
Updated Edition!
 for Cancer")





")









![]()

Have you ever wondered how good or bad the education of chiropractors and osteopaths is? Well, I have – and this new paper promises to provide an answer.
The aim of this study was to explore Australian chiropractic and osteopathic new graduates’ readiness for transition to practice concerning their clinical skills, professional behaviors, and interprofessional abilities. Phase 1 explored final-year students’ self-perceptions, and this part uncovered their opinions after 6 months or more in practice.
Interviews were conducted with a self-selecting sample of phase 1 participant graduates from 2 Australian chiropractic and 2 osteopathic programs. Results of the thematic content analysis of responses were compared to the Australian Chiropractic Standards and Osteopathic Capabilities, the authority documents at the time of the study.
Interviews from graduates of 2 chiropractic courses (n = 6) and 2 osteopathic courses (n = 8) revealed that the majority had positive comments about their readiness for practice. Most were satisfied with their level of clinical skills, verbal communication skills, and manual therapy skills. Gaps in competence were identified in written communications such as case notes and referrals to enable interprofessional practice, understanding of professional behaviors, and business skills. These identified gaps suggest that these graduates are not fully cognizant of what it means to manage their business practices in a manner expected of a health professional.
The authors concluded that this small study into clinical training for chiropractic and osteopathy suggests that graduates lack some necessary skills and that it is possible that the ideals and goals for clinical education, to prepare for the transition to practice, may not be fully realized or deliver all the desired prerequisites for graduate practice.
Their conclusions in the actual paper finish with these sentences, in the main, graduate participants and the final year students were unable to articulate what professional behaviors were expected of them. The identified gaps suggest these graduates are not fully cognizant of what it means to manage their business practices in a manner expected of a health professional.
In several ways, this is a remarkable paper – remarkably poor, I hasten to add. Apart from the fact that its sample size was tiny and the response rate was low, it has many further limitations. Most notably, the clinical skills, professional behaviors, and interprofessional abilities were not assessed. All the researchers did was ask the participants how good or bad they were at these skills. Is this method going to generate reliable evidence? I very much doubt it!
Imagine, these guys have just paid tidy sums for their ‘education’ and they have no experience to speak of. Are they going to be in a good position to critically evaluate their abilities? No, I fear not!
Considering these flaws and the fact that chiropractors and osteopaths are not exactly known for their skills of critical thinking, I find it amazing that important deficits in their abilities nevertheless emerge. If I had to formulate a conclusion from all this, I might therefore suggest this:
A dismal study seems to suggest that chiropractic and osteopathic schooling is dismal.
PS
Come to think of it, there might be another fitting option:
Yet another team of chiro- and osteos demonstrate that they don’t know how to do science.
Pancoast tumors, also called superior sulcus tumors, are a rare type of cancer affecting the lung apex. These tumors can spread to the brachial plexus and spine and present with symptoms that appear to be of musculoskeletal origin. Patients with an advanced Pancoast tumor may thus feel intense, constant, or radiating pain in their arms, around their chest wall, between their shoulder blades, or traveling into their upper back or armpit. In addition, a Pancoast tumor may cause the following symptoms:
- Swelling in the upper arm
- Chest tightness
- Weakness or loss of coordination in the hand muscles
- Numbness or tingling sensations in the hand
- Loss of muscle tissue in the arm or hand
- Fatigue
- Unexplained weight loss
This case report details the story of a 59-year-old Asian man who presented to a chiropractor in Hong Kong with a 1-month history of neck and shoulder pain and numbness. His symptoms had been treated unsuccessfully with exercise, medications, and acupuncture. He had a history of tuberculosis currently treated with antibiotics and a 50-pack-year history of smoking.
Cervical magnetic resonance imaging (MRI) revealed a small cervical disc herniation thought to correspond with radicular symptoms. However, when the patient did not respond to a brief trial of chiropractic treatment, the chiropractor referred the patient back to the chest hospital for further testing, which confirmed the diagnosis of a Pancoast tumor. The patient was then referred for medical care and received radiotherapy and chemotherapy. At 2 months’ follow-up, the patient noted feeling lighter with less severe neck and shoulder pain and numbness. He also reported that he could sleep longer but still had severe pain upon waking for 2–3 hours, which subsided through the day.
A literature review identified six previously published cases in which a patient presented to a chiropractor with an undiagnosed Pancoast tumor. All patients had shoulder, spine, and/or upper extremity pain.
The authors concluded that patients with a previously undiagnosed Pancoast tumor can present to chiropractors given that these tumors may invade the brachial plexus and spine, causing shoulder, spine, and/or upper extremity pain. Chiropractors should be aware of the clinical features and risk factors of Pancoast tumors to readily identify them and refer such patients for medical care.
This is an important case report, in my view. It demonstrates that symptoms treated by chiropractors, osteopaths, and physiotherapists on a daily basis can easily be diagnosed wrongly. It also shows how vital it is that the therapist reacts responsibly to the fact that his/her treatments are unsuccessful. Far too often, the therapist has an undeniable conflict of interest and will say: “Give it more time, and, in my experience, symptoms will respond.”
The chiropractor in this story was brilliant and did the unusual thing of not continuing to treat his patient. However, I do wonder: might he be the exception rather than the rule?
This randomized clinical trial (RCT) tested whether acupuncture is effective for the prevention of chronic tension-type headaches (CTTH). The researchers recruited 218 participants who were diagnosed with CTTH.
- The participants in the intervention group received 20 sessions of true acupuncture (TA group) over 8 weeks. The acupuncture treatments were standardized across participants, and each acupuncture site was needled to achieve deqi sensation. Each treatment session lasted 30 minutes.
- The participants in the control group received the same sessions and treatment frequency of superficial acupuncture (SA group)—defined as a type of sham control by avoiding deqi sensation at each acupuncture site.
The main outcome measure was the responder rate at 16 weeks after randomization. Followed-up was 32 weeks. A responder was defined as a participant who reported at least a 50% reduction in the monthly number of headache days (MHDs).
