pseudo-science
After all these years, I am still fascinated by what proponents of homeopathy try to tell others about their trade. Recently I found a long article in this vein. It is aimed at an audience of HEILPRAKTIKER and their patients. It should therefore be responsible, thorough, and evidence-based (yes, I am an optimist).
“With this article”, the authors state, “we aim to provide a comprehensive overview of homeopathy and help people make informed decisions about their health. Whether you already have experience with homeopathy or simply want to inform yourself, we hope that this article will provide you with valuable insights and information” (my translation).
Here I present to you just the relatively short section dedicated to the ‘pros and cons’ of homeopathy. Here we go:
Advantages of homeopathy:
- Holistic approach: homeopathy considers the human being as a whole and takes into account both physical and emotional aspects. It aims to support individual balance and the body’s self-healing powers.
- Gentle and non-invasive treatment: Homeopathic remedies are usually taken as globules, drops, or tablets and are therefore easy and convenient to use. They rarely cause side effects and are generally well tolerated.
- Individualized treatment: In homeopathy, each patient is considered unique and treatment is based on individual symptoms and characteristics. There is no “one-size-fits-all” solution, but a personalized approach.
- Support for chronic diseases: Homeopathy can be an alternative or complementary treatment for chronic conditions where conventional medicines offer limited relief. It can help improve quality of life and promote overall well-being.
Limitations of homeopathy:
- Placebo effect: Much of the effect of homeopathy is attributed to the placebo effect. It is argued that the improvements patients experience occur because of belief in the efficacy of the remedies and positive expectations, rather than due to a specific effect of the diluted substances.
- Lack of scientific evidence: The scientific evidence for the efficacy of homeopathy is limited and controversial. Many studies have failed to demonstrate benefits beyond the placebo effect. There is a lack of well-conducted randomized controlled trials that clearly show the effectiveness of homeopathy.
- Delay or rejection of conventional treatments: In some cases, the choice of homeopathy as the sole method of treatment may lead to delays in the diagnosis and timely treatment of serious or acute illnesses. It is important that serious illnesses are examined by a doctor and treated appropriately.
- Difficulties in standardization: Homeopathy involves a variety of remedies used in different potencies and dilutions. This makes standardization and the conduct of reproducible studies difficult. There are also controversial debates about whether the dilutions go beyond the extent to which molecules of the original substance are still present.
__________________________
I am sure that you have heard the BS about the alleged advantages of homeopathy often enough. Therefore, I will here not bother to comment on them again. More interesting, in my view, are the limitations of homeopathy, as seen by its proponents. Please allow me, therefore, to discuss them briefly.
- The authors state that “it is argued that the improvements patients experience occur because of belief in the efficacy of the remedies and positive expectations”. This sounds as though this is a mere aberrant opinion or at least an ongoing debate amongst scientists. In fact, it is the scientific consensus supported by tons of evidence.
- This is the same point expressed differently.
- The admission that “the choice of homeopathy as the sole method of treatment may lead to delays in the diagnosis and timely treatment” is yet another way of stating that homeopathy is not effective. What is, however, not expressed clearly enough, in my view, is the fact that homeopathic treatment usually amounts to medical neglect which is unethical and can cause serious harm, in extreme cases even death.
- It is not true that the range of potencies renders “the conduct of reproducible studies difficult”. There are plenty of examples to demonstrate this, for instance, this study. “There are also controversial debates about whether the dilutions go beyond the extent to which molecules of the original substance are still present.” Yes, I did translate this correctly. I am sorry to say that this sentence does make no sense in German or in English.
What I find particularly interesting is that the authors do not mention disadvantages that non-homeopaths would rate as quite important, e.g.:
- The assumptions of homeopathy fly in the face of science.
- Hahnemann strictly forbade homeopathy to be combined with ‘allopathy’ (yet proponents now claim this option to be an advantage).
- Treating a patient with homeopathy violates even the most basic rules of medical ethics.
- Homeopaths have no choice but to lie to their patients on a daily basis.
- Many homeopaths have the nasty habit of advising their patients against using effective treatments, e.g. vaccinations.
- Homeopathy undermines rational thinking in a general way.
In summary, the authors’ “aim to provide a comprehensive overview of homeopathy and help people make informed decisions about their health” has not been reached.
It has recently been reported that a 39-year-old woman (a mother-of-three died) died after immersing herself in a river as part of a cold water therapy session. The woman died after paramedics were called to attend a riverside in Derbyshire. The session was run by Kevin O’Neill of ‘Breatheolution’, whose previous clients include Coleen Rooney and actor Stephen Graham. The woman, who was visiting with two friends after paying up to £200 for a two-hour cold water therapy session, was rushed to hospital where she died.

Mr. O’Neill commented: “I am heartbroken. I’ve not slept and I’m finding it hard to process. I cannot stop thinking about her family. It’s tragic.” An inquest is expected to be opened into the woman’s death. East Midlands Ambulance Service said they were called to Bankside, in Bridgemont. “The caller reported a medical emergency,” a spokesperson said. “We sent a paramedic in a fast response car and a double-crewed ambulance. The air ambulance was also in attendance.”
Derbyshire Fire and Rescue Service, which was called to assist the paramedics, has warned people about the dangers of entering open water. “While we cannot and will not comment or speculate on the circumstances and cause of this tragic death, we would like to remind people of the dangers of entering open water and cold water shock,” said group manager Lee Williams.
