Edzard
I usually take ‘market reports’ with a pinch of salt. Having said that, this document makes some rather interesting predictions:
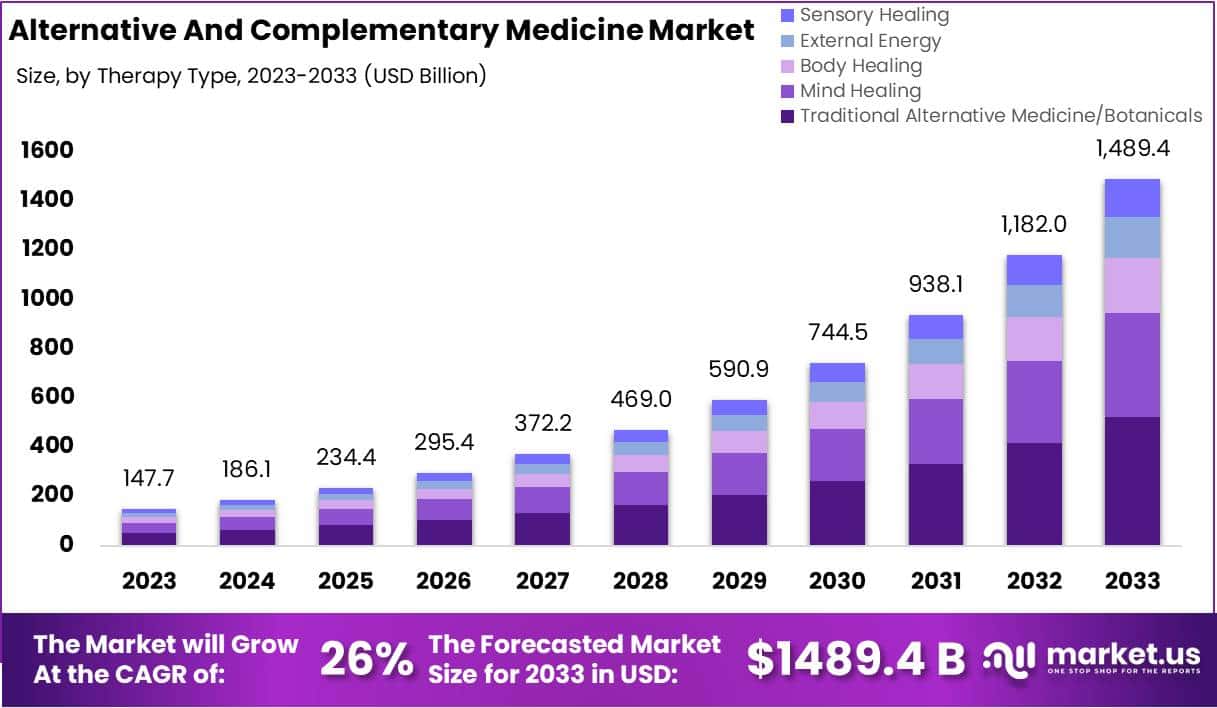
The size of the market for so-called alternative medicine (SCAM) is projected to expand from USD 147.7 billion in 2023 to approximately USD 1489.4 billion by the year 2033. This projection indicates a remarkable Compound Annual Growth Rate (CAGR) of 26% over the forecast period.
The market for SCAM is experiencing significant growth, fueled by increasing consumer interest in natural and holistic health solutions. This trend reflects a broader shift in societal attitudes towards health and wellness, emphasizing preventive care and natural health practices.
The market’s dynamics are influenced by various factors, including consumer preferences, regulatory standards, and evolving perceptions of health and wellness. As the popularity of these alternative therapies grows, it is crucial for individuals to consult with healthcare professionals to ensure that these non-conventional approaches are safely and effectively incorporated into their overall health regimen. The increasing acceptance of SCAM underscores a collective move towards more personalized and holistic healthcare solutions, resonating with today’s health-conscious consumers.
