website to sign-up to join the campaign and to get regular updates.
Therapy Expo 2017 and RCCM Membership
Therapy Expo returns to Birmingham’s NEC on 22nd – 23rd November. Conference information and booking details can be found here. Have you thought of becoming a member of the Research Council for Complementary Medicine? CAMRN membership ‘is free and provides members with access to the CAMRN research network, which provides regular email messages about conferences, events, projects, funding, new research and dissemination of members queries and requests’.
Department of Health Policy Research Programme Project – The effectiveness and cost effectiveness of complementary and alternative medicine (CAM) for multimorbid patients with mental health and musculoskeletal problems in primary care in the UK: a scoping study (The University of Bristol):
On 13th July this year, I received a circulated email from the Senior Research Associate at The School of Social and Community Medicine (University of Bristol) advising as follows:
‘…We are pleased to be able to let you know that our project ‘SCIM’ – “The effectiveness and cost effectiveness of complementary and alternative medicine (CAM) for multimorbid patients with mental health and musculoskeletal problems in primary care in the UK: a scoping study” has now finally been approved by the funders and the final report is available on their website. I have also attached our Executive Summary. I hope you find it interesting and please do get in touch with any feedback…We may well be in touch again over the summer as we progress with this piece of work and look for collaborators and input from the wider CAM, primary care and research communities…’
(The Executive Summary may be found here).
This is great news. Many congratulations to Professor Deborah Sharp and to her colleagues. There will, of course, be more about this project in my next blog (November 2017). In the meantime, CAM practitioners and others will no doubt welcome the opportunity to provide feedback and to respond to a request for further input to this project.
Professor George Lewith
Finally and most importantly, I add my belated (following its inexcusable omission from my blog in May) expressions of sadness and shock to those of countless others at the untimely and sudden death of Professor George Lewith for whom numerous obituaries have been recorded, including by the College of Medicine, the University of Southampton and The Research Council for Complementary Medicine. All practitioners, patients, students and researchers of CAM and orthodox medicine owe him so much. Along with those of many, my thoughts are with his family.
RICHARD EATON
1st August 2017
END OF QUOTE
Who is Richard Eaton?, I asked myself after reading this. The answer is here:
Richard Eaton LL.B (Hons) whose professional background is as a barrister (Bar Council – Academic Division) – now retired – and as a lecturer in law, believes that the future for practitioners of complementary and alternative medicine in private practice lies within well-managed Health Centres. He formerly owned and managed, together with his wife Marion Eaton LLB (Hons) Reiki Master Teacher, the Professional Centre for Holistic Health in Hastings, East Sussex. He now provides consultancy services through his company, Touchworks Ltd, including in relation to the practice management of CAM.
SAY NO MORE!!!
I have mentioned the German alt med phenomenon of the ‘Heilpraktiker’ before. For instance, a year ago I wrote this:
…The German ‘Heilpraktiker’ (literally translated: healing practitioner) is perhaps best understood by its fascinating history. When the Nazis came to power in 1933, German health care was dominated by lay practitioners who were organised in multiple organisations struggling for recognition. The Nazis felt the need to re-organise this situation to bring it under their control. At the same time, the Nazis promoted their concept of ‘Neue Deutsche Heilkunde’ (New German Medicine) which entailed the integration – perhaps more a shot-gun marriage – of conventional and alternative medicine. I have published about the rather bizarre history of the ‘New German Medicine’ in 2001:
The aim of this article is to discuss complementary/alternative medicine (CAM) in the Third Reich. Based on a general movement towards all things natural, a powerful trend towards natural ways of healing had developed in the 19(th)century. By 1930 this had led to a situation where roughly as many lay practitioners of CAM existed in Germany as doctors. To re-unify German medicine under the banner of ‘Neue Deutsche Heilkunde’, the Nazi officials created the ‘Heilpraktiker‘ – a profession which was meant to become extinct within one generation. The ‘flag ship’ of the ‘Neue Deutsche Heilkunde’ was the ‘Rudolf Hess Krankenhaus’ in Dresden. It represented a full integration of CAM and orthodox medicine. An example of systematic research into CAM is the Nazi government’s project to validate homoeopathy. Even though the data are now lost, the results of this research seem to have been negative. Even though there are some striking similarities between today’s CAM and yesterday’s ‘Neue Deutsche Heilkunde’ there are important differences. Most importantly, perhaps, today’s CAM is concerned with the welfare of the individual, whereas the ‘Neue Deutsche Heilkunde’ was aimed at ensuring the dominance of the Aryan race.
