bias
The increasing demand for fertility treatments has led to the rise of private clinics offering so-called alternative medicine (SCAM) treatments. Even King Charles has recently joined in with this situalion. One of the most frequently offered SCAM infertility treatment is acupuncture. However, there is no good evidence to support the effectiveness of acupuncture in treating infertility.
This study evaluated the scope of information provided by SCAM fertility clinics in the UK. A content analysis was conducted on 200 websites of SCAM fertility clinics in the UK that offer acupuncture as a treatment for infertility. Of the 48 clinics that met the eligibility criteria, the majority of the websites did not provide sufficient information on:
- the efficacy,
- the risks,
- the success rates
of acupuncture for infertility.
The authors concluded that this situation has the potential to infringe on patient autonomy, provide false hope and reduce the chances of pregnancy ever being achieved as fertility declines during the time course of ineffective acupuncture treatment.
The authors are keen to point out that their investigation has certain limitations. The study only analysed the information provided on the clinics’ websites and did not assess the quality of the treatment provided by the clinics.
Therefore, the study’s fndings cannot be generalized to the quality of the acupuncture treatment provided by the clinics.
Nonetheless the paper touches on very important issues: far too many health clinics that offer SCAM for this or that indication operate way outside the ethically (and legally) acceptable norm. They advertise their services without making it clear that they are neither effective nor safe. Desperate consumers thus fall for their promises. In the case of infertility, this might result merely in frustration and loss of (often substantial amounts of) money. In the case of serious disease, such as cancer, this often results in premature death.
It is time, I think, that this entire sector is regualted in a way that it does not endanger the well-being, health, or life of consumers.
This short news report appeared on X [formerly Twitter]:
The Ohio State Medical Board just approved the indefinite suspension Dr. Sherri Tenpenny’s medical license, an osteopathic physician and longtime figure in the anti-vaccine movement. The board got around 350 complaints into her behavior, but that’s not why she’s being suspended.
As this could easily be unreliable, I looked for confirmations … and found several, for instance, this one:
An Ohio physician who sparked widespread ridicule in 2021 after spreading bizarre COVID-19 vaccine conspiracies to the House Health Committee by claiming the jabs magnetize their hosts and “interface” with cell towers had her medical license indefinitely suspended Wednesday. Anti-vaccine spreader Sherri Tenpenny sparked a firestorm in June, 2021 after making the comments, which saw 350 complaints sent to the State Medical Board. According to Cleveland.com, the board’s decision was not based on the comments, rather on procedural grounds, citing Tenpenny’s refusal to cooperate with investigators during the inquiry. “Dr. Tenpenny, neither you nor any doctor licensed by this board is above the law, and you must comply with the investigation,” said Dr. Jonathan Feibel, an orthopedic surgeon and medical board member, according to the outlet. “You have not done so, and therefore, until you do, your license will be suspended.” A lawyer for Tenpenny, Tom Renz, described the investigation as a form of “harassment” on her “free speech rights.” Tenpenny did not speak after the announcement, however Renz declared, “This appears very much like a lynch mob.”
Who is Sherry Tenpenny? Here is what Wiki tells us about her:
Sherri J. Tenpenny is an American anti-vaccination activist and conspiracy theorist who promulgates the disproven hypothesis that vaccines cause autism.[1] An osteopathic physician, she is the author of four books opposing vaccination. A 2015 lecture tour of Australia was canceled due to a public outcry over her views on vaccination, which oppose established scientific consensus. A 2021 Center for Countering Digital Hate analysis concluded that Tenpenny is among the top twelve people spreading COVID-19 misinformation and pseudoscientific anti-vaccine misinformation on social media platforms. She has falsely asserted that the vaccines magnetize people and connect them with cellphone towers…
The story is puzzling, in my view. The biggest question for me is this:
Why only now?
She should have been suspended years ago!
Online misinformation is disproportionality created and spread by people with extreme political attitudes, especially among the far-right. There is a debate in the literature about why people spread misinformation and what should be done about it. According to the purely cognitive account, people largely spread misinformation because they are lazy, not biased. According to a motivational account, people are also motivated to believe and spread misinformation for ideological and partisan reasons. To better understand the psychological and neurocognitive processes that underlie misinformation sharing among the far-right, an international team of researchers conducted a cross-cultural experiment with conservatives and far-right partisans in the Unites States and Spain (N = 1,609) and a neuroimaging study with far-right partisans in Spain (N = 36).
