homeopathy
If you think that scanning through dozens of new scientific articles every week is a dry and often somewhat tedious exercise, you are probably correct. But every now and then, this task is turned into prime entertainment by some pseudoscientists trying to pretend to be scientists. Take, for instance, the latest homeopathy study by Indian researchers with no less than 9 seemingly impressive affiliations:
- 1Department of Organon of Medicine and Homoeopathic Philosophy, National Institute of Homoeopathy, Ministry of AYUSH, Govt. of India, Salt Lake, Kolkata, West Bengal, India.
- 2Department of Organon of Medicine and Homoeopathic Philosophy, National Institute of Homoeopathy, Ministry of AYUSH, Govt. of India, Block GE, Sector III, Salt Lake, Kolkata, West Bengal, India.
- 3Department of Homoeopathy, State Homoeopathic Dispensary, Karaila, Pratapgarh, Uttar Pradesh, India.
- 4Department of Homoeopathy, State Homoeopathic Dispensary, Tulsipur, Shrawasti, Uttar Pradesh, India.
- 5Department of Materia Medica, National Institute of Homoeopathy, Ministry of AYUSH, Govt. of India, Salt Lake, Kolkata, West Bengal, India.
- 6State Homoeopathic Dispensary, Mangalbari Rural Hospital, Matiali Block, Jalpaiguri, West Bengal, under Department of Health & Family Welfare, Govt. of West Bengal, India.
- 7Department of Repertory, The Calcutta Homoeopathic Medical College and Hospital, Govt. of West Bengal, Kolkata, West Bengal, India.
- 8Department of Homoeopathy, East Bishnupur State Homoeopathic Dispensary, Chandi Daulatabad Block Primary Health Centre, Village and Post Office: Gouripur (South), Police Station Bishnupur, West Bengal, under Department of Health & Family Welfare, Govt. of West Bengal, India.
- 9Department of Repertory, D. N. De Homoeopathic Medical College and Hospital, Govt. of West Bengal, Tangra, Kolkata, West Bengal, India.
Now that I have whetted your appetite, here is their study:
Lumbar spondylosis (LS) is a degenerative disorder of the lumbar spine. Despite substantial research efforts, no gold-standard treatment for LS has been identified. The efficacy of individualized homeopathic medicines (IHMs) in lumbar spondylosis (LS) is unknown. In this double-blind, randomized, placebo-controlled trial, the efficacy of IHMs was compared with identical-looking placebos in the treatment of low back pain associated with LS. It was conducted at the National Institute of Homoeopathy, West Bengal, India.
Patients were randomized to receive IHMs or placebos; standardized concomitant care was administered in both groups. The Oswestry low back pain and disability questionnaire (ODQ) was used as the primary outcome measure; the Roland-Morris questionnaire (RMQ) and the short form of the McGill pain questionnaire (SF-MPQ) served as secondary outcome measures. They were measured at baseline and every month for 3 months. Intention-to-treat analyses (ITT) were used to detect any inter-group differences using two-way repeated measures analysis of variance models overall and by unpaired t-tests at different time points.
Enrolment was stopped prematurely because of time restrictions; 55 patients had been randomized (verum: 28; control: 27); 49 could be analyzed by ITT (verum: 26; control: 23).
The results are as follows:
- Inter-group differences in ODQ (F 1, 47 = 0.001, p = 0.977), RMQ (F 1, 47 = 0.190, p = 0.665) and SF-MPQ total score (F 1, 47 = 3.183, p = 0.081) at 3 months were not statistically significant.
- SF-MPQ total score after 2 months (p = 0.030) revealed an inter-group statistical significance, favoring IHMs against placebos.
- Some of the SF-MPQ sub-scales at different time points were also statistically significant: e.g., the SF-MPQ average pain score after 2 months (p = 0.002) and 3 months (p = 0.007).
- Rhus Toxicodendron, Sulphur, and Pulsatilla nigricans were the most frequently indicated medicines.
The authors concluded that owing to failure in detecting a statistically significant effect for the primary outcome and in recruiting a sufficient number of participants, our trial remained inconclusive.
Now that I (and hopefully you too) have recovered from laughing out loud, let me point out why this paper had me in stitches:
- The trial was aborted not because of a “time limit” but because of slow recruitment, I presume. The question is why were not more patients volunteering? Low back pain with LS is extremely common. Could it be that patients know only too well that homeopathy does not help with low back pain?
- If a trial gets aborted because of very low patient numbers, it is probably best not to publish it or at least not to evaluate its results at all.
