systematic review
Look what I found on Facebook:
Learn how to offer the healing energy of Reiki to yourself, people, and animals while enhancing your animal connection skills!
From daily support for health or challenges during times of crisis, Reiki helps restore balance on physical, emotional, spiritual, and mental levels for all living beings, enabling the body to do what it does best—heal itself. These benefits extend to other people, animals, trees/plants, and self-healing.
Reiki offers so many benefits for animals and for their human caregivers that I call it the gift that keeps on giving!
Reiki also enables students to connect and communicate more deeply with animals. If you think animals like you now, wait until they discover you’ve got Reiki—you’ll become an animal magnet!
For 25+ years Reiki has blessed me, my animal companions, students, and as a teacher I love sharing those benefits with as many people and animals as possible.
AVAILABLE WORLDWIDE
For many years I’ve taught a LIVE personally-mentored 6-week audio class where students learn all the basic skills needed by a beginning Reiki practitioner in addition to foundational principles of energy healing. And you don’t even need to leave the comfort of your home!
TAKEN REIKI BEFORE but don’t feel confident? Students who have retaken Reiki with me share that the weekly calls, opportunities to practice, online community, and opportunity to ask questions and receive guidance have helped them make Reiki a part of their daily lives and feel confident in offering it to loved ones.
REIKI LEVEL 1 CLASS SERIES
August 3 – September 7, 2022
LIVE WEEKLY CALLS and PERSONAL MENTORING
Every Wednesday at 6:00 p.m. Pacific for six weeks. Each call will be recorded and available for replay for students, including those in other time zones/countries. You do not have to attend live to take this class.
In addition to the 60-90 minute weekly calls, each student receives handouts and personal guidance for practice sessions.
When the class concludes, and all requirements have been fulfilled, each student receives a Reiki Level 1 certificate.
To learn more or register:

AND NOW FOR THE IMPORTANT BIT:
Choose one payment for all six classes. Payment is available with Visa, MC, or PayPal (choose PayPal credit card option for payment with Amex or Discover). PayPal also offers a payment plan option. Confirmation will be sent after registration along with instructions on how to join the first call. If you were unable to register in time to attend the first class live you can very easily catch up with the replay. Final deadline for registration is the day of the second class.
Single Pay Plan: $249.00
____________________________
This seems like a good little earner to me!
Congratulations to whoever invented it.
Yet I do feel that something has been forgotten:
the evidence.
If you search for Reiki on Pubmed, you find a baffling array of papers many of which arrive at positive conclusions. If you then check out the primary studies, you realize that most of them are of extremely poor quality, published by members of the Reiki cult (often in 3rd class journals for the nursing professions). If you search for independent systematic reviews that adequately account for the quality of the primary studies, you discover that, in fact, the evidence does not support the notion that Reiki is effective for anything. Here are a few examples:
- There is insufficient evidence to say whether or not Reiki is useful for people over 16 years of age with anxiety or depression or both.
- The serious methodological and reporting limitations of limited existing Reiki studies preclude a definitive conclusion on its effectiveness.
- In total, the trial data for any one condition are scarce and independent replications are not available for each condition. Most trials suffered from methodological flaws such as small sample size, inadequate study design and poor reporting.
And what about Reiki for animals?
As far as I can see, there is no good evidence at all.
So, does this render the above and similar courses fraudulent?
I let you answer this question for yourselves.
I recently looked at the list of best-sellers in homeopathy on Amazon. To my surprise, there were several books that were specifically focused on the homeopathic treatment of children. Since we had, several years ago, published a systematic review of this subject, these books interested me. Here is what Amazon tells us about them:
Homeopathic remedies are increasingly being used to treat common childhood ailments. They are safe, have no side effects or allergic reactions, are inexpensive and, above all, effective. In this guide, Dana Ullman explains what homeopathy is, how it works and how you can use it correctly to enhance your child’s health. He recommends remedies for more than 75 physical and emotional conditions, including: allergies, grief, anxiety, headaches, asthma, measles, bedwetting, nappy rash, bites and stings, shock, burns, sunburn, colic, teething, coughs and colds and travel sickness
Without doubt, this is the most comprehensive book on homeopathic pediatrics. Included is a complete guide to the correct use of homeopathy, recommended remedies for the treatment of more than seventy-five common physical, emotional, and behavioral conditions, and valuable information on the essential medicines that all parents should have in their home medicine kits
Tricia Allen, a qualified homeopath, offers a host of practical advice on how to treat illness using natural, homeopathic remedies. Homeopathy differs from conventional medicine in that it does not only alleviate the individual symptoms of an illness, but treats the underlying state to ensure that the disease does not return, something which rarely occurs when using traditional remedies. This guide gives you advice on; what homeopathy is and how to use it; each stage of childhood and how to deal with the complaints that occur at that time of a child’s development; the most common childhood illnesses, how to take your own steps to treating them, which homeopathic remedies to use and when to seek medical help and first aid.