The Nazis thus offered to grant all alternative practitioners official recognition by establishing them under the newly created umbrella of ‘Heilpraktiker’. To please the powerful lobby of conventional doctors, they decreed that the ‘Heilpraktiker’ was barred from educating a second generation of this profession. Therefore, the Heilpraktiker was destined to become extinct within decades.
Several of the Nazi rulers were staunch supporters of homeopathy and other forms of alternative medicine. They hoped that alternative medicine would soon have become an established part of ‘New German Medicine’. For a range of reasons, this never happened.
After the war, the Heilpraktiker went to court and won the right to educate their own students. Today they are a profession that uses homeopathy extensively. The German Heilpraktiker has no mandatory medical training; a simple test to show that they know the legal limits of their profession suffices for receiving an almost unrestricted licence for practicing medicine as long as they want…
END OF QUOTE
Since about two years, a group of German scientists, clinicians and various other experts (I was a member of the panel), led by a prominent ethicist, worked on a document that was published this week. Here are its conclusions (in German):
Medizinische Parallelwelten mit radikal divergierenden Qualitätsstandards, wie sie aktuell im deutschen Gesundheitswesen in Form von Doppelstandards bei Ergebnisbewertung und Qualitäts kontrolle bestehen, sind für eine aufgeklärte Gesellschaft nicht akzeptabel. Bei Heilpraktikern stehen aufgrund ihrer ungenügenden, kaum regulierten Ausbildung die Qualifikationen und Tätigkeitsbefugnisse in einem eklatanten Missverhältnis. Heilpraktiker bieten schwer punktmäßig alternativ oder komplementärmedizinische Verfahren an, die in den meisten Fällen wissenschaftlich unhaltbar sind. Dies führt zu einer Gefährdung von Patienten. Abhilfe verspricht nur ein gleichzeitiges Vorgehen auf mehreren Ebenen:
(1.) eine einheitliche Bewertung der Patientendienlichkeit in allen Bereichen der Medizin;
(2.) ein verstärktes Engagement für die Erfordernisse einer gelingenden Kommunikation mit Patienten;
(3.) eine verstärkte Förderung wissenschaftstheoretischer Kompetenzen in Ausbildung und Studium gesundheitsbezogener Berufe; sowie
(4.) eine Abschaffung des Heilpraktikerwesens oder eine radikale Anhebung und Sicherstellung des Kompetenzniveaus von Heilpraktikern.
Wir haben uns hier auf die Reform des Heilpraktikerwesens konzentriert und dafür zwei Lösungsvorschläge skizziert: Wir empfehlen entweder die gänzliche Abschaffung des Heilpraktikerberufs oder dessen Ablösung durch die Einführung spezialisierter „FachHeilpraktiker“ als Zusatzqualifikation für bestehende Gesundheitsfachberufe. Für die Übergangsphase empfehlen wir eine gesetzliche Beschränkung des Heilpraktikerwesens auf weitgehend gefahrlose Tätigkeiten. Auf diese Weise ließen sich die Gefahren für Patienten reduzieren und die Patientenversorgung langfristig wesentlich verbessern.
END OF QUOTE
Essentially, we are saying that, the Heilpraktiker has introduced two hugely different quality standards into the German healthcare system. In the interest of the patient and of good healthcare, this double standard must be addressed. We are demanding the profession of the Heilpraktiker either is completely abolished, or is reformed such that it no longer poses a threat to public health in Germany. Our document makes concrete suggestions for such reforms.
Our suggestions have already received lots of attention in Germany, and we are therefore hopeful that they will be taken seriously, start a much-needed debate and eventually bring about progress.