_____________________
Breatheolution’ has a website where a whole page is dedicated to its leader Kevin O’Neill. I wondered what qualifications Kevin has, but all it tells us about him is this: “I struggled for so long with alcohol and other substance abuse that something had to give, I lost my sister Yvonne in 2019 and I think it was enough trauma to make me think a lot more about my own life”
The website also explains what the cold water sessions are about:
1-2-1 Breath Coaching, practice & Cold water session (river or tank)
2 hours @ £110.00
These sessions are proving popular with those who are not keen on group sessions or just prefer to have a more personal experience. The 2-3 hour sessions will be tailored to you and your breathing and will include potentially life-changing tools and methods to allow you to witness your breathing and physiology differently in the future, its all about feeling and awareness.
Another section of the site is dedicated to celebrities who Kevin seems to have treated. And then there is a video of the treatment. What I did not find anywhere, however, are the conditions that Kevin claims to treat with his cold water therapy.
In any case, it would have been wise for Kevin to read up about the risks of cold water immersion (CWI) before going into business. Perhaps this review would have helped:
In 2012, an estimated 372,000 people (42 per hour) died from immersion, assumed to be drowning. Immersion is the third leading cause of unintentional injury-related death, accounting for 7% of all such deaths (World Health Organization, 2014). These figures are underestimations owing to poor reporting in many Third World countries that have a high number of deaths. The data also do not include life-long morbidity caused by immersion-related injuries, estimated to be a much bigger numerical problem.
There is no strict definition of ‘cold water’. Given that some of the hazardous responses to cold water appear to peak on immersion somewhere between 15 and 10°C, it is reasonable to say that cold water is water <15°C (Tipton et al. 1991). However, the thermoneutral water temperature for a resting naked individual is ∼35°C, so it is possible for individuals to become very cold, with time, on immersion in water below this temperature. The corresponding temperature for those exercising (including shivering) is ∼25°C (Tipton & Golden, 1998).
Historically, the threat associated with CWI was regarded in terms of hypothermia or a reduction in deep body temperature below 35°C. This belief was established as a result of the Titanic disaster and supported by data obtained during maritime conflicts of World War II. However, more recently, a significant body of statistical, anecdotal and experimental evidence has pointed towards other causes of death on immersion. For example, in 1977 a Home Office Report revealed that ∼55% of the annual open water deaths in the UK occurred within 3 m of a safe refuge (42% within 2 m), and two-thirds of those who died were regarded as ‘good swimmers’. This evidence suggests more rapid incapacitation than can occur with whole-body cooling and consequent hypothermia.
The following four stages of immersion have been associated with particular risks (Golden & Hervey, 1981; Golden et al. 1991); the duration of these stages and the magnitude of the responses evoked within them vary significantly, depending on several factors, not least of which is water temperature:
- Initial immersion (first 3 min), skin cooling;
- Short-term immersion (3 min plus), superficial neuromuscular cooling;
- Long-term immersion (30 min plus), deep tissue cooling (hypothermia); and
- Circum-rescue collapse: immediately before, during or soon after rescue.
As a result of laboratory-based research, the initial responses to immersion, or ‘cold shock’, were identified as particularly hazardous (Tipton, 1989), accounting for the majority of immersion deaths (Tipton et al. 2014). These deaths have most often been ascribed to drowning, with the physiological responses of a gasp and uncontrollable hyperventilation, initiated by the dynamic response of the cutaneous cold receptors, resulting in the aspiration of the small volume of water necessary to initiate the drowning process (Bierens et al. 2016). Relatively little is known about the minimal rates of change of cold receptor temperature necessary to cause cold shock. The response has been reported to begin in water as warm as 25°C but is easy to suppress consciously at that temperature. In laboratory conditions, the respiratory frequency response (an indication of respiratory drive) peaks on naked immersion in a water temperature between 15 and 10°C, and is no greater on immersion in water at 5°C (Tipton et al. 1991). The corresponding average rates of change of chest skin temperature over the first 20 s of these immersions was 0.42 (water temperature 15°C), 0.56 (water temperature 10°C) and 0.68°C s−1 (water temperature 5°C). This suggests that an average rate of change in chest skin temperature between 0.42 and 0.56°C s−1 on the first 20 s of immersion is sufficient to evoke a maximal respiratory cold shock response.
More recently, it has been suggested (Shattock & Tipton, 2012) that a larger number of deaths than once thought may be attributable to arrhythmias initiated on immersion by the coincidental activation of the sympathetic and parasympathetic division of the autonomic nervous system by stimulation of cutaneous cold receptors around the body [sympathetic activation (cold shock)] and in the oronasal region on submersion or with wave splash [vagal stimulation (diving response)]. This ‘autonomic conflict’ is a very effective way of producing dysrhythmias and arrhythmias even in otherwise young and healthy individuals, particularly, but not necessarily, if a prolonged breath hold is involved in the immersion (Tipton et al. 1994). It seems that predisposing factors, such as long QT syndrome, ischaemic heart disease or myocardial hypertrophy, are necessary for fatal arrhythmias to evolve (Shattock & Tipton, 2012); many of these factors, including drug-induced long QT syndrome, are acquired. Non-fatal arrhythmias could still indirectly lead to death if they cause incapacitation and thereby drowning (Tipton, 2013). The hazardous responses associated with the cold shock response are presented in Fig. 2.