The responder rate was 68.2% in the TA group (n=110) versus 48.1% in the SA group (n=108) at week 16 (odds ratio, 2.65; 95%CI, 1.5 to 4.77; p<0.001); and 68.2% in the TA group versus 50% in the SA group at week 32 (odds ratio, 2.4; 95%CI, 1.36 to 4.3; p<0.001). The reduction in MHDs was 13.1±9.8 days in the TA group versus 8.8±9.6 days in the SA group at week 16 (mean difference, 4.3 days; 95%CI, 2.0 to 6.5; p<0.001), and the reduction was 14±10.5 days in the TA group versus 9.5±9.3 days in the SA group at week 32 (mean difference, 4.5 days; 95%CI, 2.1 to 6.8; p<0.001). Four mild adverse events were reported; three in the TA group versus one in the SA group.
The authors concluded that the 8-week TA treatment was effective for the prophylaxis of CTTH. Further studies might focus on the cost-effectiveness of the treatment.
“Our study showed that deqi sensation could enhance the effect of acupuncture in the treatment of chronic TTH, and the effect of acupuncture lasted at least 6 months when the treatment was stopped,” said co-investigator Ying Li, MD, PhD, The Third Hospital/Acupuncture and Tuina School, Chengdu University of Traditional Chinese Medicine, Chengdu, China.
Why am I not convinced?
Assuming that all the findings are correctly reported, the study does not at all show that the treatment was effective. It merely demonstrates that those patients who knew that were receiving TA told the researcher that they improved more than those who knew they has sham acupuncture. The difference in outcomes is not in the least surprising: patients’ knowledge of having had the verum leads to a placebo effect and to social desirability (patients giving the researchers positive responses simply because they were thankful for being looked after). Patients’ knowledge of having had the sham treatment leads to disappointment and thus worse outcomes.
But this is not the only reason why I am skeptical about this study. The authors claim they achieved deqi at every treatment. That is 20 treatments in 110 patients or 2 200 deqis! I think someone might be telling porkies here. Deqi cannot reliably be elicited on every single occasion. I, therefore, feel that perhaps the authors of this trial were a bit more than generous when writing up their study, and I am reminded of the recent report claiming that more than 80% of clinical trial data from China are fabricated.
One of my recent posts prompted the following comment from a chiropractor: “… please don’t let me stop you…while we actually treat patients“. It was given in the context of a debate about the evidence for or against chiropractic spinal manipulations as a treatment of whiplash injuries. My position was that there is no convincing evidence, while the chiropractor argued that he has been using manipulations for this indication with good results. Here I do not want to re-visit the pros and cons of that particular debate. Since similar objections have been put to me so many times, I want rather to raise several more principal points.
Before I do this, I need to quickly get the personal stuff out of the way: the comment implies that I don’t really know what I am talking about because I don’t see patients and thus don’t understand their needs. The truth is that I started my professional life as a clinician, then I went into basic science, then I went back into clinical medicine (while also doing research), and eventually, I became a full-time clinical researcher. I have thus seen plenty of patients, certainly enough to empathize with both the needs of patients and the reasoning of clinicians. In fact, these provided the motives for my clinical research during the last decades of my professional career (more details here).
Now about the real issue that is at stake here. When offered by a clinician to a scientist, the comment “… please don’t let me stop you…while we actually treat patients” is an expression of an arrogant feeling of superiority that clinicians often harbor vis a vis professionals who are not at the ‘coal face’ of healthcare. Stripped down to its core, the argument implies that science is fairly useless because the only knowledge worth having stems from dealing with patients. In other words, it is about the tension that so often exists between clinical experience and scientific evidence.
Many clinicians feel that experience is the best guide to correct decision-making.
Many scientists feel that experience is fraught with errors, and only science can lead us towards optimal decisions.
Such arguments emerge regularly on this blog and are constant company to almost any type of healthcare. The question is, who is right and who is wrong?
As I indicated, I can empathize with both positions. I can see that, in the context of making therapeutic decisions in a busy clinic, for instance, the clinician’s argument weighs heavily and can make sense, particularly in areas where the evidence is mixed, weak, or uncertain.
However, in the context of this blog and other discussions focused on critical evaluation of the science, I am strongly on the side of the scientist. In fact, in this context, the argument “… please don’t let me stop you…while we actually treat patients” seems ridiculous and resembles an embarrassing admission of having no rational argument left for defending one’s own position.
To put my view of this in a nutshell: it is not a question of either or; for optimal healthcare, we obviously need both clinical experience AND scientific evidence (an insight that is not in the slightest original, since it is even part of Sackett’s definition of EBM).
WHAT?
Biblical naturopathy?
Yes, it is not a hoax; it does exist!
It’s another so-called alternative medicine (SCAM) that is new to me.
This website explains what it is all about:
The Biblical Naturopathic Philosophy is based on the following principles:
Do no harm
God has designed the body to be self-healing
Recognize the healing power of nature as designed by God
Recognize the supernatural healing power of God
The natural and supernatural work together
God has made provision for recovery of sickness
Identify the cause and source
Involve the total person (body, soul, spirit)
Support the body rather than treat symptoms
Health is maintained through Biblical patterns and principles
What do we believe?
We believe the Bible is the inspired, inerrant Word of God. (2 Tim. 3:16-17; 2 Pet. 1-20).
We believe God is the Creator and Sustainer of the universe. (Gen. 1; John 1:3; Col. 1:16; Heb. 1:3).
We believe Jesus is both Lord and Christ, to the glory of God the Father. (Acts 1:9-11; 2:36; Phil. 2:9-11).
We believe that whosoever will confess with their mouth that Jesus is Lord and believes in their heart God raised Him from the dead shall be saved. (Rom. 10:9-10; Acts 2:21; 1 John 1:12).
We believe that the Holy Spirit is sent by Jesus to indwell, empower, teach, guide and comfort believers. (Luke 12:12; Rom. 8-11; John 16:13; Acts 1:7-8, 9:31).
We believe that the Lord Jesus’ death, burial, and resurrection from the dead provided for the healing of the spirit, soul, and bodies of all peoples.
We believe in the imminent return of Jesus Christ, who will come to rule as King upon the earth with the saints. (Acts 1:9-11; 1Thess. 4:13-5:2; Rev. 19:11-21, 22:20).
And this is what they offer in terms of coursework:
COUNSELING
CNS101 Christian Counseling
Covers ethics, foundations of faith, makeup of man, motivational gifts and personality, Faith-Based Therapy™, leading someone into salvation, identity / position / purpose / significance in Christ, scriptural concordance, basics of counseling, opening a counseling center, recognizing mental illness, initial forms and assessments, value of nutrition, and legal issues.