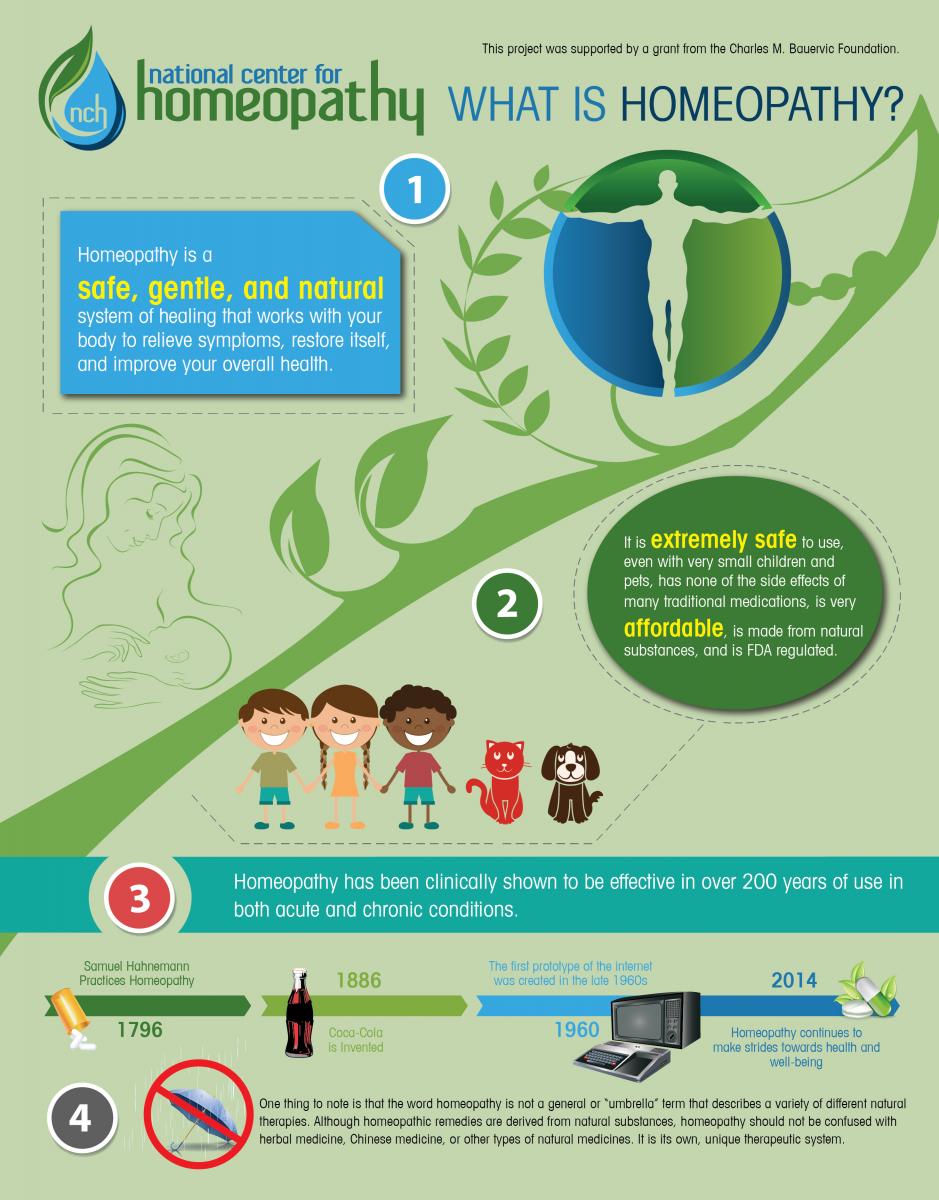
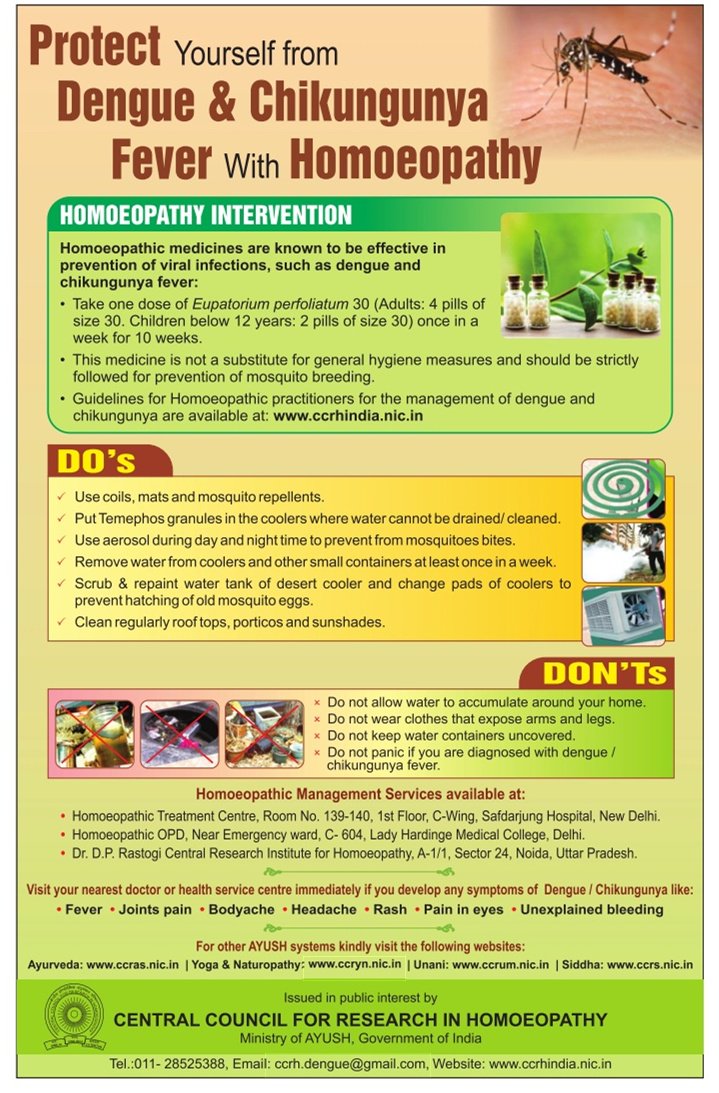
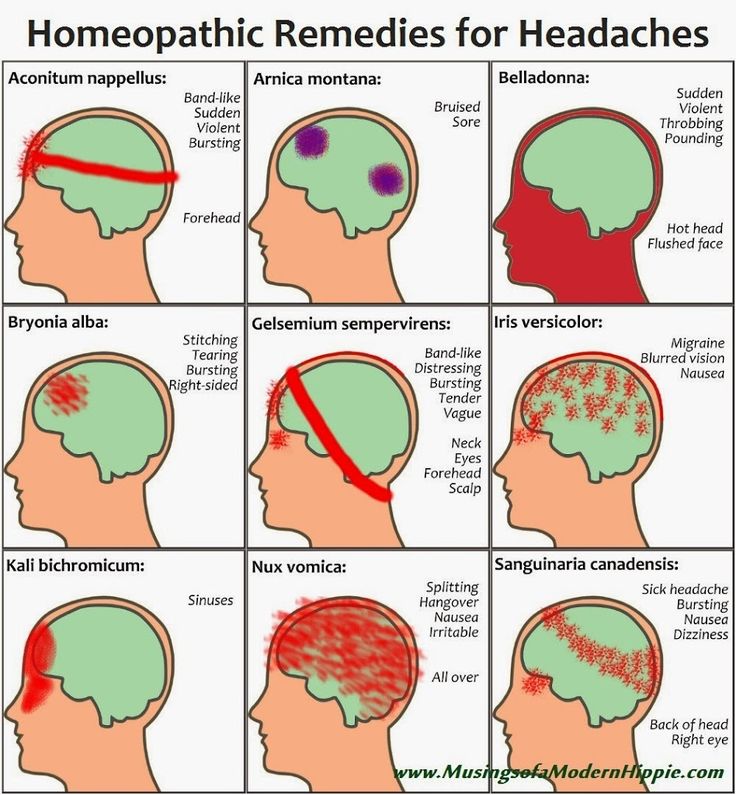
I have been collecting pictures posted by homeopaths on Twitter. When I say collection, I am exaggerating: it takes only about 10 minutes to find what I posted below.
Let’s hope that my collection cures some people from the desire to try homeopathy.
For those who, after having had a look at the pictures, still believe that there might be something in it, I have this challenge:
SHOW ME GOOD EVIDENCE FOR THE CLAIMS MADE BELOW, AND I WILL SEND YOU A FREE COPY OF MY RECENT BOOK ON THE SUBJECT.