Far-right partisans in Spain and U.S. Republicans who highly identify with Trump were more likely to share misinformation than center-right voters and other Republicans, especially when the misinformation was related to sacred values (e.g., immigration). Sacred values predicted misinformation sharing above and beyond familiarity, attitude strength, and salience of the issue. Moreover, far-right partisans were unresponsive to fact-checking and accuracy nudges. At a neural level, this group showed increased activity in brain regions implicated in mentalizing and norm compliance in response to posts with sacred values.
The authors concluded that these results suggest that the two components of political devotion – identity fusion and sacred values – play a key role in misinformation sharing, highlighting the identity-affirming dimension of misinformation sharing. We discuss the need for motivational and identity-based interventions to help curb misinformation for high-risk partisan groups.
People who have followed the discussions on this blog closely could be forgiven in assuming that right-wing political devotion also plays an important role in spreading misinformation about healthcare (e.g. vaccination) and so-called alternative medicine (SCAM). It would be good, if someone could test this hypothesis more directly.
PS
Just as I had finished writing this post, I came across a quote given yesterday by Ben Habib on GBN:
“I’m very reluctant to put my destiny in the hands of scientists. You know, unbridled authority given to faux knowledge.”
QED
We discussed the 2015 Australian NHMRC report on homeopathy many times before, e.g.:
- Homeopathy: the 2015 NHMRC report and its criticism re-analysed
- HOMEOPATHY: the NHMRC report revisited
- Ombudsman investigates ‘flawed’ homeopathic study
- The final verdict on homeopathy: it’s a placebo
In a nutshell, the report was an hugely influential analysis of the effectiveness of homeopathy which came to squarely negative conclusions. Thus it was celebrated as a thorough and conclusive piece evidence demonstrating the madness of homeopathy. Unsurprisingly, homeopaths did not like it at all and produced various criticisms claiming that it was neither thorough nor conclusive.
Now the final evaluation of what has been going on was finally published (ISSUED BY THE COMMONWEALTH OMBUDSMAN, IAIN ANDERSON, ON 4 AUGUST 2023):
The Office of the Commonwealth Ombudsman (the Office) has finalised an investigation relating to the National Health and Medical Research Council’s (NHMRC) review of the evidence for the effectiveness of homeopathy, conducted between 2010 and 2015. We commenced this investigation in September 2017 in response to concerns raised with us about how the NHMRC review had proceeded.
The Office conducts its investigations in private, and the Ombudsman generally does not make a public statement in the absence of a formal report. In the circumstances of this matter, including that the then-Ombudsman released a public statement on 4 June 2021 which acknowledged the Office was investigating, we believe it is important to share publicly the information we can, now that the investigation is complete.
Our investigation was finalised in July 2023. We acknowledge the length of time the investigation has taken. This is in part due to the extensive efforts the Office made to source independent scientific expertise to advise us on some detailed and specific questions of scientific methodology that were raised with our Office, including some that were only brought to our attention as our investigation progressed. Despite our best efforts, it was not possible to engage an expert (or experts) to provide independent advice to our Office on this subject. In the absence of independent, expert scientific expertise we have not been able to conclusively determine those matters of scientific methodology. This did not prevent our Office from forming a view on other aspects of the matter.
Our investigation did not result in any adverse findings about the review or the NHMRC. When finalising investigations, we may offer comments and suggestions to an agency about areas for future improvement. In this instance, we offered comments and suggestions to the NHMRC about how it records and publicly explains decisions about its activities. The NHMRC also independently made several improvements to its processes during the course of our investigation.
________________
In essence, this means that the conclusions of the report stand:
Homeopathy should not be used to treat health conditions that are chronic, serious, or could become serious. People who choose homeopathy may put their health at risk if they reject or delay treatments for which there is good evidence for safety and effectiveness. People who are considering whether to use homeopathy should first get advice from a registered health practitioner. Those who use homeopathy should tell their health practitioner and should keep taking any prescribed treatments.
Thus the matter is closed – that is closed for rational thinkers. For irrationalists, the matter will no doubt continue to be a stone of contention. No, homeopath will be able to accept these conclusions simply because a member of a cult ceases to be a cultist once he/she accepts the criticism agaist the cult.