The Homeopathic Treatment of Children is indispensible at giving both a clear overall impression of the various major constitutional types, and also a detailed outline for reference at the end of each chapter. Not only does Paul Herscu draw from various sources (repertories and materia medica), he also adds indispensable original information from his successful practice.
______________________________
The fact that such books exist is perhaps not all that surprising. Yet, I do find the fact that they are among the best-selling books on homeopathy surprising – or to be more precise, I find it concerning.
Why?
Simple: children cannot give informed consent to the treatments they receive. Thus, consent is given for them by their parents or (I suspect often) not at all. This renders homeopathic treatment of children more problematic than that of fully competent adults.
Homeopathy has not been shown to be effective for any pediatric condition. I know Dana Ullman disagrees and claims it works for children’s allergies, grief, anxiety, headaches, asthma, measles, bedwetting, nappy rash, bites and stings, shock, burns, sunburn, colic, teething, coughs and colds, and travel sickness. Yet, these claims are not based on anything faintly resembling sound evidence! Our above-mentioned systematic review reached the following conclusion: “The evidence from rigorous clinical trials of any type of therapeutic or preventive intervention testing homeopathy for childhood and adolescence ailments is not convincing enough for recommendations in any condition.”
And what follows from this state of affairs?
I am afraid it is this:
Treating sick children with homeopathy amounts to child abuse.
The US Food and Drug Administration created the Tainted Dietary Supplement Database in 2007 to identify dietary supplements adulterated with active pharmaceutical ingredients (APIs). This article compared API adulterations in dietary supplements from the 10-year time period of 2007 through 2016 to the most recent 5-year period of 2017 through 2021. Its findings are alarming:
- From 2007 through 2021, 1068 unique products were found to be adulterated with APIs.
- Sexual enhancement and weight-loss dietary supplements are the most common products adulterated with APIs.
- Phosphodiesterase-5 inhibitors are commonly included in sexual enhancement dietary supplements.
- A single product can include up to 5 APIs.
- Sibutramine, a drug removed from the market due to cardiovascular adverse events, is the most included adulterant API in weight loss products.
- Sibutramine analogues, phenolphthalein (which was removed from the US market because of cancer risk), and fluoxetine were also included.
- Muscle-building dietary supplements were commonly adulterated before 2016, but since 2017 no additional adulterated products have been identified.
The authors concluded that the lack of disclosure of APIs in dietary supplements, circumventing the normal procedure with clinician oversight of prescription drug use, and the use of APIs that are banned by the Food and Drug Administration or used in combinations that were never studied are important health risks for consumers.
The problem of adulterated supplements is by no means new. A similar review published 4 years ago already warned that “active pharmaceuticals continue to be identified in dietary supplements, especially those marketed for sexual enhancement or weight loss, even after FDA warnings. The drug ingredients in these dietary supplements have the potential to cause serious adverse health effects owing to accidental misuse, overuse, or interaction with other medications, underlying health conditions, or other pharmaceuticals within the supplement.”
These papers relate to the US where supplement use is highly prevalent. The harm done by adulterated products is thus huge. If we focus on Chinese or Ayurvedic supplements, the problem might even be more serious. In 2002, my own review concluded that adulteration of Chinese herbal medicines with synthetic drugs is a potentially serious problem which needs to be addressed by adequate regulatory measures. Twenty years later, we seem to be still waiting for effective regulations that protect the consumer.
Progress in medicine, they say, is made funeral by funeral!
Chiropractors often refer their patients for full-length (three- to four-region) radiographs of the spine as part of their clinical assessment, which are frequently completed by radiographers in medical imaging practices. Overuse of spinal radiography by chiropractors has previously been reported and remains a contentious issue.
The purpose of this scoping review was to explore the issues surrounding the utilization of full-length spinal radiography by chiropractors and examine the alignment of this practice with current evidence.
A search of four databases (AMED, EMBASE, MedLine and Scopus) and a hand search of Google was conducted. Articles were screened against an inclusion/exclusion criterion for relevance. Themes and findings were extracted from eligible articles, and evidence was synthesized using a narrative approach.
In total, 25 articles were identified, five major themes were extracted, and subsequent conclusions drawn by authors were charted to identify confluent findings:
- (1) The historical integration of FLS radiography in chiropractic,
- (2) Clinical indications for FLS radiography in chiropractic,
- (3) Risks associated with FLS radiography,
- (4) Chiropractic techniques which prescribe the use of FLS radiography,
- (5) Current trends in the utilisation of FLS radiography in chiropractic.
This review identified a paucity of literature addressing this issue and an underrepresentation of relevant perspectives from radiographers. Several issues surrounding the use of full-length spinal radiography by chiropractors were identified and examined, including barriers to the adherence to published guidelines for spinal imaging, an absence of a reporting mechanism for the utilization of spinal radiography in chiropractic and the existence of a spectrum of beliefs amongst chiropractors about the clinical utility and limitations of full-length spinal radiography.