[please click to see them full size]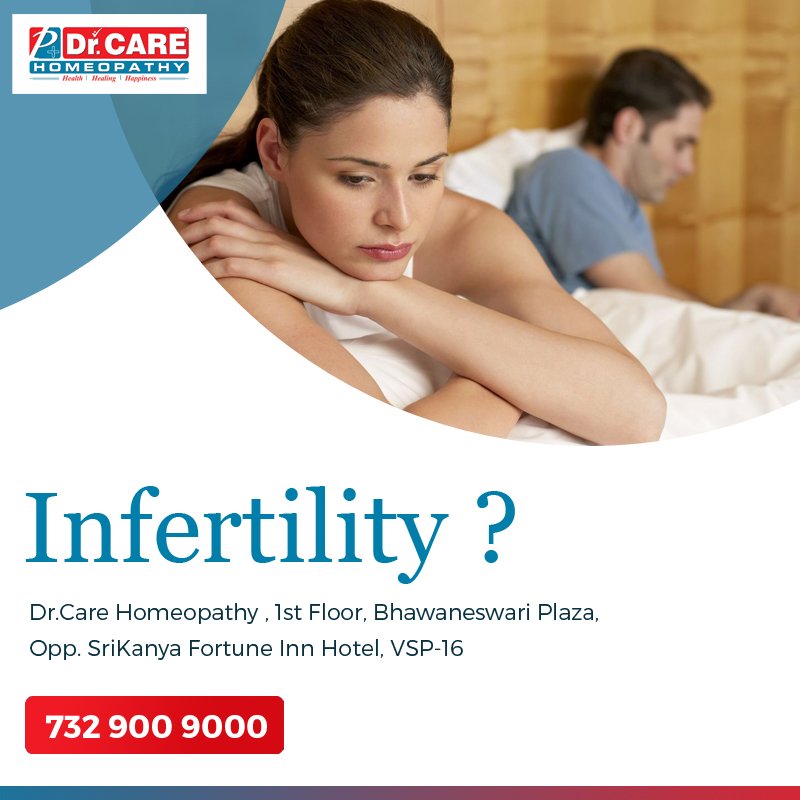












This article could well be proof that homeopathy is ineffective against paranoia.
START OF QUOTE
Given the fact that homeopathy has met with resistance simultaneously on multiple fronts, many are wondering if this is an organized effort. Dr. Larry Malerba, who has practiced homeopathic medicine for more than 25 years, says that he has never witnessed this level of antipathy toward holistic medicine before:
“When one considers the broad array of recent anti-homeopathy activities that cross international borders, it would be naïve to think that there wasn’t a common motivating influence. One has to wonder who stands to gain the most from this witch hunt.”
Homeopathy, in particular, is a thorn in the side of Pharma because of the fact that its unique medicines are FDA regulated, safe, inexpensive, and can’t be patented. Malerba asked the question,
“Could it be that the media is missing the larger story here, that a powerful medical monopoly is seeking to destroy one of its most successful competitors?”
In India, where homeopathy enjoys tremendous popularity, there are an estimated 250 thousand homeopathic practitioners. Indian homeopath, Dr Sreevals G Menon, seems to agree that there is something fishy going on. He recently wrote:
“The renewed and more vigorous attack on the efficacy of homoeopathy as a curative therapy picked up internationally by the media is nothing but a sinister pogrom by the powerful pharmaceutical corporations the world over.”
… Homeopathic supporters have long suspected that Pharma is secretly funding skeptic organizations. It appears that Pharma astroturfs by taking advantage of skeptic organizations that have strong anti-holistic medicine beliefs, encouraging them to spread false information about homeopathy.
But questions remain. Does this constitute an anti-democratic assault on freedom of medical choice? Are media outlets that have been manipulated by corporate medical interests feeding false information to consumers? Why is an increasingly popular medical therapy known for its long track record of safety suddenly receiving so much negative attention?…
END OF QUOTE
I do sympathize with those poor homeopathy fans!
Paranoia is a nasty condition!
And their placebos are useless for alleviating it.
Sad – really sad.