There is evidence that, in the US, Republican-leaning counties have had higher COVID-19 death rates than Democratic-leaning counties and similar evidence of an association between political party affiliation and attitudes regarding COVID-19 vaccination. This investigation assessed political party affiliation and mortality rates for individuals during the initial 22 months of the COVID-19 pandemic.
A cross-sectional comparison of excess mortality between registered Republican and Democratic voters between March 2020 and December 2021 adjusted for age and state of voter registration was conducted. Voter and mortality data from Florida and Ohio in 2017 linked to mortality records for January 1, 2018, to December 31, 2021, were used in data analysis. The main outcome measure was the excess weekly death rates during the COVID-19 pandemic adjusted for age, county, party affiliation, and seasonality.
Between January 1, 2018, and December 31, 2021, there were 538 159 individuals in Ohio and Florida who died at the age of 25 years or older in the study sample. The median age at death was 78 years (IQR, 71-89 years). Overall, the excess death rate for Republican voters was 2.8 percentage points, or 15%, higher than the excess death rate for Democratic voters (95% prediction interval [PI], 1.6-3.7 percentage points). After May 1, 2021, when vaccines were available to all adults, the excess death rate gap between Republican and Democratic voters widened from −0.9 percentage points (95% PI, −2.5 to 0.3 percentage points) to 7.7 percentage points (95% PI, 6.0-9.3 percentage points) in the adjusted analysis; the excess death rate among Republican voters was 43% higher than the excess death rate among Democratic voters. The gap in excess death rates between Republican and Democratic voters was larger in counties with lower vaccination rates and was primarily noted in voters residing in Ohio.
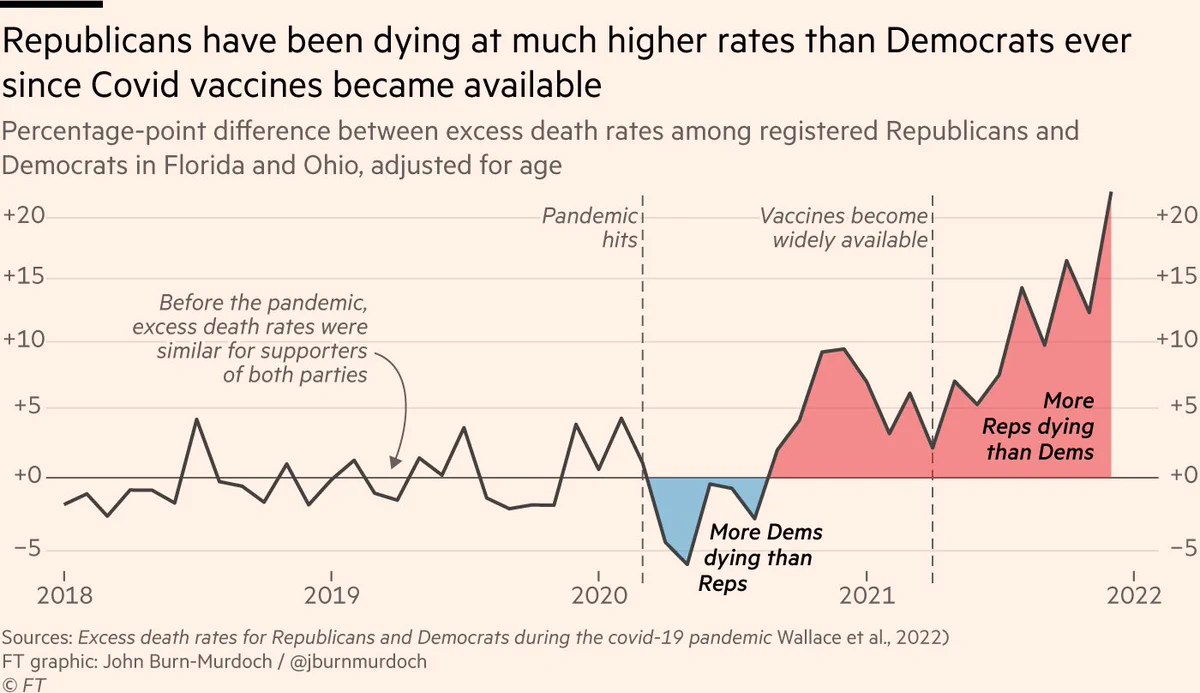
The authors concluded that, in this cross-sectional study, an association was observed between political party affiliation and excess deaths in Ohio and Florida after COVID-19 vaccines were available to all adults. These findings suggest that differences in vaccination attitudes and reported uptake between Republican and Democratic voters may have been factors in the severity and trajectory of the pandemic in the US.