In 2023, Traditional Alternative Medicine/Botanicals led the market, capturing a 35.2% share, which reflects a strong consumer inclination towards these treatments. Dietary Supplements were prominent in the market, securing a 25.1% share in 2023, which underscores the high consumer demand for nutritional aids. Direct Sales were the most favored distribution channel, accounting for 43.2% of the market share in 2023, which indicates their significant impact on guiding consumer purchases. Pain Management was the predominant application area, holding a 24.9% market share in 2023, propelled by the growing acknowledgment of non-pharmacological treatment options. Adults represented a substantial portion of the market, making up 62.33% in 2023, signifying a marked preference for SCAM therapies within this age group. Europe stood out as the market leader, claiming a 42.6% share in 2023, a position supported by widespread acceptance, governmental backing, and an increasing elderly population. The regions of North America and Asia-Pacific are highlighted as areas with potential, signaling opportunities for market expansion beyond the European stronghold in the upcoming years.
Leading Market Players Are:
- Columbia Nutritional
- Nordic Nutraceuticals
- Ramamani Iyengar Memorial Yoga Institute
- The Healing Company Ltd.
- John Schumacher Unity Woods Yoga Centre
- Sheng Chang Pharmaceutical Company
- Pure encapsulations LLC.
- Herb Pharm
- AYUSH Ayurvedic Pte Ltd.
Recent developments:
- In December 2023, Adoratherapy launched the Alkemie Chakra Healing Line, an aromatherapy range aimed at harmonizing the seven chakras.
- Coworth Park introduced the Hebridean Sound Treatment in October 2023, merging traditional Hebridean sounds with guided meditation to offer a novel, restorative wellness experience.
- The World Health Organization released draft guidelines in September 2023 for the safe, effective application of traditional medicines.
- Telehealth services, expanding significantly in August 2023, have broadened the reach of SCAM, enhancing patient access to these treatments.
Microplastics are tiny polymer fragments that range from less than 0.2 inch to 1/25,000th of an inch. Smaller particles are called nanoplastics and are measured in billionths of a metre. Microplastics and nanoplastics (MNPs) are emerging as a potential risk factor for human health and for cardiovascular disease in particular. However, direct evidence that this risk extends to humans has so far been lacking. This investigation is a first step towards filling the gap.
The researchers conducted a prospective, multicenter, observational study involving patients who were undergoing carotid endarterectomy for asymptomatic carotid artery disease. The excised carotid plaque specimens were analyzed for the presence of MNPs with the use of pyrolysis–gas chromatography–mass spectrometry, stable isotope analysis, and electron microscopy. Inflammatory biomarkers were assessed with enzyme-linked immunosorbent assay and immunohistochemical assay. The primary end point was a composite of myocardial infarction, stroke, or death from any cause among patients who had evidence of MNPs in plaque as compared with patients with plaque that showed no evidence of MNPs.
A total of 304 patients were enrolled in the study, and 257 completed a mean (±SD) follow-up of 33.7±6.9 months. Polyethylene was detected in carotid artery plaque of 150 patients (58.4%), with a mean level of 21.7±24.5 μg per milligram of plaque; 31 patients (12.1%) also had measurable amounts of polyvinyl chloride, with a mean level of 5.2±2.4 μg per milligram of plaque. Electron microscopy revealed visible, jagged-edged foreign particles among plaque macrophages and scattered in the external debris. Radiographic examination showed that some of these particles included chlorine. Patients in whom MNPs were detected within the atheroma were at higher risk for a primary end-point event than those in whom these substances were not detected (hazard ratio, 4.53; 95% confidence interval, 2.00 to 10.27; P<0.001).
The authors concluded that, in this study, patients with carotid artery plaque in which MNPs were detected had a higher risk of a composite of myocardial infarction, stroke, or death from any cause at 34 months of follow-up than those in whom MNPs were not detected.
This is an impressive study – so much so that I report it here even though it has no connection to so-called alternative medicine, the focus of my blog. The fact that 58% of all plaques contained MNPs seems alarming. The finding that the presence of these MNPs is associated with a poor cardiovascular prognosis seems even more concerning.
MNPs have been found in every environmental compartment on earth. They are ingested not just by humans but by most animals as well. Even though research into these issues is most active, their effects are so far still under-researched and not fully understood.
The authors of the new investigation are rightly cautious: “Our data must be confirmed by other studies and on larger populations,” said Marfella, professor of internal medicine and director of the department of medical and surgical sciences at the University of Campania Luigi Vanvitelli in Naples, Italy. “However, our study convincingly highlights the presence of plastics and their association with cardiovascular events in a representative population affected by atherosclerosis.”