A recent comment by a chiropractor told us this:
“If the critics do not take step 2 [point out what’s right and support] then they are entrenched carpet bombers who see reform and reformers as acceptable collateral damage. That makes them just as much a part of the problem when it comes to reform as the subbies.”
Similar words have been posted many times before.
So, are we critics of chiropractic carpet bombers?
Personally, I find the term very distasteful and misplaced. But let’s not be petty and forget about the terminology.
The question is: should I be more supportive of chiropractors who claim to be reformers?
I feel that the claim to be a reformer is hardly enough for gaining my support. I prefer to support clinicians who do the right things. And what would that be?
Here is a list; clinicians would receive my support, if they:
- adhere to the principles of evidence-based medicine;
- follow the rules of medical ethics.
What does that mean in relation to chiropractic?
I think it means that clinicians should:
- use interventions that demonstrably do more good than harm,
- make no false claims,
- advocate the best available treatments for their patients,
- abstain from treating patients for which their therapy is not demonstrably effective,
- obtain fully informed consent from their patients which includes information about the nature of the condition, about the risks of their treatments, about other therapeutic options.
As soon as I see a chiropractor or a group of chiropractors who fit these criteria, I will support them by publicly stating that they are doing alright (as should be normal for responsible healthcare practitioners). Until this time, I reject being called a carpet bomber and call such name-calling a stupid defence of quackery.
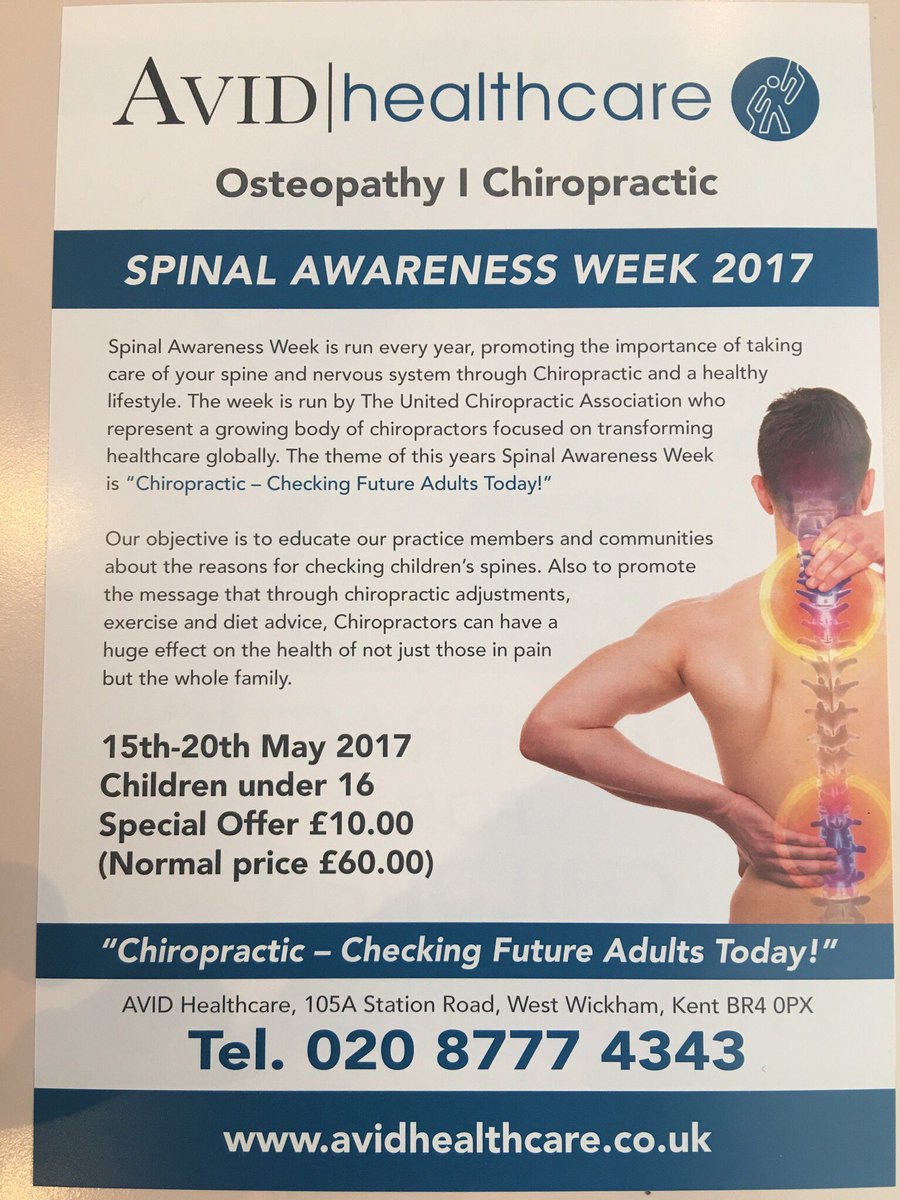
It is bad enough to mislead adult patients into believing that chiropractic is effective for conditions for which it is clearly not. However, it is far worse, in my view, to do that for paediatric conditions.