CNS102 Advanced Christian Counseling
Covers stress, co-dependency, self-esteem, anger, forgiveness, premarital and marriage counseling, divorce, family issues, blended families, depression, suicide, grief / loss, anxiety, obsessive-compulsive, sexual abuse, sexual addictions, and reality disassociation.
CNS103 Drug & Alcohol Recovery (GOD14®)
Provides an overview of drug and alcohol education, sin and disease of alcoholism, identifying the addict, AA and NA, scriptural steps, relapse and enabling, family dynamics, steps to breaking physical and psychological addiction, prescription drugs, screening, neurotransmitters, chemistry rebalancing, recovery flowchart, detox categories, and forms and assessments.
BIBLICAL
BIB210 Ministerial Ethics
All ministers should hold themselves above reproach. This course will challenge as well as encourage spiritual ethics beyond a secular view.
BIB220 Ecclesiastical Ordinances
This course outlines the duties required of ministers such as baptism, funerals, weddings, etc. The course is designed to prepare the licensed or ordained minister to structure and carry out ministerial duties.
BIB230 Doctrinal Foundations
The foundations of the Christian faith are scripturally established. Every minister should be able to give an account of what they believe and why. This course is designed to assist rather than to indoctrinate.
BIB270 Biblical Naturopathy
What is a Biblical naturopathic doctor; Biblical philosophy of healing; Creation and makeup of man; Scriptural principles for understanding and restoring health; Causes of disease; Things that block healing; History of naturopathy; Naturopathic tenets / axioms; Forefathers of health and healing; The mind & heart of God – It is God who heals; Health in America; Introduction to the techniques of health evaluation; Introduction to the healing modalities; Genetics, predispositions, generational curses; Biblical examples of natural healing; Physical to spiritual analogies; Foods of the Bible; Emotions and organs.
BIB280 Understanding & Improving Health
Health in America, History of Nutrition; Water and Sunshine; What is Protein?; What are Carbohydrates?; What are Fats, Oils, and Fatty Acids?; Issues with Sugar, Milk, Soy, MSG, Aspartame, and Genetically Modified Foods; Dietary Guidelines; Diets and Dieting; and Nutritional Deficiencies; Exercise; Biblical Principles and Perspectives; Confronting Sickness and Disease; Practical Support.
BIB290 How to Pray for Healing
Understanding who we are in Christ; The authority of the believer; The role of faith in prayer; The benefit of confession; Praying for guidance; How to pray for physical healing; Praying for Inner Healing; A balanced approach to understanding deliverance; Understanding spiritual warfare.
BIB300 Biblical Freedom Techniques
Forgiveness; Generational curses; Demonic influences; Demonic influences for sickness; Evil spirits as a cause of sickness; Biblical examples; Types of spirits; Strongholds; How do you know?; How to remove evil spirits; Inner healing.
DIET AND GENERAL WELLNESS
DGW310 Biblical Eating
Biblically speaking, are there certain foods best not eaten? What does the Bible have to say about diet and why? God has said plenty about the diet best suited for His creation.
DGW320 Biblical Health Principles
Times have changed, but the Bible and its principles have not. Learn basic principles that can be applied for maintaining health while understanding some of the changes to our foods. Have we become addicted to certain foods? This course teaches how to have a healthy diet and live healthy in a not-so-healthy world.
DGW330 Wellness with Weight Loss
For many, losing weight is a never-ending struggle — especially since our bodies are designed to keep weight on at all costs; it’s a matter of survival. But a medical revolution is under way, showing us how to work with our bodies instead of against them to ignite the natural fat-burning furnaces that lie dormant within us. Drawing on the cutting-edge science of nutrigenomics — how food talks to our genes — Dr. Mark Hyman has created a way of losing weight by eating the right foods, which in turn sends the right messages to our bodies. In this easy-to-follow eight-week plan based on each individual’s unique genetic needs, Dr. Hyman explains how to customize your personal weight-loss program with menus, recipes, shopping lists, and recommendations for supplements and exercise. Ultimately, you will rebalance and stabilize your metabolism — an UltraMetabolism — to maintain weight loss and enjoy lifelong health.
NUTRITION
NUT410 Digestion & Enzymes
Digestion Enzyme therapy is an emerging successful alternative for restoring health. Learn the basics of digestion along with how enzymes work and the benefits to immune function, pain reduction, mood stabilization, and mental clarity, and more. Discover the inexpensive yet highly effective digestive enzymes needed to restore digestive, neurological, and behavioral health.
NUT420 Nutrition 1
This is a comprehensive course that will guide you to achieve and maintain a high level of health and fitness through careful dietary planning and nutritional supplements. The elements of health are discussed along with recommendations for a multitude of conditions. This course is also a guide to various alternative remedies and therapies.
NUT430 Nutrition 2
This course provides a thorough resource and reference to natural supplements, herbs, and homeopathic remedies as well as relating them to all the major ailments and health conditions. The information is thoroughly documented by scientific data and research.
NUT435 Biblical Eating and Clinical Nutrition
What is food?; Protein, fats, carbohydrates; Foods of today; Biblical foods and diets; Food sources of vitamins and minerals; Vitamins and deficiency symptoms; Minerals and deficiency symptoms; Amino acids; Enzymes; Neutraceuticals; Synthetic verses whole food vitamins; Nutritional deficiencies as a cause of diseases; Diets and individualism; Nutrition deficiency questionnaire; Therapeutic clinical nutrition
NUT440 Emotional Biochemistry
Learn how to screen for emotional and behavioral symptoms. Recognize the mental and physical clues that indicate biochemical imbalances, particularly in the brain. This course teaches natural ways of dealing with physiological causes of depression, anxiety, paranoia, anger, emotional instability, and addictions to prescription and non-prescription drugs.
NUT450 Hair Tissue Mineral Analysis
This course teaches more than just knowing the levels of good and toxic minerals in the body from hair tissue analysis. How do you balance the levels and what do the ratios mean? Hair analysis can also reveal immune system problems, emotional trends, cellular energy levels, glucose intolerance, kidney and liver stress, adrenal and thyroid activity and more.
BOTANICAL
BOT510 Herbs of the Bible
What herbs were used in Bible times? The herbs of the Bible are reviewed in light of their past and present uses. Precautions are also explained.