- If the researchers insist on publishing it, their paper should focus on the reason why it did not succeed so that others can learn from their experience by avoiding their mistakes.
- However, once the researchers do run statistical tests, they should be honest and conclude clearly that, because the primary outcome measure showed no inter-group difference, the study failed to demonstrate that the treatment is effective.
- The trial did not “remain inconclusive”; it was squarely negative.
- The editor of the journal HOMEOPATHY should know better than to publish such nonsense.
A final thought: is it perhaps the ultimate proof of homeopathy’s ‘like cures like’ assumption to use sound science (i.e. an RCT), submit it to the homeopathic process of endless dilutions and succussions, and – BINGO – generate utter nonsense?
About 3 years ago, I reported that the Bavarian government had decided to fund research into the question of whether the use of homeopathy would reduce the use of antibiotics (an idea that also King Charles fancies). With the help of some friends, I found further details of the project. Here are some of them:
The study on individualized homeopathic treatment to reduce the need for antibiotics in patients with recurrent urinary tract infections is a randomized, placebo-controlled, multicenter, double-blind trial. Frequent urinary tract infections (more than two infections within six months or more than three infections within twelve months) occur in up to three percent of all women during their lifetime and represent a high risk for increased antibiotic use in this population.
The current guidelines therefore also provide for therapeutic approaches without antibiotic administration under close monitoring. The approach to be investigated in the study is the administration of a homeopathic medicine individually selected for the patient for prophylaxis. The number of urinary tract infections and the need for antibiotics will be recorded and evaluated at the end of the trial period, around mid to late 2023.
The aim of the study is to find out whether patients taking homeopathics need antibiotics for the treatment of urinary tract infections less often compared to the placebo group. This could lead to a reduction in the use of antibiotics for recurrent urinary tract infections.
Project participants: Technical University of Munich, Klinikum Rechts der Isar
Project funding: 709,480.75 Euros
Project duration: January 1, 2021 to December 31, 2023
____________________
This sketch is of course not enough for providing a full evaluation of the study concept (if someone has more details, I’d be interested to learn more). From the little information given above, I feel that:
- the design of the trial might be quite rigorous,
- a fairly large sample will be required to have enough power,
- the closing date of 31/12/2023 seems optimistic (but this obviously depends on the number of centers cooperating),
- I, therefore, predict that we will have to wait a long time for the results (the pandemic and other obstacles will have delayed recruitment),
- the costs of the trial are already substantial and might increase due to delays etc.
My main criticism of the study is that:
- I see no rationale for doing such a trial,
- there is no evidence to suggest that homeopathy might prevent recurrent urinary tract infections,
- there is compelling evidence that homeopathic remedies are placebos,
- the study thus compares one placebo with another placebo (in fact, it is a classic example of what my late friend Harriet Hall would have called TOOTH FAIRY SCIENCE),
- therefore, its results will show no difference between the 2 groups (provided the trial was conducted without bias),
- if that is true, enthusiastic homeopaths will claim that the homeopathic verum was inadequate (e.g. because the homeopaths prescribing the verum did not or could not do their job properly),
- when that happens, they will therefore not stop claiming that homeopathy can reduce the over-prescribing of antibiotics;
- that means we will be exactly where we were before the trial.
In other words, the study will turn out to be a waste of 709,480.75 Euros. To express it as I did in my previous post: the Bavarian government has gone barmy!
Brillia for Children is probably the most amazing homeopathic quackery I have ever encountered:
Uses: Enhance clarity, improve concentration of attention, reduce feelings of anxiety & stress, excitability, irritability and hyperactivity to improve attention, focus and mood regulation.
Active Ingredient: Lapine S-100 immune globulin mixture of homeopathic dilutions 12C, 30C and 50C.
Brillia is a unique combination of antibody science and homeopathic formulation. The active ingredient of Brillia is antibodies to the brain-specific S100 protein (S100B). This protein is an important regulator of many different intracellular and extracellular brain processes, e.g. various enzymes activities, calcium homeostasis, communication between neurons, etc. Since almost all mental and neurological diseases as well as temporal stress-induced conditions are accompanied by disturbance of the above-mentioned processes, especially communication between neurons, the normalization of these processes is considered to be a prospective way to treat people with such undesirable conditions. Brillia is an antibody conjugated to the S100B protein and does not alter the concentration of the S100B protein in the bloodstream. Brillia’s efficacy stems from its ability to regulate the activity of the S100B protein and does not alter its concentration. In order for a protein to have an effect in the body, it needs to bind to its target, such as an enzyme. Proteins have very specific conformations that ensure that only the correct protein binds to the correct target molecule. Once the protein correctly orients itself into the active site of the target molecule, this is when the protein causes an effect in the body. When Brillia binds to the S100B protein, the overall shape of the protein is altered, hindering its ability to bind to its target molecule and thereby controlling its activity in the body. In short, Brillia stops the S100B protein from acting in the body by changing its shape, consequently regulating levels of anxiety and hyperactivity.