In light of what has been discussed repeatedly, these findings are in my view most impressive and seem to speak for themselves. The authors are nevertheless prudent and stress that their study has several limitations which mean that we ought to interpret their results with caution.
- First, there are plausible alternative explanations for the difference in excess death rates by political party affiliation beyond the explanatory role of vaccines discussed herein.
- Second, the mortality data, although detailed and recent, only included approximately 83.5% of deaths in the US and did not include the cause of death. Although overall excess death patterns in our data are similar to those in other reliable sources, such as the Centers for Disease Control and Prevention National Center for Health Statistics data, it is possible that the deaths that our study data did not include may disproportionately occur among individuals registered with a particular political party, potentially biasing our results. In addition, the completeness of the mortality data may vary across states or time, potentially biasing our estimates of excess death rates.
- Third, all excess death models rely on fundamentally untestable assumptions to construct the baseline number of deaths one would expect in the absence of the COVID-19 pandemic.
- Fourth, because no information on individual vaccination status was available, analyses of the association between vaccination rates and excess deaths relied on county-level vaccination rates.
- Fifth, the study was based on data from 2 states with readily obtainable historical voter registration information (Florida and Ohio); hence, the results may not generalize to other states.
The World Federation of Chiropractic (WFC) has recently launched a new Global Patient Safety (GPS) initiative:
Unanimously approved by the WFC Board at its May meeting, the project will be overseen by the Research Committee and involve the establishment of an expert task force. Planned projects will include a scoping review, identification of best practices in incident reporting and learning, risk management in chiropractic practice and knowledge translation activities.
In recent years, patient safety has increasingly been in the spotlight as health systems strive to reduce unnecessary incidents and iatrogenic injury.
“With adverse events having the potential to impact trust and confidence in the chiropractic profession, it is important that we do as much as possible to inform ourselves in relation to the risks and benefits of chiropractic treatments and related activities,” said Prof. Richard Brown DC, LL.M, WFC Secretary- General.
“While we know that serious adverse events are rare, patients with multiple co-morbidities and known risk factors require special attention. The WFC GPS Task Force will highlight key areas of patient safety to support chiropractors, build and strengthen the existing safety culture and help to meet the expectations of patients and the public.”
Chiropractors use a package of interventions in their treatment of patients, including hands-on care, adjunct therapies, health promotion, advice and exercise prescription. The process of shared decision-making involves consideration by the chiropractor of the suitability and safety of each intervention. In addition to direct patient care, chiropractors also have a duty to consider the safety of their offices and clinics.
A WHO resolution on patient safety, passed in 2019 at the World Health Assembly, made a commitment to take global action in tackling avoidable harm.
Its subsequent publication, Global Action on Patient Safety, set out goals and targets to reduce morbidity from healthcare related incidents.
Chair of the Task Force and Research Committee vice-chair, Dr Katie Pohlman DC, PhD, said: “With the current global focus on patient safety, I’m proud to be leading this WFC Task Force, which will support the chiropractic profession but, most importantly, work to minimize adverse events and protect patients.
“The creation of an open, transparent culture of patient safety is key to maintaining trust and credibility. The Task Force is looking forward to adding to the body of knowledge and advancing safe, evidence-based, people-centered practice.”
The WFC GPS Task Force will report to Research Committee Chair, Assoc. Prof Sidney Rubinstein. It will include members of the existing Research Committee as well as external experts.
____________________________
At first, most people will think: WHAT A GOOD IDEA!
After a bit of reflection, however, some might ponder: WHY ONLY NOW AND NOT DECADES AGO?
And after reading the above text carefully, skeptics might feel that the exercise can already be classified as a PR gimmick that will not generate the needed information:
- The WFC has yet again failed to establish a monitoring system of adverse effects; without it ‘patient safety’ is not achievable.
- They claim that “we know that serious adverse events are rare”. How do they know this? And if they already are convinced of this, the new task force is bound to be a pure ‘white wash’.