There is no doubt that chiropractors continue to treat children and advertise their services for childhood conditions. I am not aware of good evidence to show that chiropractic is effective for any childhood condition at all. Yet, whenever I or anyone else says so, we get ignored. Chiropractors do not accept this sort of criticism. This blog provides more than ample evidence for that, I believe.
Perhaps chiropractors are not good at reading?
Perhaps they only understand pictures?
As for my previous post, I have assembled here a few pictures posted by chiropractors on Twitter. They all relate to chiropractic treatments for children.
Why did I do that?
Because I hope that the many chiropractors who read my blog could now point us to the evidence that support the claims made in these advertisements. If they cannot do that, it would be an ethical imperative for them to clearly state that these posts are deceitful. If they fail to do this, they are tolerating quackery in their own ranks without objection – and that would render them unethical!
Or have I got this wrong???
[please click to see them full size]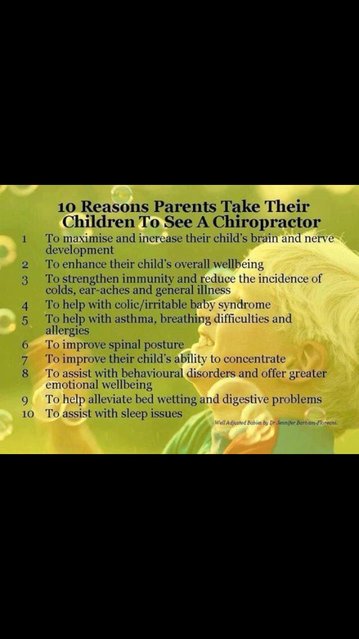











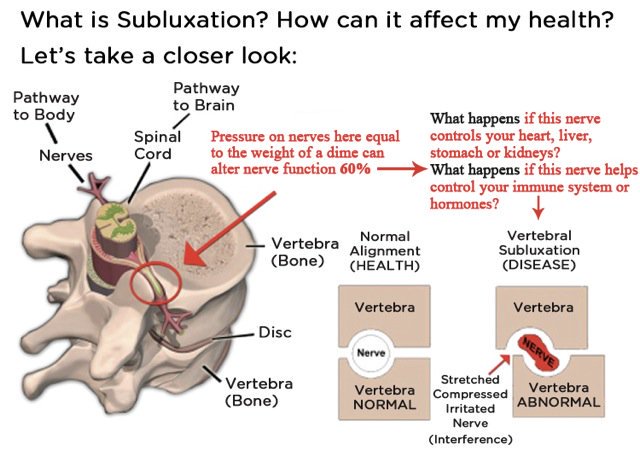
How often have we heard that chiropractic has moved on and has given up the concept of subluxation/malalignment? For sure there is no evidence for such nonsense, and it would be high time to give it up! But, as has been argued here and elsewhere, if chiros give it up, what is there left? What then would differentiate them from physios ? The answer is not a lot.
In any case, chiros have by no means given up subluxation. One can argue this point ad nauseam; yet, most chiros remain in denial.
For this post, I have chosen a different approach to make my point. I simply went on twitter and had a look what messages chiros tweet. The impression I got is that the majority of chiros are totally immersed in subluxation. To provide some proof, I have copied a few images – if chiros do not listen to words, perhaps they understand pictures, I thought.
So, here we go – enjoy!
[please click to see them full size]