PARENT TOOL | WATCH: DISCOVER BRILLIA
WATCH: WHY & HOW BRILLIA WORKS
Inactive Ingredients: Lactose monohydrate, magnesium stearate, microcrystalline cellulose. Does not contain artificial colors or artificial flavors.
Food Allergy Warning: This product contains lactose. Brillia is gluten free and nut free.
About active ingredients, the website tells us this:
Let’s start off with the active ingredient, registered with the FDA as Lapine S-100B immune globulin. Now we know this name can be intimidating, so we are going to break it down for you. Working backwards, “immune globulin” is just the “sciency” way of saying “antibody”, and don’t worry, we will get into what an antibody actually is in just a second. Next, “S-100B” is the name of the protein the antibody is designed to recognize in the body. Lastly, “Lapine” is just a descriptor of the origin of the antibody, just like the millions of other antibodies used each and every day in laboratories all across the world.
So, what exactly is an antibody? Antibodies are a naturally occurring protein and component of our immune system that are individually programmed to target a very specific protein, in the case of Brillia, the S-100B protein. It is important to understand that antibodies are one of the most specific and targeted molecules in our bodies, resulting in zero off-target effects — meaning that antibodies specifically look for and attach to their target only. This is why Brillia has no harmful side effects, because it only interacts with the S-100B protein. Not only does Brillia have absolutely zero side effects, it also has no contraindications with any other medications or supplements your child may be taking. This is due to Brillia’s extremely high level of target specificity, meaning that Brillia is so well targeted to the S-100B protein, it won’t even think about touching anything else in the body, including any other drugs or supplements.
Now that we know more about the active ingredient, let’s talk about its target, the S-100B protein.
The S-100B protein is a naturally occurring protein and is most prevalent in the brain. It is an important regulator of many processes such as regulating calcium levels and helping neurons communicate, but in our case, we care about how it influences the symptoms we mentioned earlier, such as anxiety and hyperactivity.
Given that S-100B protein influences these symptoms, it is quite intuitive that when the S-100B protein doesn’t do its job properly, these symptoms become more prevalent, and this is exactly what happens in those who suffer from anxiety, hyperactivity, stress and lack of focus.
So, what makes the S-100B protein, for a lack of a better term, mess up? The answer is quite simple, when the S-100B protein is overproduced or overactive, its activity becomes unnecessarily high, making it capable of causing these symptoms.
The firm even has something vaguely resembling evidence: a study that “shows that over the course of 12 weeks, Brillia had a significantly better effect on the severity of anxiety over those that did not take Brillia, therefore proving Brillia’s efficacy.” They show some actual results but the methods or source of the study are not disclosed. On Medline, I could not find it either. Therefore, I asked the firm to send it to me. This is the answer I got:
“Our studies were conducted in Europe and then published on our website. Please click here to view the full details found on our site.”
So, they have a study that they commissioned in Europe; it was done by researchers unnamed. The firm then put some data of it on their website. In other words:
- we don’t know who was responsible for the study;
- we cannot evaluate how rigorous it was;
- it has never been peer-reviewed;
- it is now being used for promotional purposes.
Personally, I don’t find this acceptable. In my view, this does not provide a legitimation to make far-reaching claims about the remedy. Until I have evidence to the contrary, I thus deem it safe to conclude that Brillia has no effect other than enriching the manufacturer.
It has been reported that a German consumer association, the ‘Verbraucherzentrale NRW’, has first cautioned the manufacturer MEDICE Arzneimittel Pütter GmbH & Co. and then sued them for misleading advertising statements. The advertisement in question gave the wrong impression that their homeopathic remedy MEDITONSIN would:
- for certain generate a health improvement,
- have no side effects,
- be superior to “chemical-synthetic drugs”.
The study used by the manufacturer in support of such claims was not convincing according to the Regional Court of Dortmund. The results of a “large-scale study with more than 1,000 patients” presented a pie chart indicating that 90% of the patients were satisfied or very satisfied with the effect of Meditonsin. However, this was only based on a “pharmacy-based observational study” with little scientific validity, as pointed out by the consumer association. Despite the lack of evidence, the manufacturer claimed that their study “once again impressively confirms the good efficacy and tolerability of Meditonsin® Drops”. The Regional Court of Dortmund disagreed with the manufacturer and agreed with the reasoning of the consumer association.