BOT520 Herbal Pharmacy
This is a comprehensive course reviewing the best herbs for healing, including complete herb forms, benefits, parts used, side effects, dosages and remedies for hundreds of ailments.
BOT530 Nutritional Herbology
This course teaches the nutritional components of herbs and how to determine an herb’s medicinal property. You will also learn the active chemical(s) behind an herb’s use that makes it effective. Classification of herbs and which herbs are commonly used for certain body systems is covered.
BOT540 Way of Herbs
This course blends the Eastern, European, and American Indian herbal healing traditions. Learn the three functions of herbs and the eight traditional methods of herbal therapy. Included are detailed descriptions and dosages of over 140 western herbs and 31 Chinese herbs.
BOT550 Herbals Systems
This course covers the Chinese and Ayurvedic classification of herbs and foods, and the classification of over 400 medicinal herbs available in the west, according to properties and actions. The preparation and processing of herbs is also covered.
BOT555 Leaves of the Tree (Revelation 22:2) Herbology
Comprehensive course covering the use of herbs; herb forms, benefits, parts used, side effects, dosages and recommendations for ailments; Classification of herbs and which herbs are commonly used for certain body systems.
BOT560 Aromatherapy
Science is now confirming that essential oils have healing properties for most physical and emotional conditions. This course is a hands-on guide to the understanding and use of essential oils.
ALTERNATIVE OR ANALYTICAL STUDIES
AAS610 Biblical Strategies
Is there a spiritual strategy for overcoming sickness? What choices are available when faced with terminal illnesses? This course reveals traditional as well as non-traditional natural strategies for defeating sickness and regaining health, particularly if facing death.
AAS620 Parasitology
How prevalent are parasites? What tests are available to determine if you have parasites? What role do they play in allergies, fatigue, bowel disorders, and immune function? What are the latest drugs, treatment, and herbal remedies?
AAS630 Energetic Testing
This course is a basic guide to bio-kinesiology and nutritional therapy using muscle response testing. Learn antidotal therapies using vitamins, minerals, herbs, amino acids, and homeopathic remedies.
AAS645 The Lamp of the Body 1 (Matt. 6:22) Sclerology (Basic and advanced)
Sclerology is easy to learn. Sclerology is the study of the red lines in the white of the eyes and how they relate to stress-patterns in a person’s health. What is a person’s predisposition to disease? What is the hidden cause of symptoms? What will the health challenges be five years from now? The lines in the sclera change as health conditions change. Thus Sclerology is an excellent way to confirm that a natural therapy is working. Are cold hands and feet a circulatory, thyroid, constitutional-vitality, or immunological problem? What is the key to losing weight? Is it glucose metabolism, the endocrine glands, the liver, or an allergy pattern? Is chronic fatigue attributed to a chronic infection, a weak endocrine system (thyroid/adrenals), an exhausted immune system, a liver weakness? The answer is reflected in the sclera!
AAS655 The Lamp of the Body 2 (Matt. 6:22) Iridology (Basic and advanced)
Anatomy & Physiology of the Eye; Topography/mapping; Physical Integrity Evaluation; Color Constitutional Types & Subtypes; Specific Iris Structure Irregularities; Specific Iris Pigmentation Irregularities; Misc. Signs; Collarets Signs; Syndromes; Sclera & Conjunctiva Signs; Deviation in Contraction Furrows; Exceptions to the Rules; Case Studies; Combination of Signs; Introduction to Time Risk; Iridology practice suggestions.
AAS665 The Body Electric (Genesis 2:7) – Energetic Response Testing
Our bodies, made from the dust of the earth, are very electric. Using electro-magnetic principles it is possible to determine which areas of the body are stressed and what nutrients are needed. Step-by-step hands-on training is provided in how to use and integrate Energetic Response Testing. – Brief History; Preliminaries Before Testing; The Arm Technique; Ways of Verifying a Weak Response; Why Does it Work?; Twelve Things That Can Block the Body’s Ability to Heal; Terms and Techniques; Correcting “Reversed Polarity”; Correcting “Switching”; Correcting “Blocked Regulation”; Response Testing Points (organs, glands, systems, nutritional).
AAS670 Serum Blood Analysis
This course presents an analytical system of blood chemistry and CBC analysis that focuses on physiological function as a marker of health. Optimal values are presented that increase our ability to detect dysfunction long before disease manifests. This course covers an in-depth coverage of 52 blood tests, 62 patterns of functional disorders, and 11 nutrient deficiencies, as well as correlating non-invasive in-office functional tests.
AAS685 Functional Analysis
Functional testing without labs: pH, tongue, fingernails, face, and body signs; Functional testing with laboratory assessments: hair, blood, urine, saliva, neurotransmitters, and hormones; Heavy metals; Food sensitivities; Strategies and applications.
NATUROPATHIC
NAT710 Naturopathic Heritage and Future
This course is the primer on principles and practice of naturopathy. It covers the history of naturopathy, its philosophy, the laws of disease and cure, and explains the modalities used by naturopaths.
NAT720 Homeopathy
Homeopathy is a natural, safe, inexpensive, and highly effective complement to any modality as well as to conventional medicine. You will learn the laws of homeopathy, how to assess illness, identify clues that point to the right remedy, individualize the remedy, and how to know when medical treatment is required.
NAT730 Detoxification
We live in a toxic world. This course outlines the steps needed to thoroughly detoxify and cleanse your body through fasting, juicing, oxygen therapy, exercise, heat therapy, colon cleansing, kidney cleansing, liver cleansing, and herbal detoxification.
NAT735 Cleansing the Temple
Why detox?; A cause of disease; Elimination organs/channels; Levels of detoxification; Lymph system; Fasting/exercise; Detox side effects; Avoiding a healing crisis; Foods to assist/avoid; Heavy metals; Pathogens; Infrared sauna; Ionic foot baths; Coffee enemas.
NAT740 Anatomy
Illustrated with detailed colored drawings, this course is a road map to the human body. With descriptive text, this course will educate you about the position and basic functions of all the organs and systems of the body.
NAT750 Functional Anatomy
An advanced level of anatomy is presented with more detailed information of the organs and bodily systems. With 210 color illustrations depicting all organs and systems, this course covers basic principles with special emphases on function.