Of course, many questions are as yet unanswered but the subject is as worrying as it is important, e.g.:
- Should exposure to MNPs be considered a cardiovascular risk factor?
- What organs in addition to the heart may be at risk?
- How can we reduce exposure?”
I wish I knew the ansers.
According to its authors, this study‘s objective was to demonstrate that acupuncture is beneficial for decreasing the risk of ischaemic stroke in patients with rheumatoid arthritis (RA).
The investigation was designed as a propensity score-matched cohort nationwide population-based study. Patients with RA diagnosed between 1 January 1997 and 31 December 2010, through the National Health Insurance Research Database in Taiwan. Patients who were administered acupuncture therapy from the initial date of RA diagnosis to 31 December 2010 were included in the acupuncture cohort. Patients who did not receive acupuncture treatment during the same time interval constituted the no-acupuncture cohort. A Cox regression model was used to adjust for age, sex, comorbidities, and types of drugs used. The researchers compared the subhazard ratios (SHRs) of ischaemic stroke between these two cohorts through competing-risks regression models.
After 1:1 propensity score matching, a total of 23 226 patients with newly diagnosed RA were equally subgrouped into acupuncture cohort or no-acupuncture cohort according to their use of acupuncture. The basic characteristics of these patients were similar. A lower cumulative incidence of ischaemic stroke was found in the acupuncture cohort (log-rank test, p<0.001; immortal time (period from initial diagnosis of RA to index date) 1065 days; mean number of acupuncture visits 9.83. In the end, 341 patients in the acupuncture cohort (5.95 per 1000 person-years) and 605 patients in the no-acupuncture cohort (12.4 per 1000 person-years) experienced ischaemic stroke (adjusted SHR 0.57, 95% CI 0.50 to 0.65). The advantage of lowering ischaemic stroke incidence through acupuncture therapy in RA patients was independent of sex, age, types of drugs used, and comorbidities.
The authors concluded that this study showed the beneficial effect of acupuncture in reducing the incidence of ischaemic stroke in patients with RA.
It seems obvious that the editors of ‘BMJ Open’, the peer reviewers of the study and the authors are unaware of the fact that the objective of such an investigeation is not to to demonstrate that acupuncture is beneficial but to test whether acupuncture is beneficial. Starting a study with the intention to to show that my pet therapy works is akin to saying: “I am intending to mislead you about the value of my intervention”.
One needs therefore not be surprised that the authors of the present study draw very definitive conclusions, such as “acupuncture therapy is beneficial for ischaemic stroke prevention”. But every 1st year medical or science student should know that correlation is not the same as causation. What the study does, in fact, show is an association between acupuncture and stroke. This association might be due to dozens of factors that the ‘propensity score matching’ could not control. To conclude that the results prove a cause effect relationship is naive bordering on scientific misconduct. I find it most disappointing that such a paper can pass all the hurdles to get published in what pretends to be a respectable journal.
Personally, I intend to use this study as a good example for drawing the wrong conclusions on seemingly rigorous research.
An article entitled “Homeopathy for worm infestations in children’s” caught my eye. Here is the un altered abstract:
Unusual sorts of worms can be there in a child’s stomach and may initiate several health complications such as pain, infection etc. To treat worm infections, one must identify about various categories of worms, and after understanding the kind of infection induced by the worm’s the treatment for the babies or children can planned. There are various Homeopathic medicines available which be used to treat worm infections without any side effects on the health of the children’s. In this paper we have discussed how the worm infection has been treated at our homeopathic research institute.
In the paper itself, the author, Dr. AK Dwivedi (Professor and H.O.D, Department of Physiology and Biochemistry, SKRP Guajarati Medical College, Indore, Madhya Pradesh, India), explains:
Homeopathic do not take care of just the disease, but is prescribed on the base of physical, emotional and genetic condition of a person. Homeopathic medicines act on both the mental and physical levels of individuals. Homeopathy is a natural and mild system of medicines that utilizes minute doses of well-researched remedies to improve the body’s natural curing procedure. Homeopathic medicines originate from substances that come’s from plants, minerals & animals.
The author’s conclusion is equally impressive:
On the basis of our research and after analysing the patients after medication we have found that homeopathy can completely cure the worm infection, If the dosages are properly prescribed and taken on that basis of investigation reports from time to time under guidance of experienced Homeopathic Physician worm infection can be treated with homeopathy effectively.