The authors concluded that this review has identified a scarcity of literature addressing the completion of chiropractor‐referred FLS X‐rays. Our review has outlined several pressing issues that warrant further investigation including a lack of quantitative measures to assess the utilisation of FLS X‐rays by chiropractors, a lack of consensus of what constitutes appropriate clinical justification for imaging and the existence of a spectrum of beliefs amongst chiropractic authors about the clinical utility and limitations of FLS radiography. This provides radiographers with a definitive opportunity to demonstrate clinical leadership in this space and seek to begin a constructive dialogue with chiropractic referrers about the risks associated with unnecessary or unjustified spinal radiography. In doing this, diagnostic radiographers as evidence‐based health practitioners can actively contribute to the conversation surrounding the issues identified by this study and can be better positioned to advocate for the interests of the discipline and the safety of their patients.
The authors of this review make a number of further relevant points:
- Between 2014 and 2015, approximately 130,000 three‐ to four‐region spinal X‐rays were performed in Australia. Most were requested by chiropractors.
- In Australia, chiropractors often request FLS X‐ray examinations by radiographers.
- A spectrum of beliefs and knowledge exists amongst chiropractic practitioners surrounding the appropriate use of FLS radiography which may not always align with the principles of evidence‐based practice.
- The risks associated with the overutilization of diagnostic imaging are well documented. Aside from the inherent risks of unnecessary exposure to ionizing radiation, increased reliance on diagnostic imaging by any practitioner in the absence of sufficient clinical justification increases economic burdens encumbered upon the health care system. As such, FLS radiography should be used judiciously to ensure risks associated with its use are minimized, thus ensuring that it remains available to chiropractors and other practitioners where its use is clinically justified.
- Imaging that is not clinically indicated also carries a risk of overdiagnosis that being the radiological diagnosis of disease which does not ultimately impact on a patient’s course of treatment.
- The use of FLS radiography by chiropractors for the detection of red flags in the absence of any significant clinical indications for imaging could be considered a practice that carries a high risk of overdiagnosis.
When I first raised the issue of chiropractic overuse of imaging in 1998, I got fiercely attacked by a gang of chiros. Each time hence that I mention the subject, chiros loudly protest, and I do, of course, understand why. Imaging gives chiros the flair of being ‘cutting edge’; more importantly, in most countries, it is an easy source of additional income.
So, I do not expect that things will be different this time. Yet, I feel that, instead of constantly trying to shoot the messenger, chiropractors might be well advised to consider the message.
In 2007, we published a systematic review summarizing the efficacy of homeopathic remedies used as a sole or additional therapy in cancer care. We have searched the literature using the databases: Amed (from 1985); CINHAL (from 1982); EMBASE (from 1974); Medline (from 1951); and CAMbase (from 1998). Randomized and non-randomized controlled clinical trials including patients with cancer or past experience of cancer receiving single or combined homeopathic interventions were included. The methodological quality of the trials was assessed by Jadad score. Six studies met our inclusion criteria (five were randomized clinical trials and one was a non-randomized study); but the methodological quality was variable including some high-standard studies. Our analysis of published literature on homeopathy thus found insufficient evidence to support the clinical efficacy of homeopathic therapy in cancer care.
Meanwhile, more trials have emerged, not least a dubious study by Frass et al which is currently under investigation. This means that a new evaluation of the totality of the available evidence might be called for. I am pleased to report that such an assessment has just been published.
In this systematic review, the researchers included clinical studies from 1800 until 2020 to evaluate evidence of the effectiveness of homeopathy on physical and mental conditions in patients during oncological treatment.
In February 2021 a systematic search was conducted searching five electronic databases (Embase, Cochrane, PsychInfo, CINAHL, and Medline) to find studies concerning the use, effectiveness, and potential harm of homeopathy in cancer patients.
From all 1352 search results, 18 studies with 2016 patients were included in this SR. The patients treated with homeopathy were mainly diagnosed with breast cancer. The therapy concepts include single and combination homeopathic remedies (used systemically or as mouth rinses) of various dilutions. Outcomes assessed were the influence on toxicity of cancer treatment (mostly hot flashes and menopausal symptoms), time to drain-removal in breast cancer patients after mastectomy, survival, quality of life, global health and subjective well-being, anxiety, and depression as well as safety and tolerance.
The included studies reported heterogeneous results: some studies described significant differences in quality of life or toxicity of cancer treatment favoring homeopathy, whereas others did not find an effect or reported significant differences to the disadvantage of homeopathy or side effects caused by homeopathy. The majority of the studies have low methodological quality.
The authors concluded that, for homeopathy, there is neither a scientifically based hypothesis of its mode of action nor conclusive evidence from clinical studies in cancer care.
I predict that, if we wait another 15 years, we will have even more studies. I also predict that some of them will be less than reliable or even fake. Finally, I predict that the overall result will still be mixed and unconvincing.
Why can I be so sure?