NAT755 Fearfully and Wonderfully Made – Anatomy and Physiology
Basic anatomy and physiology; Understanding the Pathology of sickness and disease, Common disease conditions (this course meets the requirements for certification with International Iridology Practitioner’s Association).
NAT760 Reflexology
Reflexology is a unique system of foot massage, which can treat and prevent a wide variety of ailments. This course covers the history of reflexology, interpreting the feet, basic techniques, the treatment sequence, and an understanding of the meridian system.
NAT770 Naturopathic Jurisprudence
This course covers the legal guidelines for unlicensed practitioners. Learn what your rights are, what the constitution has to say, and what to do if legal disputes arise. Some topics included are insurance, licensing verses certification, correct and incorrect usage of words, and legal consent and disclaimer forms.
NAT775 Establishing a Naturopathic Ministry
Starting a practice; Setting up a business; Operating as a ministry; Legalities; Ethics; Referrals; Evaluation forms; Assessments; Record keeping; Accounting and inventory; Taxes; Advertising; Vendors; Equipment; Business management, Practice management, Introduction to flower essences, Introduction to homeopathy, Introduction to essential oils, Conducting an evaluation, Disorders, Therapeutic Applications, Unusual conditions.
_____________________________
Chad Hayes who has studied the subject in some detail has published an excellent article about Biblical Naturopathy which is well-worth reading. Here are his conclusions:
So what is biblical naturopathic medicine? It’s untrained, unqualified, unlicensed practitioners that believe their religion makes them immune from government oversight. It’s people that think two individuals signing a contract to call something what it’s not prevents them from being subject to laws designed to keep people safe. It’s delusional people that don’t want to be held accountable for the things they do, doing things they shouldn’t. It’s people that are so arrogant to think that their holy book, written thousands of years before we discovered germ theory, during a time when seizures and schizophrenia were attributed to demonic possession, by authors that never intended for it to be used as a medical text, gives them superior knowledge to those of us who respect our patients enough to spend years actually studying medicine and who are willing to be held accountable for our actions. It’s biblical literalists that disingenuously omit the abortion potion recipe provided by the LORD in Numbers 52 from their biblical naturopathy curriculum, while voting for legislators who put the lives of their constituents at risk by criminalizing abortion and putting a bounty on the heads of pregnant people and the physicians that have devoted their careers to caring for them.
__________________________
In a nutshell:
Biblical Naturopathy is yet another SCAM that I recommend avoiding.
Why?
Because it is dangerous nonsense.
One of my previous posts was about a press release announcing a ‘WORLDWIDE DECLARATION’, and I promised to comment about the actual declaration. This post firstly reproduces this document and secondly provides a few comments on it. Here is the document:
DEFINITIONS
Traditional, complementary and integrative healthcare (TCIH) refers to the respectful collaboration between various systems of healthcare and their health professionals with the aim of offering a person-centred and holistic approach to health.
ABOUT US
We represent a worldwide community of users and health professionals of TCIH with a large diversity of backgrounds and experiences with a common commitment to the advancement and
promotion of TCIH.
THE HEALTHCARE WE DESIRE
• Focuses on the whole person, including physical, mental, social and spiritual dimensions
• Is patient-centred and supports self-healing and health creation
• Is participative and respects individual choices
• Is evidence-based by integrating clinical experience and patient values with the best available research information
• Respects cultural diversity and regional differences
• Is an integral part of community and planetary health
• Uses natural and sustainable resources that are respectful of the health of our planet
• Integrates traditional, complementary and biomedical practices in a supportive and collaborative manner
We appreciate the benefits of conventional / biomedicine. At the same time we recognize its limitations, including:
• The insufficient therapeutic options that biomedicine provides, especially for chronic / non-communicable diseases (NCDs)
• Frequent side effects of biomedical treatments and rising antimicrobial resistance
• Fragmentation of care from increased specialization and the limits of a disease-based model
We are inspired by countries that are successfully integrating TCIH into their healthcare systems. However, we are concerned about:
• Countries that prevent, limit or undervalue the practice of TCIH
• Uninformed or unbalanced media reporting of TCIH
• Insufficient public funding of TCIH research
• Risk of reduced availability of TCIH and unregulated practices in some countries
OUR CALL TO ACTION
All countries
• Ensure full access to TCIH as part of the right to health for all
• Include TCIH into national health systems
• Provide accreditation of TCIH healthcare professionals in accordance with international training standards to ensure high quality care
• Ensure access and safety of TCIH medicines through specific regulatory pathways
• Fund research on TCIH and disseminate reliable information on TCIH to the public
All healthcare professionals
• Foster respectful collaboration between all healthcare professions towards achieving a person-centred and holistic approach to healthcare
_____________________________
And here are my comments.
- “TCIH”: in the realm of so-called alternative medicine it seems popular to create a new name for the subject at hand; this one is yet another one in a long line of innovations – sadly, it is as nonsensical as most of the previous ones.
- Person-centred and holistic approach to health: all good healthcare has these qualities.
- We represent a worldwide community: really? Who exactly are you then, and what is your ligitimization?
- Whole person, including physical, mental, social and spiritual dimensions: all good healthcare has these qualities.
- Patient-centred and supports self-healing and health creation: all good healthcare has these qualities.
- Respects individual choices: all good healthcare has these qualities.
- Evidence-based: either they do not know what this term means or they are deliberately misleading the public.
- Integral part of community and planetary health: all good healthcare has these qualities.
- Natural and sustainable resources that are respectful of the health of our planet: like Rhino horn and similar ingredients of TCM products?
- Insufficient therapeutic options that biomedicine provides: yes, conventional medicine is far from perfect, but adding something even less perfect to it cannot improve it.
- Frequent side effects of biomedical treatments and rising antimicrobial resistance: yes, conventional medicine is far from perfect, but adding something even less perfect to it cannot improve it.
- Full access to TCIH as part of the right to health for all: the ‘right to health for all’ means the right to the most effective therapies not the right to the most bizarre quackery.
- Accreditation of TCIH healthcare professionals: giving respectability to every quack would not render healthcare better or safer but worse and more dangerous.
- Access and safety of TCIH medicines through specific regulatory pathways: regulating access to unproven treatments is nothing less than a recipe for disaster.
- Research on TCIH: yes in some areas, research might be worthwhile, but it must be rigorously testing TCIH and not promoting it uncritically.