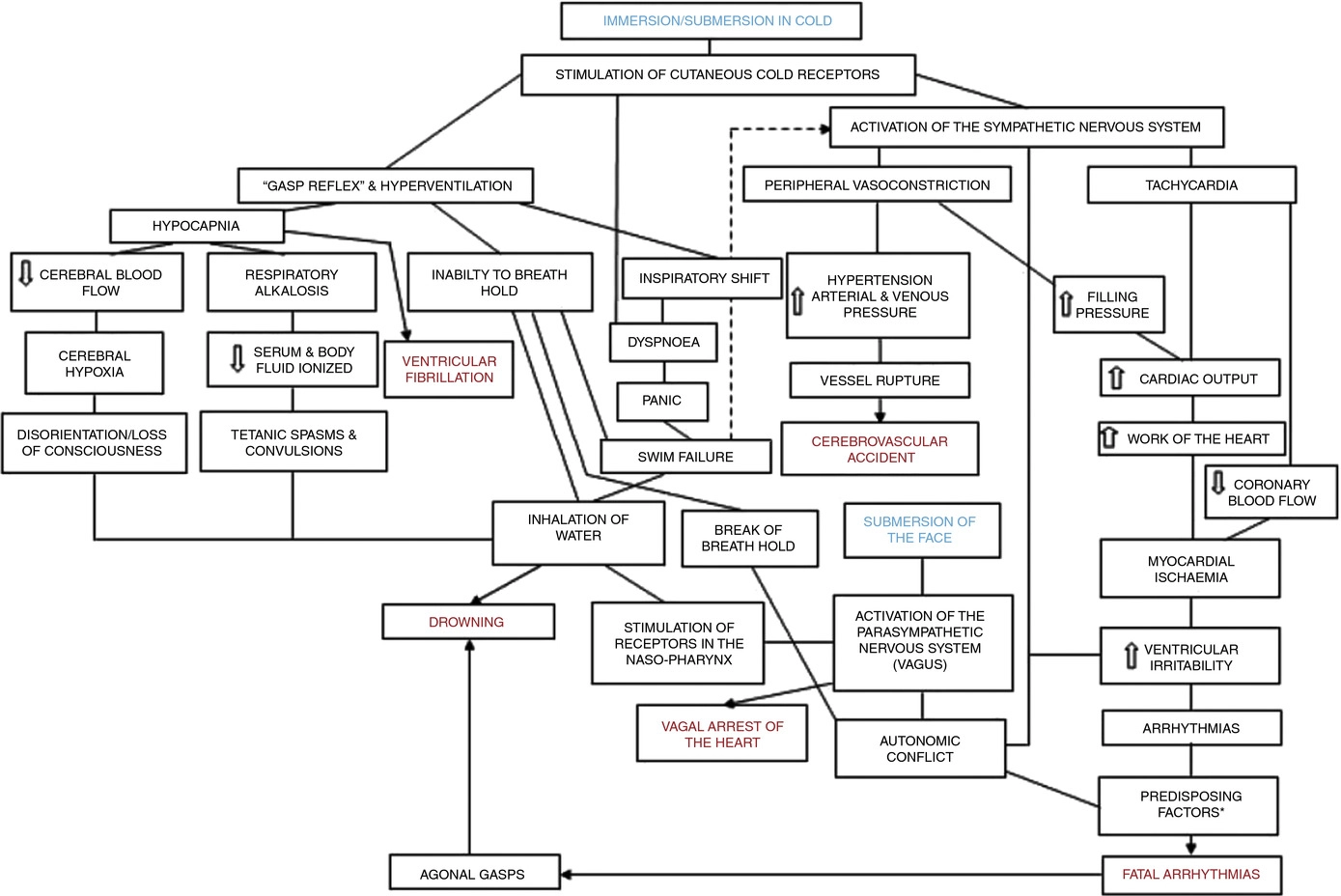
Figure 2. A contemporary view of the initial responses to immersion and submersion in cold water (‘cold shock’)
The problems encountered in short-term immersions are primarily related to physical incapacitation caused by neuromuscular cooling (Castellani & Tipton, 2015). The arms are particularly susceptible because of their high surface area to mass ratio. Low muscle temperatures affect chemical and physical processes at the cellular level. This includes metabolic rate, enzymatic activity, calcium and acetylcholine release and diffusion rate, as well as the series elastic components of connective tissues (Vincent & Tipton, 1988). Maximal dynamic strength, power output, jumping and sprinting performance are related to muscle temperature, with reductions ranging from 4 to 6% per degree Celsius reduction in muscle temperature down to 30°C (Bergh & Ekblom, 1979). At nerve temperatures below ∼20°C, nerve conduction is slowed and action potential amplitude is decreased (Douglas & Malcolm, 1955). Nerve block may occur after exposure to a local temperature of between 5 and 15°C for 1–15 min. This can lead to dysfunction that is equivalent to peripheral paralysis and can, again, result in drowning owing to the inability to keep the airway clear of the water (Clarke et al. 1958; Basbaum, 1973; Golden & Tipton, 2002; Fig. 3).

Figure 3. The ‘physiological pathways to drowning’ after immersion or submersion in cold water, with possible interventions for partial mitigation (dashed)
Abbreviations: EBA, emergency breathing aid; IS, immersion suit; and LJ, lifejacket. Reproduced with permission, from Tipton (2016b).
Even in ice-cold water, the possibility of hypothermia does not arise for at least 30 min in adults. Hypothermia affects cellular metabolism, blood flow and neural function. In severe hypothermia, the patient will be deeply unconscious. The progressive signs and symptoms (approximate deep body temperature) are shivering (36°C), confusion, disorientation, introversion (35°C), amnesia (34°C), cardiac arrhythmias (33°C), clouding of consciousness (33–30°C), loss of consciousness (30°C), ventricular fibrillation (28°C) and death (25°C) (Bierens et al. 2016). There is great variability between deep body temperature and the signs and symptoms of hypothermia. For example, although the deep body temperature associated with death is often quoted as 25°C, the lowest temperature recorded to date after accidental exposure to cold (air) and with full recovery was 12.7°C in a 28-month-old child (Associated Press, 2014). The coldest adult survivor of CWI followed by submersion had a body temperature of 13.7°C (Gilbert et al. 2000). There is also a large amount of variation in the rate at which people cool on immersion in cold water, owing to a combination of thermal factors (including water temperature and water movement, internal and external insulation) and non-thermal factors (including body size and composition, blood glucose, motion illness, racial and sex differences; Haight & Keatinge, 1973; Gale et al. 1981; White et al. 1992; Mekjavic et al. 2001; Golden & Tipton, 2002).