- Because homeopathy lacks biological plausibility as a treatment of cancer (or any other condition).
- Because highly diluted homeopathic remedies are pure placebos.
- Because homeopathy has developed into a cult where one is no longer surprised to see studies emerging that are too good to be true.
A study by an international team of researchers estimated the proportion of healthcare interventions tested within Cochrane Reviews that are effective according to high-quality evidence.
They selected a random sample of 2428 (35%) of all Cochrane Reviews published between 1 January 2008 and 5 March 2021 and extracted data about interventions within these reviews that were compared with placebo, or no treatment, and whose outcome quality was rated using Grading of Recommendations Assessment, Development and Evaluation (GRADE). They then calculated the proportion of interventions whose effectiveness was based on high-quality evidence according to GRADE, had statistically significant positive effects and were judged as beneficial by the review authors. They also calculated the proportion of interventions that suggested harm.
Of 1567 eligible interventions, 87 (5.6%) had high-quality evidence on first-listed primary outcomes, positive, statistically significant results, and were rated by review authors as beneficial. Harms were measured for 577 (36.8%) interventions, 127 of which (8.1%) had statistically significant evidence of harm. Our dependence on the reliability of Cochrane author assessments (including their GRADE assessments) was a potential limitation of our study. 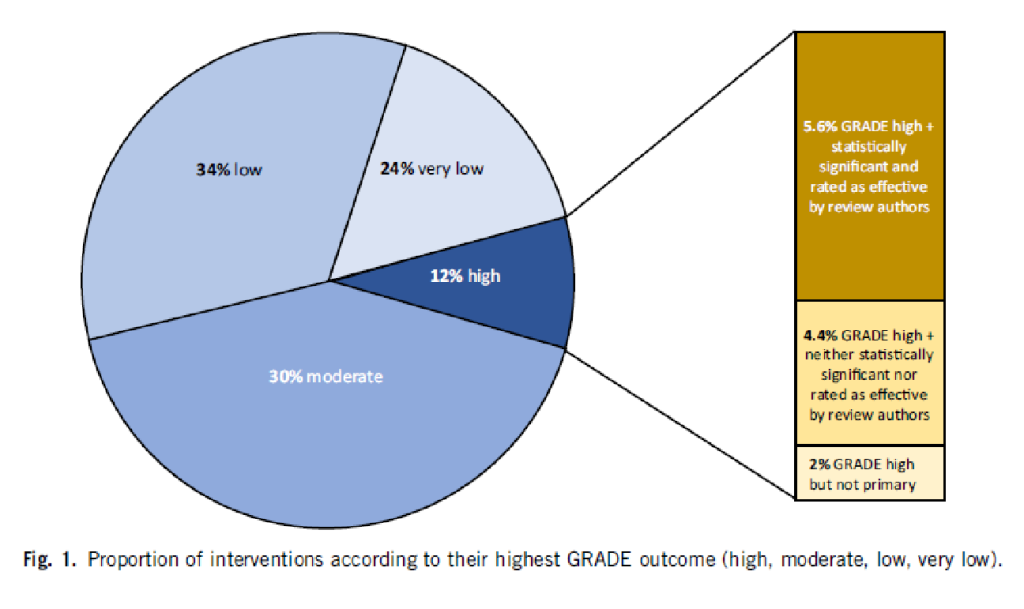
The authors drew the following conclusions: While many healthcare interventions may be beneficial, very few have high-quality evidence to support their effectiveness and safety. This problem can be remedied by high-quality studies in priority areas. These studies should measure harms more frequently and more rigorously. Practitioners and the public should be aware that many frequently used interventions are not supported by high-quality evidence.
Proponents of so-called alternative medicine (SCAM) are fond of the ‘strawman’ fallacy; meaning they like to present a picture of conventional medicine that is overtly negative in order for SCAM to appear more convincing (Prince Charles, for instance, uses this trick every single time he speaks about SCAM). Therefore I am amazed that this paper has not been exploited in that way by them. I was expecting headlines such as
Evidence-based medicine is not supported by evidence
or
Less than 6% of all conventional treatments are supported by sound evidence.
etc.
Why did they not have a field day with this new paper then?
As the article is behind a paywall, it took me a while to get the full paper (thanks Paul). Now that I have read it, I think I understand the reason.
In the article, the authors provide figures for specific types of treatments. Let me show you some of the percentages of interventions that met the primary outcome (high quality, statistically significant effect, and authors interpret as effective):
- pharmacological 73.8%
- surgical 4.6%
- exercise 5.8%
- diet 1.2%
- alternative 0.0%
- manual therapies 0.0%
So, maybe the headlines should not be any of the above but:
No good evidence to support SCAM?
or
SCAM is destroying the evidence base of medicine.