- Disseminate reliable information on TCIH to the public: thank you! This is my main aim in writing the ~2500 posts on this blog. Yet I do often get the impression that this gets disappointingly little support – and frequently the exact opposite – from enthusiasts of TCIH.
If you go on Twitter you will find that chiropractors are keen like mustard to promote the idea that, after a car accident, you should consult a chiropractor. Here is just one Tweet that might stand for hundreds, perhaps even thousands:
Recovering from a car accident? If you have accident-related injuries such as whiplash, chiropractic care may provide relief. Treatments like spinal manipulation and soft tissue therapy can aid in your recovery.
In case you don’t like Twitter, you could also go on the Internet where you find hundreds of websites that promote the same idea. Here are just two examples:
There is no question, chiropractors earn much of their living by treating patients suffering from whiplash (neck injury caused by sudden back and forth movement of the neck often causing neck pain and stiffness, shoulder pain, and headache) after a car accident with spinal manipulation.
Why?
There are two not mutually exclusive possibilities:
- They think it is effective.
- It brings in good money.
I have no doubt about the latter notion, yet I think we should question the first. Is there really good evidence that chiropractic manipulations are effective for whiplash?
When I was head of the PMR department at the University of Vienna, treating whiplash was my team’s daily bread. At the time, our strategy was to treat each patient according to the whiplash stage and to his/her individual signs and symptoms. Manipulations were generally considered to be contra-indicated. But that was about 30 years ago. Perhaps the evidence has now changed. Perhaps manipulation therapy has been shown to be effective for certain types of whiplash injuries?
To find out, I did a few Medline searches. These did, however, not locate compelling evidence for spinal manipulation as a treatment of any stage of whiplash injuries. Here is an example of the evidence I found:
In 2008, the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders (Neck Pain Task Force) found limited evidence on the effectiveness of manual therapies, passive physical modalities, or acupuncture for the management of whiplash-associated disorders (WAD) or neck pain and associated disorders (NAD). This review aimed to update the findings of the Neck Pain Task Force, which examined the effectiveness of manual therapies, passive physical modalities, and acupuncture for the management of WAD or NAD. Its findings show the following: Evidence from 15 evaluation studies suggests that for recent neck pain and associated disorders grades I-II, cervical and thoracic manipulation provides no additional benefit to high-dose supervised exercises.
But this is most puzzling!
Why do chiropractors promote their manipulations for whiplash, if there is no compelling evidence that it does more good than harm? Again, there are two possibilities:
- They erroneously believe it to be effective.
- They don’t care but are in it purely for the money.
Whatever it is – and obviously not all chiropractors would have the same reason – I must point out that, in both cases, they behave unethically. Not being informed about the evidence related to the interventions used clearly violates healthcare ethics, and so does financially not informing and exploiting patients.
Sixty thousand people are diagnosed with Parkinson’s disease (PD) each year, making it the second most common neurodegenerative disorder. PD results in a variety of gait disturbances, including muscular rigidity and decreased range of motion (ROM), that increase the fall risk of those afflicted. Osteopathic manipulative treatment (OMT) might address the somatic dysfunction associated with neurodegeneration in PD. Moreover, osteopathic cranial manipulative medicine (OCMM) might improve gait performance by improving circulation to the affected nervous tissue. Are these ideas realistic hypotheses or merely wishful thinking?
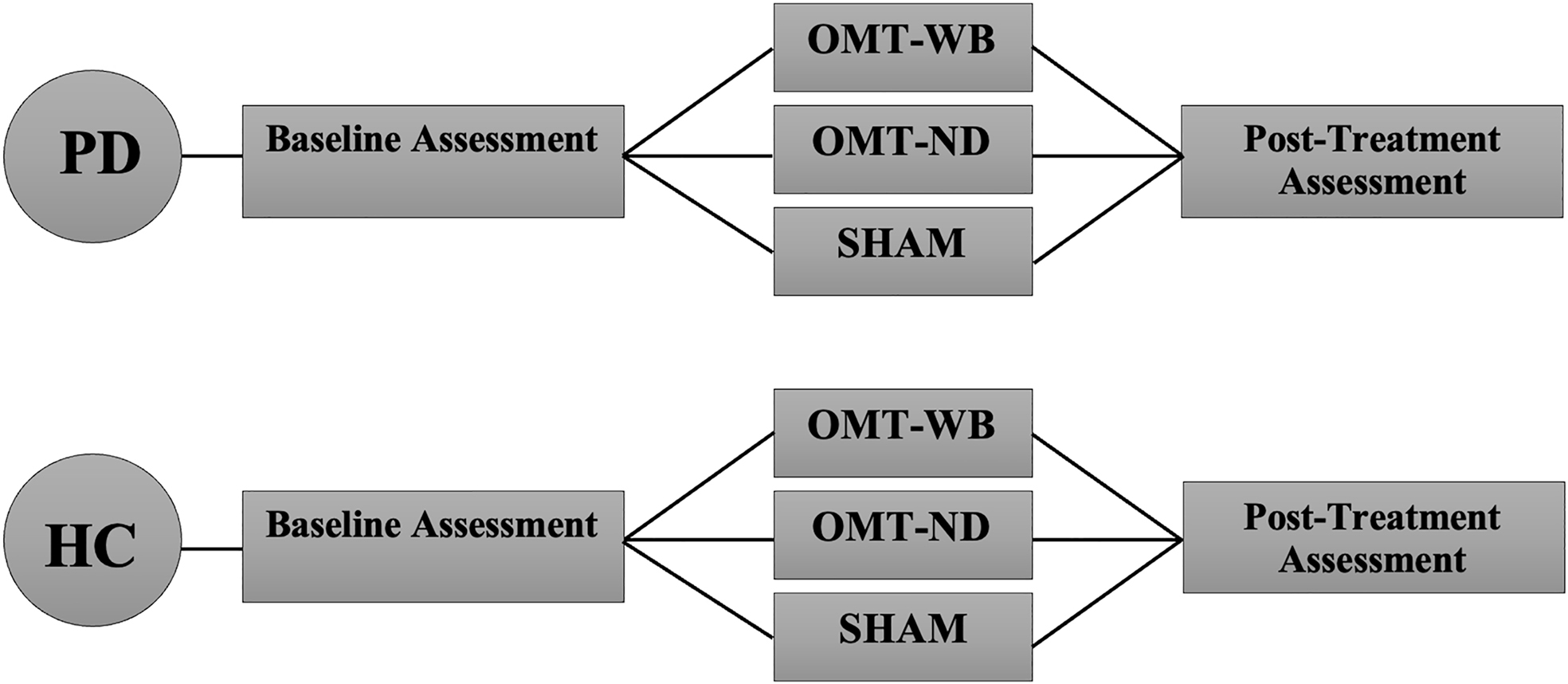
This study aimed to determine whether a single session of OMT or OMT + OCMM can improve the gait of individuals with PD by addressing joint restrictions in the sagittal plane and by increasing ROM in the lower limb. It was designed as a two-group, randomized controlled trial in which individuals with PD (n=45) and age-matched healthy control participants (n=45) were recruited from the community. PD participants were included if they were otherwise healthy, able to stand and walk independently, had not received OMT or physical therapy (PT) within 30 days of data collection, and had idiopathic PD in Hoehn and Yahr stages 1.0-3.0.