Yes, this level of incompetence could be quite funny! But sadly, it is also quite concerning. Most worm infestations are easily treated with effective conventional therapies. Untreated, they can have serious consequences. To advocate homeopathy – which is of course ineffective – is irresponsible, unethical and arguably criminal, in my view.
There are many variations of acupuncture. Electroacupuncture (EA) and Laseracupuncture (LA) are but two examples both of which are commonly used. However, it remains uncertain whether LA is as effective as EA. This study aimed to compare EA and LA head to head in dysmenorrhea.
A crossover, randomized clinical trial was conducted. EA or LA was applied to selected acupuncture points. Participants were randomized into two sequence treatment groups who received either EA or LA twice per week in luteal phase for 3 months followed by 2-month washout, then shifted to other groups (sequence 1: EA > LA; sequence 2: LA > EA). Outcome measures were heart rate variability (HRV), prostaglandins (PGs), pain, and quality-of-life (QoL) assessment (QoL-SF12). We also compared the effect of EA and LA in low and high LF/HF (low frequency/high frequency) status.
43 participants completed all treatments. Both EA and LA significantly improved HRV activity and were effective in reducing pain (Visual Analog Scale [VAS]; EA: p < 0.001 and LA: p = 0.010) and improving QoL (SF12: EA: p < 0.001, LA, p = 0.017); although without intergroup difference. EA reduced PGs significantly (p < 0.001; δ p = 0.068). In low LF/HF, EA had stronger effects than LA in increasing parasympathetic tone in respect of percentage of successive RR intervals that differ by more than 50 ms (pNN50; p = 0.053) and very low-frequency band (VLF; p = 0.035).
The authors concluded that there is no significant difference between EA and LA in improving autonomic nervous system dysfunction, pain, and QoL in dysmenorrhea. EA is prominent in PGs changing and preserving vagus tone in low LF/HF; yet LA is noninvasive for those who have needle phobia. Whether LA is equivalent with EA and the mechanism warrants further study.
Looking at the affiliations of the authors, one might expect that they should be able to design a meaningful study:
- 1Division of Hemato-Oncology, Department of Internal Medicine, Branch of Zhong-Zhou, Taipei City Hospital, Taipei, Taiwan.
- 2Institute of Traditional Medicine, National Yang-Ming Chiao Tung University, Taipei, Taiwan.
- 3Department of Traditional Medicine, Branch of Yang-Ming, Taipei City Hospital, Taipei, Taiwan.
- 4Department of Traditional Medicine, Branch of Kunming, Taipei City Hospital, Taipei, Taiwan.
- 5Department of Gynecology and Obstetrics, Branch of Yang-Ming, Taipei City Hospital, Taipei, Taiwan.
Sadly, this assumption is evidently mistaken.
The trial certainly does not show what they claim and neither had it ever the chance to show anything relevent. A clinical trial is comparable to a mathematical equation. It can be solved, if it has one unkown; it cannot produce a result, if it has two unknowns.
The efficacy of EA and LA for dysmenorrhea are both unknown. A comparative study with two unknowns cannot produce a meaningful result. EA and LA did not both improve autonomic nervous system dysfunction, pain, and QoL in dysmenorrhea but most likely they both had no effect. What caused the improvement was not the treatment per se but the ritual, the placebo effect, the TLC or other non-specific factors. The maginal differences in other parameters are meaningless; they are due to the fact that – as an equivalence trial – the study was woefully underpowered and thus open to coincidental differences.
Clinical trials should be about contributing to our knowledge and not about contributing to confusion.
Here is the abstract of a recent article that I find worrying:
In 2020, severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) challenged the world with a global outbreak that led to millions of deaths worldwide. Coronavirus disease 2019 (COVID-19) is the symptomatic manifestation of this virus, which can range from flu-like symptoms to utter clinical complications and even death. Since there was no clear medicine that could tackle this infection or lower its complications with minimal adverse effects on the patients’ health, the world health organization (WHO) developed awareness programs to lower the infection rate and limit the fast spread of this virus. Although vaccines have been developed as preventative tools, people still prefer going back to traditional herbal medicine, which provides remarkable health benefits that can either prevent the viral infection or limit the progression of severe symptoms through different mechanistic pathways with relatively insignificant side effects. This comprehensive review provides scientific evidence elucidating the effect of 10 different plants against SARS-CoV-2, paving the way for further studies to reconsider plant-based extracts, rich in bioactive compounds, into more advanced clinical assessments in order to identify their impact on patients suffering from COVID-19.