- They think an “existing safety culture” exists in chiropractic. This is wishful thinking and far from reality.
- They speak of the “expectations of patients and the public” but ignore the need for a monitoring system accessible to the public.
The website of the World Federation of Chiropractic (WFC) points out that public health is defined by the WHO as follows:
“Activities to strengthen public health capacities and service aim to provide conditions under which people can maintain to be healthy, improve their health and wellbeing, or prevent the deterioration of their health. Public health focuses on the entire spectrum of health and wellbeing, not only the eradication of particular diseases.”
The WFC then continues stating this:
As primary contact health professionals, chiropractors can play an important role as public health advocates. This can range from providing support and advice on health matters such as physical activity, diet, and fitness as well as lifestyle choices such as injury prevention and avoiding tobacco use. Chiropractors can also play a role in counselling patients and communities on the benefits of public health measures, especially as this relates to immediate health needs of each region.
I think that this might merit a few comments.
- Physical activity is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Diet is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Fitness is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Lifestyle choice is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Injury prevention is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Avoiding tobacco use is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
- Counseling is undoubtedly an important issue for public health; however, there are clearly healthcare professionals who are in a better-informed position to advise on it than chiropractors.
So, what is the real contribution of chiropractors to public health?
- Chiropractors tend to advise their clients against vaccinations.
- Some mislead the public by claiming they boost immunity and prevent serious infections.
- Many undermine evidence-based medicine by promoting obsolete myths such as ‘the innate’ or subluxations.
- Many sell supplements that could interact with prescription drugs.
- Many make bogus health claims for profit.
I would therefore argue that, on balance, the contribution of chiropractors to public health might be considerable …
sadly, however, it goes in the wrong direction.
Charles has a well-documented weakness for so-called alternative medicine (SCAM) – not just any SCAM but predominantly the type of SCAM that is both implausible and ineffective. Therefore, nobody can be all that surprised to read in THE TIMES that he has decided to use SCAM for helping women who have difficulties getting pregnant.

If one really wanted to employ SCAM for this aim one is spoilt for choice. In fact, there are only few SCAMs that don’t claim to be useful for this purpose.
A recent review, for instance, suggested that some supplements might be helpful. Other authors advocate SCAMs such as acupuncture, moxibustion, Chinese herbal medicine, psychological intervention, biosimilar electrical stimulation, homeopathy, or hyperbaric oxygen therapy.
Yes, I know! The evidence for these treatments is lousy, and I would never issue a recommendation based on such flimsy evidence.
Yet, the SCAM project at Dumfries House, the Scottish stately home Charles restored in 2007, offers acupuncture, reflexology, massage, yoga, and hypnotherapy for infertile women.
REFLEXOLOGY for female infertility?
Reflexology, also called zone therapy, is a manual treatment where pressure is applied usually to the sole of the patient’s foot and sometimes also to other areas such as the hands or ears. According to its proponents, foot reflexology is more than a simple foot massage that makes no therapeutic claims beyond relaxation. It is based on the idea that the human body is divided into 10 zones each of which is represented on the sole of the foot. Reflexologists employ maps of the sole of the foot where the body’s organs are depicted. By massaging specific zones which are assumed to be connected to specific organs, reflexologists believe to positively influence the function of these organs. While reflexology is mostly used as a therapy, some therapists also claim they can diagnose health problems through feeling tender or gritty areas on the sole of the foot which, they claim, correspond to specific organs.
Reflexology is not merely implausible as a treatment for infertility, it also boasts of some fairly rigorous trial evidence. A clinical trial (perhaps even the most rigorous of all the trials of SCAM for female fertility problems) testing whether foot reflexology might have a positive effect on the induction of ovulation stated that “the results suggest that any effect on ovulation would not be clinically relevant”.
So, as so often before in the realm of SCAM, Charles has demonstrated that his lack of critical thinking leads him to the least promising options.
Well done, Your Majesty!
Diabetic peripheral neuropathy (DPN) is a common complication of diabetes mellitus (DM) that can cause annoying symptoms. To address this condition, several treatment approaches have been proposed, including static magnetic field (SMF) therapy, which has shown promise in treating neurological conditions. Therefore, this study aimed to investigate the effects of SMF therapy on symptomatic DPN and the quality of life (QoL) in patients with type 2 diabetes.