If you have been following my blog for a while, you probably know the answer to this question. A recent article published in JAMA re-emphasizes it in an exemplary fashion:
According to National Health and Nutrition Examination Survey data, 52% of surveyed US adults reported using at least 1 dietary supplement in the prior 30 days and 31% reported using a multivitamin-mineral supplement. The most commonly cited reason for using supplements is for overall health and wellness and to fill nutrient gaps in the diet. Cardiovascular disease and cancer are the 2 leading causes of death and combined account for approximately half of all deaths in the US annually. Inflammation and oxidative stress have been shown to have a role in both cardiovascular disease and cancer, and dietary supplements may have anti-inflammatory and antioxidative effects.
Objective To update its 2014 recommendation, the US Preventive Services Task Force (USPSTF) commissioned a review of the evidence on the efficacy of supplementation with single nutrients, functionally related nutrient pairs, or multivitamins for reducing the risk of cardiovascular disease, cancer, and mortality in the general adult population, as well as the harms of supplementation.
Population Community-dwelling, nonpregnant adults.
Evidence Assessment The USPSTF concludes with moderate certainty that the harms of beta carotene supplementation outweigh the benefits for the prevention of cardiovascular disease or cancer. The USPSTF also concludes with moderate certainty that there is no net benefit of supplementation with vitamin E for the prevention of cardiovascular disease or cancer. The USPSTF concludes that the evidence is insufficient to determine the balance of benefits and harms of supplementation with multivitamins for the prevention of cardiovascular disease or cancer. Evidence is lacking and the balance of benefits and harms cannot be determined. The USPSTF concludes that the evidence is insufficient to determine the balance of benefits and harms of supplementation with single or paired nutrients (other than beta carotene and vitamin E) for the prevention of cardiovascular disease or cancer. Evidence is lacking and the balance of benefits and harms cannot be determined.
Recommendation The USPSTF recommends against the use of beta carotene or vitamin E supplements for the prevention of cardiovascular disease or cancer. (D recommendation) The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the use of multivitamin supplements for the prevention of cardiovascular disease or cancer. (I statement) The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the use of single- or paired-nutrient supplements (other than beta carotene and vitamin E) for the prevention of cardiovascular disease or cancer. (I statement)
The report also elaborates on potential harms:
For many of the vitamins and nutrients reviewed, there was little evidence of serious harms. However, an important harm of increased lung cancer incidence was reported with the use of beta carotene by persons who smoke tobacco or have occupational exposure to asbestos.
Excessive doses of vitamin supplements can cause several known adverse effects; for example, moderate doses of vitamin A supplements may reduce bone mineral density, and high doses may be hepatotoxic or teratogenic. Vitamin D has potential harms, such as a risk of hypercalcemia and kidney stones, when given at high doses. The potential for harm from other supplements at high doses should be carefully considered.
There is nothing new here, of course. I (and others) have been trying to get these points across for many years. But it is nevertheless most gratifying to see the message repeated by a top journal such as JAMA. I hope JAMA is more successful than I was in changing the behavior of the often all too gullible public!
Nausea and vomiting are common symptoms of patients with advanced cancer. While there is some evidence for acupuncture point stimulation in the treatment of these symptoms for patients having anticancer treatment, there is little for when they are not related to such treatment.
This study aimed to determine whether acupressure at the pericardium 6 sites can help treat nausea and vomiting suffered by palliative care patients with advanced cancer. The researchers conducted a double-blind randomized controlled trial-active versus placebo acupressure wristbands. In-patients with advanced cancer in two specialist palliative care units who fitted either or both of the following criteria were approached: nausea that was at least of moderate severity; vomiting daily on average for the prior 3 days.
A total of 57 patients were randomized to have either active or placebo acupressure wristbands. There was no difference in any of the outcome measures between the two groups:
- change from the baseline number of vomits;
- Visual Analogue Scale for ‘did acupressure wristbands help you to feel better?’;
- the total number of doses of antiemetic medication;
- the need for escalation of antiemetics.
The authors concluded that, in contrast to a previously published feasibility study, active acupressure wristbands were no better than placebo for specialist palliative care in patients with advanced cancer and nausea and vomiting.
When the research into acupuncture for nausea and vomiting began some 20 years ago, the evidence turned out to be encouraging. Later, as the studies became more and more rigorous, many trials failed to confirm the initial findings. Today, the totality of the evidence is far less convincing than it seemed years ago.
This is a phenomenon that can be observed not just in acupuncture research but in many types of treatment:
- Initially, over-enthusiastic researchers become victims of their own optimism.
- These investigators are less into testing hypotheses than into confirming their own wishful thinking.
- Thus, several positive trials emerge.
- These, however, turn out to be methodologically flawed.
- Eventually, the subject might be picked up by real scientists who truly test hypotheses.
- More and more negative studies thus emerge.
- Depending on how many flawed studies were initially published and how critical the authors of systematic reviews are, it can take years until the totality of the evidence depicts the true picture which discloses the initial findings as false-positive.