The most significant practical consequence of hypothermia in water is loss of consciousness; this prevents individuals from undertaking physical activity to maintain a clear airway and avoid drowning. Thus, once again, drowning is often the end-point (Fig. 3).
About 17% of those who die as a result of immersion die immediately before, during or after rescue (Golden et al. 1991). The deaths immediately before rescue are intriguing and probably related to behavioural changes at this time or the relief and psychophysiological alterations associated with imminent rescue, including a reduction in circulating stress hormone concentration and an increase in vagal tone. Death during rescue is most commonly associated with a collapse in arterial pressure when lifted vertical from the water and kept in that position for some time (Golden et al. 1991).
_____________________________
The tragic death of the woman should perhaps remind us that
- there is no SCAM or wellness treatment that is entirely harmless,
- and there are only few ‘would-be gurus’ who know what they are doing.
‘Spagyric’ is a so-called alternative medicine (SCAM) based on the alchemy of Paracelsus (1493-1541). Paracelsus borrowed the term from “separate” (spao) and “combine” (ageiro) to indicate that spagyric preparations are based on the “separation”, “extraction” and “recombination” of the active ingredients of a substance. Plant, mineral as well as animal source materials are used.
The production of spagyric remedies is based on a complex process of maceration and fermentation of a plant extract in alcohol. It takes place in dark, thick-walled glass flasks that are hermetically sealed and kept at a controlled temperature of 37 °C for 28 days. The tincture thus obtained is then decanted and the drug residue is removed from the solution, completely dried, and burned to ash to recover the inorganic components of the plant material. The ash is subsequently dissolved in the alcoholic solution of maceration, and the finished spagyric preparation is left for 12 days before use.
Spagyric is not the most popular of all SCAMs but it certainly does have a significant following. One enthusiast claims that “spagyric essences work on a vibrational level in their action upon the emotional/mind and physical spheres and can be employed in numerous situations. Most people seek help to relieve physical symptoms. Even so, it is often necessary to address the emotional and psychological aspects which may predispose the illness or imbalance. In an era where many people are experiencing life-changing events, the ability to transition smoothly is essential for well-being and vitality. Guidance and help are required to maintain homeostasis. These medicines can help the patient to understand the root cause of their illness and learn to regain control of their lives. Some medicine systems appear to be less effective than in previous times. It has been suggested that the energetic frequency of both the earth and human organism are changing. Therefore these systems may no longer be a vibrational match for the changing frequencies. Spagyric Medicine is designed to ‘tune in with’ these current frequencies. Research suggests that the Spagyric essences may instigate improved health by energetically influencing DNA.”
After reading such weird statements, I ask myself, is there any evidence that spagyric remedies work? In my search for robust studies, I was unsuccessful. There does not seem to be a single controlled study on the subject. However, there are fragmentary reports of a study initiated and conducted by a now largely unknown healer named Karl Hann von Weyhern.
Von Weyhern (1882 – 1954) had taken a few semesters of pharmacy and medicine in Freiburg but remained without a degree. In 1930, he became a member of the NSDAP (Hitler’s Nazi party) and in 1940 he joined the SS. Around 1935, he settled in Munich as a non-medical practitioner (Heilpraktiker), and Heinrich Himmler who has a soft spot for SCAM enlisted as one of his patients. By then von Weyhern had by then made a steep career in the Nazi hierarchy, and he managed to convince Himmler that his spagyric remedies could cure tuberculosis, which was still rampant at the time. They decided to carry out experiments in this regard in the Dachau concentration camp.
Thus, von Weyhern was allowed to test spagyric remedies on forcibly recruited concentration camp prisoners. These experiments lasted for about one year and included around 150 patients who, according to von Weyhern’s iridology diagnosis, suffered from tuberculosis. Half of them were treated with spagyric remedies and the others with conventional treatments. At the end of the experiment, 27 persons were reportedly released into everyday concentration camp life as ‘fit for work’. How many of the 150 prisoners lost their lives due to these experiments is not known. Von Weyhern never filed a final report. It is to be feared that the death toll was considerable. [1]
After the war, von Weyhern denied belonging to the SS, claimed that he had ‘sacrificed himself’ for his patients in the concentration camp, merely had to pay a fine, and was ‘denazified’ in 1948. Subsequently, he resumed his work as a ‘Heilpraktiker’ in Olching, a village near Dachau. [1]
Of course, these infamous experiments cannot be blamed on spagyric medicine. Yet, I feel they are nevertheless important, not least because they seem to reveal the only thing remotely resembling something like evidence.
[1] Die Ärzte der Nazi-Führer: Karrieren und Netzwerke : Mathias Schmidt (Hg.), Dominik Groß (Hg.), Jens Westemeier (Hg.): Amazon.de: BooksA ‘manifesto’ is not something that I come across often in my area of research, i.e. so-called alternative medicine (SCAM). This one is in German, I, therefore, translated it for you:
Manifesto for healthy medicine
With the Manifesto for healthy medicine, we, the citizens and patients alliance weil’s hilft! (‘BECAUSE IT HELPS’) demand a fundamental change in our healthcare system, towards a diverse medicine that focuses on people and health. Be part of it! Sign the manifesto and become part of the movement.