“It is not permitted to advertise with statements that give the false impression that a successful treatment can be expected with certainty, as suggested by the advertising for Meditonsin Drops,” emphasizes Gesa Schölgens, head of “Faktencheck Gesundheitswerbung,” a joint project of the consumer centers of North Rhine-Westphalia and Rhineland-Palatinate. According to German law, this is prohibited. In addition, the Regional Court of Dortmund considered consumers to be misled by the advertising because the false impression was created that no harmful side effects are to be expected when Meditonsin Drops are taken. The package insert of the drug lists several side effects, according to which there could even be an initial worsening of symptoms after taking the drug.
The claim of advantages of the “natural remedy” represented by the manufacturer in comparison with “chemical-synthetic medicaments, which merely suppress the symptoms”, was also deemed to be inadmissible. Such comparative advertising is inadmissible.
__________________________________
This ruling is, I think, interesting in several ways. The marketing claims of so-called alternative medicine (SCAM) products seem all too often not within the limits of the laws. One can therefore hope that this case might inspire many more legal cases against the inadmissible advertising of SCAMs.
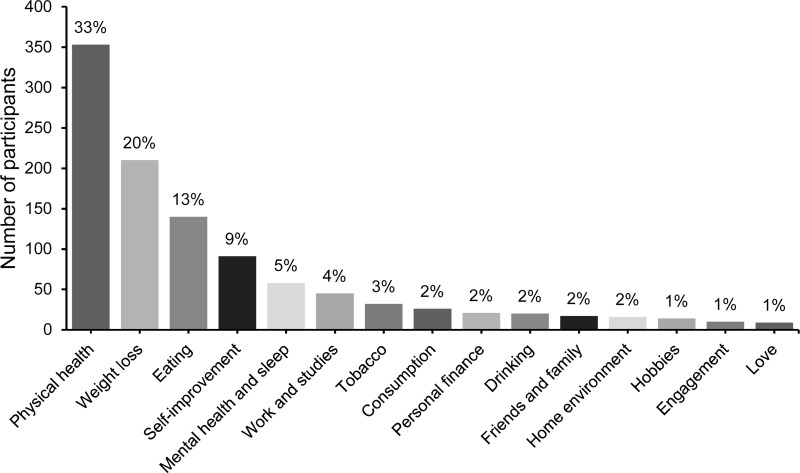
In 2020, a Swedish team published a study investigating what resolutions people make when they are free to formulate them, whether different resolutions reach differing success rates, and whether it is possible to increase the likelihood of a resolution’s success by administering information and exercises on effective goal setting. Participants (N = 1066) from the general public were randomized into three groups:
- active control,
- some support,
- and extended support.
The most popular resolutions regarded physical health, weight loss, and eating habits. At a one-year follow-up, 55% of responders considered themselves successful in sustaining their resolutions. Participants with approach-oriented goals were significantly more successful than those with avoidance-oriented goals (58.9% vs. 47.1%). The group that received some support was exclusively and significantly more successful compared to the other two.
The authors concluded that New Year’s resolutions can have lasting effects, even at a one-year follow-up.
This is a truly interesting study generating a lot of truly boring resolutions.
Boring is, however, something that we must avoid on this blog. In an attempt of doing just this, I decided to lodge my tongue in my cheek and formulate my very own resolutions for 2023 in relation to so-called alternative medicine (SCAM) and this blog. I shall:
- Never again call a comment or a commentator idiotic.
- Never state that chiropractors, homeopaths, osteopaths, naturopaths, or other SCAM practitioners are unethical charlatans.
- Never claim that subluxations, meridians, vital forces, etc. are pure fantasy.
- Never suggest that the assumptions of homeopathy fly in the face of science.
- Never imply that holism, integrative medicine, etc. are just sales gimmicks for crooks to boost their businesses.
- Never again demonstrate that a study is fraudulent just because its findings are too good to be true.
- Never again utter a critical word about our SCAM-loving sovereign, King Charles.
In case you are puzzled by my resolutions, please consider this: contrary to the above-cited evidence, it has been shown that only 12% of people who make new year’s resolutions will actually keep them. And this brings me to my last (and only realistic) resolution for 2023:
8. I shall not feel tempted to adhere to my New Year’s resolutions.
Animals cannot consent to the treatments they are given when ill. This renders the promotion and use of SCAM in animals a tricky issue. This systematic review assessed the evidence for the clinical efficacy of 24 so-called alternative medicines (SCAMs) used in cats, dogs, and horses.