PD participants were randomly assigned to one of three experimental treatment protocols:
- a ‘whole-body’ OMT protocol (OMT-WB), which included OMT and OCMM techniques;
- a ‘neck-down’ OMT protocol (OMT-ND), including only OMT techniques;
- and a sham treatment protocol.
Control participants were age-matched to a PD participant and were provided the same OMT experimental protocol.
An 18-camera motion analysis system was utilized to capture 3-dimensional (3D) position data in a treadmill walking trial before and after the assigned treatment protocol. Pretreatment and posttreatment hip, knee, and ankle ROM were compared with paired t-tests, and joint angle waveforms during the gait cycle were analyzed with statistical parametric mapping (SPM), which is a type of waveform analysis.
Individuals with PD had significantly reduced hip and knee extension in the stance phase compared to controls (32.9-71.2% and 32.4-56.0% of the gait cycle, respectively). Individuals with PD experienced a significant increase in total sagittal hip ROM (p=0.038) following a single session of the standardized OMT-WB treatment protocol. However, waveform analysis found no significant differences in sagittal hip, knee, or ankle angles at individual points of the gait cycle following OMT-WB, OMT-ND, or sham treatment protocols.
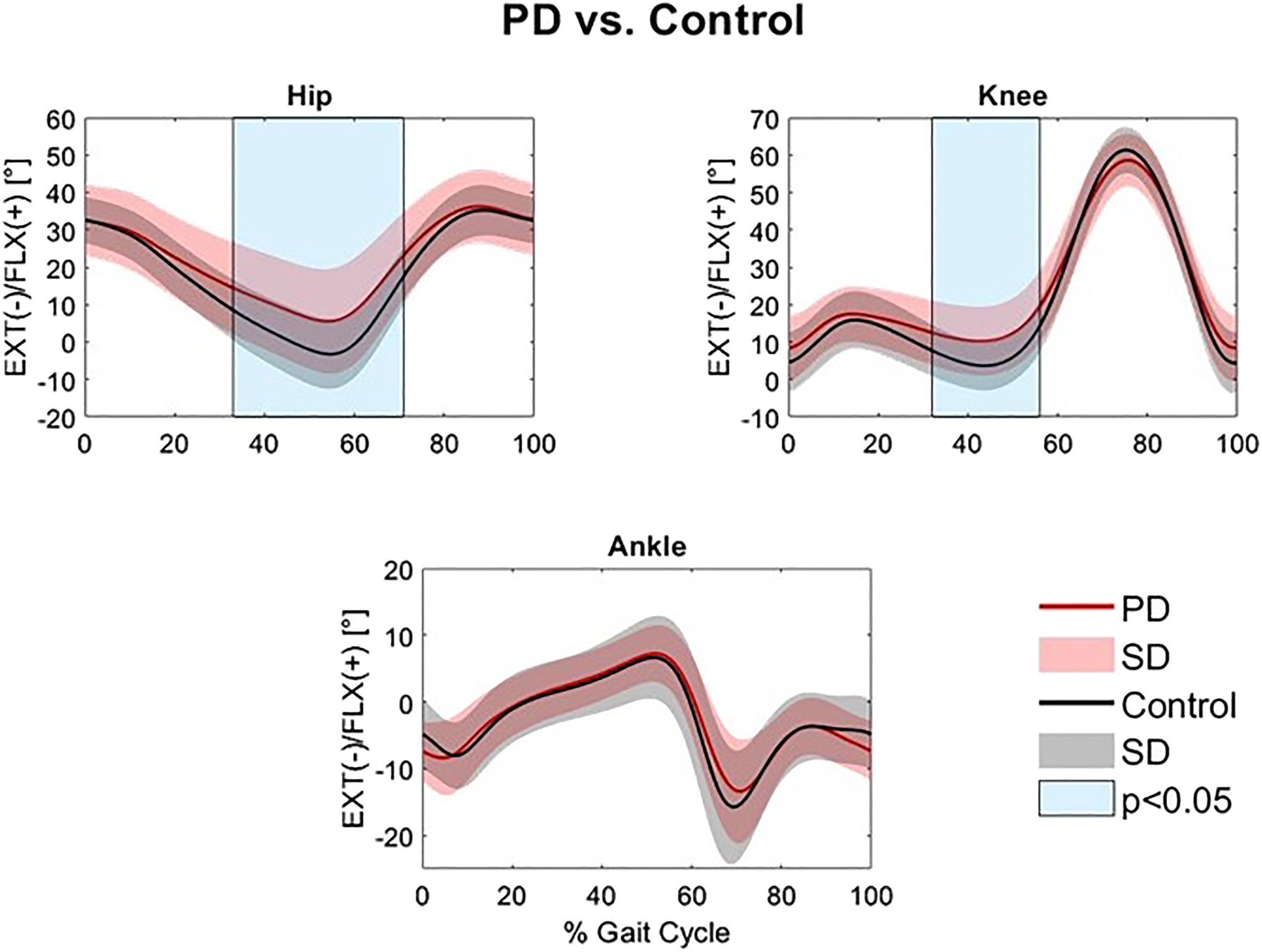
The authors concluded that the increase in hip ROM observed following a single session of OMT-WB suggests that OCMM in conjunction with OMT may be useful for improving gait kinematics in individuals with PD. Longitudinal studies over multiple visits are needed to determine the long-term effect of regular OMT and OMT+OCMM treatments on Parkinsonian gait characteristics.