It’s of paramount importance, the Manifesto for healthy medicine. About the way we live. It’s about our health. It’s about you and it’s about me.
We want our healthcare system to actually focus on health.
We want a medicine that doesn’t ask what’s missing, but what is possible.
We want a medicine that cares about people, that takes care, gets to the bottom of things, and uses innovative technologies to do so.
We want more bio, so that the chemistry is right, and we want naturopathic procedures and naturally effective medicines to be recognized, promoted, and researched further.
We want research that creates knowledge because, in addition to studies, it also takes into account the experience of physicians and the needs of patients.
We want carers and doctors to be able to work in a way that is good for their patients and for themselves.
We want people from all healthcare professions to work together as equals.
We want a medicine that creates awareness for a good and healthy life because climate protection also begins in one’s own body.
We want an integrative medicine that puts people at the center and self-evidently combines conventional and natural healing methods.
And we want this medicine to be accessible and affordable for everyone.
We fight for a healthy medicine of the future.
Be part of it!
(sorry, if some of it might sound badly translated but the German original is in parts pure gibberish)
_____________________
Who writes such tosh composed of every thinkable platitude and then pompously calls it a MANIFESTO?
BECAUSE IT HELPS! (weil’s hilft!) is a citizens’ movement that demands a change in the health care system – towards the needs and preferences of patients, towards a holistic view of people, and a focus on health instead of disease. The sensible combination of natural medicine and conventional medicine, an integrative medicine, makes an indispensable contribution to this. This is because it relies fully on the patients and involves them as active partners in the treatment. Modern medicine of the future, therefore, needs the equal cooperation of natural medicine and conventional medicine – in the everyday life of physicians and patients, in the reimbursement by the health insurance companies as well as in research and teaching.
On the information platform www.weils-hilft.de weil’s hilft! informs about current developments in integrative medicine, provides background information, and publishes a podcast once a month. The movement is also active on social media at www.facebook.com/weilshilft and www.instagram.com/weilshilft.
weil’s hilft! is supported by the health and patient organizations GESUNDHEIT AKTIV, KNEIPP-BUND, and NATUR UND MEDIZIN. Together, the alliance represents the interests of more than 220,000 people.
_______________________
One could easily disclose the funny side of this, the utter stupidity of the arguments, the platitudes, fallacies, misunderstandings, ignorance, etc. Yes, that would hardly be difficult. But it would ignore how worrying this and similar movements are. They systematically misinform consumers with the sole aim of persuading them that the integration of unproven or disproven treatments into medical routine is in their interest. Yet, if we only scratch the surface of their arguments, we realize that it is exclusively in the interest of those who profit from this type of misinformation.
There are debates in acupuncture-related systematic reviews and meta-analyses on whether searching Chinese databases to get more Chinese-language studies may increase the risk of bias and overestimate the effect size, and whether the treatment effects of acupuncture differ between Chinese and non-Chinese populations.
For this meta-epidemiological study, a team of investigators searched the Cochrane Library from its inception until December 2021, and identified systematic reviews and meta-analyses with acupuncture as one of the interventions. Paired reviewers independently screened the reviews and extracted the information. They repeated the meta-analysis of the selected outcomes to separately pool the results of Chinese- and non-Chinese-language acupuncture studies and presented the pooled estimates as odds ratios (OR) with 95% confidence interval (CI). They calculated the Ratio of ORs (ROR) by dividing the OR of the Chinese-language trials by the OR of the non-Chinese-language trials, and the ROR by dividing the OR of trials addressing Chinese population by the OR of trials addressing non-Chinese population. The researchers thus explored whether the impact of a high risk of bias on the effect size differed between studies published in Chinese- and in non-Chinese-language, and whether the treatment effects of acupuncture differed between Chinese and non-Chinese populations.
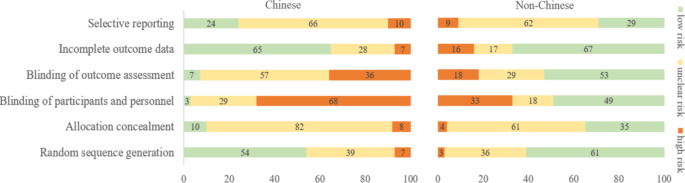
The researchers identified 84 Cochrane acupuncture reviews involving 33 Cochrane groups, of which 31 reviews (37%) searched Chinese databases. Searching versus not searching Chinese databases significantly increased the contribution of Chinese-language literature both to the total number of included trials (54% vs. 15%) and the sample size (40% vs. 15%). When compared with non-Chinese-language trials, Chinese-language trials were associated with a larger effect size (pooled ROR 0.51, 95% CI 0.29 to 0.91). The researchers also observed a higher risk of bias in Chinese-language trials in blinding of participants and personnel (97% vs. 51%) and blinding of outcome assessment (93% vs. 47%). The higher risk of bias was associated with a larger effect estimate in both Chinese language (allocation concealment: high/unclear risk vs. low risk, ROR 0.43, 95% CI 0.21 to 0.87) and non-Chinese-language studies (blinding of participants and personnel: high/unclear risk vs. low risk, ROR 0.41, 95% CI 0.23 to 0.74). However, the team found no evidence that the higher risk of bias would increase the effect size of acupuncture in Chinese-language studies more often than in non-Chinese-language studies (the confidence intervals of all ROR in the high-risk group included 1, Table 3). The researchers further found acupuncture appeared to be more effective in Chinese than in non-Chinese populations.

The authors concluded that the findings of this study suggest the higher risk of bias may lead to an overestimation of the treatment effects of acupuncture but would not increase the treatment effects in Chinese-language studies more often than in other language studies. The difference in treatment effects of acupuncture was probably associated with differences in population characteristics.