A bibliographic search, restricted to studies in cats, dogs, and horses, was performed on Web of Science Core Collection, CABI, and PubMed. Relevant articles were assessed for scientific quality, and information was extracted on study characteristics, species, type of treatment, indication, and treatment effects.
Of 982 unique publications screened, 42 were eligible for inclusion, representing 9 different SCAM therapies, which were
- aromatherapy,
- gold therapy,
- homeopathy,
- leeches (hirudotherapy),
- mesotherapy,
- mud,
- neural therapy,
- sound (music) therapy,
- vibration therapy.
For 15 predefined therapies, no study was identified. The risk of bias was assessed as high in 17 studies, moderate to high in 10, moderate in 10, low to moderate in four, and low in one study. In those studies where the risk of bias was low to moderate, there was considerable heterogeneity in reported treatment effects.
The authors concluded that the present systematic review has revealed significant gaps in scientific knowledge regarding the effects of a number of “miscellaneous” SCAM methods used in cats, dogs, and horses. For the majority of the therapies, no relevant scientific articles were retrieved. For nine therapies, some research documentation was available. However, due to small sample sizes, a lack of control groups, and other methodological limitations, few articles with a low risk of bias were identified. Where beneficial results were reported, they were not replicated in other independent studies. Many of the articles were in the lower levels of the evidence pyramid, emphasising the need for more high-quality research using precise methodologies to evaluate the potential therapeutic effects of these therapies. Of the publications that met the inclusion criteria, the majority did not have any scientific documentation of sufficient quality to draw any conclusion regarding their effect. Several of our observations may be translated into lessons on how to improve the scientific support for SCAM therapies. Crucial efforts include (a) a focus on the evaluation of therapies with an explanatory model for a mechanism of action accepted by the scientific community at large, (b) the use of appropriate control animals and treatments, preferably in randomized controlled trials, (c) high-quality observational studies with emphasis on control for confounding factors, (d) sufficient statistical power; to achieve this, large-scale multicenter trials may be needed, (e) blinded evaluations, and (f) replication studies of therapies that have shown promising results in single studies.
What the authors revealed in relation to homeopathy was particularly interesting, in my view. The included studies, with moderate risk of bias, such as homeopathic hypotensive treatment in dogs with early, stage two heart failure and the study on cats with hyperthyroidism, showed no differences between treated and non-treated animals. An RCT with osteoarthritic dogs showed a difference in three of the six variables (veterinary-assessed mobility, two force plate variables, an owner-assessed chronic pain index, and pain and movement visually analogous scales).
The results on homeopathy are supported by another systematic review of 18 RCTs, representing four species (including two dog studies) and 11 indications. The authors excluded generalized conclusions about the effect of certain homeopathic remedies or the effect of individualized homeopathy on a given medical condition in animals. In addition, a meta-analysis of nine homeopathy trials with a high risk of bias, and two studies with a lower risk of bias, concluded that there is very limited evidence that clinical intervention in animals using homeopathic remedies can be distinguished from similar placebo interventions.
In essence, this review confirms what I have been pointing out numerous times: SCAM for animals is not evidence-based, and this includes in particular homeopathy. It follows that its use in animals as an alternative to treatments with proven effectiveness borders on animal abuse.
Hypericum perforatum (St John’s wort) is often recommended as a remedy to relieve pain caused by nerve damage. This trial investigated whether homeopathic Hypericum leads to a reduction in postoperative pain and a decrease in pain medication compared with placebo.
The study was designed as a randomized double-blind, monocentric, placebo-controlled clinical trial with inpatients undergoing surgery for lumbar sequestrectomy. Homeopathic treatment was compared to placebo, both in addition to usual pain management. The primary endpoint was pain relief measured with a visual analog scale. Secondary endpoints were the reduction of inpatient postoperative analgesic medication and change in sensory and affective pain perception.
The results show that the change in pain perception between baseline and day 3 did not significantly differ between the study arms. With respect to pain medication, total morphine equivalent doses did not differ significantly. However, a statistical trend and a moderate effect (d = 0.432) in the decrease of pain medication consumption in favor of the Hypericum group was observed.