The message is, I think, clear: poor quality studies have the potential to mislead us for many years. Eventually, however, the self-cleansing ability of science should generate the truth about the value of any treatment. In other words:
poor-quality science is not just useless, it causes long-term harm
and
critical thinking prevents harm
This systematic review evaluated individualized homeopathy as a treatment for children with attention deficit and hyperactivity disorder (ADHD) when compared to placebo or usual care alone.
Thirty-seven online sources were searched up to March 2021. Studies investigating the effects of individualized homeopathy against any control in ADHD were eligible. Data were extracted to a predefined excel sheet independently by two reviewers.
Six studies were analyzed:
- 5 were RCTs
- 2 were controlled against standard treatments;
- 4 were placebo-controlled and double-blinded.
The meta-analysis revealed a significant effect size across studies of Hedges’ g = 0.542 (95% CI 0.311-0.772; z = 4,61; p < 0.001) against any control and of g = 0.605 (95% CI 0.05-1.16; z = 2.16, p = 0.03) against placebo. The effect estimations are based on studies with an average sample size of 52 participants.
The authors concluded that individualized homeopathy showed a clinically relevant and statistically robust effect in the treatment of ADHD.
This is a counter-intuitive result (to put it mildly), and it is, therefore, wise to have a look at the 6 included studies:
1.Frei, H. et al. Homeopathic treatment of children with attention deficit hyperactivity disorder: a randomised, double blind, placebo controlled crossover trial. Eur. J. Pediatr. 164, 758–767 (2005).
This was a trial with just 62 patients who had previously responded to homeopathy. The study was conducted by known proponents of homeopathy and had a highly unusual design. The results suggested that homeopathy was better than placebo.
2. Oberai, P. et al. Homoeopathic management of attention deficit hyperactivity disorder: a randomised placebo-controlled pilot trial. Indian J. Res. Homoeopathy 7, 158–167 (2013).
This one was published in an obscure journal that I could not access.
3. Jacobs, J., Williams, A. L., Girard, C., Njike, V. Y. & Katz, D. Homeopathy for attention-deficit/hyperactivity disorder: a pilot randomized-controlled trial. J. Altern. Complement. Med. 11, 799–806 (2005)
This study showed that there were no statistically significant differences between homeopathic remedy and placebo groups on the primary or secondary outcome variables.
4. Jones, M. The efficacy of homoeopathic simillimum in the treatment of attention-deficit/hyperactivity disorder (AD/HD) in schoolgoing children aged 6-11 years (2009).
This was a small unpublished (and not peer-reviewed) thesis. Its results showed no statistically significant effect of treatment.
5. Lamont, J. Homoeopathic treatment of attention deficit hyperactivity disorder. Br. Homeopathic J. 86, 196–200 (1997)
This was a small (n=46) trial with an unusual design. Its results suggested that homeopathy was better than placebo.
6. von Ammon, K. et al. Homeopathic RCT embedded in a long-term observational study of children with ADHD—a successful model of whole systems CAM research. Eur. J. Integr. Med. 1, 27 (2008).
Even though the journal is Medline-listed, I was unable to find this paper. I did, however, find a paper by the same authors with the same title. It turned out to be a duplication of the paper by Frei et al listed above.
_________________________
All in all, this brief analysis of the available abstracts (most full papers are behind paywalls) leaves many questions as to the trustworthiness of this systematic review unanswered. The fact that H. Walach (and other apologists of homeopathy) is its senior author does not inspire me with overwhelming confidence. In any case, I very much doubt that the authors’ conclusion is correct. I therefore would encourage someone with access to all full papers to initiate a more thorough analysis; the abstracts obviously leave many questions unanswered. For instance, it would be crucial to know how many of the trials followed an A+B versus B design (I suspect most studies did, and this would completely invalidate the review’s conclusion). I am more than happy to co-operate with such an evaluation.
Guest post by Derk P. Kooi
Political lobbying is not only restricted to major companies, even quackery lobbies extensively in Dutch politics as well as at a European and global level. The EUROpean Complementary and Alternative Medicine Stakeholder Group (EUROCAM) has been active in Europe for some time. EUROCAM recently attracted attention with a statement on antibiotic resistance during the European Antibiotics Awareness Day.[1] EUROCAM claims that Complementary and Alternative Medicine (CAM) could enhance the immune system and could therefore contribute to the fight against antibiotic resistance. An early study conducted by the anthroposophist Erik Baars was referenced, inter alia. However, this medical claim turns out to be pure nonsense.
EUROCAM regularly publishes so-called ‘position papers’ on the contribution CAM could provide to the European health care system. EUROCAM is currently cautious with its medical claims, and rightly so, as it has seriously overstepped the mark in the past. For example, claims about the efficacy of CAM for infections referred to research by Erik Baars, doctor, anthroposophical healthcare lector at the University of Applied Sciences Leiden and researcher at the Louis Bolk Institute. Baars is an associate of the society due to his misleading statements in his publications on the usefulness of CAM, more specifically of the anthroposophical variant.