The authors discuss that, although searching Chinese databases can substantially increase the number of eligible studies and sample size in acupuncture reviews, the potentially higher risk of bias is an argument that needs to be considered in the inclusion of Chinese-language studies. Patients, investigators, and guideline panels should be cautious when adopting evidence from acupuncture reviews where studies with a high risk of bias contributed with a high weight to the meta-analysis.
The authors observed larger treatment effects of acupuncture in Chinese-language studies than in studies published in other languages. Although the treatment effects of acupuncture tended to be greater in studies with a high risk of bias, this potential overestimation did not differ between studies published in Chinese and in other languages. In other words, the larger treatment effects in Chinese-language studies cannot be explained by a high risk of bias. Furthermore, our study found acupuncture to be more effective in Chinese populations than in other populations, which could at least partly explain the larger treatment effects observed in Chinese-language studies.
I feel that this analysis obfuscates more than it clarifies. As we have discussed often here, acupuncture studies by Chinese researchers (regardless of what language they are published in) hardly ever report negative results, and their findings are often fabricated. It, therefore, is not surprising that their effect sizes are larger than those of other trials.
The only sensible conclusion from this messy and regrettable situation, in my view, is to be very cautious and exclude them from systematic reviews.
The German Heilpraktiker (HP), a non-medically trained practitioner of so-called alternative medicine (SCAM), has repeatedly been the subject of my posts. In a nutshell: the profession was created by the Nazis and was originally destined to disappear within one generation. But this did not happen, and today there are ~100 000 HPs who are allowed to treat almost any condition without mandatory training or experience. Many HP schools exist but you can also become an HP without formal training.
Now a report has been published by undercover journalists investigating these HP schools in Germany. Here I have summarized a few crucial passages for you (if you read German, I strongly recommend reading the original article):
There are more than 150 HP schools in Germany. On average, training costs several thousand euros. There is no uniform and state regulation for the training. The curricula are mostly created by the schools themselves.
In addition to medical and psychological content, the schools often offer seminars that are not based on scientific knowledge. The curricula sometimes include courses such as astrology, homeopathy, or so-called quantum healing. HP organizations give indeed training guidelines. However, these are not met by about 83% of the schools.
The students were isolated at the HP school from their environment and urged to break off contact with their families. “Without us you are nothing. That came so often and I then, unfortunately, believed in it, because I was alone. If I had had no one else from school, then I would really have been completely alone,” explains a former student in an interview. “During that time, I also thought for the first time: Are we in some kind of cult here?
The school’s principal rejects the cult accusation: “We have been confronted with the allegation that we are a cult for some time and have always dealt with it very openly because we are not a cult. The principal also denies other accusations made by former students, saying that the allegations of suggestion, coercion, compulsion, or sweeping statements are simply false. He said he would be happy to face them “in a personal conversation outside the public eye to answer their questions.”
In order to get to the bottom of the treatment methods, the reporter also had herself treated by the principal of the school in an undercover self-experiment. In the first session, she determined that the reporter’s sciatica had been passed on to her by her mother, which is why she should sever her ties with her. In the second session, she recommended that she no longer visit her cancer-stricken grandfather. When the principal learned that the ill grandpa was of the zodiac sign Cancer, she concluded, “Cancer gets cancer.” The cancer, she said, was due to the fact that he had done nothing for his soul. And further, the patient runs the risk of adopting the grandfather’s cancer symptoms when she visits him.
The Hamburg health authority, which is listed as a “supervisory authority” on the school’s homepage, explains in response to an inquiry that no official supervision exists for HP schools. To obtain permission for opening a school, no training is necessary. Neither possible training courses nor institutions offering such training courses are regulated by the state.
The journalist also asked the Federal Health Ministry whether it sees the need for action and legal control. The Ministry’s response was evasive: “If necessary,” the HP law should be reformed in the future.
____________________
This is shocking news for many Germans who believe that HPs are well-trained healthcare professionals. However, those who have read my recently published book cannot be surprised. Poor training is only one of a myriad of deficits of HPs. It is time that the government realizes that the current is unacceptable and endangers public health. It is time, in other words, that the government does something about the HP profession.
Assigning shelf life for homeopathic medicine is – according to the authors of this new, ground-breaking study – an important yet debatable issue. Therefore, the present article is aimed at investigating the problem from a Quantum Electrodynamics point of view and suggests ten years to be a moderate estimate of shelf life.
Data were obtained by the following methods:
- dynamic light scattering,
- atomic force microscopy,
- anomalous dielectric dispersion,
- UV,
- electron spin resonance spectrometry.
The results show the formation of nanosized molecular assemblies. These water clusters containing millions to billions of water molecules, which are created by repeated dilution of aqueous solutions, have been photographed.
The authors draw the following conclusions:
- Ultra-high dilutions (UHD) contain dissipative structures.
- These structures are solute specific
- These structures are tremendously persistent
- Therapeutic values of UHDs are found to continue for a very long time (20-25 years)
Summarizing, we can say that the solute, which in this case is the starting material of homeopathic medicine, leaves its highly stable foot prints in the dissipative structure formed in the UHD solution of polar solvent. Unfortunately, no targeted experiments are done yet to find the exact shelf life. Hence, we wish to suggest that as the shelf life (with proper precautionary measures) of the homeopathic medicine are theoretically expected to be very prolonged and supported by clinical experience, let it be accepted as ten years till future targeted experiments give the exact value, which is expected to be higher than this suggested value.