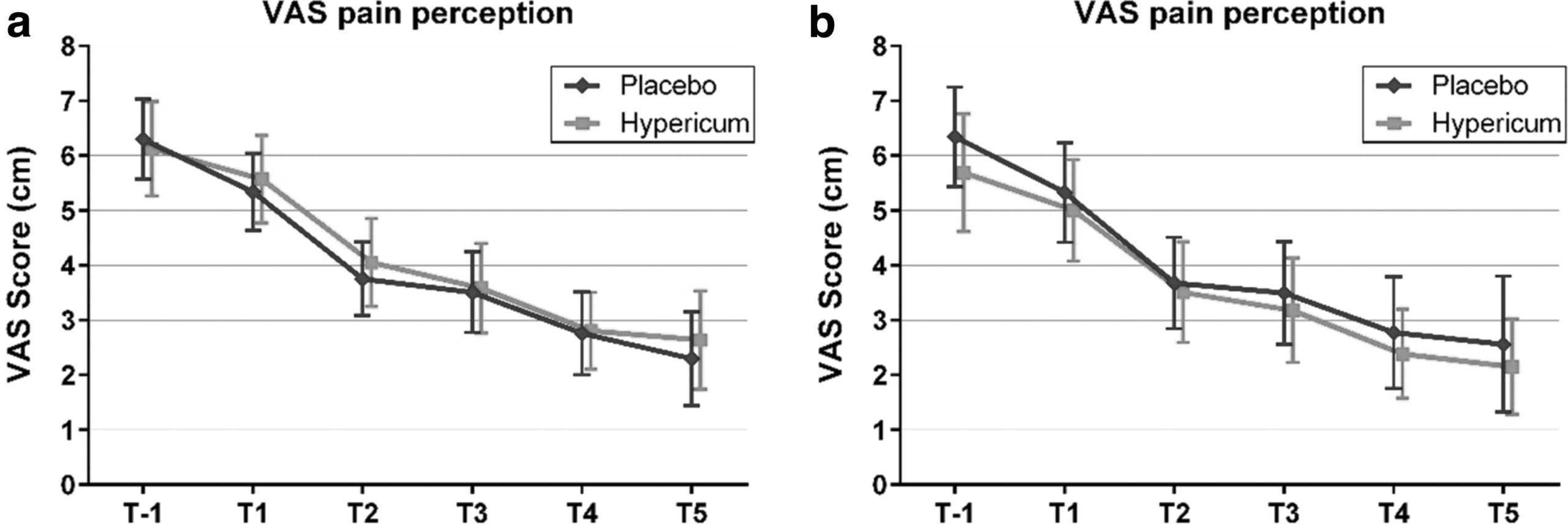
The authors concluded that this is the first trial of homeopathy that evaluated the efficacy of Hypericum C200 after lumbar monosegmental spinal sequestrectomy. Although no significant differences between the groups could be shown, we found that patients who took potentiated Hypericum in addition to usual pain management showed lower consumption of analgesics. Further investigations, especially with regard to pain medication, should follow to better classify the described analgesic reduction.
For a number of reasons, this is a remarkably mysterious and quite hilarious study:
- Hypericum is recommended as an analgesic for neuropathic pain.
- According to the ‘like cures like’ axiom of homeopathy, it therefore must increase pain in such situations.
- Yet, the authors of this trial mounted an RCT to see whether it reduces pain.
- Thus they either do not understand homeopathy or wanted to sabotage it.
- As they are well-known pro-homeopathy researchers affiliated with a university that promotes homeopathy (Witten/Herdecke University, Herdecke, Germany), both explanations are highly implausible.
- The facts that the paper was published in a pro-SCAM journal (J Integr Complement Med), and the study was sponsored by the largest German firm of homeopathics (Deutsche Homoeopathische Union) renders all this even more puzzling.
- However, these biases do explain that the authors do their very best to mislead us by including some unwarranted ‘positive’ findings in their overall conclusions.
In the end, none of this matters, because the results of the study reveal that firstly the homeopathic ‘law of similars’ is nonsense, and secondly one homeopathic placebo (i.e. Hypericum C200) produces exactly the same outcomes as another, non-homeopathic placebo.
It’s again the season for nine lessons, I suppose. So, on the occasion of Christmas Eve, let me rephrase the nine lessons I once gave (with my tongue firmly lodged in my cheek) to those who want to make a pseudo-scientific career in so-called alternative medicine (SCAM) research.

- Throw yourself into qualitative research. For instance, focus groups are a safe bet. They are not difficult to do: you gather 5 -10 people, let them express their opinions, record them, extract from the diversity of views what you recognize as your own opinion and call it a ‘common theme’, and write the whole thing up, and – BINGO! – you have a publication. The beauty of this approach is manifold:
-
- you can repeat this exercise ad nauseam until your publication list is of respectable length;
- there are plenty of SCAM journals that will publish your articles;
- you can manipulate your findings at will;
- you will never produce a paper that displeases the likes of King Charles;
- you might even increase your chances of obtaining funding for future research.