The conclusions of this paper read as follows:
…since these 10 herbs hold distinct bioactive compounds with significant properties in vitro and with remarkable benefits to human health, it is possible to prevent SARS-CoV-2 infection and reduce its symptomatic manifestations by consuming any of these 10 plants according to the recommended dose. The diversity in bioactive molecules between the different plants exerts various effects through different mechanisms at once, which makes it more potent than conventional synthetic drugs. Nonetheless, more studies are needed to highlight the clinical efficacy of these extracts and spot their possible side effects on patients, especially those with comorbidities who take multiple conventional drugs.
I should point out that the authors fail to offer a single reliable trial that would prove or even imply that any of the 10 herbal remedies can effectively treat or prevent COVID infections (to the best of my knowledge, no such studies exist). Laguage like “it is possible to prevent SARS-CoV-2 infection and reduce its symptomatic manifestations” is therefore not just misleading but highly dangerous and deeply unethical. Sadly, such evidence-free claims abound in herbal medicine.
I think the journal editor, the peer-reviewer, the authors and their universities ( University of Tripoli in Lebanon, American University of the Middle East, Egaila in Kuwait, University of Balamand, Kalhat, Tripoli in Lebanon, Lebanese University, Tripoli in Lebanon, Aix-Marseille Université in France) should be ashamed to produce such dangerous rubbish.
Acute Otitis Media (AOM) is one of the most common acute infections in children and often injudiciously treated by antibiotics. Homeopathy has been claimed to work but is it really effective?
This open label, randomized, controlled, parallel arm trial was conducted on children (aged 0–12 years), suffering from AOM. The primary outcome was changes in Tympanic Membrane Examination scale (TMES) and Acute Otitis Media-Severity of Symptoms (AOM-SOS) scale, time to improvement in pain through Facial Pain Scale-Revised (FPS-R) over 10 days. The need for antibiotics in both groups and the recurrence of subsequent episodes of AOM over 12 months were also compared.
Intention-to-treat analysis was performed on 222 children; Homeopathy (n = 117) (H-group), Allopathy (A-group) (n = 105). There was a statistically significant reduction of scores in H-group compared with A-group at each time point: at day 3 (mean diff. ± sd: 1.71 ± 0.19; 95% CI: 1.34 to 2.07; p = 0.0001), at day 7 (mean diff. ± sd: 1.29 ± 0.24; 95% CI: 0.82 to 1.76; p = 0.0001) and at day 10 (mean diff. ± sd: 1.23 ± 0.25; 95% CI = 0.74 to 1.71; p = 0.0001) favoring homeopathy. Clinical failure by the third day of treatment was observed in 11% and 24% of children in H-group vs A-group (OR: 0.03; 95% CI: 0.001 to 0.52; p = 0.03). None of the children in the H-group required antibiotics, whereas 14 children in the A-group did.
The authors concluded that both therapies seemed to produce comparable effects and appeared safe. The study consolidated the findings observed during a pilot study, i.e., homeopathy is non-inferior to allopathy in managing AOM in children and antibiotics in children can be avoided.
This study was published in the journal ‘Homeopathy’ and originates from the Central Council for Research in Homeopathy, New Delhi, India. Sadly, I do not have the full text of the paper and cannot therefore scrutinize it adequately.
Let me just mention these three facts:
- The journal ‘Homeopathy’ never publishes negative results.
- Indian researchers of homeopathy publish as good as no negative results.
- As far as I can see, the Central Council for Research in Homeopathy, New Delhi, has never published a negative result.
These points do, of course, not necessarily mean that the study is false-positive, but they do not inspire me with confidence. In any case, it seems wise to insist on better evidence. To render it credible, we would need:
- Several rigorous RCTs that test homeopathy for AOM against placebo.
- If (and only then) they show that homeopathy is better than placebo, at least one independent replication of the present study.
As the biological plausibility of all this is close to zero, the chances that this will happen are also zero.
I have left the German skeptics organisation , GWUP, two days ago. This led to many questions and confusion. I therefore feel that I owe it to those skeptics who I may have upset or unsettled to offer a few clarifications (I do appologise, if this does not make much sense to those readers who were unable to follow the various disputes and discussions that took place, mostly in German, on Twitter).