Were these sensational findings published in a journal like NATURE or SCIENCE? No, they emerged in ‘HPATHY‘ (“the World’s No. 1 Homeopathy Website: Since 2001”). That is a great shame, I think, because they might thus not be awarded the Noble Prize that they clearly deserve.
________________
Joking apart, the self life issue is evidently of some concern to homeopaths. Take this ‘study‘, for instance:
Background: Assignment of expiry date to homeopathic medicines is a subject of important concern to its pharmacists and practitioners. This study compares the regulatory framework for the expiry of homeopathic medicines in four countries: Brazil, Germany, India and the United States.
Findings: Different or no expiry periods are variously followed. Whereas Germany, with some exceptions, employs a maximum expiry of 5 years for both potencies and finished products, Brazil adopts a 5-year expiry for finished products only, potencies used in manufacture being exempted from an assigned expiry date. In India, all homeopathic medicines except dilutions and back potencies have a maximum of 5 years’ shelf-life, including those supplied to consumers. In the United States, homeopathic medicines are exempted from expiry dates.
Comments: There is neither a rational basis nor scientific evidence for assigning a short (3-5 years) expiry period for homeopathic medicines as followed in some of the countries, particularly in light of the fact that some studies have shown homeopathic medications to be effective even after 25 years. Homeopathic ultra-dilutions seem to contain non-material activity that is maintained over time and, since these exhibit different chemical properties compared to the original starting material, it is quite possible they possess properties of longer activity than conventional medicines. Regulators should acknowledge this feature and differentiate expiry of homeopathic medicinal products from that of conventional drugs.
____________________
For once, I almost agree with my homeopathic colleagues:
The activity of homeopathic ultra-dilutions is maintained over time.
However, we need to add just a little explanation to this statement:
This activity is zero.
According to a German court ruling, the homeopathic remedy Meditonsin for colds may no longer be advertised with certain statements. The Higher Regional Court in Hamm, Germany made it clear that it shares the opinion of the Regional Court in Dortmund, which had sentenced the marketing company to desist from making statements such as “rapid and reliable reduction of the intensity of the typical cold symptoms”. Such statements falsely generate the impression that therapeutic success can be expected with certainty. The court made it clear that the company’s appeal against the previous ruling was unlikely to be successful. The company subsequently withdrew its appeal today – and the judgment is now legally binding.

The lawsuit filed by a consumer organization was thus successful. It had criticized several statements as unfair and inadmissible advertising. The Dortmund court shared this view in September 2022 – and according to the spokesman, the Higher Regional Court in Hamm now followed the argumentation of the lower court.
The statements that
- “good efficacy and tolerability were once again impressively confirmed by a pharmacy-based observational study”,
- and “all cold complaints showed a clear improvement in the course of the disease”,
were deemed to be misleading advertising. They must therefore be omitted, the ruling stated.
Meditonsin is currently being advertised as follows:
For support of the immune system at the first signs of a cold to help the body build up the defense against pathogens effectively.
In addition, conditions are made more difficult for the intruders – through an effective medicine: the well-known Meditonsin® supports your defenses and naturally fights the onset of inflammation of the ears, nose and throat with pure homeopathic ingredients.
If applied early and correctly, Meditonsin® helps to ensure that the typical unpleasant symptoms have no chance to develop. Because Meditonsin® is particularly well tolerated and protects the organism, it is for both adults and children alike – a family medicine in the best sense.
Meditonsin contains two homeopathic ingredients in the D5 and one in the D8 dilution. To the best of my knowledge, there is no sound evidence that the remedy is effective for anything.
The Charité in Berlin is a medical school with considerable tradition and reputation. It, therefore, seems a little baffling that this institution agreed to the creation of a professorship in anthroposophical medicine, a branch of so-called alternative medicine (SCAM) that is not only highly implausible but also not supported by sound clinical evidence of doing more good than harm.
The TAZ (a well-known and usually reliable German news outlet) has looked into this issue and just published a report of which I translated the main passages (the additions in brackets were added by me):
In December 2010, after a discussion, the Software AG (an anthroposophical Foundation) offered to finance an anthroposophical professorship at the Charité, according to documents available to the taz. The foundation writes on its website that it wants to use its money to advance the “academization of anthroposophic medicine.” A professorship at a famous institution like the Charité seems like a major prize. The Charité is offered the prospect of 250,000 euros per year.
Investing this money is apparently so important to the Foundation that it spends five years courting the Charité for the professorship. When things don’t go fast enough for them, the project manager writes sharp emails to the Charité administration in December 2016: they are “quite irritated and correspondingly annoyed.” They would be happy “if this never-ending story can finally find a positive conclusion.”
The Foundation apparently has already had an idea of who could take up this professorship early on – although professorships are not actually allowed to be advertised “ad personam,” i.e., tailored to a person. In May 2012, it proposes to include the anthroposophical Havelhöhe Hospital in Berlin (we reported about this place before). It would make a clinical area available for this purpose. There had apparently already been an exchange of views on this.
The contract for the “establishment of a temporary W2 endowed professorship for five years” is dated April 15, 2015. It also states that Charité must indicate that the professorship is funded by the Software AG Foundation. Which it then fails to do.
At this point, the professorship has already been publicly advertised. Very specific requirements are formulated in the advertisement: Among other things, expertise in gastroenterology and oncology is desired, as well as research interest in chronic inflammatory bowel diseases. These happen to be the specializations that the medical director of Havelhöhe Hospital has to show: Harald Matthes (we have met him before on this blog).