Where does this fairly unknown club actually come from, what does it do and how seriously should we take it? Well, EUROCAM is an umbrella organisation for various alternative therapists and their patients. We are talking about Ayurveda, homeopathy, osteopathy, anthroposophy, herbal medicine, traditional (Chinese) medicine, Reiki and acupuncture. The Dutch Registry of Complementary Care Professionals (RBCZ) is also affiliated with EUROCAM. Classical homeopath Annemieke Boelsma is the contact person of the RBCZ at EUROCAM.
It is unclear precisely when EUROCAM was created, the LinkedIn page says 2009. The figurehead of the club is “secretary general” Ton Nicolaï. This homeopathic doctor is also well known to Vereniging tegen de Kwakzalverij, (www.kwakzalverij.nl) the Dutch Society against Quackery. The treasurer of EUROCAM is business administrator Wim Menkveld. Menkveld is on the Advisory Board of the Hortus Botanicus of Leiden. He is also active on the board of the European Patients’ Federation of Homeopathy. EUROCAM thus seems to have originated mainly from Dutch homeopathic circles.
Furthermore, TV producer Miranda Eilert-Ruchtie from Hilversum sits on the EUROCAM board. According to the EUROCAM website, she acts as their “operations manager” and communications advisor. The German Heilprakterin Sonja Maric, an anthropologist and “specialist in Tibetan medicine”, also acts as a communications consultant.
The European Transparency Register shows that in 2020 the total budget of the organisation was 40,498 euros; no more recent data is available. In the year 2018, 5,000 euros were reserved as an honorarium for Mr Nicolaï, for the 0.5 FTE that he works for the organisation. Miranda Eilert-Ruchtie works a number of hours a week for EUROCAM, as a freelancer. Sonja Maric does this on a voluntary basis.
EUROCAM is a member of the European Public Health Alliance (EPHA), the European Union Health Policy Platform. The World Health Organisation (WHO) recognises the organisation as a non-state actor, which means that both the EU and the WHO consider EUROCAM to be a serious legal entity. In the past, EUROCAM has intervened in public EU consultations in the fields of aging, pharmaceutical strategy, cancer, and digital data and services.
EUROCAM provides the secretariat of the MEP Interest Group on Integrative Medicine and Health, a group of five European parliamentarians who have set themselves the goal of promoting integrative medicine at the European level. Co-chairs are Finish Sirpa Pietikäinen, a European parliamentarian for the Christian Democrats, and French Michèle Rivasi, a European parliamentarian for the Greens. The other members are Luxembourg’s Tilly Metz, the Italian Eleonara Evi, and the Danish Margrete Auken. It is noteworthy that they are European parliamentarians for the Greens. They are all members of the European Parliament’s Committee on the Environment, Public Health and Food Safety (ENVI). Eleonara Evi was part of the illustrious Five Star Movement until 2020, known for its anti-vaccination stance. The Member of European Parliament (MEP) Interest Group organises annual events with speakers who are the same people who perform at EUROCAM symposia. These include the aforementioned anthroposophist Erik Baars. Baars worked closely with EUROCAM boss Ton Nicolaï in a European research project on CAM alternatives to antibiotics. More about his bad science later.
The texts EUROCAM produces nowadays (on its website) are carefully written, and the medical claims are carefully formulated. The texts are larded with synonyms for “possible”, known in linguistics as hedging. For example “Several CAM methods have shown high potential to reduce cancer pain”.[2] Generic health claims are also often used to suggest medical benefits, for example in the context of COVID-19, ‘In building and maintaining resistance to infectious illness, CAM modalities as a part of Integrative Medicine & Health can play an important role because they mobilise and stimulate people’s self-regulating capacity, thus increasing their resilience, their immune system.’.[3]
Furthermore, claims are put in the mouths of others, which can be read, for example, in quoting patient expectations: ‘While improving quality of life is the major rationale for CAM use, there is a definite undercurrent of expectation, particularly among the younger patients, that some therapies might have an anticancer effect (prolongation of remission periods) and slow/stagnate tumour growth (prolongation of survival periods), boost the immune system, making it easier to overcome the disease.’.[4]
The educated reader will immediately see through these strategies, but the question is whether the lobbied politicians targeted by EUROCAM understand these subtleties. EUROCAM has not always been so cautious, by the way. In an undated (presumably 2013) interview with the Dutch Association for Classical Homeopathy, “secretary general” Ton Nicolaï made a number of remarkable statements. For example, he claimed at the time that research shows “that for a number of herbal medicines there is a reasonable amount of evidence that scientifically confirms their effectiveness in respiratory infection treatments”. [5] Nicolaï bases his assertion on recent research by Erik Baars conducted as part of a European research programme that aimed to find CAM alternatives to antibiotics.