A double-blind, randomized, placebo-controlled trial was conducted from April to October 2021. Sixty-four DPN patients (20 males, 44 females) were recruited for the study via invitation. The participants were divided into two groups: the magnet group, which used magnetic ankle bracelets (155 mT) for 12 weeks, and the sham group, which used non-magnetic ankle bracelets for the same duration. Neuropathy Symptom Score (NSS), Neuropathic Disability Score (NDS), and Visual Analogue Scale (VAS) were used to assess neuropathy symptoms and pain. In addition, the Neuropathy Specific Quality of Life Questionnaire (Neuro-QoL) tool was used to measure the patients’ quality of life.
Before treatment, there were no significant differences between the magnet and sham groups in terms of the NSS scores (P = 0.50), NDS scores (P = 0.74), VAS scores (P = 0.17), and Neuro-QoL scores (P = 0.82). However, after 12 weeks of treatment, the SMF exposure group showed a significant reduction in NSS scores (P < 0.001), NDS scores (P < 0.001), VAS scores (P < 0.001), and Neuro-QoL scores (P < 0.001) compared to the baseline. The changes in the sham group, on the other hand, were not significant.
The authors concluded that according to obtained data, SMF therapy is recommended as an easy-to-use and drug-free method for reducing DPN symptoms and improving QoL in diabetic type-2 patients.
Our own study and systematic review of the effects of magnetic bracelets and similar devices suggested that the effects of such treatments are due to placebo responses. Therefore, I find the findings of this new study most surprising. Not only that, to be honest, I also find them suspect. Apart from the fact that the treatment has no biological plausibility, I have three main reasons for my skepticism.
- The authors stated that there was no distinguishable difference between the sham and SMF devices in terms of their appearance, weight, or texture, which helped to ensure that the study was double-blinded. This is nonsense, I am afraid! The verum device is magnetic and the sham device is not. It is hardly conceivable that patients who handle such devices for any length of time do not discover this simple fact and thus de-blind themselves. In turn, this means that a placebo effect can easily explain the outcomes.
- Authors who feel that their tiny study of a highly implausible therapy lends itself to concluding that their therapy ‘is recommended as an easy-to-use and drug-free method for reducing DPN symptoms and improving QoL’ can, in my view, not be taken seriously.
- Something that always makes me suspicious of clinical trials is a lack of a placebo response where one would normally expect one. In this study, the control group exhibits hardly any placebo response. Wearing a strap around your ankle that allegedly emits therapeutic radiation would result in quite a strong placebo effect, according to our own findings.
So, forgive me if I do not trust this study any further than I can throw it! And pardon me if I still think that our previous conclusion is correct: The evidence does not support the use of static magnets for pain relief, and therefore magnets cannot be recommended as an effective treatment.
This review assessed the role of homoeopathy in the therapeutic management of substance use disorders (SUD) through a systematic web-based literature search. A comprehensive search was conducted online and manually to identify homoeopathic research studies published between 1993 and 2022 on SUD in international databases and the Central Council of Research in Homoeopathy library. Relevant studies were categorised and assessed in terms of study designs, number of participants, evidence grades and clinical outcome parameters. A total of 21 full-text studies were screened and evaluated. Risk of bias (RoB) was assessed for all studies and model validity was appraised for the included RCTs’.
10 studies were included:
- 3 Randomised Controlled Trials,
- 3 Observational studies,
- 1 Pilot study,
- 1 observational comparative study,
- 1 retrospective cohort study,
- 1 case series.
Three studies have a level of evidence of 1b with an ‘A’ grade of recommendation, which consists of the RCTs only. The most commonly prescribed medicines identified were:
- Arsenic album,
- Nux vomica,
- Lycopodium,
- Pulsatilla,
- Sulphur,
- Staphysagria,
- Belladonna,
- Ipecac,
- Chamomilla,
- Rhustox,
- Phosphorus,
- Lachesis.
A high risk of bias was elicited in most of the observational studies accentuating the need for more robust methodological studies.
The authors concluded that the majority of the studies have a small number of recruitments. Pragmatic studies with larger sample sizes and validated outcome measures may be designed further to validate the
promising role of homoeopathic medicines in SUDs and generate quality evidence.