Matthes lands as “primo et unico loco” on the appointment list, i.e. as the first-ranked and only candidate. Whether anyone else has applied for the professorship at all, the Charité does not want to answer. Normally, there are three people on an appointment list, unless the requirements for the professorship are too niche. When the Faculty Council votes on filling the professorship, it has to take two ballots because the necessary majority is not reached in the first vote. In March 2017, Matthes is finally appointed professor at the Charité. For proponents of anthroposophic medicine, this has historic significance: “It is tantamount to a knighthood for anthroposophic medicine,” says a chronology of the umbrella organization.
Before his appointment, Harald Matthes negotiated a special request: He wants to remain chief physician in Havelhöhe, which is why he formally took a five-year leave of absence on the first day of his professorial career at Charité. This concept is called the “Jülich Model”. Harald Matthes is not the first to exercise his professorship in this way. It is unusual, however, to cooperate with a private hospital; normally, cooperation is arranged with other research institutions.
Matthes’ employer, Havelhöhe Hospital, also benefits financially from the deal. The Charité transfers a large part of the foundation’s money to Havelhöhe – the documents mention an amount equivalent to a W2 salary. In a letter, the dean of the Charité at the time, Axel Radlach Pries, called Matthes’ wishes “unusual and going beyond previous models of endowed professorships at the Charité.”
Also unusual is that Harald Matthes does not teach any courses at Charité, according to the internal course catalog, even though the contract available to taz specifies nine semester hours of teaching per week. In the Jülich model, two hours of teaching per week are the rule.
So Harald Matthes is the big winner in this: He gets a professorial title without many obligations, while at the same time, money flows to his hospital.
But what does the Charité get out of it? The contract for the establishment of the professorship states that new aspects will thus flow into research, teaching, and patient care. Matthes himself says he is convinced that he is contributing to the scientific progress of the institution. Before his professorship expires after five years, he will ask for an extension in August 2021. “I would like to point out that my work and results in research, teaching, and clinical care have led to international recognition and contributed to the reputation of Charité,” he writes. At the time, he is working on the so-called ImpfSurv study, for which people are asked about possible side effects from the Corona vaccine using an online questionnaire. He gets a lot of media attention for it.
In April 2022, for example, Matthes appears on MDR television, his name superimposed under “Charité Berlin.” He presents the interim results of his study: the serious side effects are much more frequent than the Paul Ehrlich Institute, which is responsible for vaccines, would indicate. Only: This cannot be said at all.
The study has methodological flaws, the Charité distances itself from the statements of its professor. People had participated twice in the survey, and it was not scientific to conclude that there was a connection between symptoms and vaccination without the assessment of a doctor. The study is discontinued.
Before that, when the study was still running, the evaluation commission met several times to discuss the extension of the endowed professorship. In doing so, it “thoroughly reviewed all of Prof. Matthes’ achievements.” What exactly the commission recorded is not known. The document released to the taz is extensively redacted.
What is certain is this: In February 2022, the commission votes for the extension for another five years. Anthroposophy may keep its professorship at the Berlin Charité until at least 2027. The anthroposophical foundation now transfers 293,000 euros per year for this.
_______________________________
I found this acupuncture study from the Department of Oral and Maxillofacial Sciences, “Sapienza” University of Rome, Rome, Italy. As this seems to be a respectable institution, I had a look. What I found was remarkable! Let me show you the abstract in its full beauty:
Background: Pain related to Temporomandibular Disorders (TMD) is severe, negatively affecting patients’ quality of life, and often resistant to conventional treatments. Abdominal Acupuncture (AA) is known to be particularly effective for pain, especially chronic and musculoskeletal pain, but it is still poorly studied and never investigated in TMD patients. Objectives: To analyze the efficacy of AA for the treatment of patients with subacute and chronic pain related to TMD and non-responding to previous conventional therapies (occlusal splint, medications, physical therapy).
Methods: Twenty-eight patients, 24 F and four M (mean age 49.36 years), were recruited from January 2019-February 2021. All patients underwent AA treatment: two sessions per week for four weeks, for a total of eight sessions. At the beginning of therapy (T0) and at the end of the cycle (T1) the following data were evaluated: maximum mouth opening (MMO); cranio-facial pain related to TMD (verbal numeric scale, VNS); pain interference with normal activities and quality of life of patients (Brief Pain Inventory, BPI); oral functioning (Oral Behavior Checklist, OBC); impression of treatment effectiveness (Patients’ Global Impression of Improvement, PGI-I Scale). Statistical comparison of data before and after the AA treatment was performed by Wilcoxon’s signed-rank test (significance level p < 0.05).
Results: The MMO values were significantly improved after one cycle of AA (p = 0.0002). In addition, TMD-related pain had a statistically significant decline following AA treatment (all p < 0.001). Patients’ general activity and quality of life (BPI) were described as improved following a course of AA, with statistically significant values for all aspects considered (all p < 0.05).
Conclusion: Abdominal acupuncture resulted in effective treatment of subacute/chronic resistant pain related to TMD, capable of improving mandibular function and facial pain, and reduced the interference of pain affecting patients’ quality of life.
_____________________
Shocked?
Me too!
This study did not include a control group. Such uncontrolled studies are not necessarily useless. In areas where there is no prior evidence, they can be a reasonable starting point for further research. In the case of TMD/acupuncture, however, this does not imply. Here we already have about a dozen controlled trials. This means an uncontrolled study cannot possibly contribute to our knowledge. This means that the present study is useless. And that, in turn, means it is unethical.
But even if we ignore all this, the study is very misleading. It concludes that acupuncture improved TMD. This, however, can be doubted!
- What about placebo?
- What about regression toward the mean?
- What about the natural history of the condition?
Bad science is regrettable and dangerous, as it
- wastes resources,
- misleads vulnerable patients,
- violates ethics,
- and undermines trust in science.
I fear that the Italian group has just provided us with a prime example of these points.