The study has many significant limitations. For instance, the hypotheses tested lack plausibility and the outcome measures are of doubtful validity. Most importantly, the observed effects are only short term and their clinical relevance is highly questionable.
It has been reported that the US Insurer ‘State Farm’ is fighting a fraudulent scheme that has been exploiting New Jersey’s personal injury protection (PIP) benefits law since 2014. The insurer is seeking to recover $2.6 million in what it claims are fraudulent auto injury claims and a declaratory judgment that it need not pay any further claims submitted by the providers involved in the alleged scheme.
State Farm’s suit accuses 12 chiropractic and spine clinics and doctors of fraud, unjust enrichment, and violations of the New Jersey Insurance Fraud Prevention Act. The insurer alleges these providers used a “predetermined protocol” for all patients and a patient referral system for services that were either not performed or were not medically necessary for the individual patients. Instead, the services were carried out to enrich the defendants by exploiting the patients’ eligibility for PIP benefits, according to the complaint.
The suit accuses the providers of failing to legitimately evaluate patients to determine the true nature of their injuries and of reporting the same or similar findings for all patients to justify a predetermined course of treatment that was substantially the same for all patients. Part of the “predetermined protocol” for patients with soft-tissue injuries of the neck and back consisted of
- hot and cold packs,
- chiropractic manipulations,
- massage,
- mechanical traction,
- physical medicine and rehabilitation,
- and manual therapy.
These treatments were administered to almost every patient on almost every visit, regardless of each patient’s unique circumstances and needs, according to the complaint. The chiropractors are also accused of referring patients to diagnostic clinics, some allegedly illegally owned by the chiropractors, for an “unnecessary and predetermined course of pain management and invasive treatments” including injections. State Farm says they would submit false documentation for each case representing that the treatments were legitimately performed and medically necessary.
The 80-page complaint details case after case where the patient’s responses to questions and tests were the same or similar, allegedly serving as a “pretext to justify” the chiropractors’ wide range of treatments. The defendants in the complaint filed in U.S. District Court for New Jersey are:
- Tri-County Chiropractic and Rehabilitation Center,
- Robert Matturro, D.C.,
- Advanced Spine and Pain Management,
- Varinder Dhillon, M.D.,
- Nicholas Rosania, D.C.,
- Bloomfield UAI,
- Dov Rand, M.D.,
- Primary Medical Services,
- Louis J. Citarelli, M.D.,
- Chiro Health Center P.C.,
- Marc Matturro, D.C.
- Marco Tartaglia, M.D.
_____________________________
This story made me wonder: which of the listed treatments
- hot and cold packs,
- chiropractic manipulations,
- massage,
- mechanical traction,
- physical medicine and rehabilitation,
- and manual therapy
would ever be indicated for patients with soft-tissue injuries of the neck and back? Or more specifically, are chiropractic manipulations indicated or contra-indicated for such problems following a car accident? I fail to see any sound evidence that they are effective. If I am correct, should insurance companies not sue all chiropractors who routinely use manipulations for such cases? If the answer is YES, the sum of 2.6 million might need to be increased by several orders of magnitude.
I reported about the activities of Eurocam before (see here) and I was distinctly underwhelmed with this quackery lobby group. Now they have published a press release about a ‘worldwide declaration’ in favor of integrated medicine. Here is my translation of the press release (I will comment on the actual declaration at a later stage):
With a declaration, Eurocam and the European Federation of Homeopathic Patient’s Association, among others, call for an open scientific discourse, more research funds, and more promotion of young researchers in the field of integrative medicine. The declaration is supported by the German Central Association of Homeopathic Physicians and the Homeopathy Research Institute (HRI), among others. Integrative medicine combines conventional and complementary elements in health care for the benefit of patients. The goal is patient-centred and holistic health care. Already 130 organisations have committed themselves to these goals in the medical care of the population in the Declaration.
Integrative medicine integrates complementary and conventional methods
In addition, the Declaration advocates health care that takes the whole person into account in its psychological, mental, social and spiritual dimensions. Integrative medicine in the sense of the Declaration is patient-centred and supports the body’s own regulatory abilities. In addition, it is participatory and respects individual decisions with regard to medical care. It is committed to the evidence of medical procedures, which is based on experience, patient preferences and research findings. It incorporates cultural diversity and regional differences as well as the concepts of community health and planetary health. Integrative medicine uses natural and sustainable resources and integrates complementary and conventional medical procedures.
Integrative medicine: Opportunities especially for chronic diseases and side effects
The supporters of the Declaration see opportunities for integrative medicine above all in chronic and non-communicable diseases, as well as in the frequent side effects of conventional therapies and increasing antibiotic resistance. Conventional medicine is characterised by fragmentation and divisional thinking within medical care, as well as by the increasing specialisation of the health professions. The holistic view of the patient is thus left out. Against this backdrop, the Declaration advocates anchoring integrative medicine as a legal entitlement in health care and integrating it into national health care systems. International training standards should be adapted with integrative medicine in mind, and research projects should be promoted. At the same time, balanced and high-quality patient information is needed.
________________________________
This press release requires a few short comments, in my view:
- “Integrative medicine combines conventional and complementary elements in health care for the benefit of patients.” Anyone who cares to research for longer than 10 minutes will find that very often the complementary elements are unproven and disproven treatments.
- “The goal is patient-centred and holistic health care.” By integrating unproven and disproven treatments into routine care, medicine cannot become more patient-centred but must get less effective and more expensive.
- “The Declaration advocates health care that takes the whole person into account in its psychological, mental, social and spiritual dimensions.” Any good healthcare aims at doing this.
- “Individual decisions with regard to medical care” are respected in all forms of healthcare.
- “Side effects of conventional therapies and increasing antibiotic resistance” are regrettable phenomena and much research is going on to minimize them. So-called alternative medicine (SCAM) has not yet been shown to offer a single solution to these problems.
- “The holistic view of the patient is left out” in conventional medicine. One of the most popular fallacies with SCAM advocates is the strawman fallacy.
I find the text almost comical. It reveals thought processes that lack even the most fundamental rules of logic. One really does get the impression that it had been written by people who are deplorably naive, misinformed, and quite frankly stupid.