- Conduct surveys. They are very popular and highly respected/publishable projects in SCAM. Do not get deterred by the fact that thousands of similar investigations are already available. If, for instance, there already is one describing the SCAM usage by leg-amputated policemen in North Devon, you can conduct a survey of leg-amputated policemen in North Devon with a medical history of diabetes. As long as you conclude that your participants used a lot of SCAMs, were very satisfied with it, did not experience any adverse effects, thought it was value for money, and would recommend it to their neighbour, you have secured another publication in a SCAM journal.
- In case this does not appeal to you, how about taking a sociological, anthropological or psychological approach? How about studying, for example, the differences in worldviews, the different belief systems, the different ways of knowing, the different concepts about illness, the different expectations, the unique spiritual dimensions, the amazing views on holism – all in different cultures, settings or countries? Invariably, you must, of course, conclude that one truth is at least as good as the next. This will make you popular with all the post-modernists who use SCAM as a playground for enlarging their publication lists. This approach also has the advantage to allow you to travel extensively and generally have a good time.
- If, eventually, your boss demands that you start doing what (in his narrow mind) constitutes ‘real science’, do not despair! There are plenty of possibilities to remain true to your pseudo-scientific principles. Study the safety of your favourite SCAM with a survey of its users. You simply evaluate their experiences and opinions regarding adverse effects. But be careful, you are on thin ice here; you don’t want to upset anyone by generating alarming findings. Make sure your sample is small enough for a false negative result, and that all participants are well-pleased with their SCAM. This might be merely a question of selecting your patients wisely. The main thing is that your conclusions do not reveal any risks.
- If your boss insists you tackle the daunting issue of SCAM’s efficacy, you must find patients who happened to have recovered spectacularly well from a life-threatening disease after receiving your favourite form of SCAM. Once you have identified such a person, you detail her experience and publish this as a ‘case report’. It requires a little skill to brush over the fact that the patient also had lots of conventional treatments, or that her diagnosis was never properly verified. As a pseudo-scientist, you will have to learn how to discretely make such details vanish so that, in the final paper, they are no longer recognisable.
- Your boss might eventually point out that case reports are not really very conclusive. The antidote to this argument is simple: you do a large case series along the same lines. Here you can even show off your excellent statistical skills by calculating the statistical significance of the difference between the severity of the condition before the treatment and the one after it. As long as this reveals marked improvements, ignores all the many other factors involved in the outcome and concludes that these changes are the result of the treatment, all should be tickety-boo.
- Your boss might one day insist you conduct what he narrow-mindedly calls a ‘proper’ study; in other words, you might be forced to bite the bullet and learn how to do an RCT. As your particular SCAM is not really effective, this could lead to serious embarrassment in the form of a negative result, something that must be avoided at all costs. I, therefore, recommend you join for a few months a research group that has a proven track record in doing RCTs of utterly useless treatments without ever failing to conclude that it is highly effective. In other words, join a member of my ALTERNATIVE MEDICINE HALL OF FAME. They will teach you how to incorporate all the right design features into your study without the slightest risk of generating a negative result. A particularly popular solution is to conduct a ‘pragmatic’ trial that never fails to produce anything but cheerfully positive findings.
- But even the most cunningly designed study of your SCAM might one day deliver a negative result. In such a case, I recommend taking your data and running as many different statistical tests as you can find; chances are that one of them will produce something vaguely positive. If even this method fails (and it hardly ever does), you can always focus your paper on the fact that, in your study, not a single patient died. Who would be able to dispute that this is a positive outcome?
- Now that you have grown into an experienced pseudo-scientist who has published several misleading papers, you may want to publish irrefutable evidence of your SCAM. For this purpose run the same RCT over again, and again, and again. Eventually, you want a meta-analysis of all RCTs ever published (see examples here and here). As you are the only person who conducted studies on the SCAM in question, this should be quite easy: you pool the data of all your dodgy trials and, bob’s your uncle: a nice little summary of the totality of the data that shows beyond doubt that your SCAM works and is safe.