1. Clarification – accusation of antisemitism: This accusation is completely absurd! In my opinion, the 1st re-Tweet that Bartoschek is using is not anti-Semitic. I have posted thousands of tweets, many of which are the opposite of anti-Semitic, as anyone can verify. Moreover, I have worked for the last 30 years to fight antisemitism and can probably show more results of this endeavor than my accuser.
2. Clarification – I can’t find the 2nd re-tweet that Bartoschek exhibits. No idea who found it and where! I can’t remember the text (but I do vaguely remember the graphic), and I certainly didn’t delete anything. I would delete if, if I could find it and be open about it. If it turns out that I am nevertheless at fault, I can only apologise.
3. Clarification – peer-review publications by Hirsch, Huemmler, Bartoschek (who I sarcastically called ‘the GWUP-elite’). After watching a long video of these gentlemen, I began to doubt whether they are true scientists (or even skeptics) at all. Hence my legitimate question. The answer seems to be largely negative.
4. Clarification – Bartoschek claims “Prof Ernst is on the side of the “anti-woke”. However, I have repeatedly emphasised that I do not believe in and even detest both ‘woke’ and ‘anti-woke’.
5. Clarification – Mr Hirsch is the ‘social media manager’ of the GWUP commissioned by Huemmler, the current chair of the GWUP. The fact that he spreads aggressive nonsense in this role under the pseudonym ‘Endgegner der Kommentarspalten’ is inadmissible.
6. Clarification – I have not gained the impression that the current division of the GWUP is primarily idiological in nature (both sides are not far apart in this respect), but believe that it is a rather ridiculous power struggle on a personal level.
7. Clarification – I have left the GWUP because I am sure that I can do my work better without it, because the current tone amongst GWUP members is unacceptable, because the GWUP is currently not converting its membership fees (I estimate ~200 000 per year) into meaningful activities, because the current GWUP ‘elite’ behaves neither as genuine sceptics nor as true scientists, and because I fear that things will only get worse after the AGM in May.
_________________________
My hope is that this is the last time I have to mention this sorry story here on my blog.
Traditional herbal medicine (THM) is frequently used in pediatric populations. This is perticularly true in many low-income countries. Yet THM has been associated with a range of adverse events, including liver toxicity, renal failure, and allergic reactions. Despite these concerns, its impact on multi-organ dysfunction syndrome (MODS) risk has so far not been thoroughly investigated.
This study aimed to investigate the incidence and predictors of MODS in a pediatric intensive care unit (PICU) in Ethiopia, with a focus on the association between THM use and the risk of MODS. It was designed as a single-center prospective cohort study conducted at a PICU in the university of Gondar Comprehensive Specialized hospital, Northwest Ethiopia. The researchers enrolled eligible patients aged one month to 18 years admitted to the PICU during the study period. Data on demographic characteristics, medical history, clinical and laboratory data, and outcome measures using standard case record forms, physical examination, and patient document reviews. The predictors of MODS were assessed using Cox proportional hazards models, with a focus on the association between traditional herbal medicine use and the risk of MODS.
A total of 310 patients were included in the final analysis, with a median age of 48 months and a male-to-female ratio of 1.5:1. The proportion and incidence of MODS were 30.96% (95% CI:25.8, 36.6) and 7.71(95% CI: 6.10, 9.40) per 100-person-day observation respectively. Renal failure (17.74%), neurologic failure (15.16%), and heart failure (14.52%) were the leading organ failures identified. Nearly one-third of patients (32.9%) died in the PICU, of which 59.8% had MODS. The rate of mortality was higher in patients with MODS than in those without. The Cox proportional hazards model identified renal disease (AHR = 6.32 (95%CI: 3.17,12.61)), intake of traditional herbal medication (AHR = 2.45, 95% CI:1.29,4.65), modified Pediatric Index of Mortality 2 (mPIM 2) score (AHR = 1.54 (95% CI: 1.38,1.71), and critical illness diagnoses (AHR = 2.68 (95% CI: 1.77,4.07)) as predictors of MODS.