The paper is surprising! Most of the studies are not RCTs and thus cannot come even near suggesting a causal effect of homeopathy. The three RCTs are the following:
- Manchanda RK, Janardanan Nair KR, Varanasi R, Oberai P, Bhuvaneswari R, Bhalerao R, et al. A randomised comparative trial in the management of alcohol dependence: Individualised homoeopathy versus standard allopathic treatment. Indian J Res Homoeopathy; 2016.
- Adler UC, Acorinte AC, Calzavara FO, et al. Double-blind evaluation of homeopathy on cocaine craving: A randomised controlled pilot study. J Integr Med. 2018; 16(3):178-184.
- Grover A, Bhushan B, Goel R. Double-blind placebo-controlled trial of homoeopathic medicines in the
management of withdrawal symptoms in opium addicts and its alkaloid derivatives dependents. Indian J Res Homoeopathy. 2009;3:41-4.
All of these 3 studies were assessed by the review authors as having major flaws. Only one is available on Medline:
Background: Brazil is among the nations with the greatest rates of annual cocaine usage. Pharmacological treatment of cocaine addiction is still limited, opening space for nonconventional interventions. Homeopathic Q-potencies of opium and Erythroxylum coca have been tested in the integrative treatment of cocaine craving among homeless addicts, but this setting had not proven feasible, due to insufficient recruitment.
Objective: This study investigates the effectiveness and tolerability of homeopathic Q-potencies of opium and E. coca in the integrative treatment of cocaine craving in a community-based psychosocial rehabilitation setting.
Design, setting, participants, and interventions: A randomized, double-blind, placebo-controlled, parallel-group, eight-week pilot trial was performed at the Psychosocial Attention Center for Alcohol and Other Drugs (CAPS-AD), Sao Carlos/SP, Brazil. Eligible subjects included CAPS-AD patients between 18 and 65 years of age, with an International Classification of Diseases-10 diagnosis of cocaine dependence (F14.2). The patients were randomly assigned to two treatment groups: psychosocial rehabilitation plus homeopathic Q-potencies of opium and E. coca (homeopathy group), and psychosocial rehabilitation plus indistinguishable placebo (placebo group).
Main outcome measures: The main outcome measure was the percentage of cocaine-using days. Secondary measures were the Minnesota Cocaine Craving Scale and 12-Item Short-Form Health Survey scores. Adverse events were reported in both groups.
Results: The study population comprised 54 patients who attended at least one post-baseline assessment, out of the 104 subjects initially enrolled. The mean percentage of cocaine-using days in the homeopathy group was 18.1% (standard deviation (SD): 22.3%), compared to 29.8% (SD: 30.6%) in the placebo group (P < 0.01). Analysis of the Minnesota Cocaine Craving Scale scores showed no between-group differences in the intensity of cravings, but results significantly favored homeopathy over placebo in the proportion of weeks without craving episodes and the patients’ appraisal of treatment efficacy for reduction of cravings. Analysis of 12-Item Short-Form Health Survey scores found no significant differences. Few adverse events were reported: 0.57 adverse events/patient in the homeopathy group compared to 0.69 adverse events/patient in the placebo group (P = 0.41).
Conclusions: A psychosocial rehabilitation setting improved recruitment but was not sufficient to decrease dropout frequency among Brazilian cocaine treatment seekers. Psychosocial rehabilitation plus homeopathic Q-potencies of opium and E. coca were more effective than psychosocial rehabilitation alone in reducing cocaine cravings. Due to high dropout rate and risk of bias, further research is required to confirm our findings, with specific focus on strategies to increase patient retention.
This study can hardly be said to show convincing evidence for homeopathy.
This paper is all the more surprising if we consider the affiliations of the authors:
- Clinical Research Unit (H), Aizawl under Central Council for Research in Homoeopathy, Ministry of AYUSH, Govt. of India, India.
- All India Institute of Ayurveda, New Delhi, India.
- Department of Materia Medica, Madhav Homoeopathic Medical College and Hospital, Madhav Hills,
Opposite Banas River, Abu Road, Rajasthan, India.
It is time, I think, that Indian officials and researchers learn some critical thinking and formulate the conclusions of reviews based on the evidence they produced. This would be a start:
Our review has not generated convincing evidence to suggest that homeopathy is effective in treating SUDs.