The year 2022 is drawing to a close, and I am reminded of my ‘WORST PAPER OF 2022 COMPETITION’. As a prize, I am offering the winner (that is the lead author of the winning paper) one of my books that best fits his/her subject. I am sure this will overjoy him or her. I hope to identify about 10 candidates for the prize, and towards the end of the year, I let my readers decide democratically on who should be the winner. In this spirit of democratic voting, let me suggest to you entry No 10 entitled ‘Conventional Homeopathic Medicine and Its Relevance to Modern Medicine‘. Here is the unadulterated abstract:
Context: Homeopathic medicine can be explained as a symptoms-based method of treatment, and it can act as an alternative treatment strategy against allopathy by focusing on the symptoms of illness, as opposed to causative agents as allopathic medicine does. Also, homeopathic medicines are extracted from nature rather than being chemically synthesized as western drugs are.
Objective: The review intended to briefly describe the concept of homeopathic medicine, its emergence from a historical point of view, and its broader healing properties, providing examples of key homeopathic drugs and comparing them to modern medicines.
Design: The research team performed a narrative review by searching databases like Pubmed, Google Scholar, and other national search engines. The search used the keywords homeopathic medicine, alternate medicine, materia medica, allium cepa, Zingiber officinale, penicillium, Agaricus muscaria, Botulinum toxin.
Setting: Dr. D.Y. Patil Homoeopathic Medical College and Research Centre, Dr. D.Y. Patil Vidyapeeth (Deemed to be University), Pimpri, Pune.
Results: This review highlights the rich sources homoeopathic drugs and their corelation with modern medicine. The current review focuses on the significance of the Homeopathic Materia Medica and on notable remedies in homeopathy that align with allopathy in addressing different pathological conditions, including treatments that the two types of medicine have in in common and that are effective in homeopathy.
Conclusions: Many studies are being conducted to prove the mechanism of action of homoeopathic medicines. Droplet Evaporating Method (DEM), Raman, UltraViolet-Visible (UV-VIS) spectroscopy and Transmission Electron Microscopy (TEM) are commonly used methods to characterize homeopathic medicines at ultra-low concentration and many such studies will surely indicate how homoeopathic medicines act. Such research results may subsequently lead to the betterment of treatment procedures and the integration of homeopathic principles into mainstream medical practices.
I find it quite an ‘achievement’ to put so much nonsense into such a short abstract. My ‘favorite’ statement is this one: “many such studies will surely indicate how homoeopathic medicines act.” Since he published this paper, the first author has done another article; it is entitled “Breast Abscess Healing with Homoeopathy: A Case Report” and would be a further contender for my award.
But let’s not give him an unfair chance to win the competition!
PS
The next time I post about this will be about deciding on this year’s winner. So, you might want to give it some consideration.
This Cochrane review assessed the effectiveness and safety of oral homeopathic medicinal products compared with placebo or conventional therapy to prevent and treat acute respiratory tract infections (ARTIs) in children.
The researchers included double‐blind randomized clinical trials (RCTs) or double‐blind cluster‐RCTs comparing oral homeopathy medicinal products with placebo or self‐selected conventional treatments to prevent or treat ARTIs in children aged 0 to 16 years.
In this 2022 update, the researchers identified three new RCTs involving 251 children, for a total of 11 included RCTs with 1813 children receiving oral homeopathic medicinal products or a control treatment for ARTIs. All studies focused on upper respiratory tract infections (URTIs), with only one study including some lower respiratory tract infections (LRTIs). Six RCTs examined the effect on URTI recovery, and five RCTs investigated the effect on preventing URTIs after one to four months of treatment. Two treatment and three prevention studies involved homeopaths individualizing treatment. The other studies used predetermined, non-individualized remedies. All studies involved highly diluted homeopathic medicinal products, with dilutions ranging from 1 x 10‐4 to 1 x 10‐200.
Several limitations to the included studies were identified, in particular methodological inconsistencies and high attrition rates, failure to conduct intention‐to‐treat analysis, selective reporting, and apparent protocol deviations. Three studies were classified as at high risk of bias in at least one domain, and many studies had additional domains with unclear risk of bias. Four studies received funding from homeopathy manufacturers; one study support from a non‐government organization; two studies government support; one study was co‐sponsored by a university; and three studies did not report funding support.
The authors concluded that the “pooling of five prevention and six treatment studies did not show any consistent benefit of homeopathic medicinal products compared to placebo on ARTI recurrence or cure rates in children. We assessed the certainty of the evidence as low to very low for the majority of outcomes. We found no evidence to support the efficacy of homeopathic medicinal products for ARTIs in children. Adverse events were poorly reported, and we could not draw conclusions regarding safety.”
____________________________
These findings are hardly surprising. Will they change the behavior of homeopaths who feel that
- children respond particularly well to homeopathy,
- ARTIs are conditions for which homeopathy is particularly effective?
I would not hold my breath!