The authors concluded that the incidence of MODS was high. Renal disease, THM use, mPIM 2 scores, and critical illness diagnoses were independent predictors of MODS. A more than twofold increase in the risk of MODS was seen in patients who used TMH. Healthcare providers should be aware of risks associated with THM, and educate caregivers about the potential harms of these products. Future studies with larger sample sizes and more comprehensive outcome measures are needed.
I do fully agree with the authors about the high usage of herbal and other so-called alternative medicines by children. We have shown that, in the UK the average one-year prevalence rate was 34% and the average lifetime prevalence was 42%. We have furthermore shown that the evidence base for these treatments in children is weak, even more so than for general populations. Finally, we can confirm that adverse effects are far from rare and often serious.
It is therefore high time, I think, that national regulators do more to protect children from SCAM practitioners who are at best uncritical about their treatments and at worse outright dangerous.
The 29th of February is an unusual date, and I will do something fittingly unusual today – something that I have never done before: I will with a heavy heart resign from an organisation of skeptics.
After I had observed the self-destructive debates within the GWUP for almost one year without saying a single word about it (hoping they would soon dissolve into thin air), I published a comment a few days ago. Soon after, I was aggressed, defamed, wrongly denounced as an anti-Semite, and blackmailed by leading members of that organisation.
Confronted with these events, it was inevitable that I would have doubts about my previous plan to remain a member until the upcoming general assembly in May. While I was contemplating, I received a Tweet on 27/2/2024 from someone under the pseudonym Endgegner der Kommentarspalten; it included this sentence:
Einer der verschwörungsideologischen Clowns, die seit gut einem Jahr Kulturkrieg in der GWUP mit rechtsextremen Talking Points spielen und Märchen von einem “woken Putsch” herbeiphantasieren?
My translation:
One of the conspiracy ideological clowns who have been playing culture war in the GWUP for a good year with right-wing extremist talking points and fantasising about a “woke coup”?
Next, I watched a long discussion on youtube between the new chair of the GWUP, my accuser (Bartoschek) and Sebastian Hirsch. There I learnt that the latter is, in fact, nobody else than Endgegner der Kommentarspalten. He was recently put in charge of Twitter account for GWUP by the chair.
At this point, I lost the hope that the GWUP might be saved. It seems to be in the hand of thugs who call not me personally but their opponents ‘ideological clowns who have been playing culture war’. They claim that they want to keep politics out of the GWUP, yet almost all they do is engaging in politics.
Since the former formidable chair, Amardeo Sarma, left and the rift started, the GWUP has done nothing wothwhile, as far as I can see. On the GWUP website, we are told that (my translation):
- The GWUP aims at promoting science and scientific thinking.
- The GWUP investigates parascientific theories according to the current state of scientific knowledge and reports publicly and comprehensibly on its findings.
- The GWUP aims to disseminate scientific and critical thinking and scientific methods, explain them in a generally understandable way and clearly distinguish real science from parascience. The GWUP thus wants to contribute to reducing society’s susceptibility to parascientific ideas and promises.
- The GWUP is an internationally orientated society. It is happy to work with like-minded individuals, organisations and institutions.
GWUP stands for ‘Gesellschaft zur wissenschaftlichen Untersuchung von Parawissenschaften’ (Society for the Scientific Investigation of Parasciences). The people currently in charge claim to be scientists but most of them are not (talking about science or publishing books for the lay reader about it does not, in my view, make you a scientist!). The leadership of the GWUP, it seems to me, is currently dominated by small-minded inward-looking guys with no international perspective who are in the middle of a mega-ego trip.
Instead of fighting parascience, they feel entitled to fight their colleagues. Instead of doing their job, they open the door to parascience. Instead of being scientists, they are using skepticism as an excuse for their machinations. Instead of running a scientific organisation, they turned it into a veritable kindergarden. In a nutshell: to the utmost delight of German parascientists, they have completely lost the plot.
I do not believe that the general assembly can turn things around. More likely, matters will get worse and it will come to a complete split. Personally, I cannot – not even until May – remain a member of an organisation where the man officially put in charge of the Twitter account feels entitled to collectively call his opponents ‘ideological clowns who have been playing culture war’. This remark in itself might not be all that significant but, for me, it is the ‘last straw’ and a symptom of a deep and irreversible rot.
So, I have come to the conclusion that I can do my work better without any further GWUP-hindrance. Therefore, I will now email my resignation as a member of the GWUP.