The report of this project, which ended in 2018, can be found on the EUROCAM website.[6] The authors of this report are, not surprisingly, Erik Baars and Ton Nicolaï. The report contains practically no hard science. Sub-studies focus on, for example, the frequency of antibiotic prescribing among alternative-working GPs and on the best practice of CAM believers. A so-called systematic review of systematic reviews offers good starting points to evaluate Mr Nicolaï’s claim: ‘A systematic review of systematic reviews demonstrates that there are specific, evidence-supported, promising CAM treatments for acute, uncomplicated RTIs [uncomplicated respiratory tract infections, ed.] and that they are safe.’
Here, a medical claim is made, which is weakened by the use of the hedge term “promising”. The conclusion can be summarised with “There would be ‘promising’ CAM treatments for respiratory infections, and they would be safe”. However, surprisingly, the project report does not refer to this “systematic review of systematic reviews”, nor to any of the other concrete results of the project!
Due to the lack of references, we cannot but conclude that the claim is based on a 2019 article by Erik Baars. One of the co-authors is Ton Nicolaï.[7] The article was published in the journal Evidence Based Complementary and Alternative Medicine (EBCAM), which has a shady reputation. Even one of the founders of EBCAM states that the peer-review system is a farce, and therefore the majority of the articles published in it are useless nonsense.[8] In this article, besides a large amount of vagueness about the “worldview differences” between CAM and medicine, systematic reviews are discussed about the effectiveness and safety of CAM treatments. From this systematic review of systematic reviews, it is concluded that there are promising CAM treatments for respiratory, urinary tract and skin infections and that there is even evidence that some CAM treatments are effective for respiratory infections, but what is this based on?
The reviews that were looked at were split into Cochrane and non-Cochrane reviews. Among the Cochrane reviews, there is one that would demonstrate the efficacy of CAM. It is a review on the use of immunostimulants for the prevention of respiratory tract infections in children.[9] Of the 35 studies that were analysed, six involve small molecules, such as isoprinosine, levamisole and pidotimod. In other words, regular medicine, if it turns out to work, but describing it as being experimental would be more appropriate. Baars’ article states that the review also contains herbal medicine. This is somewhat exaggerated: only one of the 35 studies deals with herbs. Of the remaining 28 studies, 25 cover bacterial extracts and three thymus extracts. Again: Baars does not make clear what this has to do with the CAM that EUROCAM represents.
In summary, EUROCAM is a small European lobbying organisation with perhaps some influence at both European and WHO level. One keeps coming across the same names. The organisation is currently using woolly, disguising language to mask medical claims and to fend off criticism. In the past, this was different when EUROCAM, by means of Ton Nicolaï among others, made very reprehensible statements about the role of CAM in (respiratory tract) infections. For the time being, this little club does not seem to pose much of a threat, but European politicians should, of course, ignore this hobby club.
References
1. ‘Improving patient resilience to reduce the need to rely on anti-infection treatment: the role of Integrative Medicine’. EUROCAM. https://cam-europe.eu/statement-on-amr-2021/ (visited on 28 December 2021) 2. EUROCAM. https://cam-europe.eu/contribution-of-cam-for-a-better-health/cam-in-the-context-of-cancer/ (visited on 3 October 2021) 3. EUROCAM. https://cam-europe.eu/contribution-of-cam-for-a-better-health/cam-in-the-context-of-cancer/ (visited on 3 October 2021) 4. EUROCAM. https://cam-europe.eu/contribution-of-cam-for-a-better-health/cam-in-the-context-of-cancer/ (visited on 3 October 2021)
5. Miranda Ruchtie. In gesprek met Ton Nicolaï, CAM integreren in de Europese gezondheidszorg. [In discussion with Ton Nicolaï, integrating CAM into the European health care system]. Nederlandse Vereniging van Klassiek Homeopaten. [Dutch Association of Classical Homeopaths] https://www.nvkh.nl/nieuwsbrieven-nvkh/interview-met-ton-nicolai (visited on 3 October 2021)
6. Erik Baars, et al. Reducing the need for antibiotics, the contribution of Complementary and Alternative Medicine. EUROCAM, 2018. https://cam-europe.eu/wp-content/uploads/2019/01/CAM-AMR-EUROCAM-Post-Conference-Paper-2018.pdf (visited on 3 October 2021)
7. Erik W. Baars et al. The Contribution of Complementary and Alternative Medicine to Reduce Antibiotic Use: A Narrative Review of Health Concepts, Prevention, and Treatment Strategies. Evid. Based Complement. Alternat. Med., 2019:5365608. DOI: 10.1155/2019/5365608
8. Edzard Ernst. “EBCAM: an alt med journal that puzzles me a great deal”, URL: http://edzardernst.com/2016/05/ebcam-an-alt-med-journal-that-puzzles-me-a-great-deal/ (visited on 8 January 2022)
9. B. E. Del-Rio-Navarro, F. J. Espinosa-Rosales, V. Flenady, and J. J. Sienra-Monge, “Cochrane Review: Immunostimulants for preventing respiratory tract infection in children,” Evidence-Based Child Health: A Cochrane Review Journal, 2012, 7 (2), 629–717.